
Abstract
Background:
Palliative care is an essential component of children’s health services but is accessed by fewer children than could potentially benefit.
Aim:
Appraise the evidence to identify factors influencing referral and access to children’s palliative care, and interventions to reduce barriers and improve referrals.
Design:
Scoping review following the six stages of the Arksey and O’Malley framework. Data were charted using an adapted version of the socioecological framework.
Data sources:
CINAHL, MEDLINE, PsycINFO, EMBASE, Cochrane Library were searched for primary studies of any design and literature/systematic reviews. Studies reporting barriers/facilitators and interventions in relation to referral of children with a life-limiting condition to palliative care, in any setting, were included.
Results:
One hundred ninety five articles (primary qualitative and quantitative studies, reviews) were retained (153 reporting barriers/facilitators; 40 interventions; 2 both). Multiple factors were identified as barriers/facilitators: Individual level: underlying diagnosis, prognostic uncertainty, parental attitudes, staff understanding/beliefs; Interpersonal level: family support, patient-provider relationships, interdisciplinary communication; Organisational level: referral protocols, workforce, leadership; Community level: cultural norms, community resources, geography; Society level: policies and legislation, national education, economic environment, medication availability. Most of these factors were bi-directional in terms of influence. Interventions (n = 42) were mainly at the organisational level for example, educational programmes, screening tools/guidelines, workplace champions and new/enhanced services; one-third of these were evaluated.
Conclusion:
Barriers/facilitators to paediatric palliative care referral are well described. Interventions are less well described and often unevaluated. Multi-modal approaches incorporating stakeholders from all levels of the socioecological framework are required to improve paediatric palliative care referral and access.
Only a minority of children and young people who could benefit from palliative care are referred.
When referral to paediatric palliative care does occur, this is often late in the child or young person’s disease trajectory.
The impact of children and young people not receiving palliative care includes unmanaged symptoms, and unaddressed emotional and psychosocial impacts of life-limiting conditions on children and their families.
A synthesis of the evidence from a large number of recent papers describing barriers and facilitators to paediatric palliative care, predominantly from the US and from healthcare professional viewpoints.
Strategies to enhance referrals to paediatric palliative care need to consider individual, interpersonal, organisational, community and societal factors.
A need for studies developing interventions aimed at enhancing referrals to paediatric palliative care to robustly evaluate effectiveness; only one-third of studies reporting interventions evaluated their effectiveness.
An approach that considers all levels of the socioecological framework is required to improve referral and access to paediatric palliative care.
Strategies to improve paediatric palliative care referrals need to be adapted to the context they are intended to be used in.
Education is required to challenge the widely held perception that paediatric palliative care equates to end of life care in order for the benefits of early integration to be realised.
Introduction
There are 21 million children and young people (hereafter ‘children’) with life-limiting or life-threatening conditions (hereafter ‘life-limiting’) worldwide that would benefit from input from palliative care services.1,2
Paediatric palliative care is a total and active approach to care, which aims to address symptom management, and enhance adherence to disease-orientated therapies, advance care planning, holistic family support, end of life care and bereavementt.3–7 Palliative care should be delivered from the point of diagnosis of a life-limiting condition in order to ensure patients and families can fully benefit from improved outcomes. 2 However, only a small number of children who could benefit from paediatric palliative care input are referred, 8 with many referred late.9,10 It is estimated that 90% of children worldwide who could benefit from specialist palliative care never receive it. 1 The impacts of children not receiving palliative care may include poorly managed symptoms and negative emotional and psychosocial effects (e.g. isolation from peers/school and anxiety and distress) on children and their families. Without assessing and addressing these symptoms and concerns, children with life-limiting conditions may not be able to maximise their opportunities in life. 11 Strategies are needed to improve referral and access to palliative care within health systems. 12
Whilst there is a wealth of studies on barriers and facilitators to referral and access to paediatric palliative care, there is currently no clear overview of the existing literature. Existing reviews have focussed on specific populations (e.g. children and families 13 ; health professionals 14 ), conditions (e.g. oncology15,16), settings (e.g. community 17 ; telehealth 18 ), contexts (e.g. countries of high income19–22; countries of lower-middle income23–26), or barriers/facilitators (e.g. professionals delaying discussions 27 ). A comprehensive synthesis of the existing evidence on all life-limiting conditions, stakeholders and contexts is necessary to inform feasible, acceptable and effective mechanisms to address the need for improved access to paediatric palliative care. The aim of this scoping review was to assess the extent and type of evidence in relation to barriers and facilitators influencing referral and access to palliative care for children with life-limiting conditions in their entirety, rather than focussing on one condition, population or context, and for interventions to reduce barriers and improve referrals.
Methods
Study design
A scoping review design was selected to determine the coverage of the body of literature and to identify and map the available evidence. 28 The review was conducted following the six stages of the Arksey and O’Malley 29 framework: (1) identifying the research question; (2) identifying relevant studies; (3) study selection; (4) charting the data; (5) collating, summarising, and reporting the results and (6) consultation with stakeholders. Recommendations by Levac et al. 30 and the Joanna Briggs Institute 31 were incorporated: linking the rationale of the review and research question (stage one); balancing feasibility with breadth and comprehensiveness (stage two); using an iterative team approach to selecting studies (stage three) and extracting data (stage four); considering the implications of study findings to policy, practice, or research (stage five); and incorporating consultation and knowledge transfer with stakeholders (stage six). Reporting follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 32 The protocol was registered on the Open Science Framework (https://osf.io/px38f).
Two consultation workshops with key stakeholders were held during the review process (parents of children with a life-limiting condition [n = 2], charity professionals across the palliative care sector [n = 2], paediatric palliative care consultant [n = 1], and children’s palliative care nurse [n = 1]). Potential stakeholders were identified through existing networks and contacts of the research team. During workshop one, preliminary findings from the review search were presented and feedback was sought on the review process and the collation and synthesis of the data. During workshop two, the final results of the review were presented, and feedback was sought on the interpretation of the findings.
Search strategy
CINAHL, MEDLINE, PsycINFO, EMBASE and Cochrane Library were searched from inception to 16th March 2023. The search strategy included three main concepts: ‘children and young people’, ‘referral and access’ and ‘palliative care’. The full search strategies are reported in Supplemental File 1. ‘Children and young people’ were defined as any individual under 18 years of age in accordance with international 33 and UK 34 definitions of a child. As the terms ‘referral’ and ‘access’ are nuanced and dependent on the specific study and context, the concept of ‘referral and access’ was defined as encompassing the process of professionals offering palliative care, the initial introduction of palliative care services, the utilisation of palliative care (e.g. a patient accessing the palliative care services), and the actual availability of palliative care services. As provision of paediatric palliative care varies within and between countries, we defined ‘palliative care’ as care provided by palliative care services or multi-disciplinary teams with paediatric palliative care training, or services who self-identified as providing specialist paediatric palliative care in any setting. Inclusion and exclusion criteria are shown in Table 1.
Inclusion and exclusion criteria.
