
Abstract
Background:
The increase in non-communicable disease burdens and aging populations has led to a rise in the need for palliative care across settings. In resource-limited settings such as Indonesia, however, notably in rural areas, there is a lack of professional palliative care. Little is known about specific palliative care navigation, as previous studies have mostly focused on cancer care navigation. A locally tailored approach is crucial.
Aim:
To explore how patients and families navigate palliative care and the problems they experience.
Design:
An ethnographic study using in-depth interviews and observations, analyzed using reflexive thematic analysis.
Setting/participants:
Interviews with 49 participants (patients, family caregivers, and health professionals) and 12 patient-family unit observations in Banyumas, Indonesia.
The analysis:
Patients and families navigated palliative care through different strategies: (1) helping themselves, (2) utilizing complementary and alternative medicine, (3) avoiding discussing psychological issues, (4) mobilizing a compassionate and advocating community, and (5) seeking spiritual care through religious practices.
Conclusions:
Our participants used intricate care networks despite limited resources in navigating palliative care. Several problems were rooted in barriers in the healthcare system and a lack of palliative care awareness among the general public. Local primary health centers could be potential palliative care leaders by building upon pre-existing programs and involving community health volunteers. Cultivating a shared philosophy within the community could strengthen care collaboration and support.
Geographical and financial barriers hinder access to adequate palliative care.
Patients and families living in rural areas in the Global South face greater challenges in caring for patients.
Thus, family caregivers of patients with serious health-related suffering carry a heavy burden of care.
Patients and families adopt creative strategies and utilize intricate care networks to access care and ease the caregiving burden.
A shared philosophy of communal cooperation (Gotong Royong) within the community strengthens care collaboration and support.
Developing local primary health centers’ leadership in palliative care by building upon pre-existing programs and involving community health volunteers.
Creating a safe space for discussion about issues and concerns in the palliative setting, including psychological issues and the use of complementary and alternative medicine.
Providing training for health professionals related to overlooked aspects of palliative care: social, psychological, and spiritual dimensions.
Introduction
Accessing healthcare, including palliative care, is an important element of basic human rights. However, with difficult access to palliative care, a better understanding is needed about how people navigate their care situation and where they run into problems. Analyzing care navigation in this case means looking closely at the strategies patients and families use to facilitate access to medical and additional services, or to solve problems in complicated healthcare systems with limited-service provision.1,2
Patient navigation emerged to support patients through the care continuum by providing personalized assistance to overcome barriers to access and offering guidance to improve patient outcomes.3,4 A previous systematic review of cancer patient navigation showed increased supportive care efforts and improved the quality of life of family caregivers. 5 Providing culturally specific patient navigation also helped improve palliative care outcomes. 6 Studies such as the Canadian Nav-CARE, 7 the European NavCare-EU, 8 and the Australian All.Can 9 were aimed at supporting people with cancer in high-income countries. Nav-CARE, for instance, improved family caregivers’ quality of life and their sense of engagement in care. 7
However, there is very limited literature that specifically investigates palliative care navigation, as previous studies mostly focused on cancer care navigation. 4 These studies have been conducted in vulnerable populations in high-income countries. The general population in low- and middle-income countries is still disproportionately underrepresented in the literature. A number of studies from India and Africa have shown that local non-governmental organizations and the integration of community efforts helped increase the coverage of sustainable palliative care through primary care services.10 –13
A robust understanding of the availability of palliative care at the grassroots level is needed to further design effective interventions aimed at improving palliative care navigation. A specific and tailored approach that considers local values and sociocultural factors is crucial. Indonesia has a strong cultural influence on care, as Indonesian families are expected to provide and be involved in the care of ill family members.14,15 Therefore, it is important to understand how patients and their families currently navigate palliative care and the problems they experience in rural and resource-limited settings of low- and middle-income countries, such as Indonesia. The palliative phase of care in this study refers to the phase in which patients are in need of palliative care.
Aim
To explore how patients and families navigate palliative care and the problems they experience in the rural, resource-limited setting, of Banyumas, Indonesia.
Methods
Design
Underpinned by hermeneutic epistemology, we conducted ethnographic research in Banyumas for 8 months (June 2022–January 2023) to understand more thoroughly the way people navigate palliative care in the study setting. This method enabled us to observe and experience the life conditions and strategies of the participants in their daily lives within more natural settings, which contributed to answering our research question.16,17
Study setting
Indonesia is facing an increase in non-communicable diseases such as cancer and chronic diseases, and an aging population,18 –23 leading to a rise in the need for palliative care, estimated at 1,451,100 people (0.52%) annually. 24 Nevertheless, a lack of professional support hinders palliative care for patients and their families in resource-limited settings, including in rural areas of Indonesia.25,26 Geographical challenges,25,27 coupled with the absence of formal and systematic integration into the national healthcare system, contribute to isolated and patchy palliative care provision.24,28
Banyumas, in Central Java, is considered a rural area due to its geographical location, demographic characteristics, and type of health services. With its population of around 1.8 million, Banyumas mainly consists of villages. The regional government minimum wage in 2024 was Rp 2,195,690 (140 USD) per month. 29 The region has 4 public hospitals, 19 private hospitals, 40 public primary health centers (Puskesmas), and 66 primary care clinics. 30 Most of the hospitals are distributed in the center of the region. Although the number of health facilities seems adequate, the type of services provided in these facilities are still limited compared to urban areas of the country. Since 2017, structured palliative services have only been available at a regional referral hospital. Meanwhile, homecare services—provided by private hospitals, health philanthropy organizations, Puskesmas, or freelance nurses—lack formal palliative care labeling and structured programs, thus impeding accessibility. Families can arrange paid homecare services, costing around Rp 100,000 (4.5% of the regional minimum monthly wage) per visit. Higher-income families are more likely to access these services due to the associated cost. Homecare teams mainly cater to patients with skin ulcers, offering wound and nursing care.
