
Abstract
Background:
Integrated multidisciplinary care is required to manage the progressive and debilitating symptoms associated with motor neurone disease. Professionals can find providing the level of care required by this population clinically and emotionally challenging. To support those working with these patients it is important to understand the experience of the entire multidisciplinary team involved and the impact of working with motor neurone disease on their emotional and psychological well-being.
Aim:
To identify what is known about (1) healthcare professionals’ experience of working with motor neurone disease and (2) the impact of this work on their emotional and psychological well-being.
Design:
Scoping review. Review protocol registered on Open Science Framework.
Sources:
Five electronic databases were searched in January 2023 and 2024. Grey literature and hand searches were completed.
Results:
Fifty-one sources published between 1990 and 2023 were included. A total of 1692 healthcare professionals are represented. Three main categories were identified: (1) The demands of providing motor neurone disease care. (2) Factors influencing professionals’ ability to provide desired levels of care. (3) The emotional impact of working with motor neurone disease. Subcategories are depicted within these.
Conclusion:
Positive experiences included job satisfaction, enhanced perspective and receiving gratitude, while negative implications such as stress, emotional exhaustion and burnout also featured. The demands of motor neurone disease patient care, the organisation of services and resources required to meet patient and family needs and the emotional burden for professionals involved, warrant greater recognition in clinical practice, guidelines and future research.
Keywords
Integrated multidisciplinary care, provided by an extensive multidisciplinary team is recommended to manage many progressive symptoms and to optimise quality of life for people living with motor neurone disease.
Professionals can find providing the level of care required and interactions with these patients and families both clinically and emotionally challenging.
Literature on the experience and impact of working with motor neurone disease from perspective of all healthcare professionals involved has not been systematically reviewed.
Motor neurone disease care can be experienced as intensive, distinctive and more time-sensitive than the care required by patients with other life limiting conditions.
Professionals have experienced emotional exhaustion, burden, frustration, anxiety, stress and burnout due to caregiving for motor neurone disease patients and their families.
The benefits of working with motor neurone disease are job satisfaction, receiving gratitude and enhanced appreciation for one’s own personal life.
External and organisational factors often perceived as outside of professionals control can limit their ability to provide desired levels of care, often resulting in feelings of stress and frustration.
Multidisciplinary care is not only necessary to meet the multiple needs of patients and informal caregivers but is also an important source of emotional support for professionals working with motor neurone disease.
The emotional burden for professionals working with motor neurone disease patients and their families should be recognised. Future research should focus on directly addressing and measuring the psychological health and well-being of professionals involved in providing this care.
The organisation of motor neurone disease patient services and processes for interservice communication and collaboration should be considered to reduce many of the external demands and associated stressors for professional care teams.
Professionals working with motor neurone disease patients should have access to collegial and multidisciplinary team support, future work should consider what additional supports, interventions or training could help to reduce the professional stress and emotional toll associated with working with this complex condition.
Future work should consider both the individual and shared needs for support of the different teams and professionals involved in providing motor neurone disease patient care.
Introduction
Motor neurone disease is a group of rapidly progressive neurodegenerative diseases, 1 of which amyotrophic lateral sclerosis is most prevalent. These terms are often used interchangeably, but in this review motor neurone disease will define the condition. Motor neurone disease is a terminal disease, with an average life expectancy of 1–4 years from diagnosis. 2 Current treatment focuses on managing associated symptoms and optimising quality of life, 3 using a multidisciplinary approach to care.4 –7 Multidisciplinary care should be delivered by a specialist team, in collaboration with community, hospital and palliative care services.4 –6
Much of the research on the delivery of multidisciplinary care has focussed on the views, experiences and needs of patients and informal caregivers’.8 –10 Patients and informal carers recognise and value high quality multidisciplinary care. 11 However, they have experienced services as being fragmented, 12 encountered healthcare providers with limited knowledge and understanding of motor neurone disease symptoms,9,13 received poorly communicated and conflicting information 14 and experienced difficulty accessing home care, respite, palliative care and specialist services.8,9,15 As the disease progresses increasing dependency and the level of care required have also been associated with high levels of burden, 16 emotional distress 17 and reduced psychological well-being 18 for patients and informal caregivers. The physical and emotional strain of informal caregiving is recognised in best practice and clinical management guidelines.4 –7
Informal caregivers provide most of the home-based care, 19 but depend on an integrated team of professionals for support with the patients and their own physical, psychological and social needs.10,20 Despite the level of support and care provided by professional care teams, in often clinically and emotionally difficult circumstances, the impact of this work on the their own well-being has not been widely considered in research to date. 21 The New Zealand best practice recommendations are the only guideline briefly referencing the clinical and emotional challenges faced by healthcare professionals. 7 To augment our understanding of the challenges to providing effective multidisciplinary care, that meets the needs and expectations of patients and their informal support network, it is important to consider the experiences and perspectives of the professional care providers. Some studies have addressed the challenges of professional caregiving for specific groups of professionals such as doctors, 22 nurses23,24 or primary care teams 25 and in specific circumstances such as supporting the withdrawal of non-invasive ventilation 26 or communicating the diagnosis. 14 However, this research has not been systematically reviewed to date.
This scoping review aims to identify healthcare professionals’ experiences of working with this complex and progressive condition and determine what is currently known about the impact of working with motor neurone disease on the emotional and psychological well-being of all healthcare professionals involved. This review also aims to identify areas for important future research on this topic.
Design
This review is based on guidance from Arksey and O’Malley, 27 Levac et al. 28 and The Joanna Briggs Institute. 29 An a priori review Protocol is registered on Open Science Framework (https://osf.io/gkjme), and was followed throughout the review process.
Eligibility criteria
Development of the selection criteria (Table 1) was guided by the Population, Concept and Context (PCC) framework. 29 and determined the parameters of sources for inclusion.
Selection criteria.
In this review the term ‘professionals’ will be used to define the population.
Search strategy
Five electronic databases; Embase, Medline, Cinahl, PsychINFO and Web of Science were systematically searched in January 2023 and January 2024. The search strategy was developed with assistance from a medical librarian (DM), using keywords for ‘motor neurone disease’, ‘multidisciplinary care’, ‘healthcare service’, ‘healthcare professionals’ and ‘experience’ or ‘perspectives’. See Supplemental Material for an example of one complete search strategy. All original study designs were included. Review articles were excluded but any relevant original studies within identified reviews were included. There was no limitation on year of publication, but sources were limited to the English language. In addition, grey literature was searched (Open Grey, ProQuest Dissertations and Google Scholar) using combinations of key words from database searching. MW completed a hand search in the reference list of each source selected for inclusion and in all review articles identified.