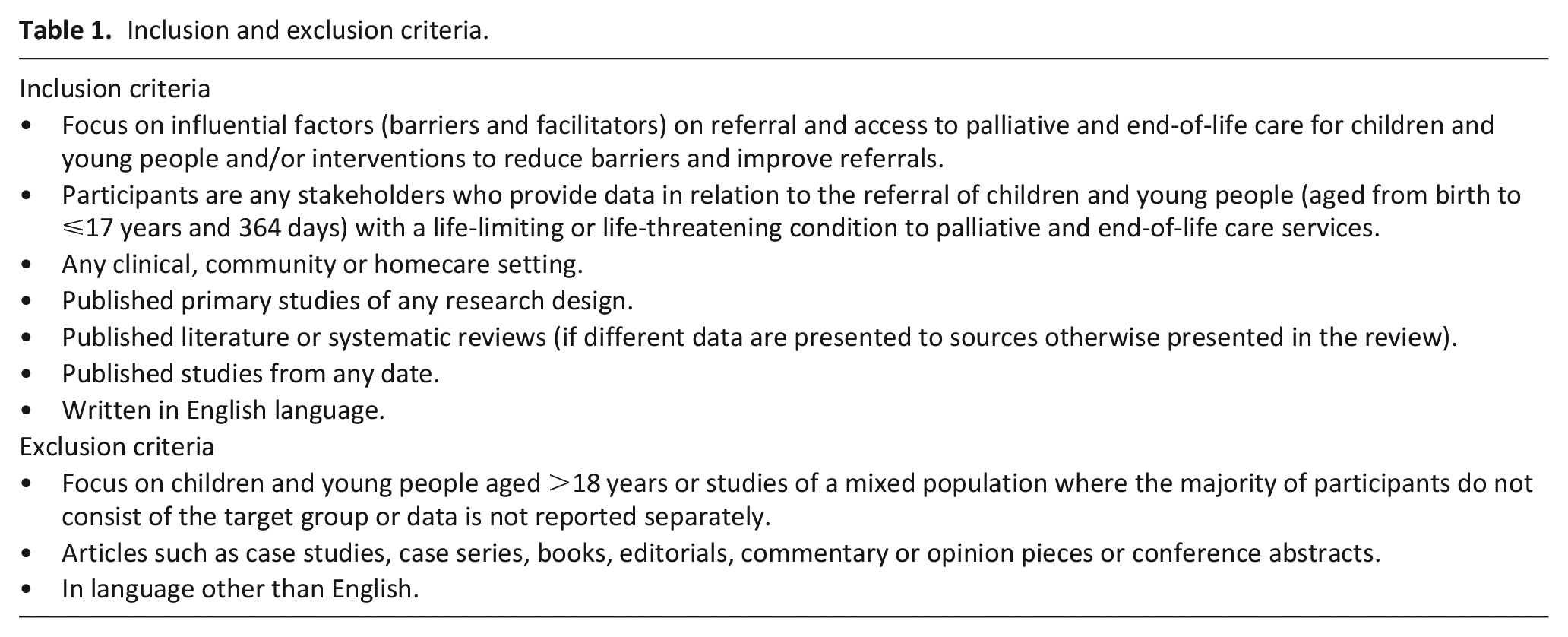
Studies of a mixed population were included if (1) the majority of the participants consisted of our target group or (2) data were reported separately, in which case we reported on the disaggregation for this population (Table 1).
Retrieved articles were imported into Covidence. 35 Titles and abstracts were screened independently by two of three reviewers (PH, JC and LC). Full text review of potentially eligible articles was independently conducted by the same three reviewers. Disagreements were resolved with a fourth reviewer (LF).
Data extraction
Data was extracted by one reviewer (PH) using a data extraction tool adapted from the Joanna Briggs Institute template 31 (Supplemental File 2). Data extraction of 25% of the included articles were verified by a second reviewer (LC). Disagreements were resolved with an additional reviewer (LF).
Collating and summarising data
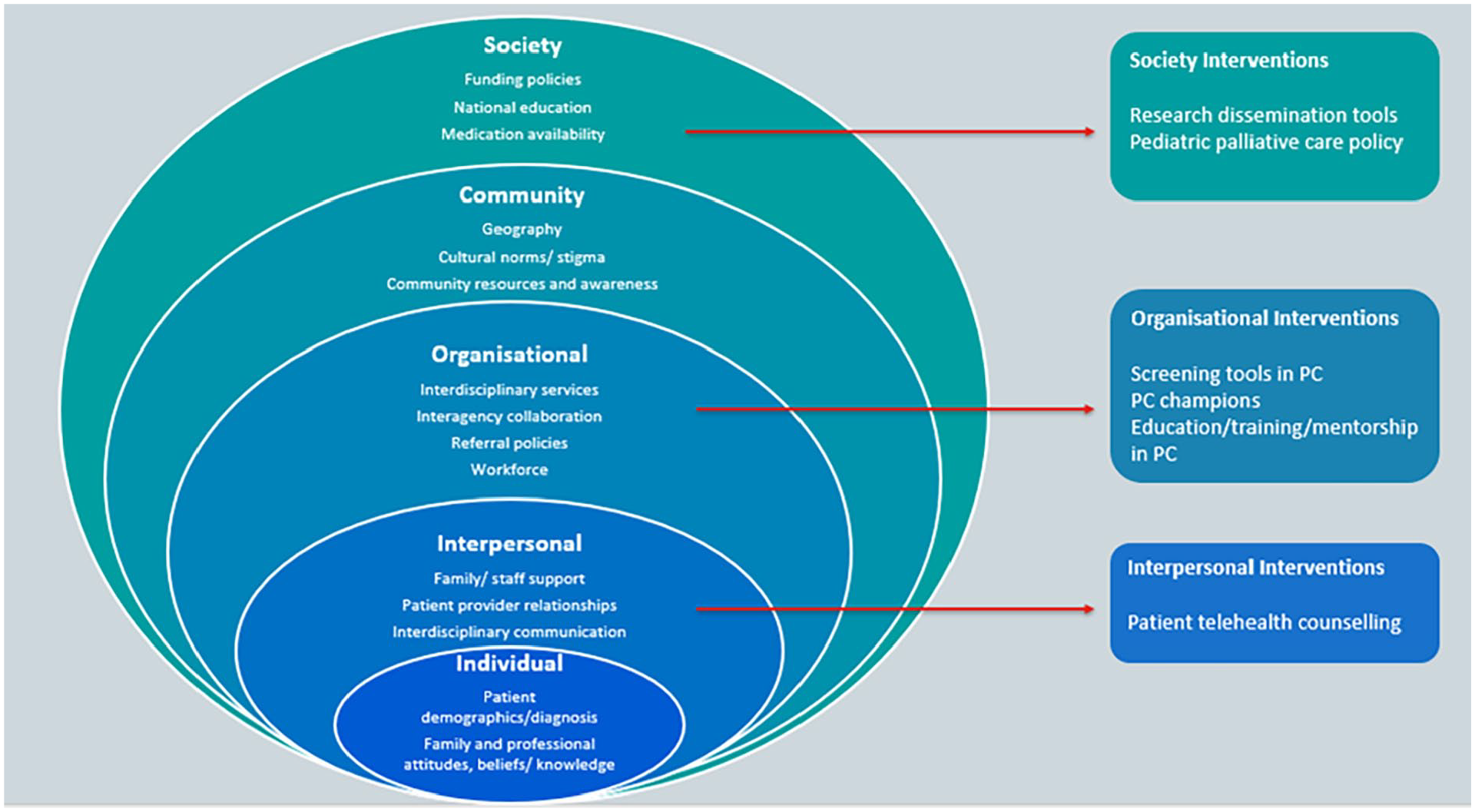
During data collation and synthesis, the authors concluded that the nature of the findings could best be represented and interpreted using an adapted version of the socioecological framework, where patterned behaviour is the outcome of interest.36,37 Extracted data were tabulated into the following levels: (1) Individual; (2) Interpersonal; (3) Organisational; (4) Community; (5) Society. 37 Quality appraisal of papers was not conducted as per Joanne Briggs Institute guidance. 38 National income levels were categorised using The Word Bank classifications. 39
Results
Searches retrieved 12,110 articles. After deduplication, 8,236 papers were eligible for title and abstract screening and 1,064 required full text assessment. A total of 195 papers were included in the review (Figure 1). Full data extraction tables are available in Supplemental File 3.
