
Abstract
Background:
Motor neurone disease is an incurable neurodegenerative condition that progressively impairs motor function. It affects mobility, speech, swallowing and breathing, leading to significant dependence on others. Home mechanical ventilation can alleviate respiratory symptoms and improve survival.
Aim:
To examine the experiences of bereaved family members involved in the care of someone with motor neurone disease who had died with home mechanical ventilation in place, or following its withdrawal.
Design:
An interpretive constructivist approach was used to carry out qualitative interviews.
Setting/participants:
Bereaved family members from England and Wales whose relative had died with ventilation in place, or after withdrawal.
Results:
Thirty-six bereaved family members took part. Their experiences highlight the extensive responsibilities and emotional burdens of managing home mechanical ventilation. Family members reported feelings of heightened responsibility, distrust in the abilities of professional caregivers, significant impacts on their mental and physical well-being and the ways in which knowledgeable care providers could lift such responsibilities.
Conclusions:
As the use of technology to sustain life increases, we need to question how much we expect of family members in providing care for those with complex interventions, such as ventilation, at home. This research underscores the critical role family members’ play in home care for people with motor neurone disease and calls for a greater understanding of the impacts of maintaining responsibility for life-sustaining treatments. There is a need for better support and training for both family and professional caregivers to alleviate some of the responsibility placed upon family members.
Keywords
The majority of people with long-term conditions, such as motor neurone disease, live at home
Advances in technology are now extending survival times and facilitating greater independence from in-patient care
Family members play a significant role in supporting people to live at home
Responsibility is a specific dimension of caring for family members
Responsibility for life-sustaining treatments can significantly add to feelings of stress and anxiety
Family members in such significant caring roles can be impacted long into bereavement
Assessment of family members in caring roles is essential to identify their needs and concerns so that these may be addressed as far as possible
We need to question the level of demand placed on family members
Training and investment in the homecare workforce is vital to sustain such models of community-based care
Background
Motor neurone disease, including Amyotrophic Lateral Sclerosis (ALS), is a progressive and incurable neurodegenerative condition that leads to the gradual loss of motor function, affecting mobility, speech, swallowing and breathing. As it advances, patients become increasingly dependent on others for activities of daily living. 1 For family members, the impact is multifaceted. They must cope with witnessing their loved one’s decline while simultaneously providing extensive physical assistance, managing complex medical needs and coordinating various aspects of care.2,3 This often requires significant adjustments to daily routines, work and living arrangements, as well as ongoing emotional support. 4
The home environment is widely recognised as the preferred place of care for patients. 5 In recent years, there has been a notable shift from institutions towards home care for people with increasingly complex and debilitating conditions.6 –8 This transition has been facilitated by advancements in management and technology. Feeding tubes, hoisting, medication regimes and home mechanical ventilation allow people to live at home for longer. 9 Consequently, patients and their family members are increasingly tasked with managing demanding care routines. Coping with the challenges of serious illness and navigating health and social care systems imposes significant burdens and responsibilities, yet family members play a crucial role in facilitating care at home.9 –11
There is a wealth of literature on the burdens of care both in motor neurone disease1,12 –14 and more broadly.9,15 Liu et al. 16 define family caregiver burden as ‘the level of multifaceted strain perceived by the caregiver from caring for a family member and/or loved one over time’. Aoun et al. 3 suggest we should advance the discussion beyond ‘burden’ by exploring palliative care interventions that support family caregivers. We propose the concept of responsibility develops this discussion by recognising it as distinct from burden. Responsibility is the caregiving duties and obligations that family caregivers undertake, often driven by a sense of duty, love and commitment to the well-being of the person they care for. Burden is the negative impacts and strains experienced by caregivers because of these responsibilities. However, as Pollock et al. state 11 there has been limited acknowledgement or understanding of the tasks undertaken by families, how they navigate the challenges of care at home or their views regarding the responsibilities involved in life-sustaining interventions such as ventilation, especially towards the end-of-life. This paper explores these responsibilities, as reported by bereaved family members. It does so in order to contribute to the advancement of the discussion on burden and provide evidence for the development of such interventions to support family members. 3 Findings in this paper focus on data from interviews with bereaved family members. These were part of a wider UK, qualitative study designed to explore end-of-life decision-making in relation to home mechanical ventilation in motor neurone disease. The study involved interviews with people with motor neurone disease dependent on their home mechanical ventilation, and their family members, including those bereaved. Broader findings are published elsewhere. 17
Study design and methods
Research objective
To examine the experiences of bereaved family members involved in the care of someone with motor neurone disease who had died with home mechanical ventilation in place, or following its withdrawal.
