
Abstract
Background:
Patients with serious illness frequently report (temporary) wishes to hasten death. Even until the end-of-life, many patients also harbor a will to live. Although both phenomena are negatively correlated according to some studies, they can also co-exist. Knowledge about the complex relationship between the seemingly opposing wish to hasten death and will to live is limited, but crucial for delivering adequate care and understanding potential requests for assisted dying.
Aim:
To study the correlation of and explore the relationship between wish to hasten death and will to live over 6 weeks.
Design:
Observatory, prospective cohort study following a mixed methods design. Analysis of quantitative (Schedules of Attitudes Toward Hastened Death, a visual numerical scale and (additional) validated questionnaires) and qualitative (semi-structured interviews) data with illustrative case descriptions.
Setting/participants:
Patients receiving palliative care with heterogenous underlying diseases from various care settings, before and after an open conversation on a possible desire to die.
Results:
In n = 85 patients, wish to hasten death and will to live were strongly negatively correlated at three time points (baseline: r(65) = −0.647, p ⩽ 0.001; after 1 week: r(55) = −0.457, p ⩽ 0.001 and after 4–6 weeks: r(43) = −0.727, p ⩽ 0.001). However, visual assessment of scatterplots revealed a small, but substantial number of outliers. When focusing on these outlier patients, they showed clinically relevant changes between baseline and 6 weeks with the wish to hasten death changing in n = 9 (15% of n = 60) and the will to live changing in n = 11 (18.6% of n = 59). Interview data of three outlier cases illustrates unusual trajectories and possible factors which may influence them.
Conclusions:
As they can co-exist in different possible combinations, a high wish to hasten death does not necessarily imply a low will to live and vice versa. Patients receiving palliative care can hold such seemingly opposing positions in mind as a form of coping when confronted with an existential threat of serious illness. Therefore, health professionals are encouraged to proactively engage patients in conversation about both phenomena.
The wish to hasten death is frequent in patients with serious illness and can associated with immense burden, potentially leading to suicidality or a wish for assisted suicide.
Many patients retain their will to live throughout their entire illness trajectory, even in palliative stages and at the end of life.
In some studies, both phenomena are found to be negatively correlated, yet simultaneous expressions of both a high wish to hasten death and a high will to live are possible.
We confirm the negative correlation between the wish to hasten death and the will to live over the observation time of 4–6 week after an open conversation in the group analysis.
However, there was a substantial number of outliers of this pattern with clinically relevant changes in both phenomena
Three illustrative cases show that factors like patient personality and individual situation influence uncommon trajectories of wish to hasten death and will to live.
Clinical and research assessment should be aware of the fact that a wish to hasten death does not necessarily imply a low will to live and vice versa, thus both phenomena should be addressed simultaneously and proactively.
The application of secondary analysis using an integrative mixed-methods-approach of validated questionnaires and in-depth interviews might be effective to reveal the nature of ambiguous or seemingly paradoxical phenomena such as double awareness of wish to hasten death and will to live.
As the double awareness of the wish to hasten death and the will to live is common at the end of life, but can be hard to endure, health professionals should develop an open and accepting attitude to support patients in dealing with it.
Introduction
Confronted with serious and life-limiting illness, patients’ experiences are complex, as they may understand “hope” in a differentiated way or may experience seemingly contrasting wishes at the same time. They may want to be left alone, but do not want to feel lonely or they may wish for impossible therapy outcomes despite a bad prognosis. 1 This phenomenon is called “double awareness,” describing the “capacity to be engaged in the world while preparing for impending death.” 1 Double awareness may explain why patients sometimes ask for exhaustive treatment but at the same time express desire to die should the treatment not succeed. 2
This desire to die is a frequent phenomenon in patients with serious disease with a prevalence of 8.5%–44%.3,4 Desire to die lies on a continuum of suicidal pressure, ranging from acceptance of death, over a hypothetical wish to die and to acute suicidality. 5 On this continuum, the wish to hasten death is an expression characterized by a relatively high pressure to act. 6 It is changeable over time and may arise due to physical symptoms, psychic distress, existential suffering, and social aspects.6,7
Another relevant, but not as comprehensively researched phenomenon that may contribute to double awareness is the will to live. 8 It is defined as a strong natural drive that can persist even in the face of severe suffering. 9 The will to live is changeable over time and can decline in some patients while it remains strong in others. 10
Evidence remains inconclusive how the wish to hasten death and the will to live relate to each other. Some empirical data suggests that they are negatively correlated: a low will to live is associated with a high wish to hasten death and vice versa. 11 This suggests a one-dimensional model with the wish to hasten death on one end and the will to live on the other. Results from Chochinov et al. support this position, finding a significant negative correlation of r = −0.427 in n = 189 patients suffering from advanced cancer. 12 This model generally seems to describe other populations as well. 13 However, we suggest this small correlation cannot suffice as evidence for a one-dimensional conceptualization of the relation between wish to hasten death and will to live. 14 In qualitative interviews with n = 32 patients receiving palliative care, some report a simultaneous will to live and wish to hasten death. 14 Despite their correlation, the authors of this study concluded that the two concepts can vary independently and exist simultaneously. Further studies conceptualize the relationship between wish to hasten death and the will to live in a similar way.15,16 We propose that the idea of “double awareness” might help to account for the simultaneity of wish to hasten death and will to live.