Data screening
All citations were exported to Covidence digital review management software, 30 for screening and data management. The lead reviewer (MW) screened all texts by title and abstract. Full texts were retrieved, read and reviewed by MW and cross-checked by the second reviewer (AC). Any disagreements were discussed, and when consensus could not be reached the third reviewer (MG) was consulted.
Data extraction
The data extraction tool was developed at the Protocol stage and pilot tested by the research team (Supplemental Material 2). The lead reviewer (MW) extracted; (1) study title, (2) author(s), (3) year of publication, (4) country of publication, (5) study design, (6) number of healthcare professional participants, (7) participants profession(s) (8) healthcare setting participants worked in, (9) experience of providing care as described by the professional and (10) any emotional or psychological response described or potential impact on their health or well-being.
Data analysis
As guided by Levac et al. 28 the characteristics of included sources were analysed using descriptive statistics in Microsoft Excel and qualitative data were analysed using conventional content analysis. 31 Qualitative data were imported to NVivo 12 32 for coding and categorisation, codes were derived directly from the data and sorted into categories and sub-categories to answer the review question. Methodological rigour of included sources was not assessed, as was not relevant to the aim of this review. 28 Findings are reported descriptively, in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews 33 (PRISMA-ScR; Supplemental Material 3).
Results
Results from the search strategy and selection process
The PRISMA diagram 34 (Figure 1) outlines the study selection process. A total of 1258 citations were identified from electronic databases (January 2023 and 2024). After duplicates were removed, 770 sources were excluded by title and abstract screening. 13 texts were identified from hand searching in the reference lists of included sources and 7 from the grey literature search. 142 full texts were reviewed and cross-checked, of these 51 met the inclusion criteria. Reasons for full text exclusion are reported in Figure 1.
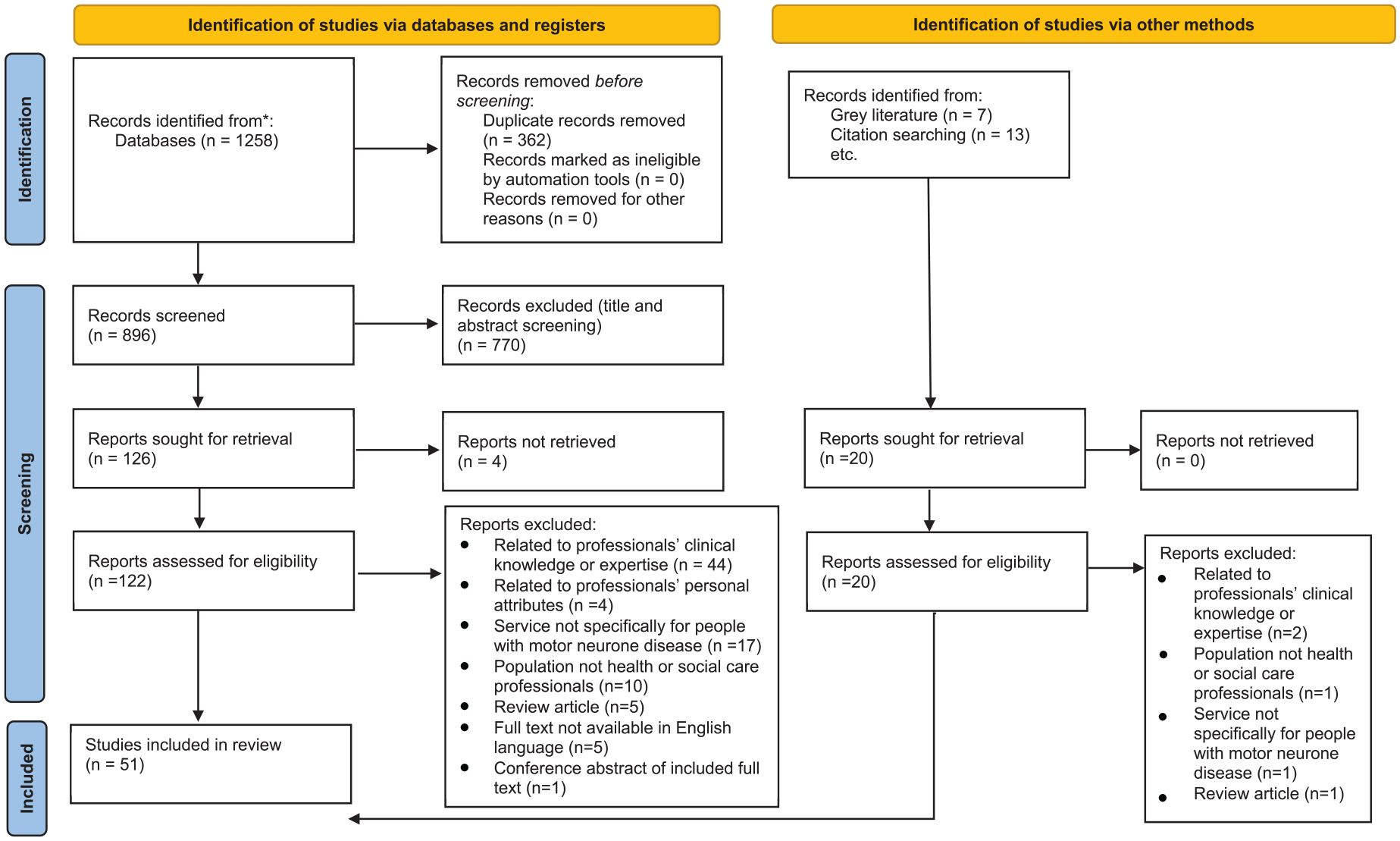
Preferred reporting items for systematic reviews and meta-analysis (PRISMA) diagram. 34
Characteristics of included sources
Fifty-one sources were included in the review, of which n = 42 (82%) used qualitative, n = 4 (8%) quantitative and n = 5 (10%) a combination of both methods. European countries were most represented (n = 31), however there was wide global representation: USA (n = 9), Australia and New Zealand (n = 8), South America (n = 2), Canada (n = 3), Asia (n = 2) and South Africa (n = 1). Included sources were published between 1990 and 2023. An increase in interest on this topic was observed over time with n = 16 (31%) of all included sources published between 2021 and 2023. See all characteristics of included sources in Table 2.