Study design
The study design drew on an interpretive constructionist approach to ethnographic, flexible interviewing. This approach focuses on understanding how individuals construct meaning through their interactions and experiences in specific contexts. It acknowledges that during the interview participants and the researcher collaborate to co-construct an understanding of the topic under investigation. 18 The approach emphasises that reality is socially constructed, subjective, and shaped by the participants’ cultural, historical and relational factors. Hence, the aim was to explore participants’ perspectives and meaning-making processes and to generate understanding by interpretation of the data. 19 The flexibility of this qualitative approach to interviews allowed the researcher to accommodate the needs of participants, encouraging them to choose the medium and timing of the interview.20 –22 By offering different options for undertaking the interview, we aimed to make the study as accessible as possible to all those who wanted to participate. 21
Population and sampling
Bereaved family members from across the UK were eligible if they had either experience of the person with motor neurone disease dying with ventilation in place or following its withdrawal. Participants were those who had been bereaved between the 31st December 2015 and at least 8 weeks prior to study involvement. All eligible bereaved family members could be selected for inclusion. See Box 1 for full details of inclusion criteria:
Study inclusion criteria.
Bereaved family members.
• Over 18 years old
• Have experienced the death of a family member (or friend) who used ventilation to alleviate the symptoms of motor neurone disease
• Bereavement took place since 2015 and at least 8 weeks prior to study involvement
• Willing to reflect on experience of death of their family members/friend and the role of ventilation
• Able and willing to use an online video conferencing tool, phone or email if in-person interaction is not feasible due to Covid-19
• Fluent in English
• Able to give informed consent
Recruitment
Study information was shared on social media, via patient and family support networks, the Motor Neurone Disease Association website and branch newsletters, as well as the Motor Neurone Disease Clinical Studies Group. There was also a study-specific website with the Participant Information Sheet publicly available. Participants either could self-refer to the study by contacting the researcher, or were approached by a clinician with whom they were familiar. Potential participants were provided with the Participant Information Sheet, with details to contact the researcher [EW] directly for more information or to take part. It is not possible to know how many people the public information reached, and due to work time constraints health professionals did not keep consistent records of how many family members they approached.
