
Abstract
Background:
Paramedics are increasingly involved in palliative care and often support community-based palliative care service delivery to facilitate integrated practice. However, the impact of specific palliative care guidelines on clinical practice remains unknown.
Aim:
To determine the impact of an ambulance service palliative care guideline on rates of supportive medication administration and non-transport.
Design:
A retrospective cohort study of electronic patient care records from January 2014 to June 2023. Baseline characteristics were compared pre- and post-guideline introduction. Interrupted time series analysis was performed to examine guideline efficacy.
Setting/participants:
Patients of all ages receiving palliative care who were attended by paramedics in Victoria, Australia.
Results:
A total of 31,579 patients were included. The median age was 75 years (IQR = 64–84 years), and 56.4% were men. Overall, 25.8% of patients were not transported to hospital. Following guideline introduction, there were no significant trend changes in administration of supportive medications. However, the non-transport rate increased significantly per month (0.2%, p = 0.007), amounting to a 9.9% (p = 0.020) total increase by the end of the study period compared to a scenario in which the guideline had not been introduced. Subgroup analysis of patients diagnosed with ‘pain’ or attended after-hours also showed significant increases in non-transport (monthly increase: pain 0.3%, p = 0.003; after-hours 0.3%, p < 0.001; total increase: pain 29.7%, p < 0.001, after-hours 22.6%, p = 0.001).
Conclusions:
Introduction of a palliative care guideline was associated with a decrease in ambulance transport to emergency departments, allowing more patients continuity of care in the community.
Paramedics provide care for patients in the community experiencing healthcare emergencies of a diverse nature.
Few studies have described paramedic palliative care clinical practice guidelines, or their impact on paramedic decision making regarding treatment and transport.
Introduction of a pre-hospital palliative care guideline was associated with a significant increase in the proportion of patients who remained at home. This finding was reflected in subgroup analyses of patients with a paramedic diagnosis of pain and those seen after-hours.
A palliative care guideline effectively expanded paramedics’ scope to treat patients symptomatically while still fulfilling their wishes to remain in a preferred place.
Understanding how the introduction of a palliative care guideline impacted paramedic clinical decision-making and patient outcomes may inform further optimisation of guidelines and associated training, including availability of referral pathways (particularly after-hours), palliative-specific medications, dosages and routes of administration and provision of holistic support for patients and caregivers.
The demonstrated ability for paramedics to value-add in assisting patients to remain in their preferred place, particularly at the end-of-life, should encourage collaboration between ambulance and palliative care services to establish consistent broader guidelines, competency frameworks and training for pre-hospital palliative care delivery.
Introduction
The trajectory of a growing, aging population, with associated increases in disease burden and life-limiting illnesses, forecasts unsustainable demand for specialist palliative care services.1 –3 Recent changes in practice to better align with shifting patient preferences towards home-based deaths means more patients and families are experiencing end-of-life in the community.1,4 –7 The World Health Organisation identifies a key attribute of palliative care as to ‘provide relief from pain and other distressing symptoms’. 8 However, patients who die at home are significantly more likely to experience severe symptoms in the acute end-of-life phase, specifically pain, dyspnoea, nausea and bowel problems. 9 Evidence suggests caregivers of patients receiving community-based palliative care are less satisfied with management of patient symptoms, comfort, psychological care and family support compared to inpatients.10,11 Funding limitations mean community palliative care services are not always available after-hours, and paramedics are often called upon to fill this void for patients requiring unscheduled care.