Population
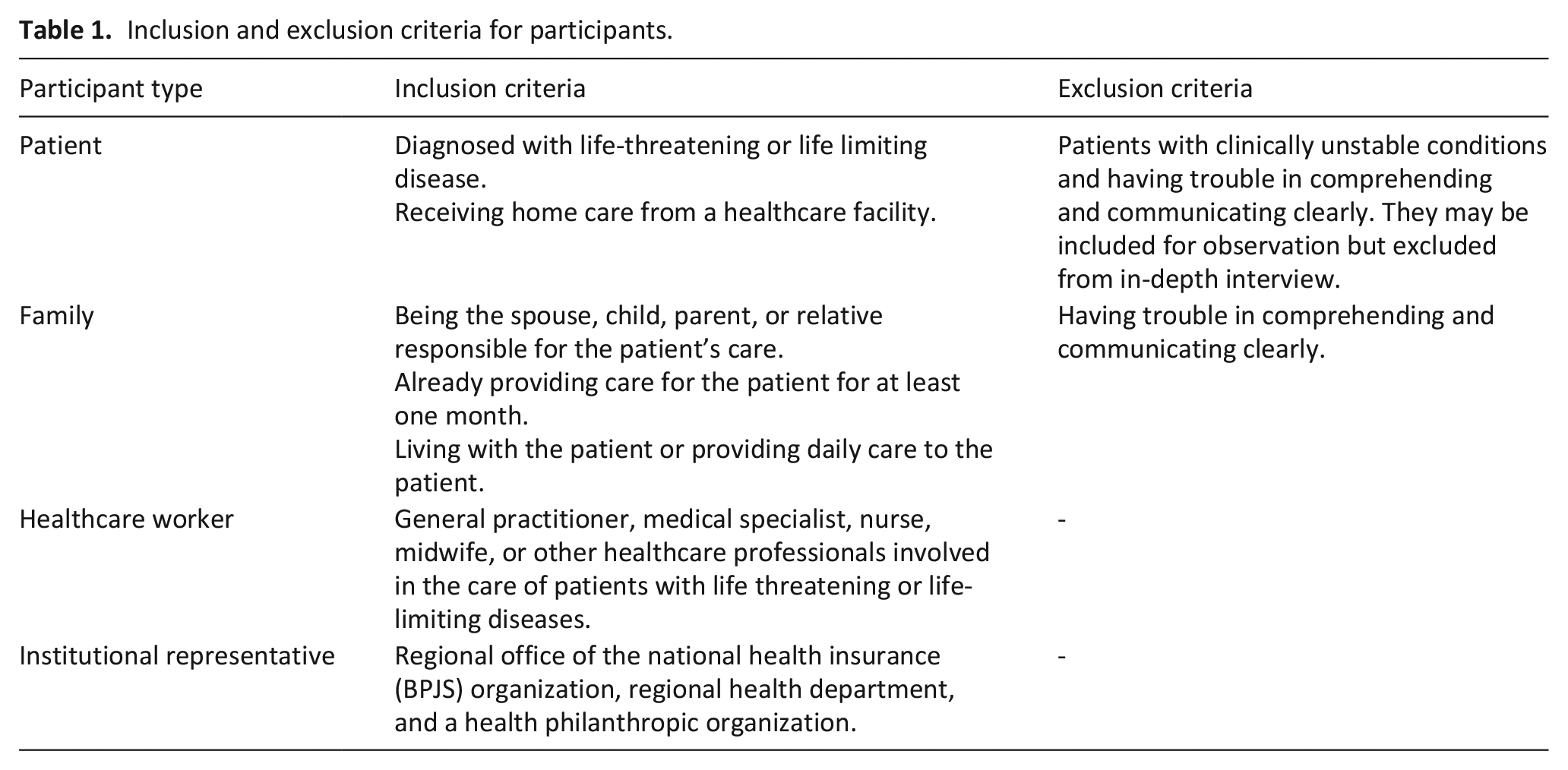
This study was part of a larger doctoral research. We aimed to investigate a wider range of phenomena in palliative care navigation by involving different types of patients, families, and health professionals. Table 1 provides information about the inclusion and exclusion criteria for this study.
Inclusion and exclusion criteria for participants.
Sampling
Participants were recruited through purposive sampling. The information power model 31 helped us position ourselves and assess the approximate number of participants needed for a robust analysis. A provisional number of 10 participants for each group (patients, family members, and health professionals) was established.