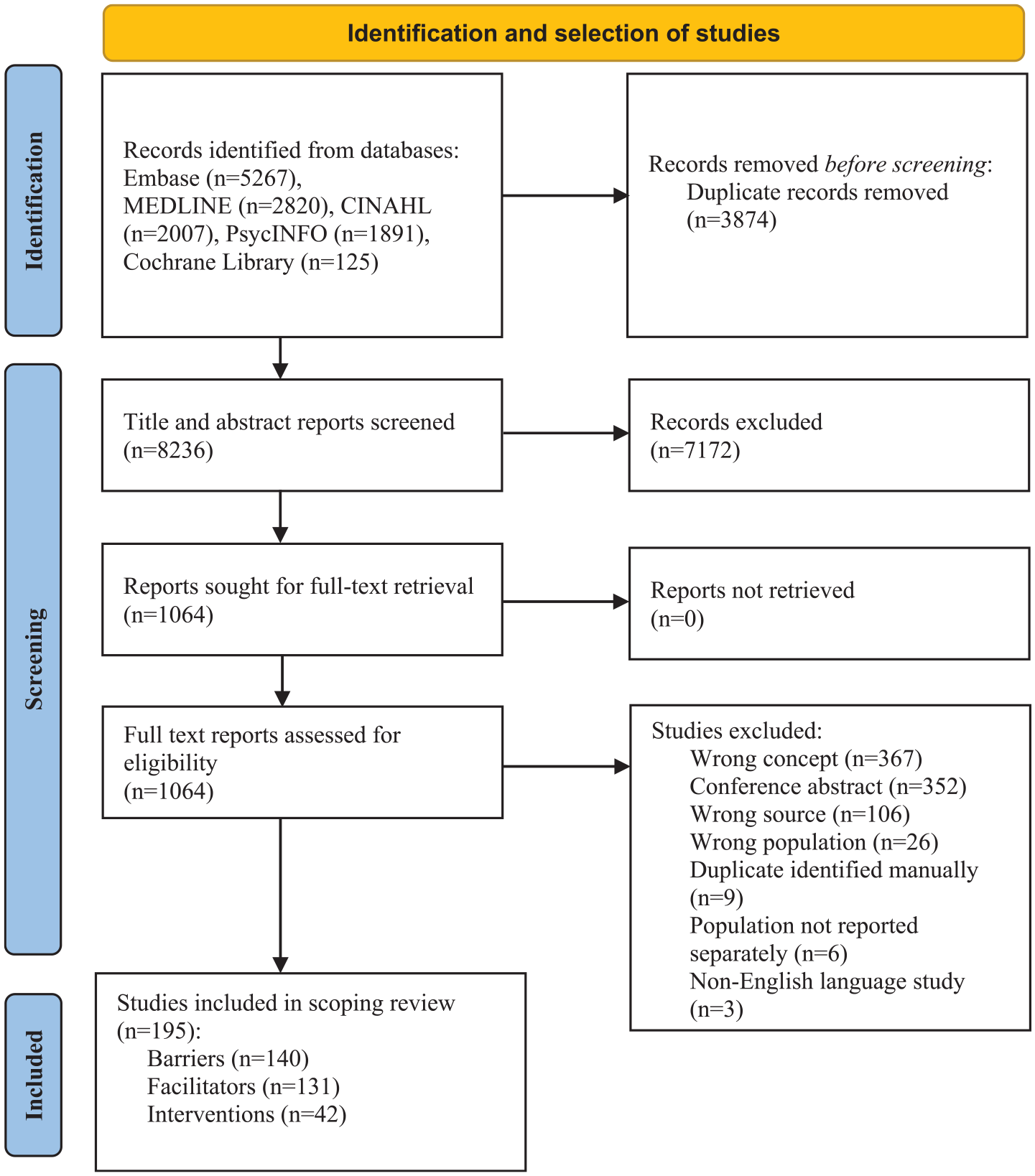
Preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews flow diagram (PRISMA-ScR). 32
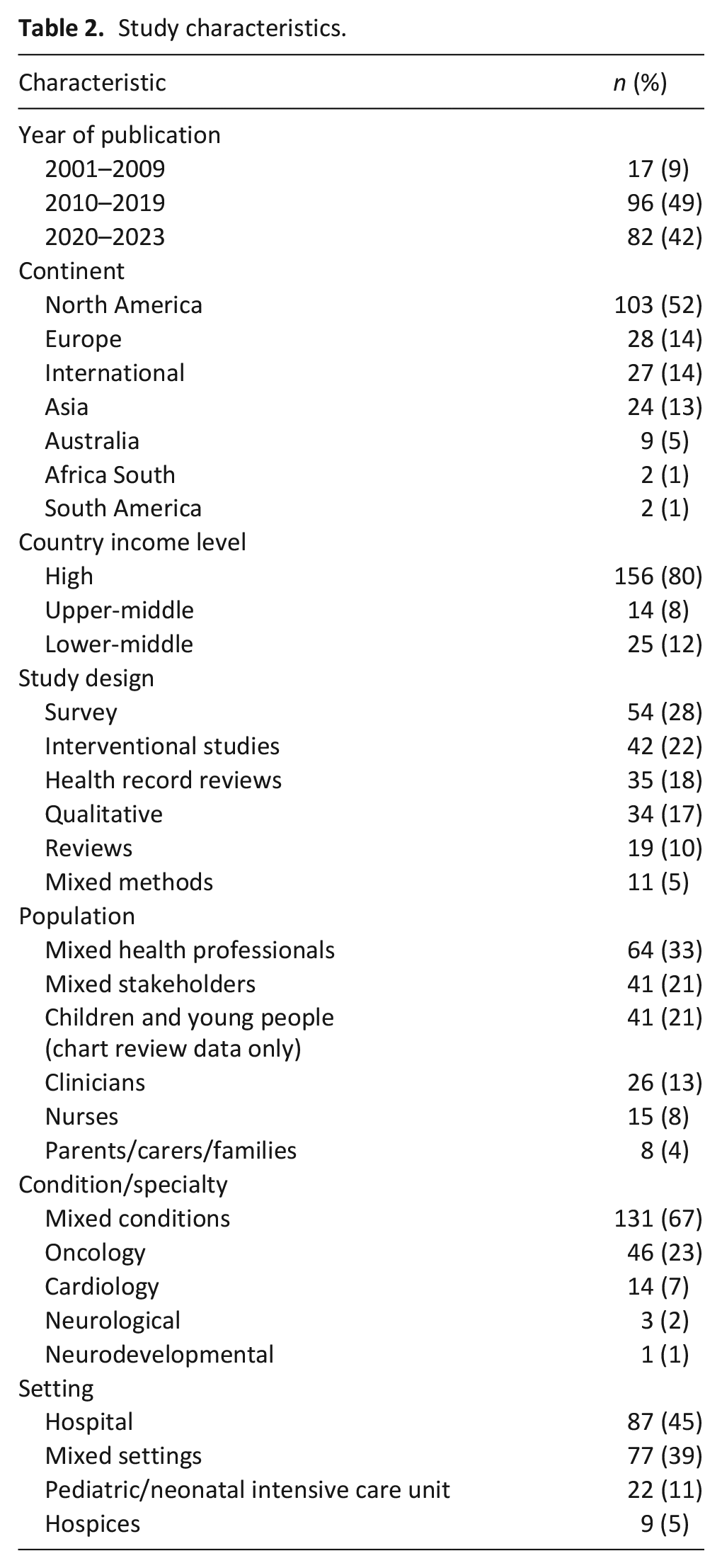
Publication dates ranged from 2001 to 2023, with the majority published after 2010 (91%) (Table 2). Studies originated from 31 countries, with over half from North America (52%),16,17,19,40–139 and the remaining from Europe (14%),22,140–166 Asia (13%),25,167–189 Australia (5%),190–198 Africa (1%),199,200 South America (1%),201,202 or international studies (14%).13–15,18,20,21,23,24,26,27,203–219 Most study participants comprised health professionals (33%), or mixed stakeholders (21%). Only three studies included the views of children.68,154,186 The primary source of data collection was surveys (28%).