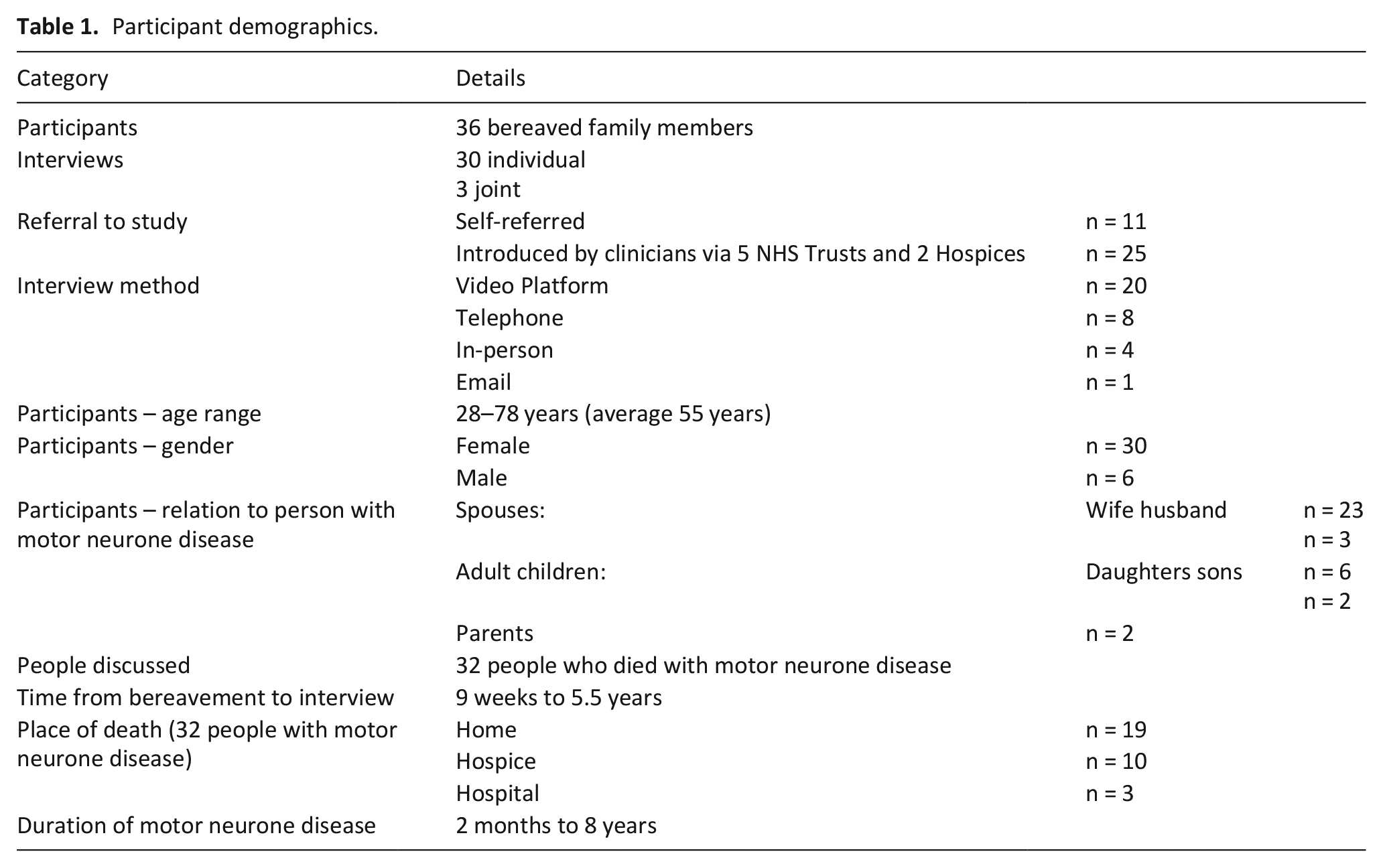
Any queries were answered before setting up a suitable time for an interview. Initially designed prior to Covid-19, we had expected the majority of interviews to take place in person, hence recruitment was restricted to the UK. The recruitment target was 35. Anticipating withdrawal of ventilation to be less prevalent, we aimed for approximately 20 bereaved family members of those who had died with ventilation in place and 15 where it had been withdrawn. In practice, in order to meet the overall sample target all those wishing to participate were recruited. This resulted in a more even spread between the two groups (please see Table 1 for participant details).
Participant demographics.
Data collection
EW conducted interviews via a video platform, telephone, email or in-person (once Covid-19 restrictions allowed) over a 2-year period (May 2021–23). EW is an experienced qualitative researcher, working on a research fellowship at the time of the study. She has expertise in conducting sensitive interviews and knowledge of motor neurone disease and end-of-life care. Consent was collected, primarily online, via Microsoft Forms© before starting the interview. However, a small number of participants chose to provide written consent, which was scanned and stored securely. Two people chose to have their verbal consent audio recorded. With permission, all interviews were audio recorded using an external digital device. An interview schedule, reviewed by the Project Advisory Group, was used to guide interviews, while allowing participants to express areas important to them.
