
Abstract
Background:
Digital advance care planning systems are used internationally to document and share patients’ wishes and preferences to inform care delivery. However, their use is impeded by a limited understanding of factors influencing implementation and evaluation.
Aim:
To develop mid-range programme theory to account for technological, infrastructure and human factor influences on digital advance care planning systems.
Design:
Exploratory qualitative research design incorporating Theory of Change workshops that explored contextual assumptions affecting digital advance care planning in practice. A mid-range programme theory was developed through thematic framework analysis using the Non-adoption, Abandonment, Scale-up, Spread and Sustainability (NASSS) framework, generating a conceptual model depicting contextual assumptions, interventions and outcomes influencing implementation.
Participants:
A total of 38 participants (16 from London, 14 from West Yorkshire and 8 online) including patients, carers and health and care professionals (including those with commissioning responsibilities).
Results:
A conceptual model was generated depicting five distinct components relating to digital advance care planning system use: (sociocultural, technical and structural prerequisites; recognition of the clinical need for conversation; having conversations and documenting decisions; accessing, actioning and amending; and using data to support evaluation, use and implementation). There were differences and uncertainty relating to what digital advance care planning systems are, who they are for and how they should be evaluated.
Conclusions:
Digital advance care planning lacks shared beliefs and practices, despite these being essential for complex technology implementation. Our mid-range programme theory can guide their further development and application by considering technological, infrastructure and human factor influences to optimise their implementation.
Keywords
Internationally, digital approaches for documenting and sharing advance care planning information are increasingly used in palliative and end-of-life care delivery.
Digital advance care planning systems are becoming an integral component of palliative and end-of-life care policy, but there have been challenges with their uptake and use in routine practice.
There is a need for robust and theoretically informed evidence to understand how digital advance care planning systems are used in practice, their intended impacts and how best to optimise and evaluate their use.
Our mid-range programme theory defines factors that influence digital advance care planning system implementation across five components (sociocultural, technical and structural prerequisites; recognition of the clinical need for conversation and digital advance care planning; having conversations and documenting decisions; accessing, actioning and amending; and using data to support evaluation, use and implementation) of their use in routine care.
Across patients, carers and health and care professionals (including commissioners) there is a lack of clarity, and divergent views, on the purpose and intended impact of digital advance care planning systems, who they are for and professionals’ responsibilities relating to their use.
Digital advance care planning systems lack shared practices essential for effectively implementing complex technological interventions and maximising their potential impact.
The five components of digital advance care planning system implementation presented in the conceptual model can support the development of defined outcomes and indicators of success important to system implementation.
There is a need to consider how digital advance care planning systems interact with wider technological, infrastructure and human factors influences to guide their further design and implementation.
Background
High-quality palliative care includes providing patients with the opportunity to discuss their wishes and preferences and coordinating services to deliver concordant care.1 –3 Digital approaches are being developed internationally to support this process through documentation and sharing of patient information and preferences.4 –8 Typically, digital advance care planning approaches involve creating a digital record of a person’s wishes and preferences that can be shared across settings involved in their care delivery. 9 Digital advance care planning is often intended for people receiving palliative care, to support multidisciplinary working and care coordination. 9 Digital advance care plans may include demographic information, diagnosis, medication and advance care planning information including resuscitation decisions and preferred places of care and death. 10 Preliminary evidence has demonstrated the potential of such approaches to improve care quality by increasing the likelihood of patients achieving their preferred place of death and avoiding unplanned hospital admissions.11 –14
While there is a growing international focus on digital advance care planning approaches in health and care policies, there has been variation in their functionality and implementation and a lack of clarity on how they might achieve impact.3,4,15 Multiple challenges, including poor interoperability across settings, exist with their use in practice. 16 Furthermore, fewer than 1 in 10 people have a digital advance care planning record created before they die,11,17 –19 often created close to the end of life. 11 The development, implementation and evaluation of digital approaches to advance care planning have been hampered by a lack of a robust theoretical underpinning, concerns surrounding data privacy and inadequate consideration of the multiple stakeholders involved in their use.16,20,21 This study aimed to develop mid-range programme theory to account for technological, infrastructure and human factor influences on digital advance care planning systems.
Methods
Study design
An exploratory qualitative research design using theory of change workshops 22 was used to explore technological, infrastructure and human factor influences on digital advance care planning. Theory of change approaches are one way of developing mid-range programme theory (i.e. a theory of how and why a programme or intervention works; mid-range indicates the theory has a level of abstraction from specific context while remaining close enough to empirical data to be used as an applied framework 23 ), explicating the different ingredients (i.e. elements and contextual factors) required to improve the likelihood of achieving impact. 24 The mid-range programme theory is developed iteratively with stakeholders and represented in a theory of change map (i.e. a graphical representation of what is required for its intended impact to be realised). 24 We sought to develop a mid-range theory delimited to a specific application, to provide a framework for understanding and developing digital advance care planning. 25 The study was developed with patient and public involvement representatives who contributed to the design and development of the study and advised on recruitment, participant information, consent materials and workshop design.
Setting
Two regional workshops took place in England, in Greater London (workshop 1) and West Yorkshire (workshop 2), alongside an online event (workshop 3).