Study characteristics.
155/195 articles reported barriers and facilitators to referral and access to palliative care13–27,40–42,44–55,57–65,68–71,73–75,79–84,86–88,90–92,96–99,103,105,107,110–115,117,118,120–127,131–134,136,138–150,153–163,165,167–169,171,173–194,196–199,201,203,205–207,211–219 (Table 3). Contrasting barriers and facilitators were identified at each level of the of the socioecological framework; these are shown in Table 3 and described below.
Key barriers and facilitators to referral and access to palliative care (n = 155 papers).
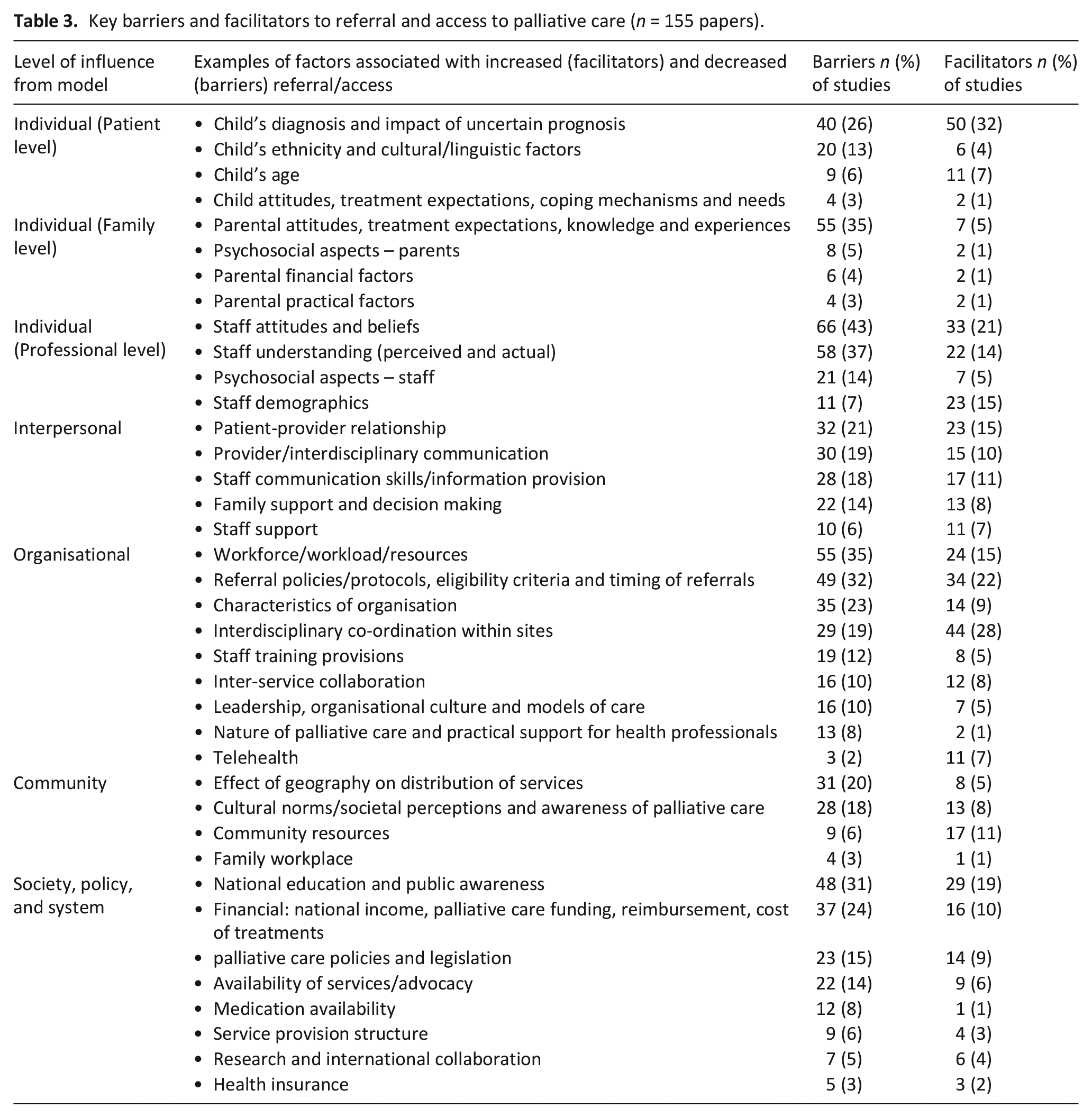
Key differences in barriers to referral and access between countries depending on national income level were identified. Key barriers prevalent in low-and middle-income countries included lack of paediatric palliative care provision or services dedicated to adults which children could access,25,26,206 and poor availability of symptom management medication.26,184,203,206,213 Key barriers in high income countries included need for improved palliative care education,14,16,20,22,23,26,45,48,51,70,81,110,123,140,148,153,160,162,169,174,185,189,190,205,207,211,213,215 and lack of reimbursement20,81,86,88,148,149,160,205,211 and insurance coverage.16,127,145,148,160
Individual level factors
Patient level
Children with non-malignant illness55,148,190 or an uncertain prognosis20,27,42,48,54,75,81,127,153,162,163,207,214 were frequently reported as least likely to be referred to palliative care or were associated with late receipt of palliative care. Multiple, complex and/or chronic conditions,17,44,59,60,65,113,124,155 solid tumour or oncological diagnoses,17,47,71,73,80,83,96,98,126,141–144,168,175,187,190,191,218 and neuromuscular disease17,96,98 were frequently reported as resulting in a referral or early receipt of palliative care. Child’s age17,19,55,59,60,73,83,92,96,98,103,111,141,143,144,191 and ethnicity17,58,86,96,98,141,191 were associated with palliative care access and/or referral, although direction of influence across different age groups and ethnicities was not consistent between studies.