Recruitment
We asked health professionals from local hospitals and Puskesmas to recommend adult patients diagnosed with life-threatening or life-limiting illnesses who were in the palliative phase and receiving home care. After meeting these recommended patients, the ethnographer confirmed that all were eligible for the study. Two elderly patients with severe joint disorders were included due to their non-operable condition. Only one cancer patient was receiving homecare from the Puskesmas. We excluded four patients who were too ill to be interviewed, but they were still included for observation. Adult family caregivers and health professionals involved in the patients’ care were also included. Midwives were included as they were involved in palliative care, utilizing their nursing and communication skills.
Ethics declarations
Ethical approval was obtained from the Ethics Committees of the Faculty of Medicine, Universitas Jenderal Soedirman (Ref:009/KEPK/PE/VI/2022), and the Prof. Dr. Margono Soekarjo General Hospital, Purwokerto, Indonesia (No:420/07606). All methods adhered to relevant guidelines and regulations including the ethical principles for medical research involving human subjects as outlined in the Declaration of Helsinki, World Medical Association. Informed consent was obtained from all participants, with compensation (Rp. 100,000) provided for family units and a small present for health professionals. The compensation amount was chosen as it was similar to a single homecare visit cost and given after data collection was finished.
Dataset generation
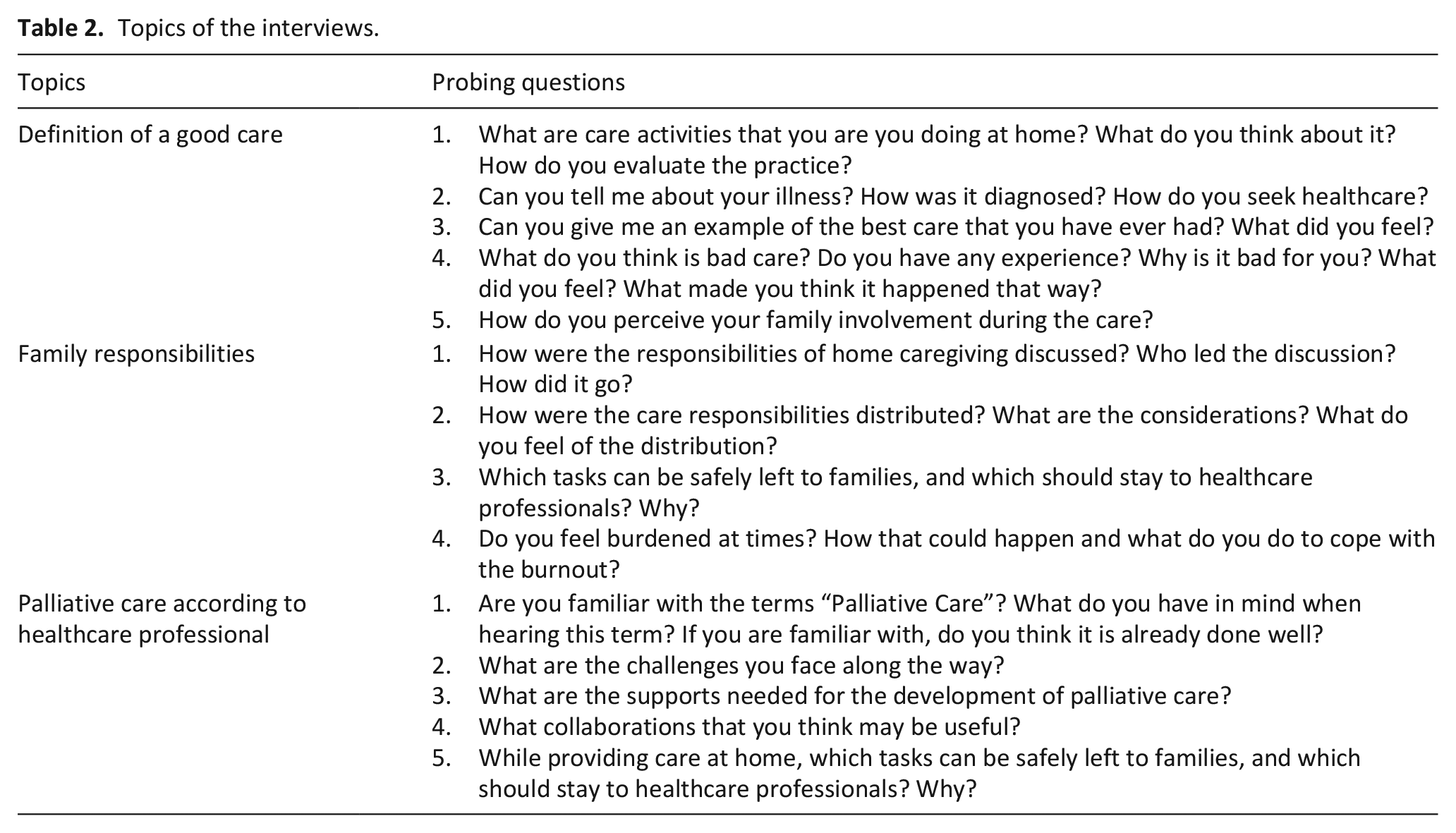
The first author (RBW) conducted ethnographic in-depth interviews and observations. After receiving participants’ consent, in-depth interviews (ranging from 17 to 88 min) were conducted. In-depth interviews were chosen to meticulously explore each participant’s perspectives and views on the topics of the interviews, which are listed in Table 2.
Topics of the interviews.