Analysis
Interviews were between 40 and 126 min in length. Following each interview, summary notes were documented, and time was spent reflecting on the interview to improve questioning techniques and identify potential areas needing further investigation. After transcription and anonymisation of interviews, a thematic analysis was facilitated by managing transcripts in NVivo14©. Drawing on a constant comparison approach, interviews were read and initial inductive, open coding, undertaken by EW. 18 Transcripts were compared against each other and in conjunction with interview notes containing initial interpretations. To support this dynamic process, initial codes were reviewed, refined, and revised through reading and re-reading both transcripts and coded nodes to interpret meaning.18,23 This has ensured that the presented findings are founded in participants’ experiences, and rigour is enhanced by identifying shared and unique, perspectives within the data. Members of the Project Advisory Group read and commented on 10 (28%) of the transcripts, highlighting areas of interest and consistency. In online meetings held three times a year, emerging themes were presented and discussed. After each of these discussions, data were revisited to review and refine codes as needed. 18 Codes were then grouped into categories. Written summaries, memos and diagrams were utilised consistently to organise and delineate connections between categories and generate themes. 18 Themes were then arranged in a way that reflects their relationships and represents the data, creating a coherent narrative.
Ethics
The primary ethical concern in this study is the sensitivity of the topic. Engaging participants in discussions about end-of-life care and decisions can be emotionally challenging. However, previous research has shown that participants, including bereaved family members, often report positive experiences in qualitative studies of this nature, despite the subject’s difficulty.24 –26 This study was carefully designed to ensure a flexible and personalised approach to data collection, tailored to participants’ abilities, preferences and wishes. Research suggests that participants often appreciate the opportunity to share their experiences and may find participation beneficial.21,27
Participants were given as much time as they needed to consider the information about taking part in the study, and were asked to consider carefully how they might feel discussing issues relating to motor neurone disease, ventilation and end-of-life care before agreeing to take part. All were assured that participation was voluntary and that they could withdraw at any time, including during the interview. If at any point a participant became distressed, time was taken to establish whether the participants wished to continue at that time, at another time or to withdraw from the study. No participants chose to stop their interviews or to withdraw and many expressed thanks at having the opportunity to share their experiences.
Ethical approval for the study was granted by the Faculty of Medicine and Health Sciences, University of Nottingham ethics committee for non-NHS recruitment in February 2021 (REC ref: FMHS152-0121) and subsequently by London-Dulwich Research Ethics Committee for the NHS Health Research Authority in April 2021 (REC ref: 21/PR/0252).
Results
Thirty-six bereaved family members from across England and Wales took part in 30 individual, and three joint interviews, discussing 32 people who had died with motor neurone disease, either with their ventilation in place (n = 15) or after its withdrawal (n = 17). Table 1 provides further details of participants.
Pseudonyms have been used throughout the presentation of findings, and due to the relatively small population of participants and thus risk of potential identification, no further identifying data has been attributed to direct quotes. This is particularly important as the study generated data with complex narratives encompassing a diverse array of subjects. Findings on the themes of decision-making, 17 and the impact of ventilation on time and manner of death 28 are published elsewhere. This paper presents a key theme drawn from an extensive dataset exploring the experiences of caring for someone at the end-of-life and the use of ventilation as a complex life-sustaining intervention for motor neurone disease. Feelings of responsibility was a consistent theme through the data, expressed in a variety of ways, but always illuminating its significance to family members. We present this as the four sub-themes below: Family members’ responsibilities; distrust in the abilities of other carers; the impact of sustained responsibility; and lifting responsibility.
Family members’ responsibilities
Bereaved family members described a range of responsibilities, in particular how ventilation added to the responsibility of managing and maintaining complex treatments, alongside care organisation and coordination. Participants in this study spoke about people with motor neurone disease who were dependent on their ventilation to support their breathing. As such, many saw this life-sustaining treatment as intensifying responsibilities beyond that of feeding tubes, medications, and moving and handling tasks.