Children’s attitudes including refusal to access palliative care, 45 reluctance to accept new services or healthcare providers, 13 poor acceptance of condition or prognosis 182 and a desire to not be defined by their condition 154 were reported as barriers. In contrast, children’s confidence in the healthcare team 149 and unmet needs (e.g. poor quality of life) 218 facilitated their acceptance of palliative care.
Family level
Parental attitudes and treatment expectations were related to access to palliative care. Specifically, preference for curative treatment/life extending care,16,19,49,54,74,110,127,140,146,154,156,159,171,173,174,188,218 denial of their child’s condition/prognosis,20,64,81,177,211 fear of giving up,53,149,163 mistrust or scepticism about resources/technology,107,131 fear of abandonment/losing contact with healthcare services they know,13,153,205 poor heath knowledge/awareness/misconceptions of prognosis or palliative care13,24,27,49,80,158,162,180,182,184,186,189,190,197,205,207 (i.e. associating it with end of life care 68 ), unrealistic expectations of treatment,14,22,27,81,160,194,211 and a refusal to accept a palliative care consultation44,70 were reported as barriers to access. Recognition/acceptance of their child’s terminal prognosis,17,177 openness to integrating palliative care in the course of treatment 159 (particularly early on 16 ) and a desire to reduce caregiving burden 211 were reported as facilitating factors.
Psychosocial barriers for parents/families included anxiety,22,64 grief,20,171 distress,16,53,149,182 and guilt 176 which could interfere with their decision-making capacity. 22 Practical barriers included parental health problems and physical exhaustion, 197 medical and technical burdens in the domestic environment, 149 and limited family finances/financial burdens86,162,171,190,193,197 including issues with private insurance. 96 Practical facilitators for families included family income, 86 health insurance, 87 and the release of caregiving burden when ceasing curative treatments. 180
Professional level
Professional’s demographics such as role,15,47,53,84,110,122,123,133,138,142,162,188,218 field of specialisation,68,79,165,215 age,47,86,87,122,167,189,215 gender,70,86 ethnicity,47,87,126 and number of years in practice/since graduation15,47,50,86,87,123,138,189 were associated with their experience of referring or delivering palliative care. Direction of influence across these demographic categories was not consistent between studies. Lower levels of formal education24,167 and a lack of skills, knowledge and/or experience16,19,22,27,42,54,71,80,107,110,126,139,162,169,185,187,190,197,203,214,217 were reported as barriers.
Staff attitudes and beliefs such as fear of undermining parental hope and increasing parental anxiety,40–42,45,61,63,79,86,105,110,125,196,207,214,215,218 perceived lack of palliative care value/prioritisation of curative treatment,20,27,44,48,50,61,75,105,111,173,178,180,181,183,184,189,190,213,218,219 misunderstanding of what palliative care offers and/or when to offer it,24,45,46,64,163,165 unease/personal attitudes about dealing with death14,48,146,160,162,178 and negative attitudes towards opioids26,213 were reported as referral barriers. A favourable perception of palliative care,40,41,46,48,53,63,111,125,146,149,162,163,165,173,188,189,216 a sense of privilege/fulfilment in providing palliative care,15,180,211 and contributing to the child and family’s wellbeing140,150 facilitated referral.
Psychosocial barriers to professionals referring and providing palliative care included emotional response/burden,48,125,139,140,149,156,178,180,196,219 work stress,14,15 trauma,14,146,173,183 sense of personal failure,140,173,211 embarrassment, 15 fear, 180 anxiety,14,64,211 grief,15,196,205 poor perceived competence/confidence15,81,91,118,122,123,140,148,149,165,184,188,207,211 and impact on personal life. 15 Conversely, positive coping skills such as resilience, 150 self-care strategies,15,123 avoidance of negative emotions, 189 and handling of uncertainty, 27 as well as high perceived competence/confidence40,48,81,118,165,184,188,203,211 and a willingness to participate in palliative care training 149 facilitated the referral or delivery of palliative care.
Interpersonal level factors
Support for family and staff
For families, a lack of psychosocial,71,148,158,185 practical 82 and bereavement support,203,205 as well as familial conflict/lack of inter-familial communication/social isolation15,27,42,49,54,148,160,171,176,182,197,211 hindered palliative care access. Emotional or practical support for parents and siblings from family, peers, social networks, community organisations or providers were reported as facilitators.17,44,62,81,107,125,161,176,179,187,189,196
For professionals, lack of emotional/psychosocial,15,27,156,160,185 bereavement 205 and logistical support, 15 professional counselling145,174 and supervision 145 were reported as barriers. Provision of clinical supervision,140,160 peer support, 15 reflective practice 205 and consistent provision of counselling and support systems for professionals48,81,146,189 were facilitating factors.
Staff communication skills and the patient-provider relationship
The importance of effective communication (patience, compassion and a flexible and honest approach) in order to facilitate children’s access to palliative care was reported.17,81,125,147,148,150,177,187,196,205,211 Poor communication between families and staff (i.e. individual communication skills/style,15,48,61,75,181,203 anxiety/discomfort around discussing palliative care,16,27,50,51,110,147,190,207,211 and the withholding of information160,177,197 were reported as barriers. Conflict and mistrust among families and providers,20,27,42,49,54,63,113,125,136,154,180 as well as insufficient time available to build rapport 150 and limiting the family’s and/or child’s involvement in palliative care discussions13,22,159,171,176 were reported as barriers. Greater familiarity,140,150 trust,13,140,149,154,180 rapport161,184 and collaboration15,146,159,174,183,189 between providers and families were reported as facilitating factors for referral and access. However, health professionals’ personal attachment and involvement with families could also make it difficult for them to offer or provide palliative care.15,27,53,64,75
Provider/interdisciplinary communication
Poor and fragmented communication or collaboration between providers20,51,68,136,140,160–162,181,184,185,211 (e.g. lack of teamwork or trust 15 ), conflicting opinions or approaches,14,48,61,75,110,113,136,177,190,207 and exclusion of staff from decision-making27,42,136,174,177,183 served as barriers to the provision of palliative care. Mutual trust between teams due to repeated interactions over time, 46 the ability to express values, opinions and beliefs,146,189 team problem solving/sharing of responsibility,27,71 and opportunities for communication/discussion15,147,161,180,196 facilitated provision of palliative care.
Organisational level factors
Characteristics of organisation
Issues such as limited access to paediatric palliative care resources,40,41,70,81,82,111,139,167,188,189 bed shortages,140,203,219 unconducive physical environment for paediatric palliative care14,160,174,183,184,194 (i.e. lack of privacy for families178,185,196), inconsistent access to interpreters,91,193 and restrictive visiting hours 177 were barriers to children’s access and referral to palliative care. Larger free-standing hospitals17,132 with fewer caseloads per provider, substantial financial assets, technology, paediatric facilities and medical equipment, 17 as well as a suitable physical environment (i.e. ensuring privacy and comfort) for palliative care48,146,177,180,193 were associated with increased access to palliative care.
Interdisciplinary services, care co-ordination within sites and telehealth
A lack of or poorly integrated/underutilised palliative care services/hospice facilities within institutions was reported as a key barrier,16,45,46,48,51,70,145,205,217 and this was notably worse in paediatric services when compared with adult services.79,211 A lack of respite options,132,190 24-7 access to providers,71,161,190,197 telephone support71,190,219 and home based services145,214 were all negatively associated with access to palliative care. Multi-disciplinary care, including integrated palliative care with paediatric-trained staff,16,17,46,51,111,147,163,180,184 24-7 availability of services,16,17,23,82,125,149,161,176,178,190 presence of nursing coordinators16,190 and home care provision17,19,23,26,111,140,205 were reported as facilitating factors.