Paramedics as a workforce are well positioned to address this demand and support the delivery of community palliative care services.12,13 Interview and focus group studies from the United Kingdom, Germany, Canada and Australia have explored paramedic, patient and family experiences of pre-hospital delivery of palliative care.12,14 –16 Findings support leveraging paramedics to complement community palliative care service delivery. However, to date, there have been few studies describing pre-hospital palliative care, relevant clinical guidelines or the impact of such guidelines on clinical practice.17,18 Existing evidence primarily evaluates efficacy of localised or pilot programs, often involving specialist paramedic teams.12,19 –21
This study seeks to fill this gap in the literature by quantitatively describing trend changes in clinical practice post implementation of a generalist palliative care guideline. A recent pre-hospital palliative care guideline content review highlighted the value in an international shift from protocol-driven practice towards paramedic-led clinical decision-making models. 22 The aim of this study was to determine if the introduction of a palliative care clinical practice guideline was associated with a shift in paramedic clinical decision-making, represented as an increase in the rate of non-transport or supportive medication administration.
Methods
Study design
A retrospective cohort study design was chosen to utilise pre-existing electronic patient care record (ePCR) data to examine the effect of palliative care guideline introduction on analgesia administration and ambulance transport. Interrupted time series analysis (ITSA) with autocorrelation was employed for statistical analysis as it is a strong quasi-experimental design, frequently utilised for evaluation of health system quality improvement interventions.23 –25 This study was approved by the Monash University Human Research Ethics Committee (Project ID: 38802).
Setting
The state-based ambulance service in Victoria, Australia (Ambulance Victoria) services a population of 6.8 million, from metropolitan, regional and rural communities across >227,000 km2. Paramedics in Victoria are registered with the Paramedicine Board of Australia, and make autonomous clinical decisions regarding treatment, transport and referral, informed by clinical practice guidelines. 26
In October 2017, Ambulance Victoria introduced a palliative care clinical practice guideline (Supplemental Appendix A) applicable to patients already registered with a palliative care service, not receiving active treatment and wanting to remain at home. 13 With a scope of practice including provision of analgesia, sedatives and antiemetics, paramedics can liaise directly with patients’ palliative care teams or the 24-h Palliative Care Advice Service and implement treatment plans allowing patients to remain in place.22,26,27 The guideline provides guidance for paramedics to administer supportive medications without the requirement for transport to hospital, although patients <16 years old require medical consultation. 26 These medications include morphine or fentanyl for dyspnoea, pain or associated agitation and midazolam for agitation not associated with pain. Subcutaneous route administration was introduced as a new skill during face-to-face training for the guideline between May and October 2017. 28
Data collection
Paramedics in Victoria complete comprehensive electronic patient care records (ePCR) including scene details, patient demographics, clinical observations, treatments, final assessment and a free-text case description. The ePCR software template is utilised for all cases and is described elsewhere. 29 Data from ePCRs is uploaded wirelessly into a data warehouse, from which data were extracted for analysis. Data from 1 January 2014 through to 30 June 2023 was collected for all patients identified as receiving palliative care. Data was analysed for two chronological subgroups defined as Pre-Guideline (01/01/2014–19/10/2017), and Post-Guideline (20/10/2017–30/06/2023).
Epidemiological data extracted from the data warehouse included patient age, gender and rurality. Ambulance service operational data obtained included an indicator for transport, at scene time and total case-time. Clinical data extracted included final primary assessment/provisional diagnosis, not transported reason where applicable and indicator variables for the administration of morphine, fentanyl, midazolam, ondansetron and metoclopramide. The two primary outcome variables were non-transport and administration of supportive medications. Supportive medications included morphine, fentanyl, midazolam, ondansetron and metoclopramide. Total case-time was defined as time elapsed between arrival at scene and ‘clear time’ when the paramedic crew became available for a new case.
Participants
Patients of any age attended by paramedics who had the following search terms recorded in their ePCR met inclusion criteria: ‘not transported reason’ recorded as ‘patient for palliative care only’; free-text ‘case description’ containing key terms allowing for spelling errors: ‘palliative; palliated; palliate; paliative; paliated; paliate; pallative; pallated; pallate; terminally ill; terminal patient; terminal pt; terminal cancer; terminal ca’. Exclusion criteria focussed on cases with potential to confound the data. Patients with a provisional diagnosis of ‘fracture’, ‘dislocation’ or ‘burns’, indicating an acute traumatic injury, were excluded as these presentations were likely to require transport and administration of supportive medications for traumatic pain. Cases where patients were identified as ‘deceased on arrival’ were excluded as these did not require paramedics to make treatment or transport decisions. Further, cases within a 3-month period of industrial action (26/09/2014–20/12/2014), during which very few ePCRs were generated, were excluded due to lack of data availability. Lastly, patients with pre-booked ‘non-emergent patient transfers’ were excluded.