Twelve family units were involved in the observation, each was visited twice (1–3 h per visit) to capture the care provision at home by healthcare workers and family caregivers. Elements of the observation are described in Table 3.
Elements of the observation.

Observation field notes, photographs, and audio recordings were taken. After repeated meetings with all research team members, we decided the data was sufficient to develop new knowledge through conceptualization of the themes.
Data analysis and study rigor
Ethnographic methods allow us to see participants enacting their values in everyday practice and reflecting upon these values through conversations about their situations. 32 Therefore, we deemed reflexive thematic analysis 33 to be suitable for the ethnographic principles. We also considered and reflected upon how the ethnographer’s (RBW) background as a medical doctor majoring in bioethics, being Muslim, and residing in Banyumas shaped the observations, interviews, and interpretation of findings. For instance, some participants approached RBW with medical questions due to their hesitancy to ask the attending physician. RBW assured them that the anonymized results of the study would be reported and shared with relevant parties. These instances highlighted potential unmet needs for effective communication channels between patients and healthcare workers.
Authors (RBW and AM), with native proficiency in Bahasa Indonesia, read and reread the transcripts and observation field notes to become familiarized with and immersed in the data. We inductively analyzed the data using latent coding and created mind maps to visualize the connections between codes. Photographs were coded and analyzed together with the same categories from the transcripts and observation field notes. RBW generated the initial themes. Biweekly meetings with all research team members (RBW, AM, DW, and JP) were conducted to review and develop the themes through collaborative discussion and critical revision. The iterative reflection during these meetings helped us develop, refine, and define meaningful themes. We report this study based on the Reflexive Thematic Analysis Reporting Guideline. 33
Consistent with the ethnographic approach, we involved participants with different characteristics in the interviews and observations. This helped ensure that conflicting perspectives were considered, reflected upon, and situated among each other, thus enhancing the study’s validity. Prolonged exposure to participants also strengthened the credibility of the study. Extensive field notes were taken after each observation to gain a thorough understanding of the findings. All data are stored in a MAXQDA Plus 2022 project file. Every reflection note, change in coding, and additional modification to the categories and themes were recorded in the project file to maintain a transparent audit trail.
The analysis
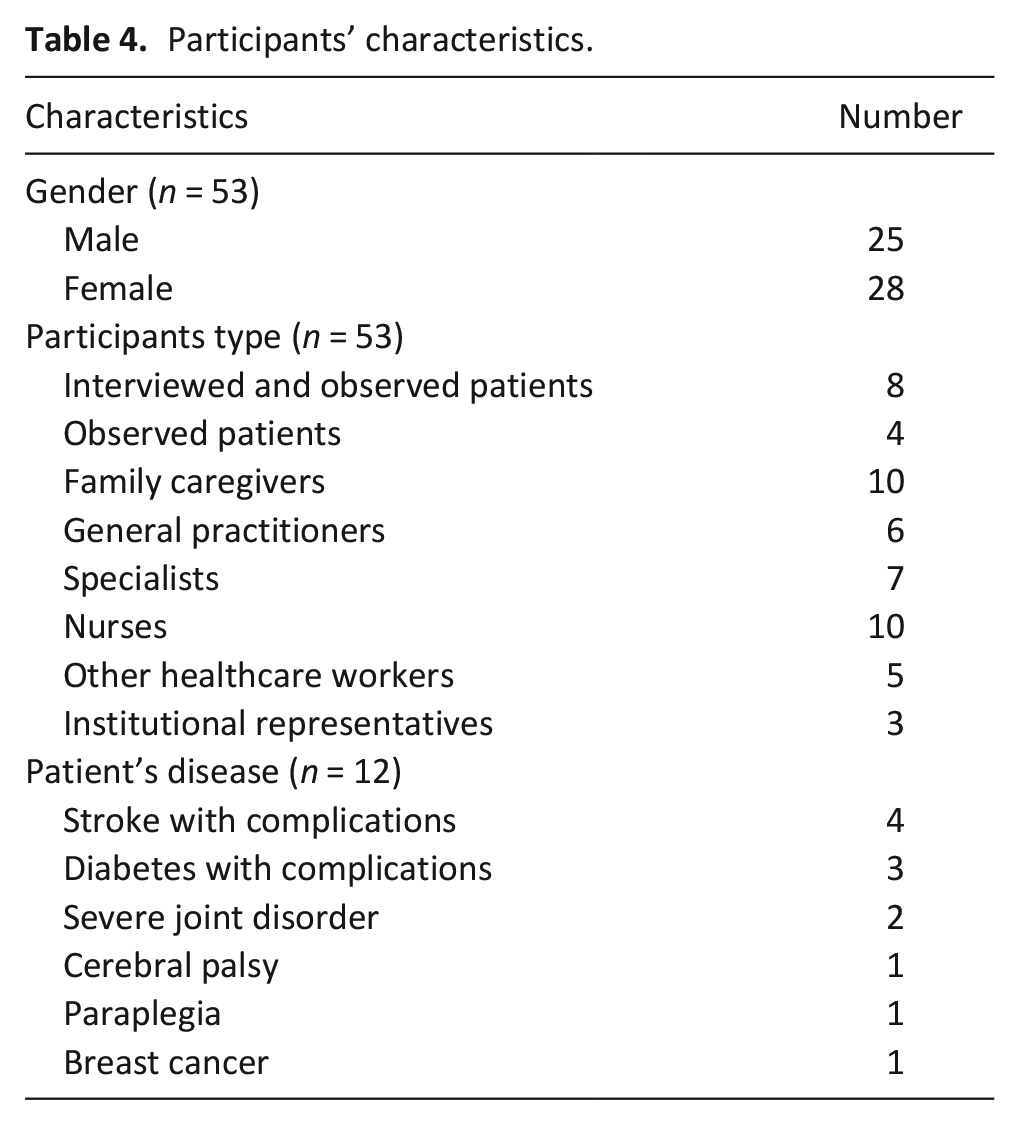
A total of 53 participants were recruited in this study. Participants’ characteristics are described in Table 4.