Telehealth was shown to both positively and negatively affect access. This included interruption to clinician-family relationships, depersonalisation of care and rushed pacing of information, 131 as well as provider hesitancy as to whether telemedicine delivered equivalent care compared with in-person consultations. 18 Conversely, telehealth was beneficial in creating accessible support131,184 (particularly in remote or rural areas 18 ), enabling participant inclusion with a wider support network,131,196 offering timely communication, 131 and the fostering of familiarity. 131
Interagency collaboration and care and coordination
Many studies reported poor collaboration and partnerships between agencies,16,71,107,147,190,197,207 which could be due to limited opportunities to network, 80 poor awareness from staff,126,148,149 as well as sub-optimal patient data sharing between institutions. 157 Environments with better inter-organisational care coordination across settings including medical, social and community support agencies and services17,21,80,81,161,178,190 and optimised local specialist services 149 facilitated the provision of and access to palliative care.
Referral policies and protocols, timing and eligibility criteria
Lack of palliative care policy/guidelines,15,146,173,189 consultation process guidelines,46,111 and standardised, objective referral criteria/screening tools for palliative care20,24,51,74,82,121,181,184,205 (or those that were rigid, restrictive or inconsistent136,154,196,197) delayed or impeded the initiation of palliative care. Standardised referral tools, guidelines, and protocols,16,46,107,156,184,196,205 as well as policies for automatic consultations, 110 and the documentation of advance care plans73,218 facilitated referral and access.
Workforce, practical support for professionals, leadership, and organisational culture
Palliative care was often described as challenging, complex, and time-consuming with high logistical demands.14,15,20,148,194,205 This was often compounded by staff shortages14,51,54,136,145,156,158,167,169,174,183–185,188,194,197,203,214 (particularly palliative care experts81,111,157,176,190,203,205,216 or paediatric trained staff19,80,127), heavy workload/staff burnout,20,71,113,139,150,154,185,189,207,215 high staff turnover,20,46,178 vague roles and responsibility,15,53,71,161,179,185 no clear lines of authority,15,140,178 lack of support from management,14,22,196,207 staff hierarchy and structural problems,27,107,140,160 lack of administrative support,136,139,178,207 and the unavailability of an ethics committee54,177; all of which were barriers to palliative care. Facilitating factors to palliative care access included the presence of physician/administrator champions, 48 the provision of adequate time to spend with families 48 adequate staff levels,146,197 flexible staffing models, 160 teamwork, 27 specialist palliative care team/experts and programme coordinators,71,80,84,111,136,140,148 clear roles and responsibilities,148,161 strong leadership 196 and institutional buy-in.80,180
Staff training provisions
Staff training and development needs and concerns15,51,64,107,136,146,157,167,181,189,190,196,203 and a lack of mentors 20 within institutions were reported as palliative care access and/or referral barriers. Hospital enrolment for accreditation programmes,132,178 availability of additional training in rural areas, 19 and presence of staff mentors64,196 had positive effects on staff’s experience of offering or delivering palliative care.
Community level factors
Geography
Poor access to and quality of palliative care/hospice services were reported in remote, rural and low-income regions.17,19,20,24,71,80,97,134,148,184,190,196,207 A widespread distribution of patients22,107,156,157,190,203 and logistical issues/limited transport options158,182,186,193,197 restricted the implementation of and access to services. Palliative care tended to be more developed or easier to access in urban or metropolitan areas23,98,212 and areas with better transport facilities. 186
Cultural norms/societal perceptions and awareness
Negative public attitudes,107,158,189,190 limited awareness and understanding of palliative care and its associated terminology,16,22,25,53,71,139,148,160,182,186,190,197,199,207 and societal stigma and prejudice14,71,156,176,180,182,184,185,205 (compounded by the media 194 ), hindered access. Studies reported high community awareness and knowledge of palliative care,16,21,25,71,182,205 the re-framing of palliative care as ‘supportive care’ 79 or ‘symptom control services’, 184 and the provision of education/information resources for communities53,80,148,156,176 as facilitators to access.
Community resources
Inconsistent availability of community-based hospice care,81,158,197,203,217 poor access to medication in the community, 193 and a reduction in charitable donations 190 (or donations predominately allocated to curative care 16 ) were considered to impede palliative care access and provision. The availability of community resources and supports16,98,176,190,196,212,217 including mobile or ‘pop-up’ services,21,156,161 social media outreach, 80 and the use of rural and remote liaison nurses to act as link between treating services and local communities 193 were considered conducive to palliative care access.
Family workplace factors
Unsupportive parental workplace policies such as the lack of/limited paid sick leave, 17 and risk of wage 182 and job losses which had financial and insurance status implications17,176 were barriers to access. Supportive workplace policies such as flexible work hours and paid sick/annual leave 17 were considered conducive to palliative care access.
Society level factors
Financial factors
Low-national income,26,206 a lack of consistent and/or adequate funding mechanisms to establish and maintain palliative care services16,48,71,107,157,190 (or those which were adult-focused 190 ) were barriers to palliative care availability or quality of provision. Many studies reported on the high treatment, referral and consultation costs for palliative care71,176,184,207,214 which were often compounded by a lack of reimbursement20,81,86,88,148,149,160,205,211 and insurance coverage.16,127,145,148,160 Factors including government and state support/funding for palliative care services,16,80,178 financial assistance for families,186,190,217 or reimbursement mechanisms17,160 and adequate private and public insurance coverage16,176 were facilitators to access.
Specific policies and legislation
Studies highlighted a lack of or inconsistent/restrictive national palliative care or pain management policies and regulations,14,20,22,23,25,136,140,157,161,199,205,207,213,217 and a limited legal framework for palliative care71,148,162,185 which impeded access. This was compounded by inadequate support, awareness and advocacy from policy makers.71,156,160,217 Studies reported the presence of state-based models, public policies/guidelines or regional standards for palliative care,17,21,26,80,99,157,190 legal safeguarding 149 and the prioritisation of palliative care by policy makers153,205 as facilitating factors.
National education, core training, public awareness
A lack of formal or national palliative care education or training for professionals was reported as a key barrier14,16,20,22,23,25,26,45,48,51,70,71,81,110,123,140,146,148,153,160,162,167,169,174,177,185,189,190,199,205,207,211,213,215,217 and many studies reported its need and benefit.15,16,21,25–27,53,70,71,80,107,110,148,149,153,160,161,184,189,190,196,205,215,217
Service and medication availability
Essential palliative care medication availability was reported as limited,23,26,71,184,203,205–207,213,214,217 particularly paediatric pharmacy resources. 19 Adequate availability of paediatric palliative care facilities in a variety of settings,48,70,154,184 advocacy networks 212 and access to medication 71 were described as facilitating factors to access.
Service provision structure
Access to palliative care was restricted in areas with no formal structure for provision 217 and a lack of palliative care integration into the primary care system. 199 Access was affected by the conditions of the healthcare system22,23,26,149 and was restricted in areas with a fragmented or insufficient health-care infrastructure.16,24 Adequate infrastructure to integrate palliative care in the health system 176 was a facilitating factor.
