
Abstract
Background:
Patient and Public Involvement (PPI) is an important component of healthcare research. Conducting PPI within paediatric palliative care research requires specific ethical and practical considerations. Regular reviews of PPI activity are important.
Aim:
To evaluate a paediatric palliative care research centre’s PPI activity to determine what went well, or less well; and how future activities can be improved.
Design:
Two stage evaluation: first a review of PPI study logs; second a qualitative exploration using a survey, structured interviews and a focus group. Data were analysed thematically.
Settings/participants:
Parents of children with life-limiting conditions, bereaved parents and researchers, all engaged in PPI activity within a paediatric palliative care research centre.
Findings:
The review of PPI logs for 15 studies highlighted the crucial role of funding in enabling PPI throughout the research. Eight parents completed the survey, 4 parents were interviewed and 12 researchers participated in a focus group. Three themes were developed: Clarity of processes and purpose; balanced relationships created a safe space; and mutual respect and value for PPI. These themes highlight what is working well within the Centre’s approach to PPI and the opportunities to improve.
Conclusions:
To undertake meaningful PPI in paediatric palliative care research, adequate time and resources are required. Roles, processes and expectations must be explicitly agreed. Establishing relationships ensures trust and enables authenticity and vulnerability. In addition to improving research, PPI has personal benefits for researchers and parents. The evaluation led to the development of a ‘route map’ for establishing an impactful PPI group for paediatric palliative care research.
● Patient and Public Involvement (PPI) is recognised as an important component in healthcare research, it can take many forms and should occur at all stages in the research cycle.
● There are sensitivities, and ethical and practical considerations when involving parents of children with life-limiting conditions or bereaved parents in paediatric palliative care research.
● Many generic PPI toolkits are available, but there is a lack of specific guidance to steer PPI practice or evaluation for those conducting palliative care research, particularly within paediatrics.
● Parents need to balance their commitments and so need explicit communication about the purpose of PPI activities and clarity around expectations, roles and processes.
● It is important to establish balanced relationships that combine professionalism, friendliness and support, in order to create a safe space where parents and researchers are comfortable sharing their experiences and discussing difficult topics.
● The impact from PPI is expressed in terms of personal growth and development for both researchers and parents, and for parents it can also offer a sense of community and therapeutic benefit.
● Tracking PPI activities in such a way that enables regular evaluations of impact and reporting back to contributors will strengthen best practice.
● Successful PPI within paediatric palliative care research requires substantial investment of time and resources, and so needs to be accounted for appropriately in funding applications.
● A route map to successful PPI in paediatric palliative care sets out practical steps to establishing an impactful PPI group.
Background
Patient and Public Involvement (PPI) is the active involvement of patients and members of the public in the design and conduct of research, and is recognised as a key component of healthcare research.1,2 International evidence shows PPI can improve the quality and relevance of research.3,4 PPI should occur at all stages of the research cycle and can be achieved through a range of approaches.1,5 –8 In the UK, input from service users and those with personal experience is commonly a perquisite from policy makers, service commissioners and research funders and this is increasingly becoming an expectation in other countries.9 –11
Conducting PPI within paediatric palliative care research has its challenges including involving appropriate people with relevant experiences, and sensitively managing the specific ethical, emotional and practical considerations that accompany this subject area.2,7 The Public Involvement Impact Assessment Framework Guidance (PiiAF) describes how PPI impacts on the research process and outcomes, and also on stakeholders involved (e.g. PPI-partners, researchers, funders). 12 It is a complex social process and it is important to understand the impact of involvement for everyone. 12 While recent reviews have highlighted the large number of different guidelines, frameworks and standards,13,14 there is still a lack of consensus about the best way to evaluate PPI in research.4,10,12,15 –17 This is especially true within palliative care research, particularly within paediatrics.6,7,10
PPI has been a key priority of a Paediatric Palliative Care Research Centre in the UK (‘the Centre’) and has been embedded into all its activities. The Centre’s PPI lead and activities were funded as part of the core funding of the Centre and via an associated grant from a charity. A PPI family advisory board was established (‘the Board’) consisting of about 20 parents of children and young people with life-limiting conditions and complex healthcare needs, referred to herein as PPI-partners. The Board meets monthly and provides input on the design and conduct of individual research studies, as well as advising on the development and coordination of PPI for the Centre.
This study aimed to evaluate the Centre’s PPI activities. Study objectives:
RQ1: To review and map the range of the Centre’s PPI activities and their impact on the research processes, outcomes and on the people involved.
RQ2: To gain an understanding of how the Centre’s PPI-partners and research staff perceive PPI activities they have engaged with and what could be done better.
RQ3: To determine the areas of success and required improvement in how PPI activities have been conducted and plan a route forward.