Statistical analysis
Statistical analyses were undertaken using Stata™ Statistical Software version 18. 30 Statistical outcomes were considered significant if p-values were less than 0.05. Categorical variables were reported as frequencies and proportions (%), with chi-squared analysis used to draw comparisons across the two defined time periods. Continuous data were reported as median and interquartile range (IQR), with the Kruskal-Wallis test used to compare time periods.
Interrupted time series analysis was conducted to estimate the effect of guideline introduction on the monthly proportion of non-transported patients, the proportion of patients administered supportive medication and the proportion who were both not transported and received supportive medication.23 –25 ITSA allows estimation of an immediate ‘step’ increase or decrease in each outcome following implementation of the guideline, as well as estimation of a post-intervention change in trend of each outcome. A predefined interruption in October 2017 represented palliative care guideline introduction. Subgroup analyses were performed to examine the effect of the guideline on patients seen after-hours and patients with a diagnosis of ‘pain’. All models were adjusted for season and after-hours presentation (excluding the after-hours subgroup analysis). All models were adjusted for the following changes in ambulance service delivery: October 2016: (1) alterations to the ambulance dispatch model 31 which involved an increase in the proportion of lower acuity patients being referred to alternative service providers; and, (2) introduction of antiemetic ondansetron; April 2018: an education campaign encouraging transport of patients with deranged vital signs which were associated with an increase in transport rate; March 2020: commencement of COVID-19 pandemic lockdown restrictions which were associated with decreased ambulance demand and transport rate.26,32,33 For each model, data for the 4 months of 2014 with missing data were interpolated from 2014 means. The partial autocorrelation function was examined for each outcome, and Newey-West standard errors were used to account for autocorrelation of error terms. In total, five to seven lags were used in each model to ensure robustness, allowing for autocorrelation reflecting variations in service utilisation due to factors not fully captured by other covariates in the model. We calculated counterfactuals to estimate each outcome assuming that the guideline was not implemented. This involved calculating predictive margins for each outcome with the guideline and post-guideline trend terms equal to 0. We also performed supplementary negative control exposure analysis using a fictitious intervention (see Supplemental Appendix B). Results were presented as proportions (%) and 95% confidence intervals (CI).
Results
Population sample
A total of 41,732 palliative care cases were attended between January 2014 and June 2023. Of these, 31,579 (75.7%) cases met inclusion criteria, as shown in Figure 1. A total of 8,850 (28%) cases occurred prior to palliative care guideline implementation (pre-guideline), while 22,729 (72%) occurred post-guideline.