Population
We sought to involve patients and informal carers with experience of palliative care, health and care professionals involved in palliative care delivery and clinical and non-clinical professionals with palliative and end-of-life care commissioning and service leadership responsibilities.
Sampling
Patients and carer participants included those who accessed services for people with life-limiting or long-term conditions or non-governmental organisations that support people to make advance care plans. Health and care professionals were purposively sampled based on their professional role and included specialist palliative care (i.e. hospices and hospital teams) and community nursing, general practitioners, paramedics and care homes. We also sought the involvement of clinical and non-clinical staff with palliative and end-of-life care commissioning and leadership responsibilities.
Recruitment
This was the final study in a five-phase project exploring the implementation of digital advance care planning systems. 16 For workshops 1 and 2, we targeted participants who had taken part in earlier phases of the project, supplemented with recruitment of new participants from underrepresented groups. Recruitment to workshop 3 took place using commissioner networks across Yorkshire. 16 Between January and May 2023, we emailed invitations to potential participants. All workshop attendees provided consent either written or via a secure online form.
Data collection
Workshops 1 and 2
These in-person, 4-h workshops used the theory of change approach to explore how interactions between individuals, organisations and system-level contextual assumptions affect how and why digital advance care planning systems work in practice.24,26 In England, digital advance care planning systems are commonly called Electronic Palliative Care Coordination Systems (abbreviated to EPaCCS). 8 Consistent with a collaborative approach, participant groups (patients, informal carers, health and care professionals) were mixed across three tables, with 4 – 6 participants (ensuring representation of each participant group) at each table accompanied by two experienced research team members (a facilitator and a scribe). Four activities were completed: (1) discussion of intended impacts and outcomes of EPaCCS, (2) prioritisation of impacts and outcomes, (3) development of a theory of change map, sequentially working backwards from identified outcomes to consider the preconditions required to achieve them and (4) circulation between tables to discuss the emergent theory of change maps. The structure and overall facilitation of workshops 1 and 2 were led by a research team member, acting as a theory of change champion (SY). Event artefacts (see Appendix A) generated across activities (e.g. notes taken by scribes, sticky notes, flipcharts, cards, photographs and researcher field notes) were treated as data for analysis.
Workshop 3
Preliminary findings from earlier workshops informed the four areas pursued during this online event (via Microsoft Teams): (1) the purpose and intended outcomes of EPaCCS (e.g. with whom EPaCCS should be used); (2) how EPaCCS differ from other plans that may have relevance in end-of-life situations (e.g. Recommended Summary Plan for Emergency Care and Treatment [ReSPECT] 27 ) and EPaCCS relevance to end-of-life policy and commissioning priorities; (3) challenges experienced when implementing EPaCCS; and (4) future research priorities. Whole group discussions took place, followed by two smaller breakout rooms which were facilitated by members of the research team (KS and MA). The meeting lasted 90 min with discussions auto-transcribed by Microsoft Teams, then checked and anonymised by the research team.