It was a bit daunting at first, just like ‘oh what do I do?’ . . . And it was like ‘oh gosh this is quite a big thing really’. I suppose it was the first obviously medical intervention that mum had, yeah she was in a wheelchair, yeah she had her feeding tube and things like that, but you could almost not notice those . . . And actually when you learn how to use it it’s really, really simple, but the initial idea of, this is like helping someone to live and I have to be in charge of it. (Olivia)
The majority of participants reported that they were given some instruction and demonstration of how to manage the ventilator and other equipment. However, for some this was brief and they felt they were ‘left to it’. Others praised the support they received from respiratory teams and described how ventilation could be monitored remotely, receiving telephone support and regular home visits. Those with more support seemed to express greater confidence in managing equipment but this did not necessarily lift the weight of responsibility.
It was a big responsibility because you think what if something goes wrong and you’re really thrown into the deep, like from within 10 seconds really. (Emma) To keep changing the mask and you knew you had to stop the machine, change the mask and wash his face a bit and try and put Vaseline and cream on to make him a bit more comfortable. Get the mask on and then just you, even though the machine would work, you just prayed to God that it would start again because you felt basically doing all this changing, it just panicked you because I felt so responsible . . . that’s the scariest bit . . .I felt I was turning off the piece of equipment that was really helping [him]. (Mary)
Responsibility for the ventilation was part of the complex roles bereaved family members reported, many also took considerable responsibility for co-ordinating care:
I was knackered from, coordinating his care, looking after him, fighting battles on his behalf with the [Primary Care Trust] about funding and, you know. We did direct payments so I employed nine carers and finding carers and dealing with all of their, like all the HR stuff for them. . . So there’s all that to deal with, plus two kids. (Lauren) Well I could see her getting more and more respiratory distressed at home, . . . she went for the breathing test. . . There was no follow-up, nobody acted on that, and then it got into October and I rang the nurses at the [hospital] again and said, look, we’re bordering on respiratory arrest here, you need to do something. I can remember at that time actually thinking, if I don’t make that call she’s just going to stop breathing and actually that could be a blessing in disguise, and I could just let her, go home and I could just ignore it, because nobody else is here to see and she could just actually go. Now I’m thinking, that wasn’t fair for me to even have that dilemma. I was in 50/50, every day I thought, do I make the call or do I just let her go? But I obviously made the call. (Elaine)
Further to the responsibility of managing and maintaining the ventilation, bereaved family members may also need to be involved in making choices about the use of ventilation at the end of their family member’s life. This occurred especially when the person with motor neurone disease had the lost ability to communicate and had not made, or conveyed, their own wishes around end-of-life and continuing or withdrawing ventilation. In these instances, decision-making was defaulted to close family members, as Jacky notes in her explanation of her husband’s death.
Interviewer: You mentioned that [his sister] was there on that final day. So, was she involved in that decision [to withdraw ventilation] at the end or? Jacky: No, she just said, I did ask her, she said it was down to me, so, yeah. (Jacky)
Even when withdrawal of ventilation had been discussed in advance, once the person with motor neurone disease was no longer able to confirm or consolidate that decision with health professionals, some family members felt the responsibility for the final decision.
The feeling of responsibility and being implicated in plans for [my husband’s] future in a way that I didn’t want to be, but knew that I had to be really, because there was no other way out. (Penny)
Distrust in the abilities of other carers
Participants’ feelings of responsibility for the complex care needed by their loved ones were often exacerbated by believing they could not rely on others. Bereaved family members expressed this as their own, or the person with motor neurone disease’s, distrust in the skills and abilities of homecare workers and other health professionals in the home. Subsequently, family members reported rarely taking breaks, being unwilling to leave the person with motor neurone disease alone with carers, and feeling they needed to watch over homecare workers.