Further research on wish to hasten death and will to live gives insight into their complex relationship: With a high corresponding pressure to act, desire to die can lead to suicidality and a wish for (medical) assisted suicide. 5 However, a desire to die can also designate an acceptance of death or provide the patient with the subjective feeling of being in control. 5 In the context of most diseases, a high will to live is associated with survival and better subjective quality of life. 17 Despite this positive effect, a high will to live might not always be preferable for patients close to death, as accepting death might ease the dying process. 18 With changing legislations regarding (medical) aid in dying in numerous countries world-wide, knowledge about the will to live and the wish to hasten death becomes even more relevant for the assessment of patients receiving palliative care. 19
Within a recent sequential mixed-methods study, we evaluated effects of a proactive conversation about desire to die on patient-reported outcomes including wish to hasten death and the will to live over three time-points as well as within qualitative interviews.20,21 Using a pre-post-design, the desire to die conversation was conducted after the first and before the second assessment point. In this paper, we return to this data for a second analysis to answer the following research questions:
What is the interrelation between the wish to hasten death and the will to live over time? What might constitute different ways in which these two phenomena relate to each other?
Methods
Design and procedure
This paper presents a secondary analysis of quantitative and qualitative data from a prospective three-phase mixed methods cohort study following a pragmatism- and constructivism-based paradigm. Main goal of the study was a pre-post assessment on the effects of proactive desire to die conversations for patients receiving palliative care. 20 As part of a data-based strategy, we integrated qualitative data into our quantitative data, with quantitative data being dominant in this study. 22 For other primary study results, please refer to previous publications.20,23 –26
Population
For the study phase preceding the one reported on in this paper, we aimed to include palliative care providers from different professions and work settings for participation in 2-day trainings based on a clinical approach on dealing with desire to die.20,23
The population of interest for the present paper were patients receiving palliative care with heterogenous diagnoses and settings of care. Inclusion criteria for participation were: (1) adult patients, (2) adequate German language ability, (3) prognosis of death within 3–12 months (assessed by the surprise question: “Would you be surprised if the patient died within the next 3–12 months?” 27 ), and (4) cognitive ability to participate. All patients gave informed consent. For interview participation, a sub-set of patients with insightful experiences was purposefully sampled by the research team.
Setting
All research was conducted within a 100 km radius surrounding the study site in Cologne, Germany. Patient questionnaire assessments as well as qualitative interviews took place at patients’ current place of care, mostly at their home.
Sampling
We followed a convenience sampling strategy for inclusion of patients, 28 aiming for a required sample size of n = 300. For interview participation, a sub-set of n = 15 patients with insightful experiences was to be purposefully sampled by the research team.
Recruitment
For quantitative evaluation, trained palliative care providers were asked to recruit patients from their practice. Upon agreement to study inclusion, patient socio-demographic data and (validated) questionnaires were assessed at baseline (t0). Then the health professional held a single desire to die-conversation with the patient within the next 2 weeks. Two post-assessments followed about 1 (t1) and 6 weeks (t2) later. A sub-set of patients was approached by the research team for qualitative evaluation through semi-structured interviews. 24 All health professionals and patients gave written informed consent.
Data collection
Patient-reported outcomes were assessed at t0, t1, and t2 for evaluating the effect of the single desire to die-conversation held by health professionals. 20 For assessment, members of the research team (KB, KK, among others) visited patients and went through the questionnaires together. As part of these outcomes, wish to hasten death was assessed with the German Schedule of Attitudes Toward Hastened Death (SAHD-D), a validated questionnaire consisting of 20 items with dichotomous true-or-false answers and a score ranging from 0 to 20. 29 The will to live was assessed with a single-item Visual Numerical Scale (VNS) with possible scores ranging from 0 to 10. While the VNS is not a validated scale, it is a common instrument. As other patient outcomes, we collected depressiveness, hopelessness, death and dying distress as well as patient-health professional-relationship through several other validated questionnaires as reported in Table 1. 20
Validated questionnaires used for evaluation of desire to die conversation.
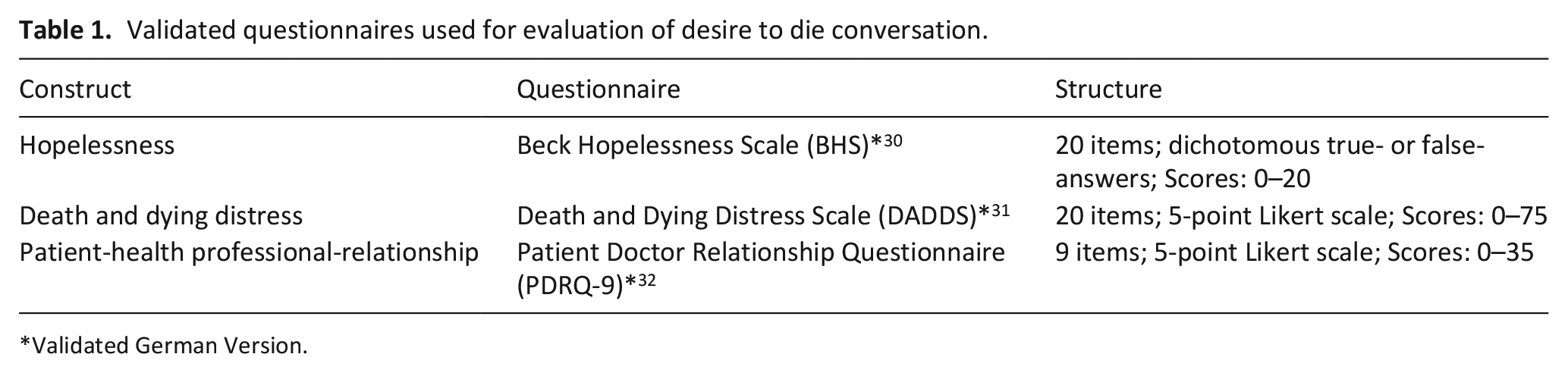
Validated German Version.