Across all workshops, at least seven research team members remained constant, facilitating and participating in discussions to support continuity. In all workshops, disagreement among participants was explored through discussion.
Data analysis
We adopted a pluralistic approach to data analysis.28,29 Using different, but mutually enriching, analytic techniques enabled us to explore the complexity and nuance across the datasets. 30 Initially, we used thematic framework analysis (Figure 1) to develop an overarching conceptual model based on conceptual models generated during workshops and refined using workshop discussion notes. 31 The preliminary conceptual model was a diagrammatic representation of the mid-range programme theory, describing the contextual assumptions, interventions and outcomes influencing EPaCCS implementation, alongside areas of uncertainties surrounding these. 32 Thematic framework analysis allowed an overarching synthesis of all data, but could not capture the granularity, nuance (‘real life’ messiness) and divergence within the data. This was evident when we started to chart, describe and interpret data (steps 5 and 6, Figure 1). To embrace these complexities, we engaged in ‘thinking with theory’, drawing on multiple theoretical lenses to produce different knowledge and ways of thinking.33,34 We identified the Non-adoption, Abandonment, Scale-up, Spread and Sustainability (NASSS) framework 35 as offering explanatory power that supported the development of a rich and situated narrative, accommodating data from conceptual models, scribe discussion notes and researcher field notes. The NASSS framework consists of seven domains (health condition, the technology, the value proposition, the adopter system, the organisation(s), the wider system and changes over time). It was used deductively to categorise and explain the nuances and divergences in views regarding different elements of our conceptual model. Our conceptual model evolved iteratively through multiple research team discussions over two months, drawing on findings and experiences from earlier phases of the research project,16,36,37 and combining findings aligned to the NASSS framework. From this, we developed an initial mid-range programme theory. This sought to convey the contextual assumptions, interventions and outcomes of EPaCCS.22,38
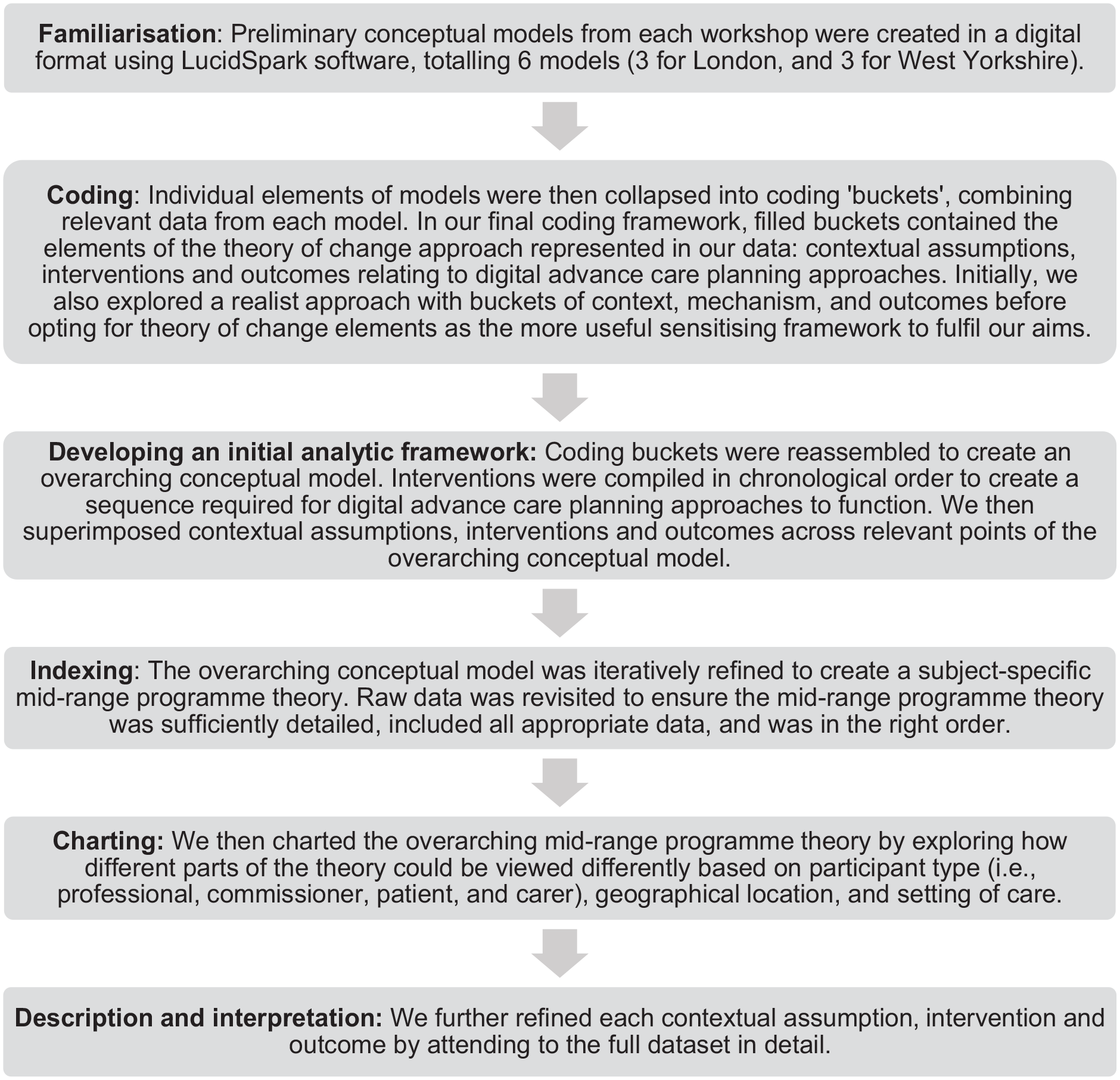
Steps followed during thematic framework analysis.
We adopted a relativist approach to rigour. 39 We used contemporaneous methodological discussions on rigour and lists of quality criteria and techniques. 40 We made informed choices in selecting criteria and techniques that were most applicable to the context, aims and design of this study39,41 (Appendix B lists quality criteria and how they were met). A sub-sample of four patient and carer participants acted as ‘critical friends’ during analysis, discussing developing analyses, providing alternative interpretations of the data and ensuring the conceptual model (representing our mid-range programme theory) was an accurate reflection of participants’ accounts.