Research and international collaboration
A lack of empirical research and evidence base for paediatric palliative care was reported in studies,25,53,157,205 particularly in under-resourced settings which compounded the underestimation of need.24,26 Research on the need for and cost effectiveness of services,21,190,205 integration of evidence-based care, 25 international training collaborations with international experts, 217 and sharing of best practices between countries 212 were key recommendations to facilitate access to palliative care.
Interventions
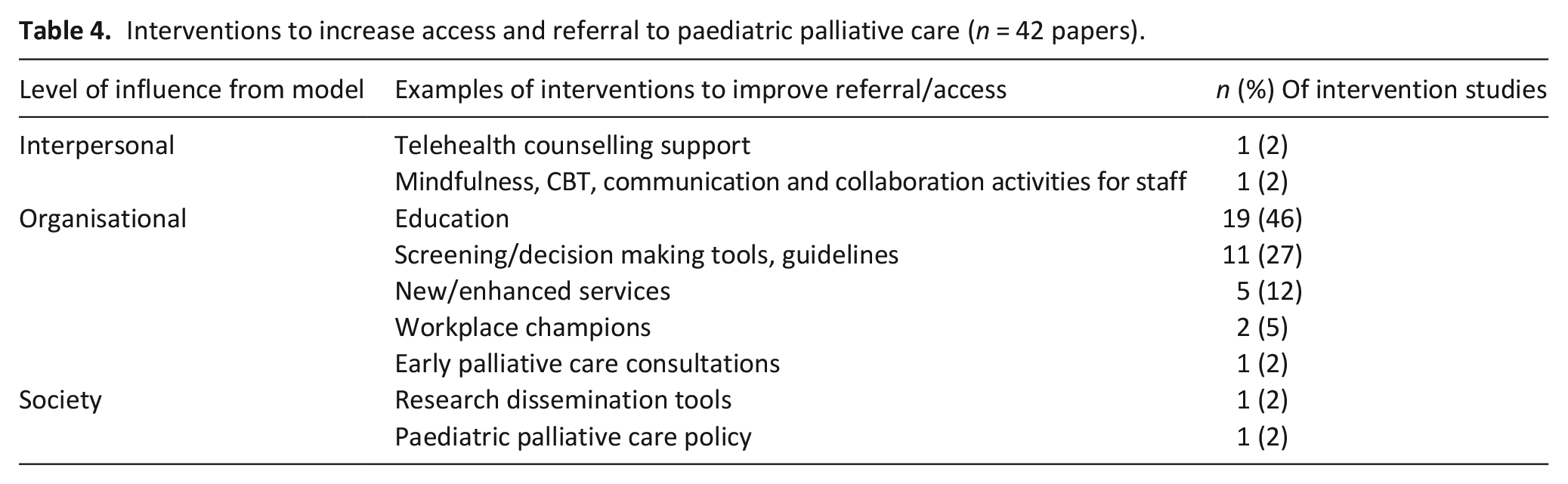
Interventions to improve referral to paediatric palliative care were reported by 42/195 papers43,56,66,67,72,74,76–78,85,89,93–96,100–102,104,106,108,109,116,119,128–130,135,137,151,152,164,166,170,172,195,200,202,204,208–210 (Figure 2 and Table 4).
Interventions to increase access and referral to paediatric palliative care.
Interventions to increase access and referral to paediatric palliative care (n = 42 papers).
Interpersonal level interventions
Interventions at the interpersonal level included a telehealth and counselling service delivered via a hospital-based palliative care social worker. 137 This improved access for patients who would not otherwise have been able to receive this service. Another study used co-design sessions to consider techniques for staff for managing uncertainty and negative emotions. 74 This was based on mindfulness and cognitive behavioural interventions, interprofessional training in palliative care communication, capacities and skills, and team collaboration activities.
Organisational level interventions
The majority of interventions at the organisational level consisted of educational programmes.72,77,78,93–95,108,128–130,135,152,164,172,195,200,202,209,210 For staff this included training courses78,93–95,108,128,129,195,210 toolkits and workshops164,202 lectures, 152 mentorship programmes,172,200 professional development programmes,72,130,209 and care curriculum development.77,130,135 For families, this included informational packets on palliative care. 95 Of these 19 studies, one was unevaluated, 200 13 were shown to increase staff’s self-reported confidence, self-efficacy and/or knowledge in delivering palliative care,72,77,78,94,128,135,152,164,172,195,202,209,210 and only five evaluated the number of palliative care consultations/referrals or hospice enrolment93,95,108,129,130 (four of which showed an increase93,95,108,130).
Other studies described or evaluated new and enhanced services including the integration/expansion of paediatric palliative care programmes,56,89 paediatric palliative care clinics, 119 ‘supportive care clinics’, 43 and palliative care teams into multidisciplinary services. 166 The integration of palliative care champions to improve the provision of paediatric palliative care were discussed in two studies,66,106 although neither evaluated the effectiveness of this on referrals. Other studies described the establishment and/or evaluation of referral protocols, standard recommendations, screening scales and decision-making tools for health professionals to assess palliative care needs in children,76,85,100,116,151,170,204 as well as standard recommendations for paediatric palliative care and consultation guidelines.67,101,104,109 Another study focussed on early palliative care consultations, 102 which was shown to be acceptable to families although it was unclear if number of referrals increased.
Society level interventions
Interventions at the society level included a paediatric palliative cancer care advocacy tool aimed at enhancing dissemination of research findings regarding palliative care integration for children with cancer, although its direct impact on access to palliative care services was not tested. 208 Another study in the US examined the effect of a palliative care policy on hospice utilisation for children and their families residing in paediatric policy counties relative to those who did not. 96 No effect on hospice enrolment was found, although, the policy was positively associated with length of stay in hospice care.
Of the 42 interventions reported, 17 (36%) were evaluated and either shown to positively impact receipt of paediatric palliative care or number of consultations/referrals43,56,66,67,76,89,93,95,101,108,109,116,119,130,137 or have no impact on number of consultations/enrolment.96,129 15 (33%) were shown to improve professional’s confidence, awareness and understanding of paediatric palliative care72,77,78,85,94,104,128,135,152,164,172,195,202,209,210 and 10 (31%) did not measure impact on receipt of paediatric palliative care or provider experience of referring or delivering palliative care.74,100,102,106,151,166,170,200,204,208
Discussion
Main findings
This review has identified a large volume of literature describing barriers and facilitators associated with referral and access to paediatric palliative care.13–27,40–42,44–55,57–65,68–71,73–75,79–84,86–88,90–92,96–99,103,105,107,110–115,117,118,120–127,131–134,136,138–150,153–163,165,167–169,171,173–194,196–199,201,203,205–207,211–219 In line with the socioecological framework, which recognises that interactions between individuals and their environment are reciprocal, this review found multiple contrasting and interlinked barriers and facilitators across every level of the framework. Most of these findings come from professional views and opinions rather than direct report from parents or children themselves.