They said it’s a specialist disease and really Hospice at Home or the hospice aren’t used to dealing with that sort of reality, that a lot of it was down to me. So I probably didn’t feel as though I couldn’t ask for help because I didn’t think they knew what they were doing. (Julia) Although we had carers, I was always in charge. . . .At the beginning it was ‘oh you can go out for a walk, you can go and see your friends for a coffee, you can do this’ - nothing, no break whatsoever. . . .No confidence. I would not have left him. No, would not have left him. (Elizabeth)
Even when the person with motor neurone disease was in hospital bereaved family members recounted feeling unable to hand over the responsibility of care, as staff were often unable to take this on. These feelings were compounded when staff demonstrated a lack of understanding of ventilation and /or motor neurone disease or when staffing levels were insufficient.
Because they said we couldn’t stay with him, and I said well are you going to tell me then, if anything happens to him because he can’t call you, because he can’t speak and he can’t push a bell for help, if anything happens to him I’m going to hold you responsible. And then they started letting us stay there. Just as well we did, because nobody ever come, even when we asked them to help. (Grace) They put [the mask] on, and he’d be like ‘oh [Susan] can you redo it’ when they left the room because he didn’t want to say to them but he just wasn’t comfortable really. And so, we would kind of worry about who was on shift as to whether they could fit his mask properly and things like that. (Susan) I was actually staying overnight with [him] and similarly in [local hospital] because he needed help with the ventilator and his feeding tube and things. So basically I was living with him 24 hours. (Lesley)
Impact of sustained responsibility
Some participants went on to express how sustained periods of caring and heightened responsibility had affected their mental and physical well-being. Often this was not fully recognised until sometime into their bereavement. Some recognised this as a trauma that continued to impact their lives:
. . .you’re really left alone with a lot of medication, you could kill the whole household if you wanted to. . . . You’re always anxious. You’re always anxious. It has changed me, it has changed me completely, because I can’t really tolerate much stress anymore. I get anxious if there’s any stress. (Emma)
Images and experiences of ventilation use at the end-of-life remained vivid for many participants:
But my son said you need to let him lie flat mum, and we did. But you see at the time you’re thinking you’re doing the right thing then, but then after you think ‘I’ve just killed my husband’. . . . the ventilation, but I can only say to you that I think people who deal with the ALS, the motor neurone disease, whatever you want to call it, I think you get a bit of post-traumatic stress, because you re-live all that’s gone on, and what they went through, and you question everything that you’ve done. (Connie)
A number of participants reported frequently reflecting on this, with some expressing gratitude for participation in this research to allow them to talk through these difficult thoughts.
I felt like I had failed, I couldn’t save him. Whether I reacted too late with the infection or maybe the suction killed him. I mean these things are with me all the time still. (Emma)
A few participants had been diagnosed with depression and were continuing to have treatment for this. Others identified symptoms that they likened to post-traumatic stress and considerable exhaustion after the death of their loved one.
Because you do get to, it does ruin your life. Because I had no life, I didn’t go anywhere. . . . I wouldn’t dare go away for the weekend or anything because I thought what if he dies?, if that happens in night-time? I will never forgive myself, I’ll be full of guilt. (Madeline)
Lifting responsibility
Some participants highlighted the importance of being relieved of this responsibility and how this might be achieved. This could be having trust in well-trained formal carers to take over the weight of the ventilation and care at the end-of-life. Hospices were sometimes noted for having staff with the right training to do this:
I was fortunate that they let me have a room at [hospice], so I was there 24 hours a day with her for the last week. But not having the responsibility of washing her but keeping an eye on her all the time. I felt that if there was something I, I was able to call the nurses and things like that and say look, and not having to worry about anything else but just be with her. That was very special in a way. (John)
As John notes, being allowed to relinquish this carer role is significant. Some family members felt being a caregiver had overtaken their primary relationship role as spouse, partner, child or parent.
Having comprehensive discussions about ventilation use at the end-of-life was seen as a way to reduce the weight of responsibility family members felt when having to make decisions. Knowing the wishes of the person with motor neurone disease and knowing that these had been communicated to the care team relieved family members from having to contribute to decisions made in their best interests.