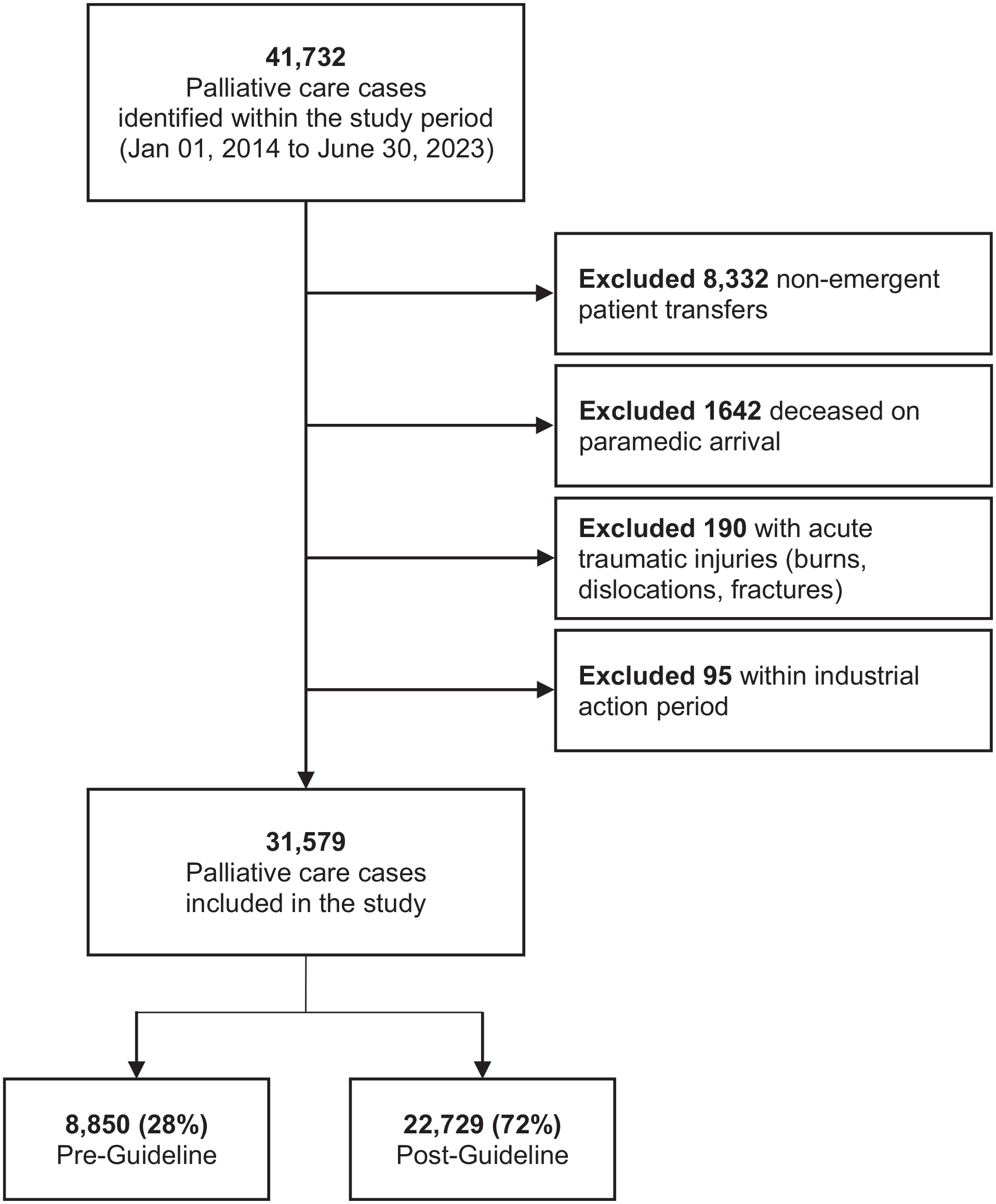
Palliative care cases attended by paramedics during study period.
Baseline characteristics
Baseline characteristics are presented in Table 1. Median patient age was 75 years (IQR = 64–84 years), and 56.4% of patients were men. The majority of patients attended were in metropolitan regions (57.1%), however this decreased after guideline implementation, p < 0.001. Total case-time for transported patients increased from 149-min (IQR = 117–186) to 185-min (IQR = 142–239) post-guideline, p < 0.001. In contrast, case-time for non-transported patients decreased from 87-min (IQR = 62–124) to 84-min (IQR = 57–121), p = 0.006. There were significant increases in the proportion of patients with paramedic diagnoses of pain (17.6% vs 21.1%, p < 0.001) and dyspnoea (14.8% vs 17.5%, p < 0.001).
Patient and case characteristics.