Characteristics and summary of data extracted from sources included in the scoping review.

Healthcare professionals represented
A total of 1692 professionals are represented from 15 different professional backgrounds (Figure 2). Medical n = 558 (33%) and nursing n = 537 (32%) professionals are more highly represented than allied health or social care professionals n = 310 (18%) combined. Profession or discipline was not reported for n = 288 (17%).
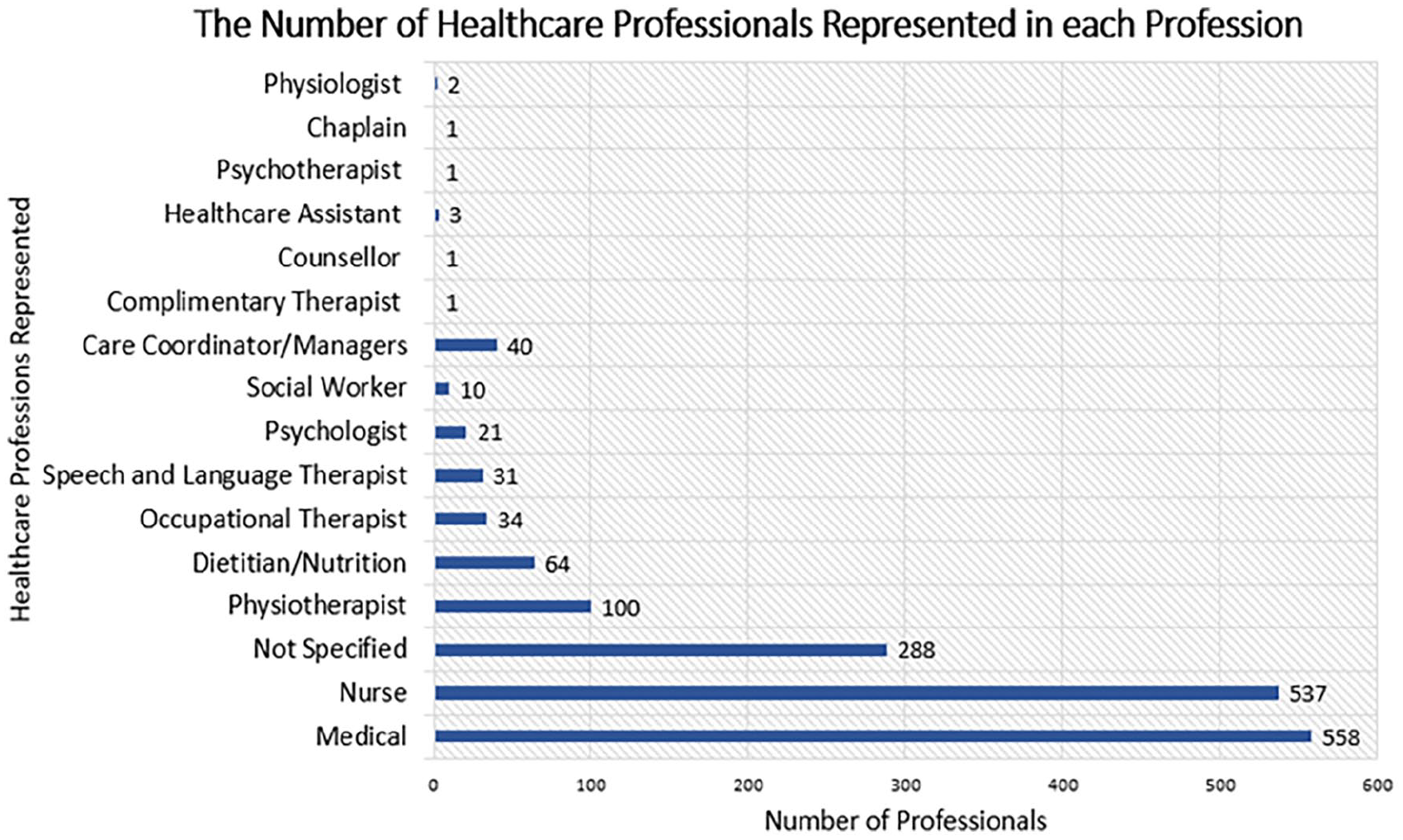
The number of healthcare professionals within each of the represented professions.
Healthcare settings
Professionals were working in six main healthcare settings. Hospice and palliative care were most highly represented (n = 20) followed by community/primary care (n = 18), hospital (n = 17) and specialist multidisciplinary team clinics (n = 15). Voluntary organisations (n = 4) and residential care facilities (n = 2) were least frequently represented. The majority of sources n = 32 (63%) recruited professionals from a single setting and only n = 10 (19%) recruited professionals from three or more different settings.
Results from the qualitative synthesis
Three main categories were generated: (1) The demands of providing motor neurone disease care (2) factors influencing professionals’ ability to provide desired levels of care (3) The emotional impact of working with motor neurone disease. Sub-categories are depicted within each of these (Figure 3).