[we discussed his choice to withdraw his ventilation] I think he felt better as well that, well because I was saying that and ‘it’s your decision’ which is my belief, I think he didn’t want me to have the responsibility of doing things if you can understand that. (Amy)
Discussion
Bereaved family members of those with motor neurone disease dependent on their ventilation to support their breathing reported feeling responsible for managing and maintaining this life sustaining treatment. Their role requires them to do this whilst undertaking and supporting activities of daily living for the person with motor neurone disease. Some did not feel they were given enough instruction on how to manage the ventilator and many, at least initially, found the responsibility of this to be daunting. This augments evidence that lack of information and training can contribute to burden for family members.2,29 Increased knowledge and experience with the machine helped to build confidence and reduce discomfort in undertaking tasks. 30
If the person with motor neurone disease could no longer participate in discussions, family members could be asked to contribute to decisions about continuing or withdrawing ventilation at the end-of-life. This placed them in the challenging position of having at least some responsibility over their family member’s death or continued living. This could be alleviated if the person with motor neurone disease had made, and effectively communicated to healthcare professionals, decisions about their ventilation use in advance so that this did not default to family members. 17
Evidence suggests that those caring for someone with motor neurone disease are at greater risk of having a more complex grieving process.31,32 This study has shown that increased levels of responsibility for managing life-sustaining treatments may add to negative caregiving experiences. Such heightened responsibility was considered extremely stressful at the time, with reported impacts long into bereavement. 33 This responsibility shapes additional roles for family members such as ‘decision-makers’, ‘care co-ordinators’ or ‘informal health surveillance officers’. Bereavement results in a loss of such newly adopted roles as well as existing roles as wife, husband, son and daughter, which could compound their loss. The effects reported in this study resonates with those cited in other studies focused on caring for someone at home at the end-of-life.11,34,35 Despite the complexity and strain of the experience, bereaved family members consistently report positive aspects about their overall caring journey. 36
Burdens of care were reported to be amplified when family members felt unable to entrust care responsibilities to others. Echoing the findings of O’Brien et al’s 2 interview study, bereaved family members often reported being unable to take breaks or have time away due to safety concerns when health professionals were not familiar with the use of ventilation or motor neurone disease. This is likely to have been compounded by the severe shortage of trained homecare workers in the UK and beyond.33,37,38 With no national guidance in place, little is known about the roles and responsibilities of homecare workers, particularly when complex interventions such as ventilation are in place.39,40 Future work on how to transfer some of these responsibilities to formal caregivers to alleviate the strain on family members would be of benefit in supporting family members and reducing family caregiver anxiety.
These data suggest that ventilation as a life-sustaining treatment can heighten the level of responsibility expected of, and experienced by, family caregivers. As such, this can increase the burdens of care and have impacts into bereavement. While responsibility can be demanding and challenging it is typically perceived as a natural and expected part of the caregiving role as perceived by both external agents and families themselves. However, as technology advances and patients’ needs become more complex we continue to see expectations for family member responsibilities expanded further. This is the first exploration of how the use of life-sustaining ventilation might compound burdens of care for those caring for loved ones with motor neurone disease at the end-of-life. It draws together arguments about the weight of responsibility family members endured and the impact of this on bereavement. This leads to questions about what it is reasonable to ask family members to do as part of their informal caregiving roles. 11 Family members are not paid, nor professionally trained and may have a limited understanding of the impact of ventilation on the dying process. 17
Implications for practice
It is essential to understand the differences between the concepts of responsibility and burden to enable the provision of support and interventions that address caregivers’ needs effectively while mitigating the burdens they experience. More consistent and broad use of tools such as the Carers Support Needs Assessment Tool (CSNAT https://csnat.org/), which has now been adapted for use with MND 41 could support professionals to explore the needs of caregivers and identify ways to meet those needs. Advancing AI also provides ongoing potential in multiple areas, such as 24 h Chatbots to support family caregivers, improved communication tools for those with motor neurone disease, monitoring the environment and smart household appliances to support meal times and reduce labour inputs.