After completion of quantitative evaluation, members of the research team (KB, KK, among others) conducted qualitative interviews following a semi-structured guideline. 24 Patients were asked about death, dying, and desire to die communication with their health professionals and relatives. 24
Statistical analysis
After evaluation of the effects of an open desire to die conversation on the patient-reported outcomes mentioned above, 20 we performed a secondary analysis of patient data on wish to hasten death and will to live and consulted further related data (questionnaires on depressiveness, hopelessness, death and dying distress as well as patient-doctor-relationship) in cases of interest.
(1) We established the relationship between wish to hasten death and will to live for all three assessment points by correlation according to Pearson and created scatterplots for each. This enabled us to identify outliers by visual judgment.
(2) Applying cut-off values for both outcomes, clinically relevant frequencies of change between t0 and t2 were calculated descriptively for all patients. Thereby, different directions and intensity of change could be identified.
(3) Based on information from step (1) and (2), three illustrative individual patients from our data were analyzed descriptively as a form of case study regarding wish to hasten death, will to live, related outcomes, and sociodemographic data. For better visualization, we created visual graphs for each case.
SPSS Statistics 25 was used for statistical analysis. 33
Qualitative analysis
As part of our sequential mixed-methods approach, we first re-read the particular interviews of patient cases of interest that were previously identified statistically. Secondly, qualitative interviews underwent a secondary analysis following the data integration strategy of “following a thread” according to Pluye et al. 34 Two authors with experiences in psychology and qualitative analysis (KB, TD) coded interviews to account for patient experiences, life situation, illness trajectory, and attitudes toward desire to die. 24 Through utilizing this mixed-methods approach, we were able to write three rich illustrative case summaries (in form of short case studies) for each patient.
MAXQDA 2022 for management of interview transcripts and coding of data for qualitative analysis. 35
Ethical considerations
In the primary study, numerous measures were taken to avoid bias and unnecessary patient distress. During quantitative and qualitative assessment and interviews, the study topic was presented as “end-of-life communication.” 20 Patients were encouraged to interrupt or end assessments or interviews as well as call afterward, if they experienced any distress at all. Additionally, researchers kept close contact to recruiting health professionals and gave feedback (with patient approval) in cases of potential suicidality. 20 We followed the Declaration of Helsinki and obtained ethical approval from the Ethics Committee of the University of Cologne (#17–265). The study was registered in the German Clinical Trials Register (DRKS00012988; registration date: 27.9.2017). We followed the STROBE Reporting Guideline. 20
Results
Between 04/2018 and 03/2020, n = 49 of trained health professionals invited n = 173 patients for study participation. A baseline assessment was conducted with n = 85 patients. Afterward, n = 29 trained health professionals with an average of 11.6 years (SD = 10.3) of experience held an open conversation about desire to die with n = 79 of these patients in their respective care settings. Subsequently, n = 64 and n = 46 patients completed post-assessments. Reasons for drop-out included mortality or severely reduced health. Please see Table 2 for sociodemographic data of recruiting health professionals and patients.
Characteristics of recruiting health professionals and patients.
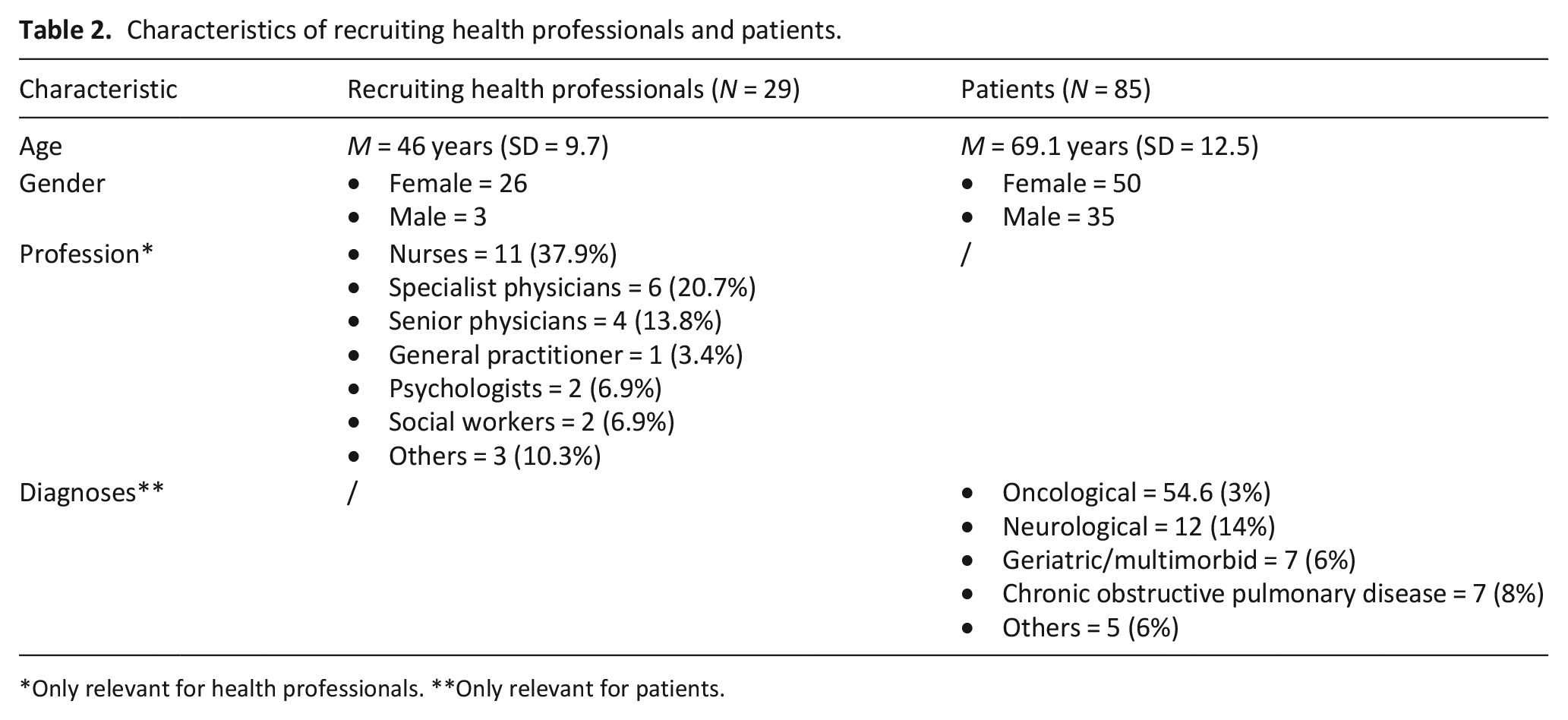
Only relevant for health professionals. **Only relevant for patients.