Results
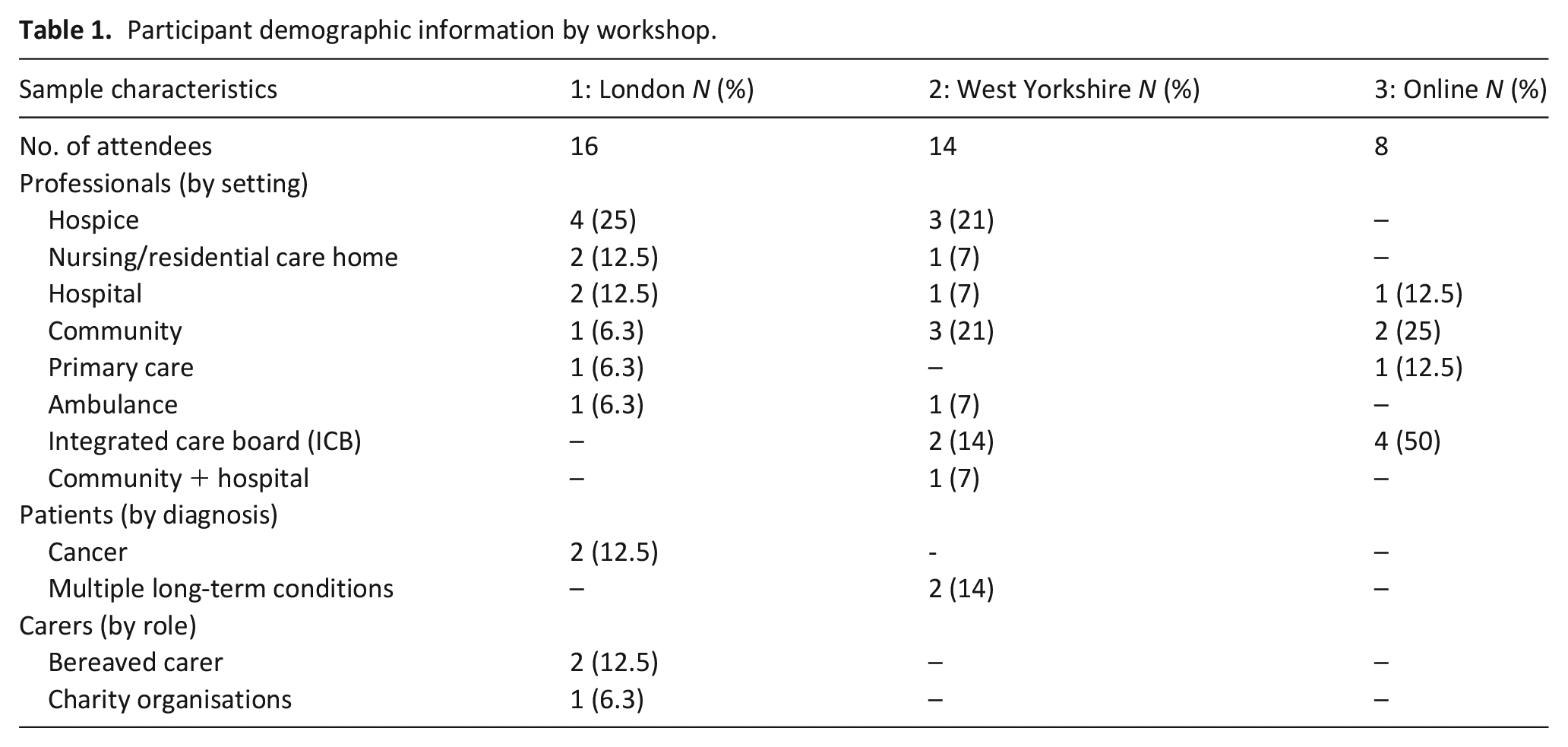
Across the three workshops, we recruited 38 participants (Table 1). In workshops 1 and 2, 53.3% of recruits had participated in the preceding study phases.
Participant demographic information by workshop.
Mid-range programme theory
A mid-range programme theory is presented in Figure 2, providing a graphical representation of the different elements required for digital advance care planning systems to achieve their short-term impact. The mid-range programme theory comprises five components: sociocultural, technical and structural