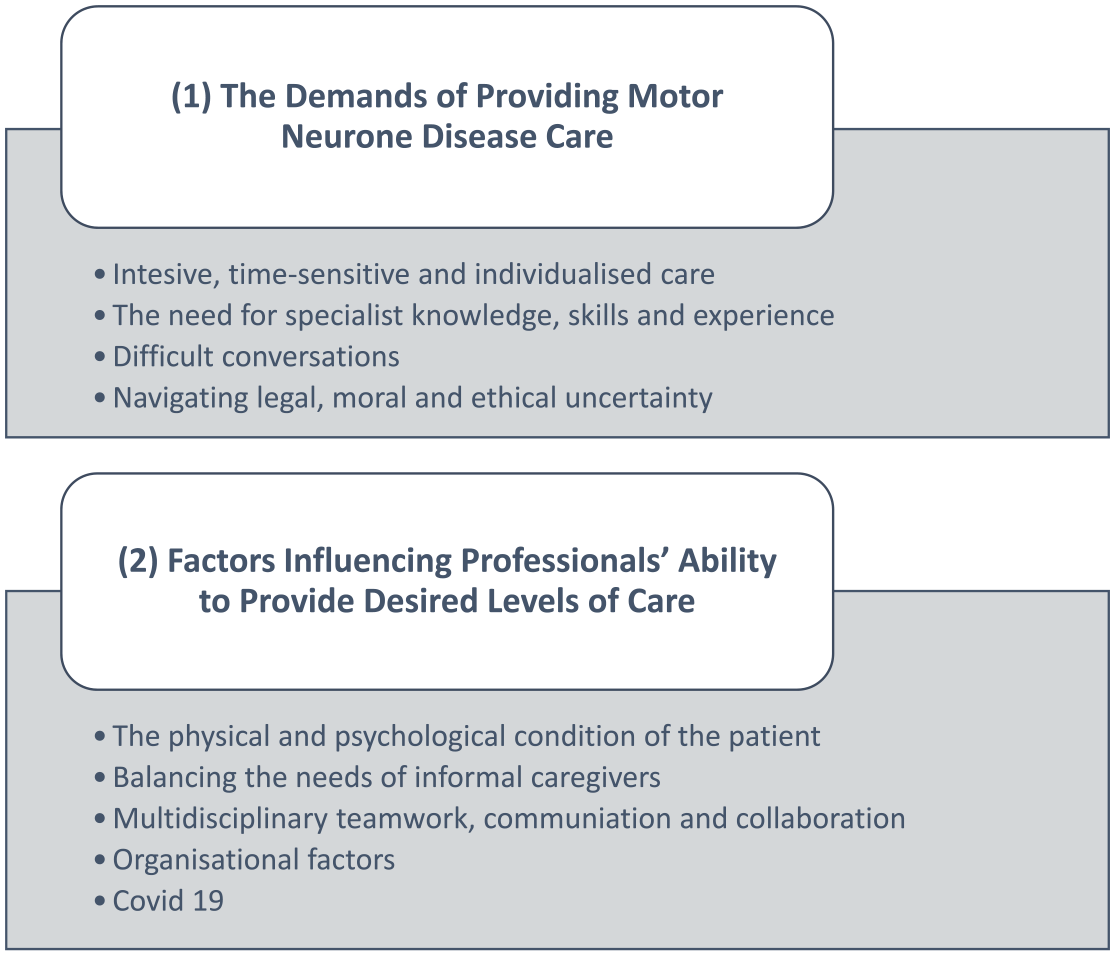
Overview of categories one and two and the sub-categories within each main category.
The demands of providing motor neurone disease care
Intensive, time-sensitive and individualised care
Providing care for people living with motor neurone disease and their families required exceptional multidisciplinary team effort.23,25,58,64 Professionals described going above their ‘usual practice’ or ‘typical role’ to meet the complexity and extent of patient care needs.13,23,37,38,44,55,56 Their care was described as distinctive and often prioritised over patients with other conditions.13,24,25,39 Some professionals were described as committed and passionate,61,65,77 while others avoided working with this population due to the perceived complexity. 25 Nurses particularly described the intensity of care as physically and mentally exhausting and the associated workload as limiting their capacity to care for other patients.43,61,78 In one source the unequal time nurses had to give to those with motor neurone disease, over others in their care, caused them ‘ethical discomfort’ and they felt that reduced patient-to-nurse ratios were required to provide safe and quality care for these patients. 78
The continuous, heterogeneous, unpredictable and often rapid nature of disease progression is a unique feature of motor neurone disease, that contributed to professionals feeling under ‘time pressure’ and ‘working within windows of opportunity’.13,24,35,37,39,51,57,60,65,66,72 –74 Professionals in many sources reported having inadequate time to address all the clinical needs motor neurone disease patients presented with.14,22,24,26,35,37,39,43,49,54 –56,58,60 –62,65,76 Professionals could feel overwhelmed by the multitude of clinical problems40,43 and perceived the duration of standard appointments as insufficient to adequately address all identified issues.62,65 Homecare nurses in one source felt able to provide adequate person-centred care, because of additional time available to them. 72
Interventions and care needed to be individualised for each patient and family.35,37,39,49,56,67,75,77 Developing relationships with patients and families was important to understand their needs and priorities and facilitate an individualised approach to their care.23,25,37,65,78 Professionals expressed concerns about quality of care in the absence of a patient-provider relationship. 25 However, they acknowledged that developing and sustaining relationships with these patients and families required emotional effort and adjusting their demeanour and approach for each individual situation was challenging. 37
The need for specialist knowledge, skills and experience
Having up to date knowledge about the condition and available treatments was essential37,39,42,60,66 as patients hope for a cure, meant they often sought information from multiple sources
51
and were interested in ongoing research.
53
Keeping up to date with evidence and the availability of services was difficult for professionals who provided this care infrequently.37,39,66 One General Practitioner stated:
the clients with MND usually know about them [treatments] before us. . . you know they’re on the internet.