Participants’ characteristics.
Patients and families in our study navigate palliative care in various ways. We developed five themes reflecting these strategies, as illustrated in Figure 1.
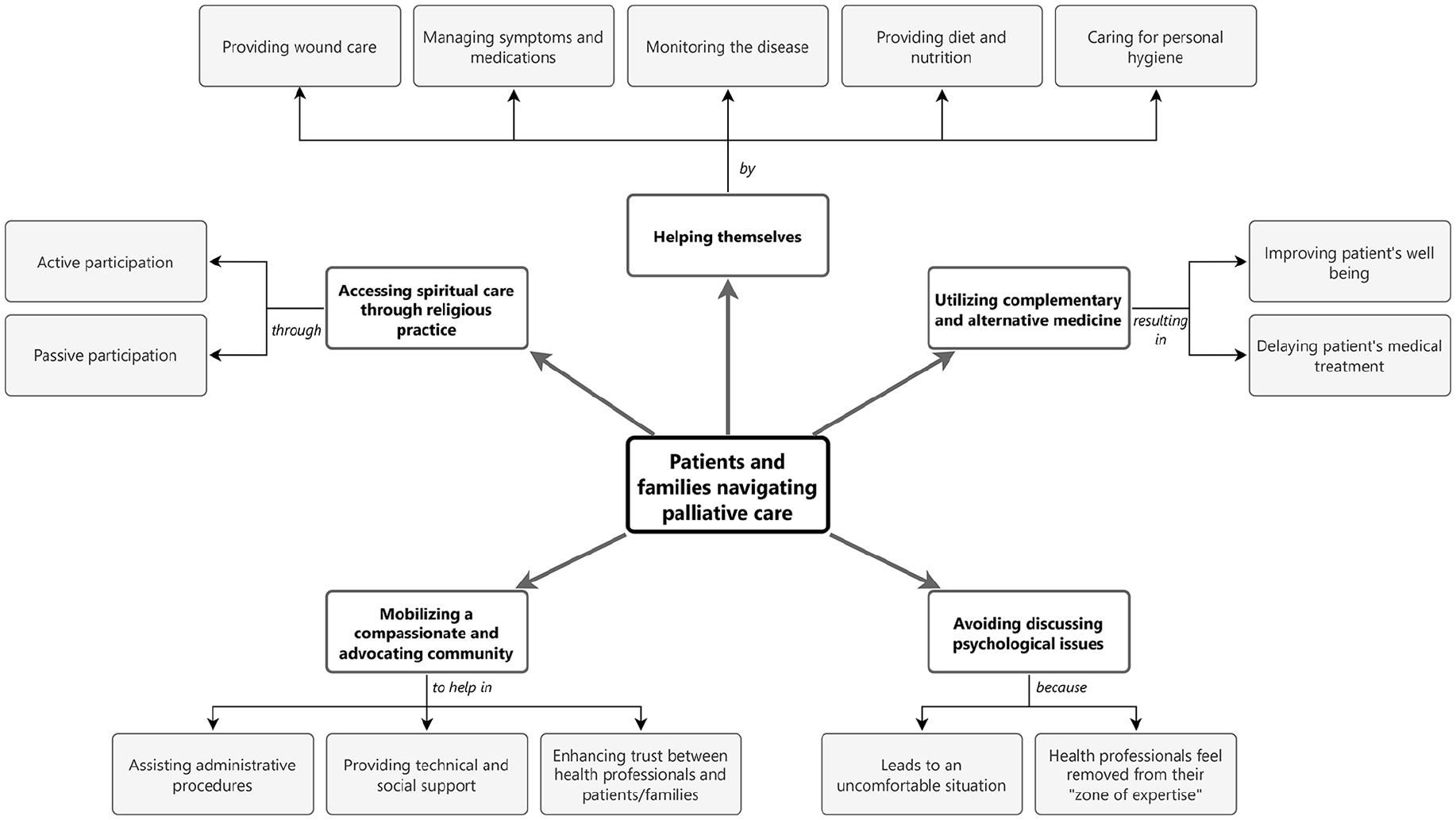
Themes and categories in a mind map.
Patients and families helping themselves
Family caregivers took on a larger role in home care than health professionals. They handled various aspects of care with different levels of proficiency. Some had basic nursing skills training from hospital or homecare health professionals. The training enabled them to provide basic wound care for patients with diabetic or pressure ulcers:
Yesterday, I opened the wound dressing and cleaned it with NaCl (normal saline) solution and gauze. My brother said it felt cold and nice after I cleaned it. (Patient’s sister, Family no. 11, Row 185-196).