In our study, patient depression was significantly reduced after an open conversation on desire to die at t1 and all other patient-reported outcomes showed positive, yet not significant, trends (as also described in further detail in Voltz et al 20 ).
Relationship between wish to hasten death and will to live
During step (1), we discovered a strong negative correlation between wish to hasten death and will to live data in our sample at all three assessment points (t0: r(65) = −0.647, p ⩽ 0.001; t1: r(55) = −0.457, p ⩽ 0.001 and t2: r(43) = −0.727, p ⩽ 0.001). We see no discernable impact of the desire to die conversation held between t0 and t1 on the significance of this negative correlation, despite the smaller r value at t1. By using boxplots, statistical outliers could be identified to be n = 2 at t0 and n = 5 at t1 and t2, respectively. In a next step, we selected cases of potential clinical interest which were defined as being in opposition of the general trend of the negative correlation (e.g. had a high wish to hasten death at the same time as a high will to live). These cases were identified visually through examination of created scatterplots, see Figure 1.
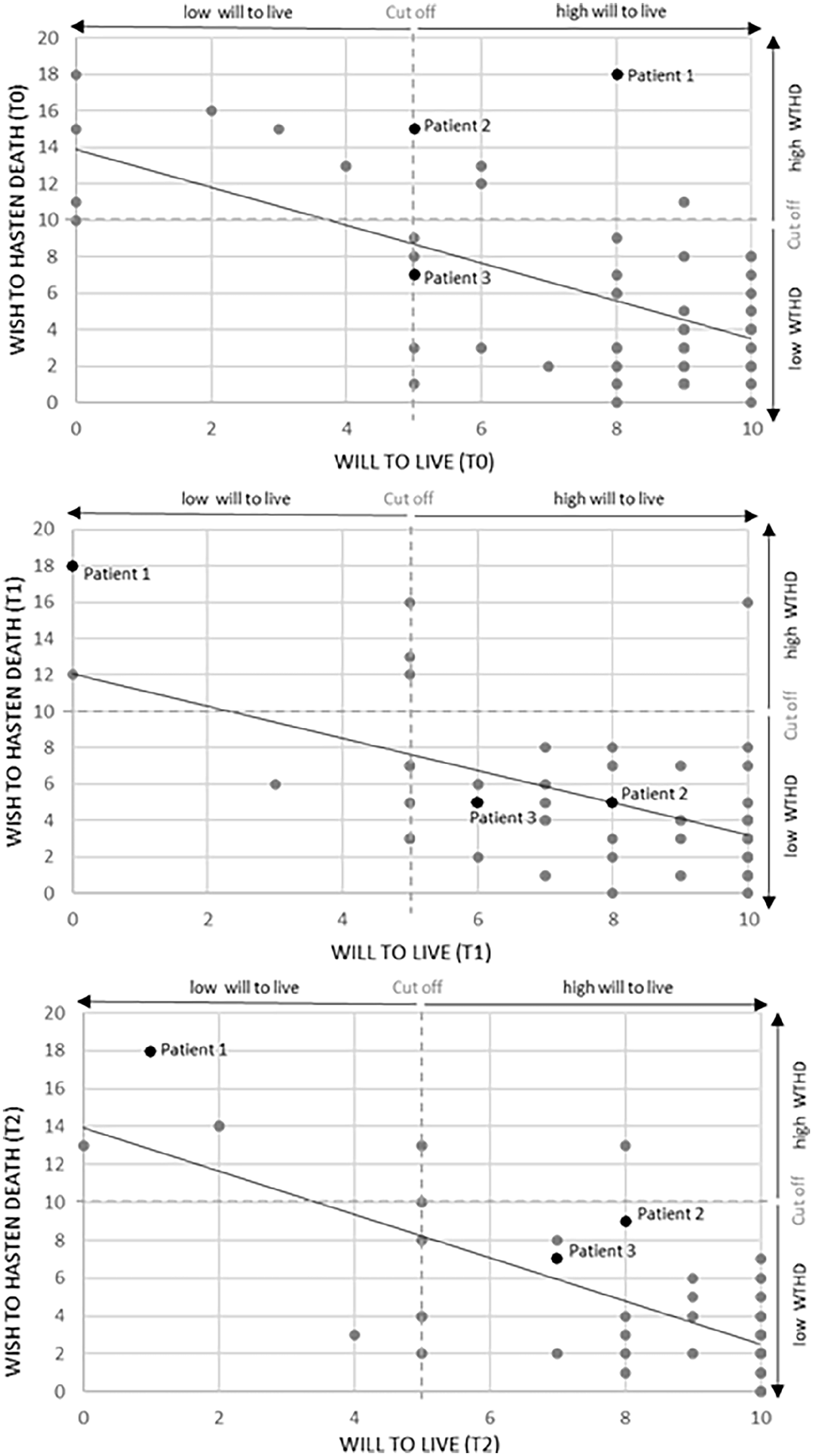
Scatter plots of the correlation between WTHD and will to live at all three assessment points (t0, t1, t2). Cut offs for WTHD and will to live are shown as dotted lines. Patients selected as case studies are highlighted.