39
Professionals who specialised in motor neurone disease care valued having specific and profound knowledge, 40 while access to expert knowledge was important to those who encountered the condition less frequently.24,60
In many sources, professionals acknowledged their limitations in having the required skills and experience to confidently provide motor neurone disease care.37,39,45,56,60,62,66 Nurses reported needing to draw on all their nursing skills to meet the associated challenges.39,46 In one source, professionals felt significantly less confident managing patients with motor neurone disease than those with a less progressive neurological condition. 42 Lack of confidence with the use of medical equipment, assistive devices and technology commonly used by these patients was also discussed.25,54,60
Some felt that previous experience allowed them to provide greater hope and optimism for motor neurone disease patients and their families. They felt able to talk about what could be done to manage symptoms and offer solutions rather than just seeing barriers.42,60 More years of experience was related to lower levels of stress for doctors and clinic managers in one source, 22 while neurologists who were not experiencing burnout were working with motor neurone disease for longer than those experiencing burnout in another. 77 Many professionals felt that most of what they learned about providing motor neurone disease care was through their prior clinical experiences37,56,65,77; others felt that previous experience did not necessarily help with the most challenging aspects, such as end-of-life care conversations. 35
Difficult conversations
In one source 65% of neurologists reported ‘moderate-high’ levels of stress and anxiety on delivering the diagnosis and 43% reported finding it ‘very – somewhat’ difficult responding to patients’ emotional reaction to the diagnosis. 36 Neurologists in another source reported this to be the most emotionally challenging aspect of their job and that delivering more than three diagnoses in a day, could leave them emotionally and physically exhausted. 77 73% struggled to reveal the diagnosis to a patient they personally identified with because of a demographic similarity such as age, gender, family composition or career; one neurologist reported ‘having a migraine after each MND clinic and feeling stressed and anxious about having so little to offer’. 36 In multiple sources, professionals struggled because of the lack of a cure for this disease.36,42,53,60,77
Eight sources discussed the dilemma professionals faced when determining the appropriate time to introduce conversations about advanced care planning, palliative or end-of-life care.26,35,44,48,49,51,57,76 Professionals aimed to start these conversations early, recognising that skilled communication and good clinical judgement was required to determine the appropriate time for each individual.38,44,49,51,57,76,80 This involved considering factors such as the rate of disease progression, social factors, coping and acceptance and challenged even those experienced in delivering motor neurone disease care. 49 Professionals found it difficult to provide honest information without taking away the person’s sense of hope or optimism.14,42,51,77 They feared causing additional distress and wanted to avoid ‘piling on the bad news’.24,63
Conversations about end-of-life could be uncomfortable, overwhelming and, sometimes avoided by professionals,24,26,52 with some families wanting to discuss issues such as euthanasia and physician assisted suicide. 55 Professionals experienced anxiety about engaging patients in conversations about advance care planning when they were still relatively well. 50 Being comfortable talking about end-of-life 39 and having a positive perspective on working with death was considered helpful, but difficult, for most. 40 Professionals perceived that a big part of their job was often ‘to be present without intervening’ 40 , ‘to be a listener 37 ’, ‘simply allowing them to be sad’ 40 or ‘taking on the burden of grief’.24,37,77 Those working in specific palliative care positions were more comfortable with difficult conversations about signs of deteriorating health, than those without palliative care experience.24,42,58
Navigating legal, moral and ethical uncertainty
Legal, moral and ethical dilemmas were frequently described in relation to decision making, planning, communicating and managing end-of-life care.24,26,50,55,56,58,64,74,76 The withdrawal of non-invasive ventilation raised significant legal, moral and ethical concerns for professionals involved in this process.26,55,56,58 The legal and ethical complexity was compounded when the underlying reason for the patient requesting ventilation withdrawal was their wish to die, rather than the removal of burdensome treatment.55,56 Several sources also discussed the ethical dilemma professionals faced between respecting patient autonomy and beneficence.43,44,59,60,64,74 Circumstances were described when professionals were faced with complex ethical dilemmas between supporting patient wishes and ensuring their own, the patients or informal caregivers’ safety or welfare.43,60,74
Factors influencing professionals’ ability to provide desired levels of care
The physical and psychological condition of the patient
The rate of disease progression could impact the quality of care provided.26,57,65,72,74 Professionals described situations when the patient’s condition changed more rapidly or abruptly than expected, rendering current supportive measures immediately ineffective.57,66 Professionals were required to respond rapidly to what were described as ‘crisis’ situations.39,51 With a slower rate of progression, the need for assistive devices, home care services and other supports were less acute and professionals had time to effectively plan and support implementation. 72 Professionals highlighted the need to take a proactive or anticipatory approach to deliver good care for these patients.39,44,48,49,51,65,70,75 They aimed to stay ‘one step ahead’ by anticipating, planning and preparing for interventions before they were required39,44,49,51 and described how situations could spiral into ‘chaos’ when professionals were unprepared or uncertain about the trajectory of deterioration.25,35,39
Patient psychological adjustment and coping was discussed in 13 sources.13,24,25,35,42,46,49 –51,65,66,72,76 Acceptance13,49,51,65,75 and denial24,25,35,49,51,66 were raised as enablers and barriers to the level of care that could be provided. How patients adjusted to the diagnosis or deterioration in their condition influenced when interventions were provided. Patient and family acceptance of the diagnosis could influence clinician’s stress levels. 44 Patients with some degree of acceptance of their condition, were perceived as more open to discussions, engaged in decision making and pro-active in managing their symptoms.49,66
The ‘need for control’ could vary between patients, for some it manifested as taking control of managing their condition while for others it was exerted as avoidance or disengagement. 66 Professionals encountered patients who were in denial or shock at the terminal nature of the diagnosis and avoided engaging with services. This was frustrating, as it significantly limited their ability to deliver what was perceived as good anticipatory care.51,62,76
Professionals found it challenging to manage cognitive and behavioural symptoms motor neurone disease patients presented with.62,77 Cognitive and behavioural changes impacted patients’ understanding of information and the quality and timing of their healthcare decision making.35,51,61,63,65,77 It also impacted their ability to use aids and devices such as high-tech communication aids and powered wheelchairs.61,63 Professionals felt that patients who received cognitive and behavioural screening, received better clinical care, as their difficulties were identified and validated;51,63 without routine cognitive screening, mild cognitive changes were not always identified. 51 Professionals felt that more specific and detailed knowledge of these symptoms could improve their approach with these patients. 51
Presence of communication impairments presented particular challenges.23,24,39,42,73 Professionals highlighted that having knowledge of communication devices and how to effectively use them was essential to provide good care39,73 and that training for professionals on how to use these devices should be addressed. 73 Understanding patient’s wishes, ensuring they were appropriately included in discussions and respecting their autonomy was challenging when communication was a problem.24,26,55,73,74
Balancing the needs of informal caregivers
Professionals recognised the important role of informal carers and the exhausting level of care they provided.37,39,74,78 ‘The heavy care burden brought the family to the verge of ruin’. 74 Professionals reported difficulty assessing how much strain the family could manage 25 and providing emotional support and hope, in the face of deteriorating illness.60,78 They were exposed to ‘a lot of tears, frustrations and helplessness’ 60 and found it ‘awful to look at’ 25 the emotional distress and burden family members experienced. 78 Some felt pressured for time or lacked knowledge about how best to support families.60,78
It was important for professionals to develop good relationships with family caregivers as in many cases they were the conduit between the patient and the care team.24,39,78 Professionals described collaboration with families as a balancing act and often encountered dilemmas and family dynamics.24,49,51,52,60,74,77,78 Lack of concordance between the wishes of the patient and their family made things more difficult for the team supporting them.
49
Decision making was challenging when the patient and their family could not reach agreement, patient’s decision-making placed family members at risk,51,78 or family members engaged in activities that were deemed unsafe for the patient.