The sister expressed her satisfaction with independently cleaning her brother’s wound. Families were advised to provide wound care only for less severe wounds to avoid complications, with a strong recommendation to contact a nurse if needed. However, a nurse was not always available, leading families or patients to do it themselves. Family caregivers also supervised patients to take their medications at prescribed times, which can be complex due to various medications, including disease-modifying drugs, symptomatic medications, and supplements. Challenges arose when managing severe symptoms or when medication was not available, leaving families unsure of their next steps:
The patient is lying on his bed, sideways [. . .] He said that his wound is now feeling so much more painful than the days before [. . .] His wife said that he had just screamed from the pain before we came [. . .] It turns out that the pain medicine, ketorolac, is finished. Then the patient and his family asked whether they could purchase it independently (at a local pharmacy) without prescription. (Fieldwork note no. 5).
The homecare nurse assured the participants that they would try to provide additional painkillers in the next visit.
Some families fed patients who were unable to eat independently, while also adjusting diets based on medical advice. These diets were sometimes completely different to what they were used to. One participant bought baby food, free from flavor enhancer and preservatives, perceived as healthier and easier to swallow for the patient.
Families managed the physically challenging task of providing daily bodily hygiene, including frequent washing for patients who experienced frequent secretions. Assisting patients to the bathroom, even with a wheelchair, was described as overwhelming; one participant expressed it by asking “when will this (condition) eventually end?”. When facing difficulties, caregivers sought help from other family members, neighbors, or used diapers instead.
Some patients and families creatively designed home-made devices, such as holes in the bed or a chair, or in-bed urine pipe installation (Figure 2), to ease patient’s urination or defecation:
It was my idea (to make this urine pipe installation), my nephew helped me make it and connected it to the septic tank. (I understand that) it is bothersome to collect my urine, I would feel sorry for my son if he did it every day, as he must go to school. (That is why) I think about it a lot. (Patient no. 2, Row 26-31).

In-bed urine pipe installation: when the patient needs to urinate, he can insert his penis into a disposable plastic pipe, which is connected directly from the bed to the PVC pipe leading to the septic tank.
The patient’s motive resonated with another patient (P01) who said that “I don’t want to further burden my children”, illustrating how patients worked together with families to ease the caregiving. However, some devices were contaminated with urine or feces residue and not adequately cleaned.
We show that patients and families work together to provide care for themselves. Similar to previous studies, families provide most care, leading some of them to experience care burdens which reduce quality of life.14,34,35 Despite challenges, most family care is motivated by love and cultural-religious factors. 14 The lack of structured professional support and insurance coverage contributed to unmanaged patient symptoms and unmet needs for communication with healthcare professionals. Patients and families would benefit from sharing concerns with health professionals, emphasizing the importance of professional home palliative care teams with 24/7 availability. This support would provide a sense of security and preparedness. 36 Health professionals could offer hotlines for information and assistance.37 –39 Providing nursing skills training for families and effective communication skills for health professionals could enhance their confidence in caregiving.15,40,41 Including palliative care and home care in Indonesian health insurance coverage is crucial for improved access, as seen in other countries. 42
Utilizing complementary and alternative medicine
Indonesia, known for its medicinal plant biodiversity,43,44 also has a high prevalence of complementary and alternative medicine use.
45
Some participants in this study used complementary and alternative medicine to improve their condition, while others deemed it unnecessary and potentially harmful. Some patients and families combined prescribed drugs with complementary and alternative medicine, such as acupuncture, herbal drinks (jamu), and traditional massages (pijat), to improve patient’s condition and well-being:
He did not drink any medication because he felt no effect from it. I took him to different traditional massage healers for a few months, but our money ran short. Therefore, I tried to make jamu myself at home. The jamu consisted of turmeric, garlic, lemongrass, cardamom, and free-range chicken egg yolk. But it was quite difficult to find the egg, I had to search everywhere. I made this jamu so he can walk again. Alhamdulillah (praise God), he felt healthier and had more energy. (Patient’s wife, Family no. 9, Row 124-125).
One neurologist approved acupuncture as “an adjuvant therapy that might be supportive”, although the medical evidence was uncertain.
An integrative approach in palliative care supports combining complementary and alternative medicine and conventional therapy to enhance patients’ quality of life.46,47 Previous studies indicate growing interest in complementary and alternative medicine within palliative care,48,49 suggesting potential symptom improvement. 50
However, accessing complementary and alternative medicine is difficult as it is not covered by national health insurance, and providers are often located far away and unavailable for home visits. Patients and families also face additional expenses for travel and long queues at the complementary and alternative medicine providers. Not all experiences with complementary and alternative medicine were positively appreciated:
The alternative treatment is inconsistent, sometimes it is helpful, sometimes it makes the condition worse, like what happened to my younger sibling. He followed suggestions from his friends to seek alternative treatment. If it was me, I would only go to the doctor. They know better. (Patient’s husband, Family no. 3, Row 213-229).
Complementary and alternative medicine involvement could delay medical treatment, as illustrated by this patient with breast cancer:
Before I finished the chemotherapy series, someone told me there was another way, by putting some egg on the breast skin. I felt tricked (after trying), as the breast wound was worsening. Finally, I asked Puskesmas (local primary health care) doctor, then I was referred again to the hospital for breast surgery three months ago. (Patient no. 10, Row 10-11).