During step (2), we examined the changes of wish to hasten death and will to live and applied the following cut-off values to designate clinically relevant changes in expression: (a) wish to hasten death: low and medium expression ⩽10; high expression ⩾11 and (b) will to live: low and medium expression ⩽5; high expression ⩾6.34,35 Between t0 and t2, most patients did not show a clinically relevant change in wish to hasten death with n = 45 (75%) remaining below and n = 6 (10%) above the cut-off. However, from those who showed a clinically relevant change, n = 5 (8.3%) sank below and n = 4 (6.7%) rose above the cut-off. Results for will to live followed a similar pattern with n = 8 (13.6%) remaining below and n = 40 (67.8%) above the cut-off, while n = 7 (11.9%) sank below the cut-off while n = 4 (6.8%) rose above it.
Results from (1) and (2) show that about two-thirds of patients remain with a low wish to hasten death and a high will to live and that the two phenomena are negatively correlated across all assessment points. Figure 2 illustrates the relative percentage of patients with each expression of wish to hasten death and will to live at all three time points.
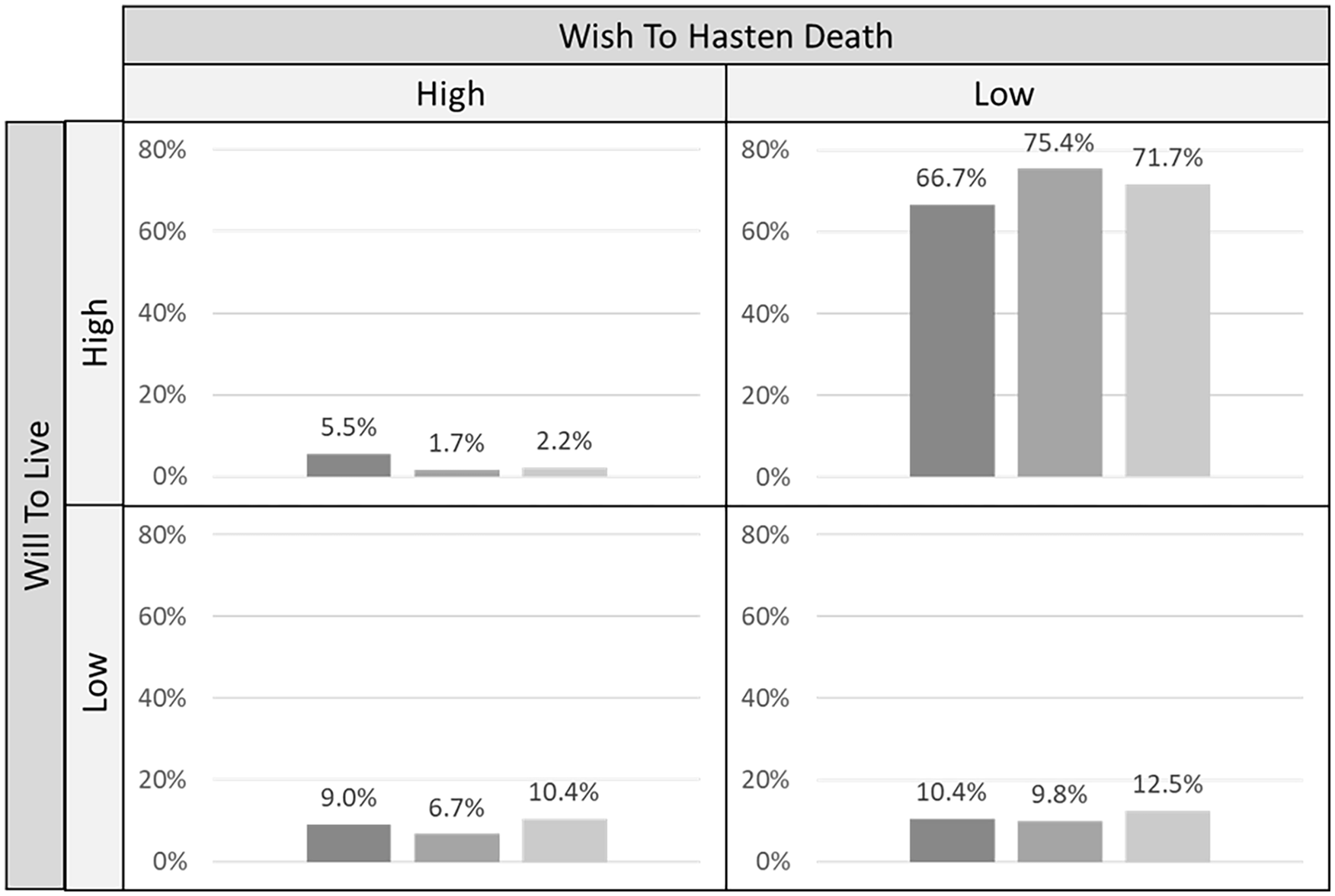
Relative percentage of patients expressing four groups of possible combinations of wish to hasten death and will to live at all three time points.