81
Professionals were required to take both sides into account:
I don’t think you can only talk to the person with ALS and find out just what they want, because what their carer wants might be totally different. . . The client might say I want to stay at home, it’s the only thing I want to do’, and the partner might be going ‘there is no way I can handle physically their behaviours’. So, you’ve got to take both into consideration
51
Multidisciplinary teamwork, communication and collaboration
Managing the complex needs of motor neurone disease patients and their families, required a large team and a union of authorities, teams and professionals.39,60 Co-ordinating the number of people involved was a frequently cited challenge.39,51,60,74,76 There could be uncertainty about who’s role it was to co-ordinate patient care or the clinician responsible for initiating certain discussions or interventions.26,35,62,76 Professionals counteracting or duplicating each other’s work was experienced when ‘one side doesn’t know what the other is doing’. 39 Feelings of frustration and powerlessness were experienced by professionals working with external teams who did not assign the same level of priority to motor neurone disease care, 40 or refused to provide a service, due to the perceived level of complexity.25,40,60 The need for better communication and transfer of information between the teams and services involved was identified.13,35,39,76
The value of multidisciplinary team working, and strong professional relationships was discussed in 21 sources.23,24,26,37,40 –42,51,52,55,56,58 –60,69,72,73,76 –79 Six sources described challenges when there were differences of opinion about how care be provided within the healthcare team.26,52,55,56,62,74 Effective teamworking was important for professionals and contributed to their job satisfaction.40,79 When professionals worked in what they perceived as a well-functioning multidisciplinary team, they felt enabled to deliver effective support and care for patients and their families.52,60,69 Professionals also recognised the emotional support they received from working within a strong multidisciplinary model of care.23,40,41,52,55,59,77,78 Professionals reported that collegial support was invaluable in helping them to process ‘heavy’ thoughts and emotions that arose from the difficult situations they were faced with when working with these patients. 40 In the absence of team support professionals reported feeling overwhelmed, 43 vulnerable 56 and isolated 25 when faced with making decisions or providing care alone. This was particularly relevant for nurses and healthcare assistants providing care in patient’s homes.25,43,78
Organisational factors
Ten sources referenced lack of personnel or high rates of staff turnover as a problem for delivering consistent and high-quality care.22,24,25,37,43,62,63,65,67,77 29% of neurologists and 34% of motor neurone disease clinic managers in one source considered leaving their position due to stress or financial issues. 22 High rates of turnover resulted in inconsistent team composition and prevented important aspects of care from being delivered,25,43,62,63,65,67 for example, lack of neuropsychologists prevented routine cognitive assessment in multidisciplinary clinics. 63
It could be challenging to recruit professionals to work with motor neurone disease patients, as ‘people avoided’ working with this patient group. High levels of turnover made it challenging to develop professionals’ expertise and retain professionals with the required level of competency to meet the demands of motor neurone disease patient care. 25 With low staff turnover, professionals established a connection with their patients that allowed them to gather sensitive and personal information about their care preferences. This was considered essential to provide good person-centred care. 25
Availability of finances, resources, access to services and assistive devices were identified as barriers by professionals in 14 sources.22,25,37,42,43,46,53,58,62,65,67,70,71,77 Geographical variation in funding and services available impacted equitable service delivery.62,65,70 Professionals identified that standard pathways for accessing services and medical devices were inappropriate for these patients.51,53 Long delays with administration and obtaining financial approval was more problematic for this population than other less quickly progressing diseases. 53 A number of sources discussed how bureaucratic processes resulted in patients receiving necessary medical aids or devices after the disease had further progressed and the device was no longer suitable.25,37,46,51,53,70,71,51 Professionals found this stressful, 51 while organisational factors such as being understaffed and institutional demands contributed to others experiencing burnout. 77
Covid 19
Healthcare professionals’ experiences of delivering motor neurone disease care for patients during the COVID-19 pandemic was discussed in three sources from 2020 to 2022.64,68,69 Enforcing visiting restrictions was described as causing ‘palpable distress’ and ‘emotional devastation’ for members of a palliative care team involved in the care of a young lady with motor neurone disease. This case was identified as an ‘exceptional case’ and ‘ethically challenging’ for the staff involved, due to the patient’s motor neurone disease associated communication impairment. She could not use technology to engage with her family, as others could and staff viewed the restrictions imposed as ‘wrong on so many levels’. 64
Specialists’ ability to carry out important assessments, such as the physical examination required to confirm the diagnosis and spirometry testing, one of the key assessments for monitoring disease progression could not be completed virtually. 68 Professionals reported feeling concerned about missing important clinical details and the impact of this on the patient’s quality-of-life and survival. 69 Professionals also experienced delayed access to key services including gastrostomy insertion, provision of wheelchairs and home help and hospice services being unavailable at certain times. 68 Professionals described how they developed new models of service delivery to overcome many of these challenges, but some expressed reduced confidence in their ability to deliver optimal care during this time. 69