Most cases of alternative medicine use would not have led to trouble if they had been first discussed with biomedical care providers. Some health professionals questioned its evidence and feasibility. 51 To minimize potential risks and harm, health professionals should openly discuss complementary and alternative medicine with patients and families.52,53
Avoiding discussing psychological issues
Patients and families often felt it was inappropriate and irrelevant to discuss psychological and emotional issues with healthcare workers:
Maybe I need psychological support [. . .] But I don’t know what kind of psychological support, how to say it. If the psychologist asks me “What would you like to discuss with me today?” I am confused, what to discuss? [. . .] I am embarrassed (to cry and tell my sadness). I am a mother; I should not cry in front of others. I must be strong, steadfast, happy. . . Otherwise, people will call me “weak”, not grateful, or not capable of having her as my daughter. . . (Patient’s mother, Family no. 8, Row 137-141).
This revealed the participant’s inner conflict and fear of being labeled by others when discussing her burden. Despite being with family, patients might still feel a lack of attention. This loneliness and unmet psychological support needs were reflected when patients expressed their feelings while reaching out to the ethnographer. The challenge and hesitation to openly discuss psychological concerns are probably influenced by personal, family, and public stigma surrounding mental health issues. 54 Cultural expectations for care also contributed to family caregivers’ discomfort in dealing with their concerns.14,55 –57
Likewise, health professionals often avoided discussing psychological distress among patients and families, perceiving it as inappropriate and outside their expertise:
I have not provided psychological support. We are still busy coordinating within the village for patients’ transportation and everything else. [. . .] From my perspective, it is more about our (lack of) competence. (We don’t care for) the psychological aspect. We have not coordinated this yet. (Puskesmas Nurse, Nurse no. 3, Row 105-107)
When health professionals observed family tensions, some preferred to hold back and ask the family to solve the issue themselves. The healthcare workers’ feeling of being unequipped to engage further may be due to personal discomfort, negative emotional responses, or lack of training.58 –60 Comprehensive moral and psychological support is needed, 39 thus including psychologists or psychiatrists in the care team and providing psychological care training for the team could be beneficial. 61
Mobilizing a compassionate and advocating community
In rural Indonesia, some low- or middle-income patients struggled to access healthcare due to their lack of knowledge about applying for health insurance. Neighbors attempted to assist by connecting them with free homecare services from philanthropic organizations. Neighborhoods are organized in tiers, with the smallest being Rukun Tetangga (RT), which consists of 10-20 houses. Several RT combine into Rukun Warga (RW). Several RW form villages (Desa/Kelurahan). The local neighborhood chief (Ketua RT) could assist patients in applying for free health insurance through the regional Social Department. Currently, homecare is not covered by national health insurance, necessitating hospital visits with travel costs of up to Rp 300,000 (14% of the regional minimum monthly wage). Neighbors could offer free transportation, either voluntarily or through the Mobil Desa program, a village-level program aimed at providing transportation by car for health-related purposes. Although low-income families might receive irregular government stipends, patients with immobility found it challenging to collect them at the village hall.
Neighbors and friends showed support through house visits, financial contributions, or delivering food. A patient with hemiplegic stroke and a diabetic ulcer experienced a more positive atmosphere due to visits from neighbors:
From what I observe, they look happy, as if nothing is going on. They were passionate when explaining their condition. [. . .] Some moments later, I noticed one neighbor visited them and they started comfortably teasing and making fun of one another. [. . .] I can see that this is a close and intimate neighborhood, I felt welcome here! (Fieldwork notes no. 13).
Family caregivers, when leaving the house, could ask neighbors to be with the patient at home while they were away. Community figures like the village chief or community health volunteers (kader) were crucial for healthcare workers to gain trust from patients and their families:
Usually, on every initial home visit, we invite kader to come with us, to gain patient’s trust. Patients are more familiar with kader. Without them, we may be perceived by patients as ‘fake healthcare workers’. If the patient or family still do not want to cooperate, we also invite the Pak Lurah (village chief) to come along. (Village midwife, Row 30-35).
Without community involvement, healthcare professionals might encounter rejection and suspicion, particularly in better-off neighborhoods. However, visits from community figures were not systematically regulated, resulting in unequal levels of support for different patients.
In our study, patients and families could mobilize their nearby community networks for support, aligning with previous literature highlighting the benefits of Indonesia’s tiered neighborhood organization and the Gotong Royong philosophy—the spirit of communal cooperation.27,62 Gotong Royong’s growth stemmed from the establishment of tonarigumi, a neighborhood system during the Japanese colonial era in Indonesia, fostering collaboration and a sense of belonging within communities.63,64 We found that local primary health centers (Puskesmas) already had community-targeted programs and a multidisciplinary coordination forum, upon which palliative care could be built. This study reinforces prior studies emphasizing the importance of collaboration between compassionate communities and healthcare providers for addressing inequities in palliative care access.7,65,66
Accessing spiritual care through religious practices
Patients and families sought spiritual care through various religious practices: active participation in daily prayers or reciting the holy book, or passively listening to preaching by religious figures and recorded Quran recitations.