prerequisites; recognition of clinical need for conversation and digital advance care planning; having conversations and documenting decisions; accessing, actioning and amending; and using data to support evaluation, use and implementation.
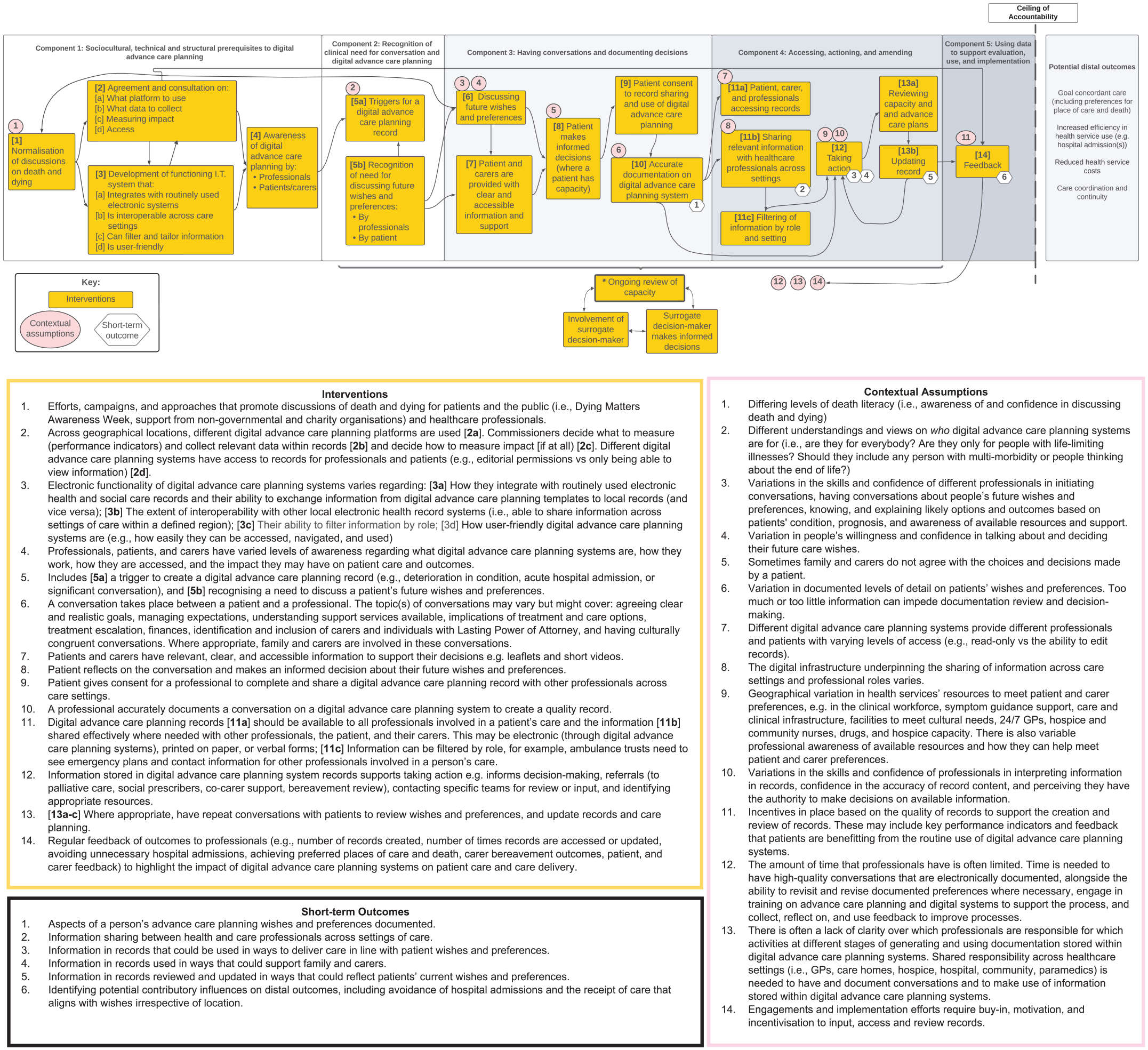
Mid-range programme theory depicting the contextual assumptions, interventions and outcomes influencing digital advance care planning implementation.
Alignment with the NASSS framework
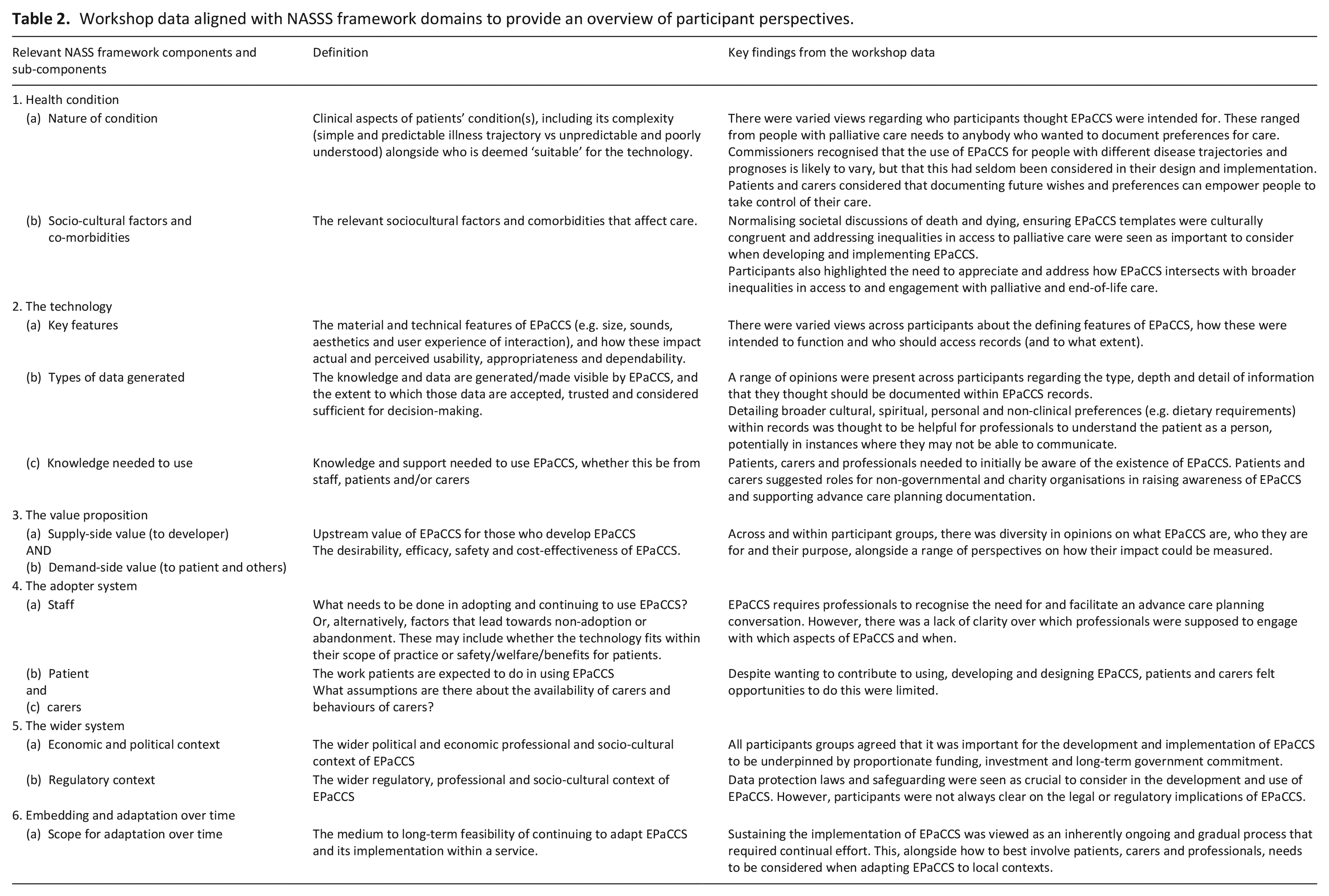
We aligned our findings with the domains of the NASSS framework (Table 2).