The emotional impact of working with motor neurone disease
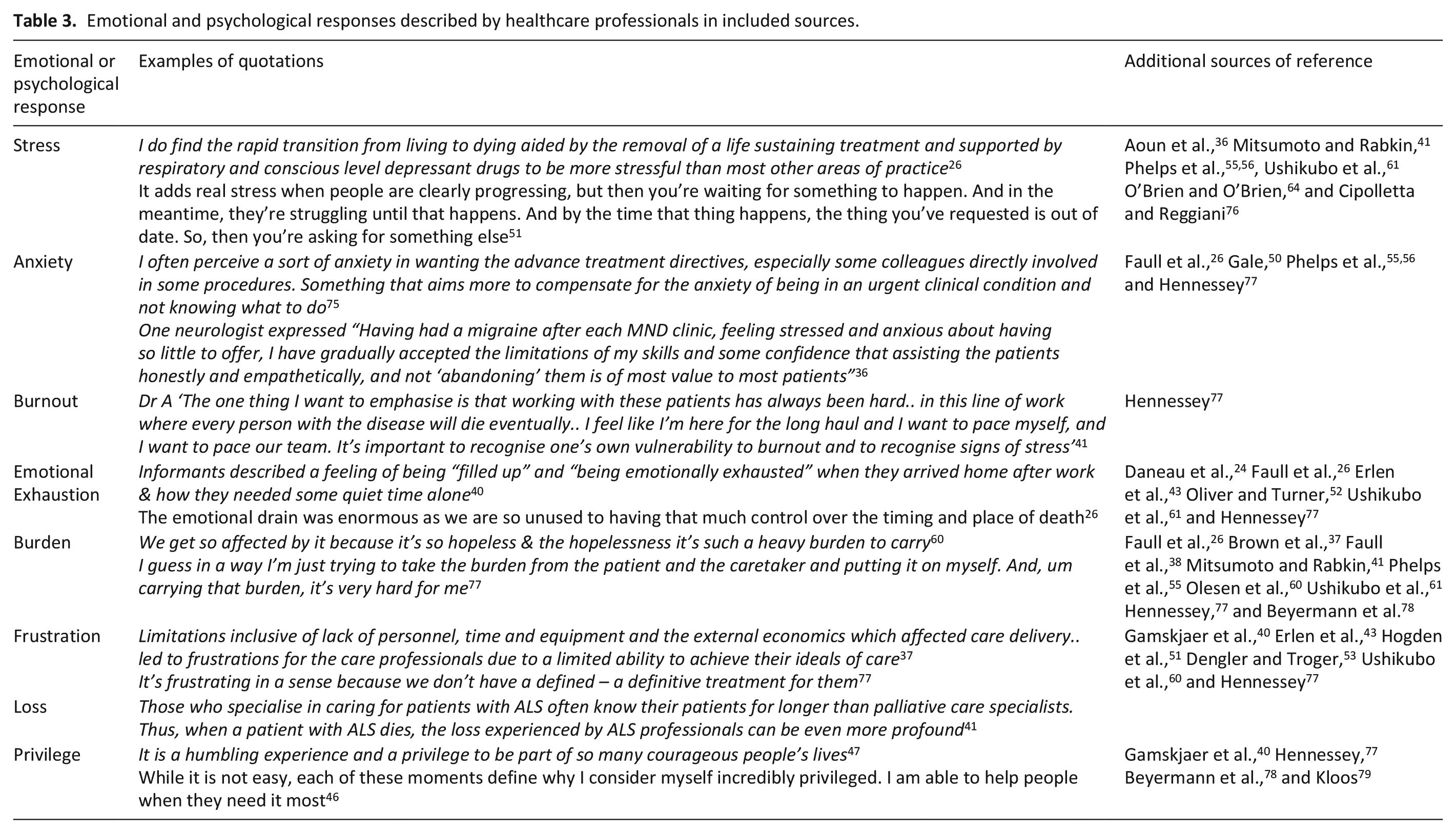
Many sources referenced the emotional involvement for professionals working with motor neurone disease.22,24,26,37,38,40
–42,45,46,52,55,56,58,64,68,73,76
–78 A full overview of the emotional and psychological responses described are provided in Table 3. Professionals reported needing to disengage their personal feelings38,64 and using compartmentalisation as a coping mechanism, whereby they avoided thinking about work situations outside of work, many felt they would not be able to continue in their role otherwise:
77
I kind of have to separate a bit emotionally because obviously I wouldn’t be able to survive
77
Emotional and psychological responses described by healthcare professionals in included sources.
Other professionals, particularly those who spent a lot of time with patients such as clinical specialists, homecare nurses and primary care teams reported developing close relationships and for some an emotional connection or bond.37,41,58 These professionals could feel profound loss on the patient’s death.41,58 In one source, 66% of neurologists and 94% of clinic managers contacted a patient’s family after their death and 25% of neurologists and 55% of clinic managers attended patient funerals;
22
another neurologist reported:
I don’t go to funerals, it’s kind of like my line. I can be sad with the patient and the family all the way to their death, but I just can’t go to a funeral a week. . . it’s just too much for me
77
Professionals discussed how some cases affected them more than others, such as when the disease progressed quickly, or patients were younger. 40 Others found it emotionally challenging to witness patient and family suffering.25,45 Professionals described how it could be hard to leave their jobs behind when they were not working 60 and that episodes from work could occupy their minds in their private lives. 40 In two sources professionals reported lack of preparation and education about how to manage the emotional and moral suffering they experienced from working with these patients.51,82
Five sources discussed the profound emotional intensity for professionals involved in withdrawing non-invasive ventilation.26,38,55,56,58 Professionals reported a huge emotional strain planning for the withdrawal, ‘it felt like setting a date for someone to die’ 56 and ‘a personal sadness’ after the withdrawal had taken place. 38 In a study of UK doctors over half of the respondents rated the emotional challenge of withdrawing ventilation as 7/10 with over 20% rating this as 9/10 on the scale. 55 Three studies reported the lasting effects on professionals involved in this process with some reporting vivid memories that stayed with them for years after the event.38,55,56
Nine sources discussed a sense of job satisfaction and reward that professionals experienced from working with motor neurone disease patients.22 –24,40,45,46,56,77,79 Professionals described how they felt privileged to be in the position to support patients and families through a difficult time, help them when they ‘needed it most’40,46,47,56,77 and felt appreciated by the level of gratitude they received.40,46,77,78
you really get so much in return, you know, when you are in the midst of all the hopelessness – you actually feel the appreciation or gratitude coming from the patient or the relative
40
In two sources professionals reported that a benefit of their work was that the life and death scenarios they encountered, gave them greater perspective and appreciation for their own personal lives.40,77
Discussion
Main findings
To the best of our knowledge, this is the first review that has comprehensively identified the available literature representing professionals’ experience and the emotional and psychological impact of working with motor neurone disease. A total of 1692 professionals are represented, from 15 disciplines and 6 key healthcare settings. There are few examples of other conditions requiring intervention from this number of professionals and teams, within a typically short trajectory of illness.
From this review it is evident that working with motor neurone disease is distinctive and more stressful than other areas of practice. The care provided is intensive, time-sensitive and needs to be individualised for each patient and their informal support network. It is necessary to keep up with emerging knowledge and evidence, specialist skills, technology and aids to meet the evolving needs and expectations of patients and families. Developing trusting relationships with patients and families was seen as important as professionals frequently engaged in difficult and emotionally charged conversations about deteriorating health and future care planning. Complex decision-making also raised significant legal, moral and ethical uncertainty for many professionals involved.
Factors were identified which could restrict or support professionals to provide what they considered high-quality care. These included the physical and psychological condition of the patient, the needs of their informal caregivers, team and collegial support and a range of organisational factors. Three sources also discussed practical and emotional challenges to providing adequate care for this population during the COVID-19 pandemic. This is widely supported in the literature with many professionals experiencing mental health problems and moral injury because of difficulties delivering optimal care for severely unwell patients during this time. 81 Despite the added impact of COVID-19, the emotional and psychological toll for those working with motor neurone disease was evident before this period, with both positive and negative implications identified in this review.