Paramedic interventions
Paramedic interventions are presented in Table 2. The rate of non-transport increased from 23.5% pre-guideline implementation to 26.7% post-guideline implementation, p < 0.001. Specifically, for patients who received supportive medications, non-transport increased from 4.0% to 13.5%. Patients with a non-transport reason of ‘Referred to other provider/Pt for palliative care only’ were similar between groups, however, it was not possible to determine whether paramedics consulted with the patient’s physician or palliative care team. There was a significant increase in documentation of ‘Transport not required’ as the reason for non-transport (5.9% vs 8.6%, p < 0.001). Overall administration of supportive medications also increased significantly (14.7% vs 23.3%, p < 0.001), a trend which was reflected in each individual medication. The frequency of subcutaneous administrations was very low (46, 0.2%; Table 2).
Paramedic initiated interventions.

Time series analysis
There was no immediate step change in number of patients who were not transported following guideline introduction. However, there was a statistically significant, sustained increase per month (0.2%, 95% CI = 0.04%–0.3%, p = 0.007), such that by the end of the study period, the guideline was associated with a 9.9% increase in non-transport, p = 0.020 (Table 3). Guideline implementation was not associated with a change in level or trend of supportive medication administration. However, there was a significant step increase in the proportion of patients who were both administered supportive medications and not transported to hospital after guideline introduction (0.7%, 95% CI = 0.2%–1.1%, p = 0.008). The fictitious intervention analyses are presented in Supplemental Appendix B (Figure 2).