Workshop data aligned with NASSS framework domains to provide an overview of participant perspectives.
Health condition
Nature of condition
Participants had divergent views on who EPaCCS are intended for. Commissioners and professionals generally saw EPaCCS as intended for people with life-limiting illnesses and/or palliative care needs, regardless of prognosis. Patients and carers had varied and broader views on who EPaCCS are intended for and included people with severe mental health conditions and those with long-term physical conditions (e.g. people with sickle cell disease). Some patients, carers and professionals suggested that EPaCCS were relevant for anyone who wanted to document their preferences for care (regardless of any diagnosed illnesses) and supported an ‘opt-out’ approach in which everybody is given an EPaCCS unless they state an explicit preference not to have one.
Sociocultural factors
Participants broadly agreed that normalising discussions of death and dying (in society and across health and care) was important in supporting relevant discussions and EPaCCS implementation. Some patients and carers suggested that diverse community groups could play a role by providing information on EPaCCS at critical points in people’s lives (e.g. when creating advance funeral plans, writing a will and recording Lasting Powers of Attorney). Commissioners highlighted the importance of ensuring underserved groups can have their preferences discussed, documented and acted on. Patients and carers highlighted the need for EPaCCS templates to be culturally congruent by including information on cultural and religious elements of their care.
The technology
Key features
The meanings that participants attributed to EPaCCS and their intended purpose varied markedly. For some professionals, EPaCCS represented an electronic form that simply replaced paper-based records. For others, EPaCCS had the potential to transform how professionals communicate with and share information about patients. This lack of clarity contributed to difficulties in differentiating EPaCCS from other initiatives (e.g. ReSPECT 42 documentation, and disease-specific care plans). Most participants agreed that EPaCCS should be accessible to all professionals involved in the care of patients (including general practitioners, community nurses and allied health professionals, social care staff, palliative care teams, hospital teams and paramedics). Patients and carers wanted access to their EPaCCS record. However, views varied on the level and type of information that should be accessible to carers and the extent to which records should be editable by patients.
Types of data generated
There was a range of opinions regarding what data should be documented within an EPaCCS record. Patients and carers were concerned that records could be overly focussed on physical (condition and symptoms), medical (e.g. medications, treatment plans and DNACPR decision) and clinical (e.g. contact information for professionals and services involved in care, preferred place(s) of care and death) aspects of care. They felt information within a record should be detailed and holistic, including broader cultural, spiritual, personal and non-clinical preferences (e.g. dietary requirements). Including caregiver information in records was deemed important but there were concerns regarding what and how much information about the caregiver could be included. In contrast, professionals (including paramedics) considered that records should be concise, enabling fast access to information in an emergency.
Knowledge needed to use
Health and care professionals, patients and carers must understand what EPaCCS are, how they work, how they can be accessed, how to use them (e.g. document, revise, update and share information) and potential impacts on patient care and outcomes. Patients and carers suggested roles for non-governmental and charity organisations in raising awareness of EPaCCS.
The value proposition
Demonstrating the benefits of EPaCCS on patient care was considered essential for health and care professionals to dedicate the necessary time and resources required to use them. However, there were mixed perspectives between and among patients, carers, professionals and commissioners on what the intended benefits of EPaCCS were, for whom and how their impact could be measured. Commissioners saw EPaCCS as a tool for ‘soothing the system’ and managing resources, including reducing emergency hospital admissions to relieve pressures on the acute system. Health and care professionals identified additional benefits, including prompting conversations on wishes and preferences, providing a template to guide advance care planning and informing decision-making in crises and emergencies. Patients and carers spoke of the value of EPaCCS in supporting personalised goal-centred care, as opposed to its impact on service delivery.
The adopter system
For staff
For professionals, ‘wrap-around’ work (i.e. activities related to, but not directly involving, EPaCCS) is needed for EPaCCS to impact on patient outcomes. This includes having conversations about preferences for care (as in Figure 1). Participants suggested that any professionals seeing patients for routine, urgent or inpatient care should be able to access and edit records. Ensuring access for all professionals was seen as a way of reducing duplication of effort and flexible use of systems (e.g. enabling emergency services access to view records and alert other health and care professionals to review a record).
For patients and carers
There were disconnects within the patient and carer participant group about what they were permitted to contribute within the current system. All patients wished for access to their own EPaCCS records. All believed that patients should have access to their own EPaCCS record. For some, this was limited to viewing their records, while others wanted to be able to edit their preferences. Many patients wanted to use EPaCCS to trigger conversations with professionals by requesting appointments to discuss, review and update their preferences. Patients and carers wanted to be involved in the future development of EPaCCS (for example, through patient and public involvement). This included being consulted on information contained within records and access.