At all three time points, 66.7%–75.4% of patients fall either into the group low wish to hasten death and a high will to live or 9%–10.4% into the group high wish to hasten death and low will to live, both in line with the negative correlation found in step (1). However, there is a substantial number of exceptions in cases with varying patterns of change in the other groups. Patients with either a simultaneously high or low expression on both wish to hasten death and will to live make up to 5.5%–12.5% of the total sample, expressing an ambivalence similar to the concept of double awareness. For step (3), we identified three exemplary cases that followed atypical patterns which helps to gain a deeper understanding of the interrelation between wish to hasten death and will to live.
Patient 1 (stable high wish to hasten death, decreasing will to live)
“I would like to leave this world because (. . .) I’m done. You know, if it weren’t for the pain, then it would be okay. But I have this pain here and I have a pressure sore in my bottom and my toenails have been operated on. I am always in so much pain.”
Patient 1 is an 88-year-old woman with geriatric multimorbidity in the early stages of cognitive impairment, living in residential care. Since she suffered a femoral neck fracture, she is bound to the bed and plagued by pain and pressure ulcers on her back and bottom. Due to her situation which she describes as increasingly unbearable, she repeatedly asks for assisted suicide by the hands of her son. Her death would come as a “release,” so that she “no longer has to suffer.” Her son supports her request. However, they are both (due to lack of correct information) afraid that if he assists her in suicide, he “becomes a murderer and will be criminally charged.”
Patient 2 (fluctuating high wish to hasten death, rising will to live)
“I’m feeling far too good to do anything now. But (. . .) I can’t guarantee that it will happen at some point, [i.e.,] that it changes quite radically. That I’ll be in such a bad spot that I’ll say ‘This can’t go on any longer. This must end now.’ And then I will try to do something about that.”
Patient 2 is a 65-year-old woman with pancreatic cancer living alone, cared for by a specialist home palliative care team. She reports well-controlled physical symptoms but suffers from exhaustion and a nervous temper. When asked about her desire to die, she aptly describes her ambivalence, reporting how she asks herself: “‘Is [my] life worth living?’ And I say: ‘Yes, completely’ and then: ‘[Do I] think about ending [my] life?’ I also say: ‘Completely’.” She openly voices these thoughts with her son and her palliative care physician but is very eager not to alarm anyone. Yet, when she asked her physician about the (legal) possibility for medical aid in dying, she was disappointed by her inconclusive answer: “[she answered] more like a cotton ball. Nothing consistent, nothing constant, nothing tangible behind it.”
Patient 3 (stable medium wish to hasten death, medium to high will to live)
“Let’s say that, if life has no quality any longer it would be best to just be released.”
Patient 3 is a 64-year-old man with multiple severe chronic diseases, including COPD, spina bifida, and cardiac insufficiency. He suffers from difficulties in walking and constant pain due to polyneuropathy and reports vague but recurring thoughts about “no more quality of life” and a wish to be “released” during previous hospitalizations. Although he describes his past situation as “borderline,” his symptoms are currently well-adjusted, and he does not desire to die. In a scenario wherein he might feel worse, he would seriously consider seeking assisted dying—an option that gives him relief.
His health professional (a hospice coordinator) went through the process of preparing an advance care plan with him and informed him about the possibility of palliative sedation. Although patient 3 wishes to receive more concrete information on assisted dying, he never asked him about it, because “it still seems to be a huge problem in Germany (. . .) due to the Third Reich and euthanasia policy.”
Expressions on wish to hasten death and will to live, as well as all other patient-reported outcomes by these three illustrative cases in comparison to the whole sample are compiled in Figure 3.