Strengths and limitations
The substantial sample size for this cohort of the motor neurone disease population is of benefit to the study. The option to self-refer to the study and that a third of recruited participants engaged with this option suggests there was interest in the study and confirms the suitability of the inquiry. We recognise that gathering data via different mediums may have affected the nature and fullness of that data. The broad timescale from bereavement to interview may have influenced recall, but we suggest that for this study the level of engagement in care and the impact of this on the family meant that its significance remained vivid despite the passage of time. Bereaved family members were within the anticipated age range, with the inclusion of some adult children slightly widening the range. The study has a high proportion of female caregivers; this is in line with the caregiver population 10 and the heightened prevalence of motor neurone disease in males. It was not feasible to sample for diversity in any way due to the small population of potential participants. Although a few participants commented on their religious beliefs, data were not routinely gathered on ethnicity or religion. We note that this may have impact on responses in relation to cultural values around responsibility. However, given the nature and sensitivities of the study, we were cautious not to include a full range of demographic questions alongside the interview in this instance. While the primary goal of this research was to generate insights and establish a foundational understanding, we recognise it would be beneficial to record diversity information in future studies.
Conclusion
This study highlights the significant responsibilities placed on bereaved family members caring for individuals with motor neurone disease dependent on ventilation. Family caregivers often reported feeling unprepared and inadequately trained to manage this life-sustaining treatment, which added considerable stress to their caregiving roles. The burden of making critical end-of-life decisions about ventilation use further complicated their responsibilities, potentially exacerbating the grieving process. The lack of trained homecare workers and the inability to delegate responsibilities compounded the strain, reflecting broader systemic issues in UK healthcare support. Understanding the distinction between responsibility and burden is crucial for developing interventions that effectively address the needs of family members while mitigating the long-term impacts on their well-being. With technological advancement improving mortality, it is becoming increasingly important to re-evaluate what is reasonable to expect from family members and our current health and social care services. Currently, this research underscores the need for better support mechanisms, including comprehensive training for family members and the integration of formal caregivers to alleviate some of their responsibilities. Looking forward, we must consider the growing impact of life-sustaining treatment on end-of-life care and how new technologies may be utilised to support family members in their ever-growing care roles.
Footnotes
Acknowledgements
We thank all the participants who so willingly gave their time and shared their experiences. We acknowledge all of the clinical teams who supported the study throughout, particularly for their efforts in recruitment, clinical knowledge and discussion of the findings. In addition to the authors, these include: Dr. Ben Messer, Alison Armstrong, Dr. Edward Presswood, Alice Richards, Louise Dudley, Dr. Emma Husbands, Professor Christopher McDermott, Dr Ester Hobson, Dr. Thomas Lambert. We would also like to thank the Motor Neurone Disease Association UK for their support and for sharing information about the study with their members and on their website.
Author contributions
The study has been undertaken as part of EW’s Fellowship. EW undertook all study management, data collection and analysis. CF, JP, GK and JSL were involved in recruitment to the study and contributed to data analysis and interpretation. All have been involved in drafting the article and revising it critically for important intellectual content. EW, CF, JP and GK also contributed to the study design.
Data management and sharing
The data generated and analysed during the study are not publicly available. Data sharing was not included in the ethical approval as the study involves personal accounts of families’ experiences, much of which are extremely sensitive. It is essential that we maintain confidentiality and anonymity but sufficiently anonymised parts of the data are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded as part of Dr. Eleanor Wilson’s University of Nottingham, Anne McLaren Research Fellowship.
Research ethics and participant consent
Ethical approval for the study was granted by the Faculty of Medicine and Health Sciences, University of Nottingham ethics committee for non-NHS recruitment in February 2021 (REC ref: FMHS152-0121) and subsequently by London-Dulwich Research Ethics Committee for the NHS Health Research Authority in April 2021 (REC ref: 21/PR/0252). R&D approvals for each NHS Trust were also acquired. Informed consent was gained from all participants to undertake interviews.