The wider system
Economic and political context
All participant groups highlighted that long-term investment was needed to raise public and professional awareness of EPaCCS, further develop information technology systems so that they are functional (i.e. accessible, interoperable and easy to use), and train professionals in integration of EPaCCS within routine care. Some participants felt a national (rather than piecemeal) solution – that is, a universal EPaCCS platform that works across all care settings – was needed. Initiatives to increase professional engagement (particularly non-palliative care professionals) in advance care planning and use of EPaCCS were proposed.
Regulatory context
Participants recognised the importance of legal, ethical and regulatory frameworks governing data collection and protection, documentation, levels of access, data ownership and data security. However, participants across all groups were uncertain about the legal status of EPaCCS records (i.e. if the information within records was bound to any laws). Commissioners queried how EPaCCS related to and differed from other end-of-life plans (e.g. living will, ReSPECT planning documentation and Lasting Power of Attorney). Some professionals expressed concern about their lack of clarity regarding the legal and regulatory implications of EPaCCS.
Embedding and adaptation over time
Scope for adaptation over time
There was an appreciation, especially amongst commissioners, that promoting professional engagement with EPaCCS required considerable effort in return for slow shifts in clinical practice and culture. Geographical differences in types of EPaCCS led to suggestions for locally tailored implementation plans. These could adapt how EPaCCS are used when changes in organisations are made (e.g. during the introduction of new services), and being able to extract and use data from EPaCCS records to monitor and improve care. Integral to the adoption of EPaCCS over time was professional, patient and carer engagement to understand what works, what does not and what needs to change for EPaCCS to function better for each of these groups.
Discussion
Main findings
This study contributes a mid-range programme theory that outlines contextual assumptions, interventions and outcomes influencing the implementation of digital advance care planning systems. The theory draws upon the NASSS framework and captures granular and divergent views of patients, carers, health and care professionals and commissioners to enrich understanding of digital advance care planning system implementation, including the technological infrastructure and human factor influences. Participants from professional groups understood the value of digital advance care planning systems primarily in terms of service delivery and clinical decision-making, including achieving the preferred place of care and death, reflecting existing research and policy. 12 Patients and carers considered additional, broader, aspects such as symptom management, not receiving unwanted medical interventions, family and carer support (including through bereavement), maintaining social ties and achieving a ‘good death’.
What this study adds?
We identify five components of digital advance care planning that can support implementation and evaluation. The proximal, process-related outcomes may be simpler to quantify (e.g. whether a record is documented or updated, and how many times a record is accessed). However, we are reticent to hypothesise links between proximal process-related outcomes and more distal outcomes related to care quality (e.g. achieving a preferred place of care or death, delivering care in line with wishes and preferences, avoidance of hospital admissions). This aligns with earlier theory of change approaches exploring advance care planning in nursing homes, similarly narrowed to proximal outcomes. 43
Digital advance care planning approaches are an emerging area of practice internationally. 8 Further research that determines whether digital advance care planning systems are effective in achieving patient-centred outcomes is essential. The widespread variation and unstructured evolution of such systems 16 may contribute to divergence in views on their purpose and intention. Changing work practices and evolving technology systems could create a context in which unintended consequences (e.g. care delivered that does not align with a person’s wishes due to inaccessible, outdated or inaccurate information) arise. 44
Strengths and weaknesses
This study is the first to integrate the perspectives of patients and carers, alongside healthcare professionals and commissioners, to understand the contextual assumptions, interventions and outcomes that influence the implementation of digital advance care planning approaches. Participants were recruited across two major regions of the UK, representing a diverse range of experiences as well as several different digital advance care planning systems. Our novel pluralistic approach adopts a theory of change approach, supplemented by the NASSS framework. Approaches combining a theory of change approach with complementary theoretical frameworks have been used previously to develop palliative care-based interventions. 45 We chose a theory of change approach over alternatives such as realist evaluation, we found it was better suited for explicating implementation theory for the purpose of improvement and development of robust monitoring at a macro programme level. 46 Our mid-range programme theory provides a novel understanding of digital advance care planning, alongside the complexities, nuances and conflicts regarding their implementation. The depth and detail of study findings provide a strong foundation for naturalistic generalisations to be made to other contexts in which digital advance care planning approaches are being used (e.g. MyHealthRecord in Australia and online patient portals in the USA 47 ). However, we recognise that programme theory is developed iteratively, and the existing mid-range programme theory may be further refined in future work to incorporate additional elements, including indicators and rationale, and greater linkage of intervention activities and outcomes.
Study findings were reviewed and discussed with a sub-sample of patient and carer participants to ensure the representation of participants’ perspectives. However, settings were geographically limited, it was not possible to involve all key stakeholder groups, and the full extent of experience of using digital advance care planning systems may not be reflected in the data. The use of the NASSS framework helped identify and understand uncertainties and interdependencies but orientated the reporting towards a problem rather than a solution-focussed narrative.