Interrupted time series analysis results summary.

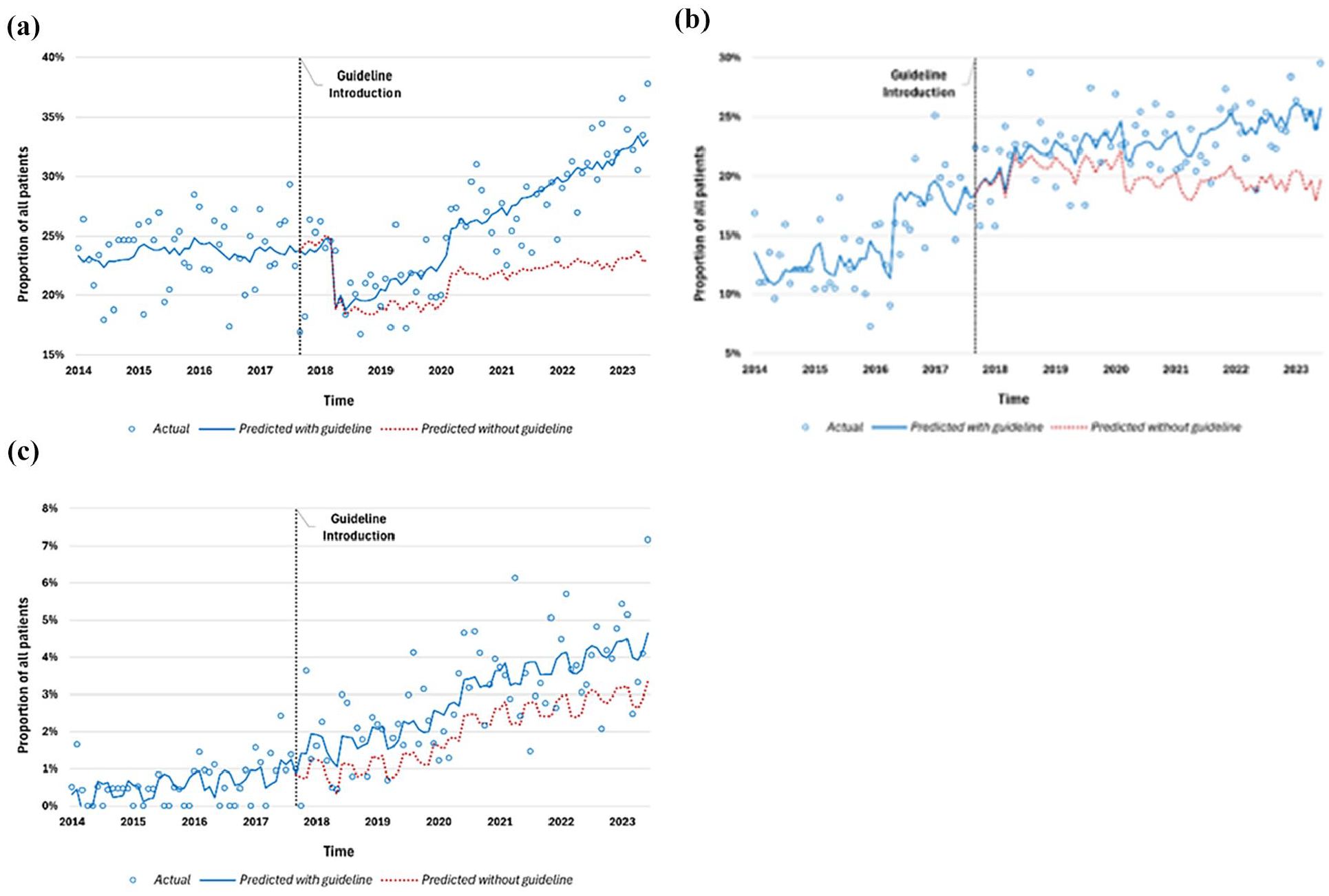
Interrupted time series analysis graphs: (a) non-transport, (b) supportive medication administration and (c) medication with non-transport.
Subgroup analyses
After guideline implementation, there was no immediate increase in non-transport rate for patients seen after-hours, however, there was a significant change in trend (0.3%, 95% CI = 0.18–0.52, p < 0.001, Figure 3(a). By the end of the study period, this equated to a 22.6% (p = 0.001) increase compared to a scenario where the guideline had not been introduced. Patients with a paramedic diagnosis of ‘pain’ demonstrated a significant step increase in non-transport after guideline introduction (8.9%, 95% CI = 6%–12%, p < 0.001, Figure 3(b)), and a significant post-guideline increase in trend (0.3% per month, 95% CI = 0.1%–0.5%, p = 0.003). By the end of the study period, there was a 29.7% (95% CI = 15.4%–44%, p < 0.001) increase compared to a scenario without guideline introduction. Patients with a paramedic diagnosis of ‘pain’ also demonstrated a step increase in administration of supportive medications without transport (2.1%, 95% CI = 0.6%–3.6%, p = 0.007).
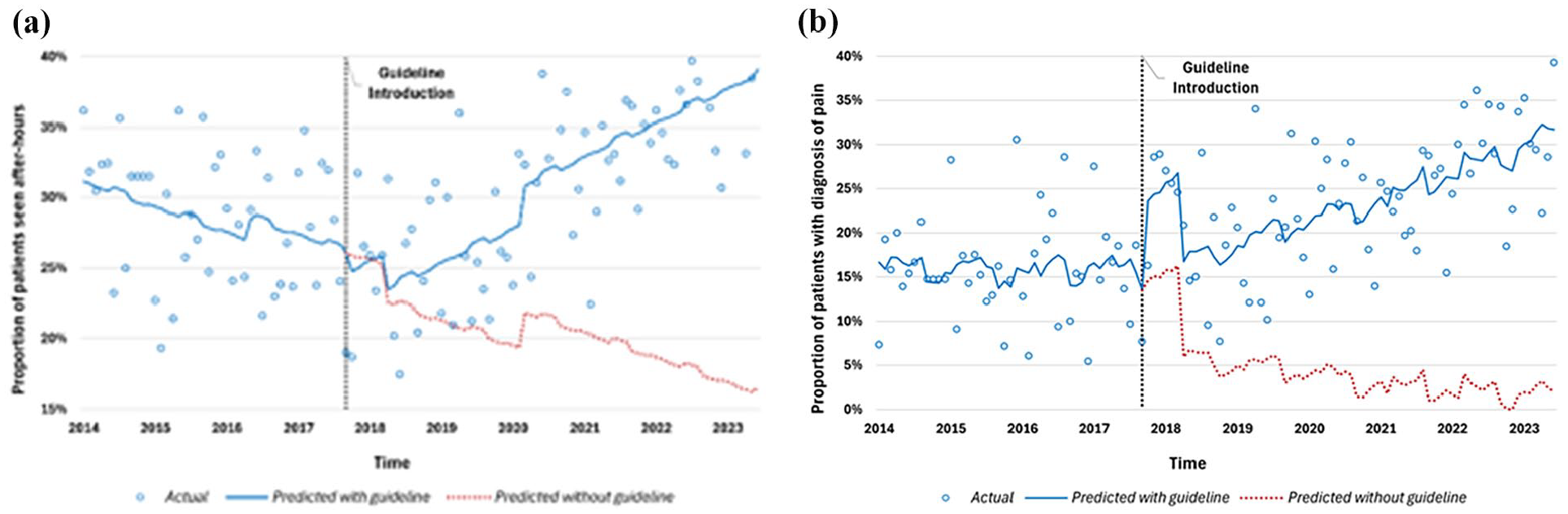
Subgroup analysis graphs: (a) after-hours non-transport and (b) pain non-transport.