There was a much smaller body of literature describing interventions to address these barriers,43,56,66,67,72,74,76–78,85,89,93–96,100–102,104,106,108,109,116,119,128–130,135,137,151,152,164,166,170,172,195,200,202,204,208–210 with few evaluating impact on receipt of paediatric palliative care or number of consultations/referrals.43,56,66,67,76,89,93,95,96,101,108,109,116,119,129,130,137
What this study adds
Key differences in barriers and facilitators associated with referral and access to paediatric palliative care were found between national income level. Findings prevalent in high income countries included need for improved palliative care education,14,16,20,22,23,26,45,48,51,70,81,110,123,140,148,153,160,162,169,174,185,189,190,205,207,211,213,215 and lack of reimbursement20,81,86,88,148,149,160,205,211 and insurance coverage.16,127,145,148,160 Most research was conducted in the US,16,17,19,40–67,69–78,80,81,83–93,95–118,120,124–132,136–139 a country which has a healthcare system reliant on health insurance coverage. Many healthcare plans exclude supportive services often required in paediatric palliative care such as psychosocial support and respite. 16 Home visit provision is often capped, meaning palliative care is mainly provided in the inpatient setting. 16 Within many other high income countries healthcare is state funded, and provision of non-medical support services and home care is more widespread. This review also highlighted issues prevalent in low- and middle-income countries. These include lack of any paediatric palliative care provision or services dedicated to adults which children could access,25,26,206 and poor availability of symptom management medication.26,184,203,206,213 Therefore, strategies to improve paediatric palliative care referrals may need to be developed within the resources available in the setting they are intended to be used in. Lower cost strategies developed with those from low- and middle-income countries may also be useful in high income countries.
Many of the barriers and facilitators to paediatric palliative care identified in this review were related to underlying diagnosis,17,22,40,41,47,52,57,59,60,62,65,69,71,73,80,83,96,98,99,111,112,126,133,134,141–144,155,159,175,187,190–192,218 prognostic uncertainty,20,27,42,48,54,75,81,127,153,162,163,207,214 and parental expectations of care outcomes such as preference for curative treatment or life extending care.16,19,49,54,74,110,127,140,146,154,156,159,171,173,174,188,218 Children with certain diagnoses, such as solid tumours,17,83,175,187,218 multiple complex or chronic conditions17,44,59,60,65,113,124,155 and neuromuscular disease17,96,98 were more likely to be referred or access palliative care, presumably due to more certainty regarding prognosis. Development of referral guidelines and policies relevant to individual settings may be beneficial to allay some of this uncertainty regarding referral. Previous research with parents of children with a cancer diagnosis identified that parents do not see curative and symptom-directed supportive care as mutually exclusive. 220 This review found that parental openness to integrating palliative care in the course of treatment facilitated acceptance of palliative care. 159 Our findings support this notion that children and families with life-limiting conditions should be offered a dual approach to care, whereby palliative care is received alongside disease-focussed management. Palliative care should be integrated early for all children identified as having a life-limiting condition, and parallel planning should occur. 221 By taking this approach professionals can be less concerned with prognostic uncertainty and more children that could benefit from paediatric palliative care would receive it.
This review also found that staff beliefs and attitudes to paediatric palliative care impacted provision and access.13–16,24,26,27,40–42,44–46,48,50,53,61,63,64,68,74,75,79,86,88,91,105,107,110,111,113,118,121–123,125,133,136,138,140,146,149,150,153,156,158,160–163,165,173,174,178,180,181,183–185,188–190,194,196,207,211,213–219 Previous research has shown that professionals tend to equate paediatric palliative care with non-curative treatment, rather than as a dual approach to care as described above. 222 The findings of this review support previous research that paediatric palliative care is often equated to end of life care,53,163,222 rather than embracing the definition that palliative care should begin at diagnosis of a life-limiting condition.2,223 Our findings also showed that positive health professional attitudes, including a sense of privilege/fulfilment in providing palliative care15,180,211 and a perception of contributing to the child and family’s wellbeing,140,150 facilitated the provision of palliative care. This highlights the need for improved palliative care education at an undergraduate level, as well as ongoing training for paediatric specialists to improve understanding of and attitudes towards paediatric palliative care.
Publication dates of included studies ranged from 2001 to 2023. Despite the evolution of paediatric palliative care since the early 2000s, no clear differences in barriers/facilitators by decade emerged, and barriers identified in earlier studies still persist and are relevant now. Therefore, even though paediatric palliative care services have advanced in recent years, this does not mean they are any easier to refer to or access and thus this is an area of need that still needs to be addressed.
We found a relatively small amount of literature on the development of interventions to increase referral to palliative care for children and young people across the interpersonal, organisational, and societal levels of the socioecological framework.43,56,66,67,72,74,76–78,85,89,93–96,100–102,104,106,108,109,116,119,128–130,135,137,151,152,164,166,170,172,195,200,202,204,208–210 Most of these interventions focussed on educational programmes and professional development72,77,78,93–95,108,128–130,135,152,164,172,195,200,202,209,210 and there was a clear need for more professional education regarding paediatric palliative care. Educational interventions that were evaluated were done so by asking about knowledge relatively soon after the intervention was administered, so it is not known whether this had a long-term benefit. Future studies should focus on feasibility, evaluation and implementation of interventions to ensure they are effective within the context they are intended to be used in. 224 No interventions were identified at the individual or community levels. Future interventions could address the successes identified at these levels including positive parental, child and professional attitudes towards palliative care, improved societal awareness of palliative care and the provision of community resources.
Strengths and limitations of the study
This review was conducted using a registered protocol and following published guidance. All identified studies were screened by two reviewers against inclusion/exclusion criteria and our stakeholder group contributed throughout the review process. Limitations of our study include inclusion of only English language articles, and potentially grey literature searching may have yielded further information. Citation searching was not conducted due to the volume of studies identified.
Conclusions
The barriers and facilitators to referral to paediatric palliative care, especially from the views of professionals, are well described in the literature. There are fewer reports of interventions designed to increase referrals. Future research should focus on intervention development and evaluation that should understand the context in which it is to be delivered, utilise a multi-pronged approach and incorporate robust evaluation of the impact.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241271010 – Supplemental material for Barriers and facilitators influencing referral and access to palliative care for children and young people with life-limiting and life-threatening conditions: a scoping review of the evidence
Supplemental material, sj-docx-1-pmj-10.1177_02692163241271010 for Barriers and facilitators influencing referral and access to palliative care for children and young people with life-limiting and life-threatening conditions: a scoping review of the evidence by Pru Holder, Lucy Coombes, Jane Chudleigh, Richard Harding and Lorna K Fraser in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163241271010 – Supplemental material for Barriers and facilitators influencing referral and access to palliative care for children and young people with life-limiting and life-threatening conditions: a scoping review of the evidence
Supplemental material, sj-docx-2-pmj-10.1177_02692163241271010 for Barriers and facilitators influencing referral and access to palliative care for children and young people with life-limiting and life-threatening conditions: a scoping review of the evidence by Pru Holder, Lucy Coombes, Jane Chudleigh, Richard Harding and Lorna K Fraser in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank all members of the advisory group for their invaluable input into this work and The True Colours Trust [grant number TCT1869] for funding this work.
Author contributions
All of the authors, PH, LC, JC, RH and LF, have made substantive intellectual contributions to the manuscript. PH, LC, JC, RH and LF contributed to the conception and design. PH, LC, JC and LF were involved in literature searching and selection, data extraction and analysis. PH and LC drafted the manuscript, which was then revised critically for intellectual content by JC, RH and LF.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The True Colours Trust [grant number TCT1869].
Ethics and consent
As the study involved only secondary analyses of published data, no ethical approval was required. There are no human participants in this article and informed consent is not required.
Data management and sharing
The review was conducted using data that were already available in the public domain, with appropriate references provided throughout. The full search strategy used in the present review can be found in the Supplemental Material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.