Conclusion
The implementation of digital advance care planning systems can be conceptualised in five components: sociocultural, technical and structural prerequisites; recognition of clinical need for conversation and digital advance care planning; having conversations and documenting decisions; accessing, actioning and amending; and using data to support evaluation and implementation. Patients, carers, professionals and commissioners hold varying and sometimes uncertain views on what digital advance care planning system are, who they are for, their purpose and how they should be evaluated. Breakdowns in the technological, infrastructure and human factor influences related to digital advance care planning systems risk undermining the safety and quality of patient care and increasing the risk of unintended consequences. To optimise digital advance care planning system implementation, amendments to technical features of systems must consider wider technological, infrastructure and human factor influences.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241280134 – Supplemental material for Exploring the contextual assumptions, interventions and outcomes of digital advance care planning systems: A theory of change approach to understand implementation and evaluation
Supplemental material, sj-docx-1-pmj-10.1177_02692163241280134 for Exploring the contextual assumptions, interventions and outcomes of digital advance care planning systems: A theory of change approach to understand implementation and evaluation by Andy Bradshaw, Matthew J Allsop, Jacqueline Birtwistle, Catherine J Evans, Samuel D Relton, Suzanne H Richards, Maureen Twiddy, Robbie Foy, Pablo Millares Martin, Sarah Yardley and Katherine E Sleeman in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163241280134 – Supplemental material for Exploring the contextual assumptions, interventions and outcomes of digital advance care planning systems: A theory of change approach to understand implementation and evaluation
Supplemental material, sj-docx-2-pmj-10.1177_02692163241280134 for Exploring the contextual assumptions, interventions and outcomes of digital advance care planning systems: A theory of change approach to understand implementation and evaluation by Andy Bradshaw, Matthew J Allsop, Jacqueline Birtwistle, Catherine J Evans, Samuel D Relton, Suzanne H Richards, Maureen Twiddy, Robbie Foy, Pablo Millares Martin, Sarah Yardley and Katherine E Sleeman in Palliative Medicine
Footnotes
Acknowledgements
The following are members of the OPTIMAL CARE (OPTIMising PALliative CARE through electronic coordination) project group: This includes Dr Matthew J Allsop (University of Leeds), Professor Michael Bennett (University of Leeds), Mrs Jacqueline Birtwistle (University of Leeds), Dr Andy Bradshaw (King’s College London), Mr Paul Carder (NHS West Yorkshire Integrated Care Board), Professor Catherine J Evans (King’s College London), Professor Robbie Foy (University of Leeds), Dr Pablo Millares Martin (Whitehall Surgery, Leeds), Dr Samuel D Relton (University of Leeds, United Kingdom), Professor Suzanne H Richards (University of Leeds), Professor Katherine E Sleeman (King’s College London) and Dr Maureen Twiddy (University of Hull). We thank Dr Hüsna Sarıca Çevik for supporting the conduct and delivery of the regional workshops. We also thank Dr Matthew Mulvey for supporting the facilitation of the West Yorkshire workshop. We also thank Michael H Stone for his helpful feedback and review of the manuscript. We extend particular thanks and gratitude to our patient and public involvement co-applicant, Mrs Barbara Hibbert, who supported the development of project plans, formed our patient involvement group and facilitated inclusive and insightful patient and public involvement group meetings.
Author’s note
Catherine J Evans is also affiliated to Sussex Community NHS Foundation Trust, Brighton, United Kingdom.
Author contributions
MA is the grant holder and Chief Investigator and was responsible for study conceptualisation and development of the study protocol, with critical input from grant co-applicants, SR, RF, MT, KS, CE, PC and PMM. Specific contributions aligned with the Contributor Roles Taxonomy are as follows: A. Bradshaw (Data curation, Formal Analysis, Investigation, Methodology, Project administration, Validation, Visualisation, Writing – original draft, Writing – review & editing); M. J. Allsop (Conceptualisation, Data curation, Formal Analysis, Investigation, Funding acquisition, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing); Jacqueline Birtwistle (Data curation, Formal Analysis, Investigation, Methodology, Project administration, Validation, Writing – review & editing); C. J. Evans (Formal Analysis, Investigation, Funding acquisition, Methodology, Supervision, Validation, Writing – review & editing); S. D. Relton (Formal Analysis, Investigation, Funding acquisition, Methodology, Validation, Writing – review & editing); S. H. Richards (Formal Analysis, Investigation, Funding acquisition, Methodology, Validation, Writing – review & editing); M. Twiddy (Formal Analysis, Investigation, Funding acquisition, Methodology, Supervision, Validation, Writing – review & editing); R. Foy (Funding acquisition, Methodology, Validation, Writing – review & editing); P Millares Martin (Funding acquisition, Methodology, Validation, Writing – review & editing); S. Yardley (Formal Analysis, Investigation, Methodology, Validation, Writing – review & editing) and K.E. Sleeman (Formal Analysis, Investigation, Funding acquisition, Methodology, Supervision, Validation, Writing – review & editing). Artificial Intelligence was not used to generate any portions of the submitted manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the National Institute for Health and Care Research (NIHR) [Health Services and Delivery Research (NIHR129171)]. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. MJA is a University Academic Fellow, funded through a research fellowship from Yorkshire Cancer Research. KES is the Laing Galazka Chair at King’s College London, funded through an endowment from Cicely Saunders International and the Kirby Laing Foundation.
Ethical approval
Ethics approval was sought from the North of Scotland Research Ethics Committee (research ethics committee reference: 21/NS/0046). This study was conducted in accordance with the relevant guidelines and regulations. All participants gave their written informed consent to participate.
Data availability
Deidentified transcripts generated and analyzed during this study are available from the corresponding author on reasonable request.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.