Discussion
Main findings
We found that the introduction of a pre-hospital palliative care guideline which encouraged administration of supportive medications without subsequent ambulance transport was successful in increasing non-transport of patients. However, the majority (73.3%) of patients receiving palliative care presenting to paramedics are still transported to emergency departments. Whilst we did not see an increase in administration of supportive medications, we did see an increase in the proportion of patients who received supportive medications without subsequent transport to an emergency department. These findings demonstrate that paramedics were already administering supportive medications to patients experiencing pain; however, prior to guideline implementation, they were also frequently transporting these patients to hospital. The introduction of a palliative care guideline appears to have effectively expanded paramedic scope to facilitate symptomatic management while still fulfilling patient wishes to remain at home where expressed.
What this study adds?
This study addresses a significant gap in the literature through analysing the effect on clinical practice trends of a large, jurisdictional ambulance service generalist palliative care guideline. In contrast, other studies globally have examined efficacy of localised or pilot programs, typically involving specialist paramedic teams.34,35 Whilst there has been extensive qualitative research exploring clinician and patient perspectives in the area of palliative paramedicine,17,18 there are limited population-based studies within the international literature and a mixed-methods approach is essential to accurately represent efficiency and efficacy. 36 Nova Scotia’s ‘Paramedics Providing Palliative Care at Home Program’ identified essential elements for implementation and scaling, including de-siloed communication, locally-tailored training and shifting the traditional paramedic mindset from medication necessitates transport and from curative to supportive cares.20,35 Similarly, evaluation of the first 100 patients enrolled in British Columbia’s ‘Palliative Care Assess, See, Treat and Refer (ASTaR)’ non-transport clinical pathway found paramedics provided a critical role and value-add in palliative care delivery, especially after-hours, aligning with our findings in after-hours care. 20 The value of integration is also recognised in low-to middle-income countries, where a South African study of patients receiving palliative care conveyed by ambulance reported symptoms such as pain (16%) and dyspnoea (36%), which could be managed within the paramedic scope of practice. 21 Globally, optimisation should target co-designed, integrated guidelines and models of care through collaboration between local ambulance and palliative care services.11,35,37
Effective symptom management and psychosocial support can prevent unwanted transport to hospital, allowing patients to remain in their preferred place.17,38 However, whilst many patients express and document wishes to die at home, the decision often becomes that of substitute decision makers and shifts towards hospital-based care as deterioration occurs, care needs escalate and carer burnout occurs.10,39,40 Canadian studies found >50% of patients who remained in place did not receive pharmacological management, but instead required non-technical skills such as repositioning; mobility assistance; education; goals-of-care discussions; support for carer medication administration; or suction, wound or personal cares.12,20 Of those who did require pharmacological management, 99.2% were not transported to hospital, a significant shift in practice from the traditional paramedic mindset. 20 In contrast, patients not transported after medication administration in our study increased from 4.0% to 13.5% post-guideline implementation. This may be a more realistic estimate of palliative care-specific guideline impact within the broader paramedic workforce.12,34 This study complements international pre-hospital palliative care guideline content review literature by providing data on outcomes associated with implementation. 22 Existing guidelines highlight a clear international shift towards paramedic-led clinical decision-making models, supported by palliative teleconsultation services; however, gaps remain for patients not known to palliative care services, and bereavement support.19,22
Implications for clinical practice