One philanthropy organization provided spiritual care through the Bina Rohani program, which seeks acceptance through religious practices and reframing the condition as a path to redemption for past sins:
We involve a different team to provide spiritual care for ‘truly palliative’ patients: those losing hope and refusing to do chemotherapy [. . .] It is a spiritual enhancement: more prayers to God, to enhance fate acceptance, to facilitate them to realize the inevitable loss. (Health philanthropy leader, Row 71-74).
The program emphasized perseverance and not losing faith in God despite difficult situations, but it targeted only end-of-life stage patients. Families could independently arrange spiritual care by reaching out to a religious figure (Ustaz). The Ustaz might encourage the patient to seek for God’s forgiveness and recite the Quran to calm the patient.
Family caregivers also encouraged religious practices, motivating patients to engage in Shalat (Islamic daily prayers, performed five times a day) and the Quran by saying:
“What are you waiting for? Until when will you not pray to God due to this illness?” (Fieldwork notes no.4).
Family members helped immobile patients to pray while lying in bed. One family faced challenges motivating the patient to perform Shalat and chose to refrain to prevent conflict. Instead, the family turned on an Islamic TV channel with prayers and preachings.
Spiritual care in our study involved active and passive participation in religious practices facilitated by local religious figures. Despite focusing on religious needs rather than other spiritual and existential needs, 67 our participants found this helpful. Previous studies in highly religious countries support this, indicating that spiritual care is enhanced through religious practice.39,68 –70 Our prior study illustrated the influence of religious values on attitudes toward palliative care. 71 A previous study showed how specific training in spiritual care for health professionals could improve spiritual well-being and enhance palliative care provision. 72
General discussion
We outline five themes illustrating the strategies that Indonesian patients and families use to navigate palliative care in a resource-limited setting, showcasing their agency and creativity amid limited healthcare resources, and their use of an intricate social networks. These themes are helping themselves, utilizing complementary and alternative medicine, avoiding psychological issues, mobilizing community support, and accessing spiritual care. To contextualize our work in a country with a similar setting, we would like to specifically draw a comparison with Kerala, India.
Kerala is considered a leader and a good-practice example of palliative care in the Global South through enhanced collaboration among clinicians, community volunteers, and policymakers. 10 The Keralite palliative care is maintained financially through funding from different sources, mainly micro-donations. 11 Home-based palliative care services are available in Kerala and are accessible to patients with lower socioeconomic status. 73 Meanwhile, most Indonesian homecare services are paid and not specific to palliative care, therefore, they are more accessible to patients with higher socioeconomic status.
Similar to Indonesia, Keralite family members are the most vital providers of care. 73 The strong community participation in Kerala enables the empowerment of local communities to take responsibility and solve their own health problems, with guidance from nearby palliative care facilities. 74 Sustained availability of active volunteers ensures the continuity of the program. 11 These trained volunteers provide psychosocial and spiritual support for patients and their families. 74
Implications for practice and further research
Our study reveals the problems participants encountered when navigating palliative care, some rooted in systemic barriers like the lack of insurance-covered professional support for home palliative care. We recommend improving government support, such as ensuring insurance coverage, a specific palliative care budget, regular stipends for patients and families, and greater flexibility in administrative procedures. Reflecting on our previous scoping review, 39 some key elements of good palliative care were not yet present in this setting. Local primary health centers (Puskesmas), we argue, could emerge as potential leaders in palliative care, utilizing their grassroots coverage and established community collaboration. Cultivating a shared philosophy within the community, such as Gotong Royong, might be helpful in strengthening care collaboration. It might be feasible to integrate palliative care as one of Puskesmas’ key programs by building upon pre-existing programs and involving community health volunteers. As shown by experience in Kerala, community participation is critical for maintaining continuity of care. 74 These recommendations might help people navigate palliative care and improve the quality of care. Further research, employing both quantitative and qualitative research methods, is needed to identify effective strategies for involving Indonesian local communities in palliative care.
Strengths and limitations
This ethnography provides a deeper understanding of palliative care navigation in Indonesian resource-limited settings, specifically in Banyumas. In-depth interviews and prolonged observations offer a rich description of participants’ experiences, enhancing the understanding of patient and family navigation processes and challenges. The number of study participants was sufficient to conceptualize meaningful themes. Due to the qualitative nature of this study and its focus on Banyumas, Central Java, Indonesia where the majority of the population is Muslim, we encourage readers to carefully consider and reflect on the findings in a broader context.
Conclusions
We provide insights and recommendations to improve palliative care in the specific context of rural Java. Our participants’ creativity, strengthened by their social support networks and a shared community philosophy, aids in navigating palliative care. Nevertheless, problems persist in providing and receiving care. Public health centers, in collaboration with community volunteers, could be potential leaders in delivering accessible palliative care by building upon pre-existing programs. We offer recommendations that might be applicable in other settings with similar characteristics. Countries with better palliative care resources could also learn from this study, such as the importance of cultivating a shared philosophy among the community that could help in improving community engagement and boosting community cohesion.
Footnotes
Acknowledgements
We sincerely thank the participants for their time and commitment, and the anonymous reviewers for their valuable comments. The first author would also like to express his gratitude and utmost respect for his mother and father who inspired this paper and the whole PhD trajectory.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is part of a PhD scholarship funded by the Indonesian Endowment Fund for Education (LPDP), grant number 202112220808210. The funding source has no influence on this article.