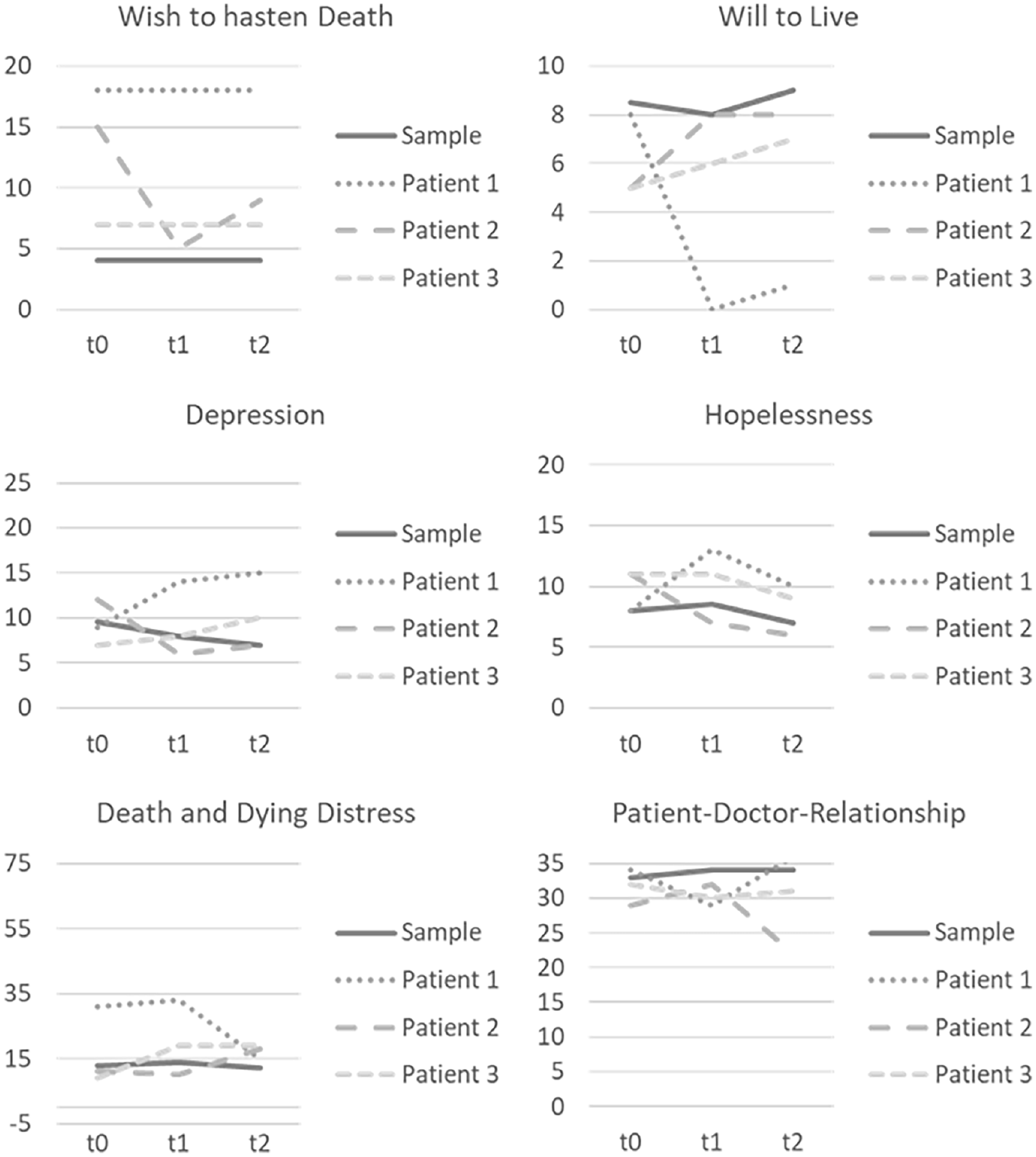
Upon visual interpretation illustrative cases show a noticeable diversion from the averaged values of the whole sample beyond the wish to hasten death and will to live. Their ratings on depression are changeable (lower and higher), their hopelessness and death and dying distress are higher and their patient-doctor-relationship is not as good. Despite the exploratory nature of these results, they give first indication that those patients with an unusual expression on wish to hasten death and will to live might stand out due to conspicuous expressions on other psychosocial outcomes as well. Here, too, changes over time can be observed.
Discussion
Main findings
Some patients with serious illness report a wish to hasten death, yet study results are inconclusive whether this necessarily implies a diminished will to live. In our secondary analysis of patient data within palliative care, we found a negative correlation between the wish to hasten death and the will to live that is stable over three time points. An open conversation about desire to die between patients and their health professional between t0 and t1 did not significantly influence this correlation. Changes within the wish to hasten death and the will to live may happen on individual basis—either triggered by conversation or other factors.
Despite this negative correlation, there are exceptions in which wish to hasten death and will to live can co-exist. Illustrated in our individual patient cases we see patients’ individual situation and personality as possible influences on these changes.
Strengths and limitations
Our original study sample is a comparatively small sample with numerous high ceiling and floor effects, therefore limiting interpretability. 20 As cases are only illustrative and present outliers, they cannot be interpreted as generalizable. 37
However, analyzing individual patient cases is a valuable way to examine exceptional or rare cases and widely used in medicine, 37 for example, in cases of assisted suicide.38,39 In this article, the richness of data (numerous health outcomes as well as qualitative interview data) and the possibility to analyze will to live and wish to hasten death over time adds to the quality of our results.
What this study adds
Our data provided support for a general negative correlation of the wish to hasten death and will to live. Beyond that confirmation, we add to the growing evidence that these phenomena can co-exist and vary over time and situation.14,40 Examining those “outliers,” we offer a deeper understanding on how wish to hasten death and will to live are experienced by patients in their own words.