Paramedics are increasingly becoming decision makers in palliative care. De-siloing and integration of paramedicine and community palliative care requires effective communication using shared language and tools. 41 Future research should determine if hospital-based tools adapted to triage palliative referral among residential aged care facility residents are translatable to the pre-hospital environment, and could add value in communication with palliative consultation services and facilitate palliative care referrals.42,43 It is notable that a significant number of patients had a paramedic diagnosis of ‘infection’, as end-of-life symptoms can mimic or occur concurrently with infection. 8 Ongoing education of paramedics in recognition of end-of-life may assist with expectation management, interprofessional communication and decision-making to facilitate deaths in line with patient wishes.1,44 As integration of palliative care within paramedicine expands, research evaluating the efficacy of ongoing education, guidelines and frameworks is essential to improve clinician confidence in palliative care assessment, referrals, recognition of end-of-life and bereavement support.17,14,15 Moving forward, a 2024 Delphi study developed a 32-component framework to standardise practice for paramedics delivering unscheduled palliative care. 41 Our results may help to inform service-based guideline adaptations as well as implementation of this national framework.
Strengths, weaknesses and limitations
To our knowledge, this is the first study to evaluate an ambulance service statewide palliative care guideline through interrupted time series analysis.23,24 Analyses were based on monthly observations due to insufficient caseload to create weekly observations. Incorporation of a non-palliative care patient cohort for negative control was outside the scope of this study. Models were not adjusted for all environmental or community-level factors which may have influenced ambulance utilisation or treatment provided. Retrospective studies are inherently limited in their ability to demonstrate causality, as trends observed may have been confounded by environmental and patient characteristics not adjusted for in analysis. Changes in case-time and transport rates may have been confounded by broader healthcare system changes, for example, introduction of the Victorian Virtual Emergency Department, alternate service referral, ramping mitigation strategies and the COVID-19 pandemic.26,31,33,45,46 Our results are applicable in Victoria, and generalisability to other ambulance services may be limited by variations in palliative care guideline structure, content and scope. 22 The guideline itself limited the study scope as it was only applicable to patients already known to palliative care services, not to all who could benefit from a palliative approach. Further, this study was limited by paramedic ePCR documentation and available data extraction parameters. Despite comprising a large proportion of paramedic value-add for this patient cohort, non-technical skills are not currently documented in ePCRs.44,47
Conclusion
The introduction of an ambulance service palliative care guideline for patients who expressed a wish to stay at home was associated with an increase in non-transport rates, including among patients seen after-hours, and those with pain who received supportive medications. This enabled more patients to remain in their preferred place, decreasing avoidable transfers to emergency departments. However, there remains room for improvement in assessment of the safety and efficacy of patients remaining in place. Important opportunities exist for guideline optimisation, framework and tool development to enhance holistic patient assessment and paramedic-integrated community palliative care services.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251331167 – Supplemental material for Palliative paramedicine: An interrupted time series analysis of pre-hospital guideline efficacy
Supplemental material, sj-docx-1-pmj-10.1177_02692163251331167 for Palliative paramedicine: An interrupted time series analysis of pre-hospital guideline efficacy by Mostyn Gooley, Belinda Delardes, Sarah Hopkins, James Oswald, Cheryl Cameron and Emily Nehme in Palliative Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EN is supported by a National Health and Medical Research Council postgraduate scholarship. All other authors received no funding for the research, authorship, or publication of this article. An Australasian College of Paramedicine grant was received for dissemination of results.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.