What this study adds, implications for practice and future research
The findings of this review corroborate research outlining the difficulties experienced by motor neurone disease patients and informal caregivers in their interactions with the healthcare system. Their experience of services as being fragmented and difficult to access12,82 is echoed by professionals in this review. Professionals identified geographical variation in services and funding available, 62 different team compositions and priorities, 13 poor communication between teams and services, 39 time pressures and varying degrees of professional confidence and experience 65 as limiting their ability to provide adequate levels of care in some circumstances. Feelings of powerlessness and frustration were expressed by professionals in several situations when they felt constrained in their ability to efficiently meet their patient’s needs;37,40,51,60 organisational factors were also attributable to experiences of stress and burnout.22,51,77 Organisation-focussed changes and interventions have been shown to effectively reduce burnout for healthcare workers. 83 The need to standardise care pathways and inter-service communication among professional teams has been previously called for 84 and is required to alleviate the stress associated with poorly co-ordinated care for patients, their families and the healthcare teams involved.
The emotional toll for professionals exposed to repeated patient suffering, death and dying are well established in oncology and palliative care.85,86 Previous research has identified the need for greater recognition of the emotional burden for professionals caring for people with terminal neurological diseases. 87 Harris et al. 21 found that professional well-being was almost completely ignored in the motor neurone disease literature, despite alluding to stress and burnout as a problem. Similarly, this review found that professional well-being was not directly questioned or measured and was not the primary aim of most identified sources. However, feelings of being overwhelmed, burdened, emotionally exhausted, frustrated, stressed, anxious and burnt-out were identified by professionals’ managing different aspects of motor neurone disease patient care. The psychological well-being of healthcare professionals is a growing concern internationally. 88 Reduced professional well-being in many clinical areas, is linked to absenteeism, high rates of turnover and has implications for the quality of patient care. 89 Phenomena, such as occupational stress, burnout, compassion fatigue and moral distress have been widely recognised for clinicians faced with prolonged exposure to patient suffering, complex end-of-life care dilemmas90,91 and for those working in high intensity clinical environments.92,93 The challenges described by professionals in this review further strengthen the need to investigate the well-being of this population. Identifying specific risk factors for reduced professional well-being is important to mitigate the consequences for professional retention and motor neurone disease patient care.
It is important to highlight the positive experiences identified by professionals working with motor neurone disease, including feelings of pride and satisfaction in being able to help 46 and enhanced appreciation for their own health and personal lives. 77 Having good multidisciplinary team and collegial support was important for job satisfaction; 40 for those who were working alone feelings of stress and anxiety were more prominent.56,76 This is concordant with the palliative care literature, whereby homecare assistants and community nurses providing hospice care at home identify loneliness and isolation as factors negatively influencing their job satisfaction. Peer support and contact positively impact their well-being and intention to stay. 94 Potentially protective or supportive factors were not explicitly measured in any identified source or explored with members of the multidisciplinary team, other than neurologists. Coping mechanisms, such as compartmentalisation and debriefing with colleagues were identified in one study. 77 Previous experience was helpful in certain circumstances, 60 but was not always the case. More years of experience could be associated with higher stress levels, 22 and years of experience was not helpful in the most challenging clinical scenarios.35,49 Personal protective factors, meaning in work 95 resilience 96 and coping styles97,98 have been identified as supporting professionals working in palliative and other end-of-life care positions and warrant greater consideration for those working with motor neurone disease.
This review identified that while professionals from different disciplines and working within different service and organisational structures share many of the same stresses, frustrations and emotional responses to working with this patient population, they also have different experiences, responsibilities and needs for support. Despite many sources recognising these differences, they were not explored in depth. To facilitate professionals to work synergistically and provide the level of integrated care required by motor neurone disease patients, future work is needed to identify both the individual and shared needs for support of the different groups of professionals involved in providing care for these patients.
Strengths and limitations
This is the first review to provide a comprehensive overview all healthcare professionals’ experience and perspective of providing motor neurone disease care. The primary strength of this review is the use of a transparent, systematic and reproducible search strategy and broad inclusion criteria. Included sources were limited to the English language typically reflecting middle to high income countries such as the UK, USA and Australia. This may have excluded representation of healthcare services from other countries that may have provided alternative cultural insights or challenges. Some included sources can be considered low level evidence such as case reports and opinion pieces. Title and abstract screening were completed by the first author only. Although due care was taken, some relevant sources may have been excluded in error, as they were not cross-checked. Critical appraisal of included sources was not undertaken, as was not relevant for the purpose of this review.
Conclusion
By reviewing the literature available from 1990 to 2024, we have categorised how healthcare professionals describe the experience of working with those affected by motor neurone disease. Professionals perceive working with motor neurone disease as distinctive from other life-limiting conditions. External and organisational barriers could limit their ability to provide optimal levels of care and working with these patients and families had implications for professional well-being. The potential for some to remain working in this clinical area over time was questioned, while others avoided working with this patient group. Working within an effective and supportive multidisciplinary team was important for both job satisfaction and emotional support. Addressing some of the external and organisational issues identified has the potential to support and retain professionals to provide the intensive, integrated and specialist level of care required by these patients and their informal support network. It is also important to acknowledge and recognise the potential for professional stress and emotional burden for those interacting with these patients and their families. Future research should focus on identifying specific risk and protective factors for professional well-being and tailored support strategies to address the unique needs of professionals working with motor neurone disease.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241291745 – Supplemental material for Working with people living with motor neurone disease and the impact on professionals’ emotional and psychological well-being: A scoping review
Supplemental material, sj-docx-1-pmj-10.1177_02692163241291745 for Working with people living with motor neurone disease and the impact on professionals’ emotional and psychological well-being: A scoping review by Megan Walls, Austin Claffey, David Mockler and Miriam Galvin in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163241291745 – Supplemental material for Working with people living with motor neurone disease and the impact on professionals’ emotional and psychological well-being: A scoping review
Supplemental material, sj-docx-2-pmj-10.1177_02692163241291745 for Working with people living with motor neurone disease and the impact on professionals’ emotional and psychological well-being: A scoping review by Megan Walls, Austin Claffey, David Mockler and Miriam Galvin in Palliative Medicine
Footnotes
Author contributions
MW developed the study protocol, completed the search process, extracted and analysed data and wrote the manuscript. AC reviewed the study protocol, assisted with the search process, reviewed, edited and approved the final version of the manuscript. DM developed the search strategy and assisted with the search process. MG reviewed the study protocol, assisted with the search process, reviewed, edited and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Irish Health Research Board.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.