In these cases, as well as in the visual illustration of the scatter plots, our data provides evidence for the concept of double awareness as introduced previously.1,2 In our sample, patients reported a wish to hasten death (e.g. as a future exit strategy or a continuous and on-going wish) and a simultaneous high will to live that is changeable depending on situation. Following recommendations made by the German national guideline for patients with incurable cancer, we also suggest to accept this double awareness as part of dealing with one’s own end-of-life. 40 As a low wish to hasten death does not need to imply a high will to live and vice versa, it is important to address both phenomena in conversations with patients. 40
Beyond this interrelation of wish to hasten death and will to live, the cases contain multiple other factors. To get a comprehensive picture of the patient’s experience, fears, and wishes, influencing factors such as depression, death and dying distress, or hopelessness should be kept in mind. Other studies report depressive symptoms, loss of meaning and purpose, loss of control, and low self-worth to mediate the effect of quality of life on wish to hasten death. 41 Similar results found depression and hopelessness as well as physical symptom distress, spiritual well-being, and a history of mental health treatment influence the development of wish to hasten death.7,42 The will to live, too, is influenced by differing variables reported in the literature such as resilience, life satisfaction, happiness, purpose in life (positive correlations), or suicidal intent and depressive symptoms (negative correlations). 4
In their daily practice, health professionals should consider the multifaceted complexity of the phenomena to avoid premature conclusions about the immutability of a patients’ wish to hasten death, especially in the context of requests for (medical) aid in dying. 43 A proactive approach in addressing desire to die—as well as will to live—based on an attitude of respect for and interest in the unique patient experience is therefore advised. 20 A clinical guideline on dealing with desire to die can be a helpful tool in realizing such a proactive approach. 20 Asking about wishes or fears regarding the end-of-life can be a door-opener for those topics most important to the patient. 25 Within such conversations, background, meaning and functions of the wish to hasten death should be explored. As our results suggest, the same is true for double awareness with a simultaneous will to live and its possible functions. Health professionals should help patients understand double awareness as a normal response to the existential threat of a life-limiting disease. The back and forth between the duality of hope and fear is common at the end-of-life and sometimes difficult to endure. 44 For some patients, it necessitates coping strategies such as solely focusing on living—for others, it is regaining control through ideating about the wish to hasten death. 44 In particularly difficult cases, patients can be accompanied therapeutically through interventions such as Managing Cancer and Living Meaningfully (CALM). 45 This ambiguity of double awareness can be hard to understand or follow not only for patients, but also for health professionals as well. 40 A basic attitude of openness and acceptance regarding situational changes in the relationship of the wish to hasten death and the will to live is recommended. 40
Our results also allow for numerous methodical implications to be discussed. When comparing the outcomes assessed by the Schedules of Attitudes Toward Hastened Death to patient’s descriptions of their experience, the additional richness of the qualitative data becomes apparent. Only through utilizing an integrative mixed-methods approach in our secondary data analysis, we were able to account for the vast spectrum of double awareness in patient cases. Especially when researching the wish to hasten death, the Schedule of Attitudes Toward Hastened Death assesses its narrower definition. 29 Successive qualitative interviews reveal more of patients’ desire to die which includes forms of desiring death without an immediate inner pressure to act. 40 Moreover, the mixed-methods approach using has the potential to deepen understanding of the data 31 : the relationship between wish to hasten death and will to live gains a new dimension through patients report influencing factors and reasons for change. Through using secondary analysis, potential patient burden through re-interviewing is prevented. 46
We therefore suggest that using questionnaires with solely numerical outcomes is a valid method, yet might lead to important aspects being overlooked. 47 Patients might weigh information differently than a questionnaire might imply and have other communication needs. 47 However, a newly developed scale for assessing double awareness might better cover the phenomena and could be used on a supplementary basis in mixed-methods designs for better understanding. 48
As we report a secondary analysis of data drawn from a larger study with the focus on effects of a conversation on desire to die, we are aware that our findings can only be exploratory in nature. The will to live and its interrelation with the wish to hasten death as a topic of interest emerged inductively late into the conduction of the study. Therefore, further research would benefit from in-depth qualitative analysis of the interrelation of wish to hasten death and will to live to account for the complexity and multiple facets of the two phenomena. Additionally, an expanded path analysis of the interrelation which statistically identifies determinants of changes over time could provide insight into approaches for clinical intervention.
Footnotes
Author contributions
KB contributed to recruitment, data collection, data analysis, and dissemination and is responsible for writing the original draft. TD contributed to data collection, data analysis and dissemination, and contributed to writing. MH contributed to data analysis and dissemination and editing the draft. RV is principal investigator and responsible for funding acquisition, study design, project management, supervision, dissemination and editing the draft. As guarantor, he takes full responsibility for the work and the conduct of the study, had access to data and controlled the decision to publish. KK is principal investigator and responsible for funding acquisition, study design, project management, recruitment, data collection, data analysis, dissemination and editing the draft.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KB, TD, and KK declare no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work. RV reports grants from the Federal Ministry of Education and Research during the conduct of the study. Grants from the Federal Joint Committee (G-BA) Germany, Innovation Fund; EU—Horizon 2020; Robert Bosch Foundation; Trägerwerk Soziale Dienste in Sachsen GmbH; Association Endlich Palliativ & Hospiz e.V.; Ministry of Labor, Health and Social Affairs of North Rhine-Westphalia; German Cancer Society, Association of the Scientific Medical Societies, German Cancer Aid; Ministry of Culture and Science of North Rhine-Westphalia; personal fees from AOK Health Insurance; German Cancer Society/National Health Academy (NGA); MSD Sharp & Dome; Hertie Foundation and Roche Germany.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Federal Ministry of Education and Research (01GY1706).
Ethics and consent
Research was conducted according to the Declaration of Helsinki. Ethical approval for this study was obtained from the Ethics Committee of the University of Cologne (#17–265) and the study was registered in the German Clinical Trials Register (DRKS00012988; registration date: 27.9.2017). All study participants gave written informed consent.
Data sharing
Data cannot be shared publicly because participants were guaranteed protection of personal data within the confines of the German data protection act. Data are available from the University of Cologne, Medical Faculty, Department of Palliative Medicine, Cologne, Germany (contact via