Methods
Methods used were designed in consultation with the Board and a two-stage evaluation was conducted. First, a review of recorded PPI activity mapped against different research stages to understand when and how researchers are engaging with PPI-partners and how this impacted on research design, delivery and outcomes. Secondly a qualitative exploration of PPI-partner and researcher experiences to understand perceptions of the PPI they are involved with, and what could be done better. The findings from both stages were combined to produce guidance for the Centre’s future practice.
Stage 1: Reviewing PPI activity
A standardised spreadsheet record is kept for each study in the Centre, which logs the details of PPI activities including funding, type of activity, who was involved and impact on the study. The structure of the logs was informed by the PiiAF framework and the GRIPP2 reporting checklist.12,18 Data was extracted from the PPI logs of studies undertaken in the Centre, (LB, female, health researcher) in conjunction with a researcher from each study. Using an NIHR research framework 19 each entry was mapped to the stages of the research cycle to see when PPI was occurring, and the PPI input was assessed for its effect on the relevance, quality and impact of the study.
Stage 2: Qualitative exploration
Participants: All PPI-partners, involved in either the work of the Board or study specific PPI groups and all the Centre’s researchers with experience of working with PPI-partners, were invited to take part in the research. All potential participants were emailed an invitation letter, information sheet and consent form.
Data collection: Data were collected concurrently in September–October 2022. The Board proposed that PPI-partners were given a choice of data collection methods, either an anonymous online survey or an interview. An anonymous survey allowed those PPI-partners who may feel uncomfortable being interviewed and those who may want to talk negatively about their experiences, the opportunity to do contribute privately. Interviews allowed PPI-partners to provide more depth. Survey data was collected via the Qualtrics© survey 7 platform. 20
PPI-partners who chose to be interviewed, could opt for a face-to-face, telephone or video-call interview, these were recorded and were conducted by AP (male, PPI coordinator) and JH (female, PPI lead), both health researchers known to the participants. PPI-partners were offered financial reimbursement for their time.
The topic guide was developed from the literature and then the Board were consulted and suggested further topics, helped structure the questions and advised on wording. The same question set was used for both the interviews and survey, and covered participants understanding of PPI, personal experiences of involvement with the Centre and ideas for improvement of how the Centre conducts PPI (Supplemental File 1).
In order to provide a discursive environment and to gain a breadth of understanding, an online focus group was held with the Centre’s researchers during which they were asked to share and discuss their perspectives and experiences on the PPI activities they have been involved in. AP and JH facilitated and participated in the focus group.
Data analysis: Data from the survey, interviews and focus group were transcribed and then analysed together, thematically.21,22 First, LB listened to all audio-recordings, then interview and focus group transcripts and survey data were read and re-read for familiarisation, with notes taken on key concepts, issues and experiences. Data were systematically coded inductively across all transcripts, identifying all data in relation to each code. Codes were grouped into descriptive categories to explore the meanings of codes and potential relationships between codes. Divergent cases were sought. LB and JH developed analytical themes by summarising and seeking to understand coded data and descriptive categories. 22 Themes were then further developed through discussion with the Board and other team members. NVivo 12 was used for managing data. 23
Developing guidance
The findings of Stage 1, the review of PPI activity, and Stage 2, the qualitative exploration of PPI-partner and researcher experiences, were then examined with a lens of providing practical guidance to researchers. A ‘route map’, which aimed to provide workable steps that addressed the issues and needs of the groups and that will lead to impactful PPI, was drafted by the authors (LB and JH). This was then refined within the team and in consultation with the Board.
Reflexivity
Reflexivity enhances the credibility of findings and deepens understanding by emphasising the contextual and interconnected relationships between participants and researchers. The team recognised the importance of being reflexive and acknowledging they were both part of the evaluation team and the participants in the research. The team discussed and critical reflected throughout the process including around methods chosen, the topic guide and the analysis and interpretation of findings.
PPI in the evaluation
Members of the Centre’s Board were involved at all stages of this study, including a co-author (GW). They were consulted about the objectives of the evaluation and helped design the methodology, including which aspects of PPI to focus on. They were presented with potential research questions derived from PPI literature, and asked if these resonated and if they had additional questions to add. They provided advice on how feedback should be collected from PPI-partners and suggested the use of interviews and an anonymous survey. Topic guides and survey questions were designed in partnership between the researchers and PPI-partners, and the survey was piloted with two PPI-partners. Preliminary findings were presented and discussed with the Board, and their input refined the final themes.
Findings
Stage 1: Reviewing PPI activity
PPI logs from 15 research studies (9 complete, 2 in the dissemination phase and 4 ongoing) were examined and compared, and the activities were mapped against stages of the research process. 19 (Figure 1)
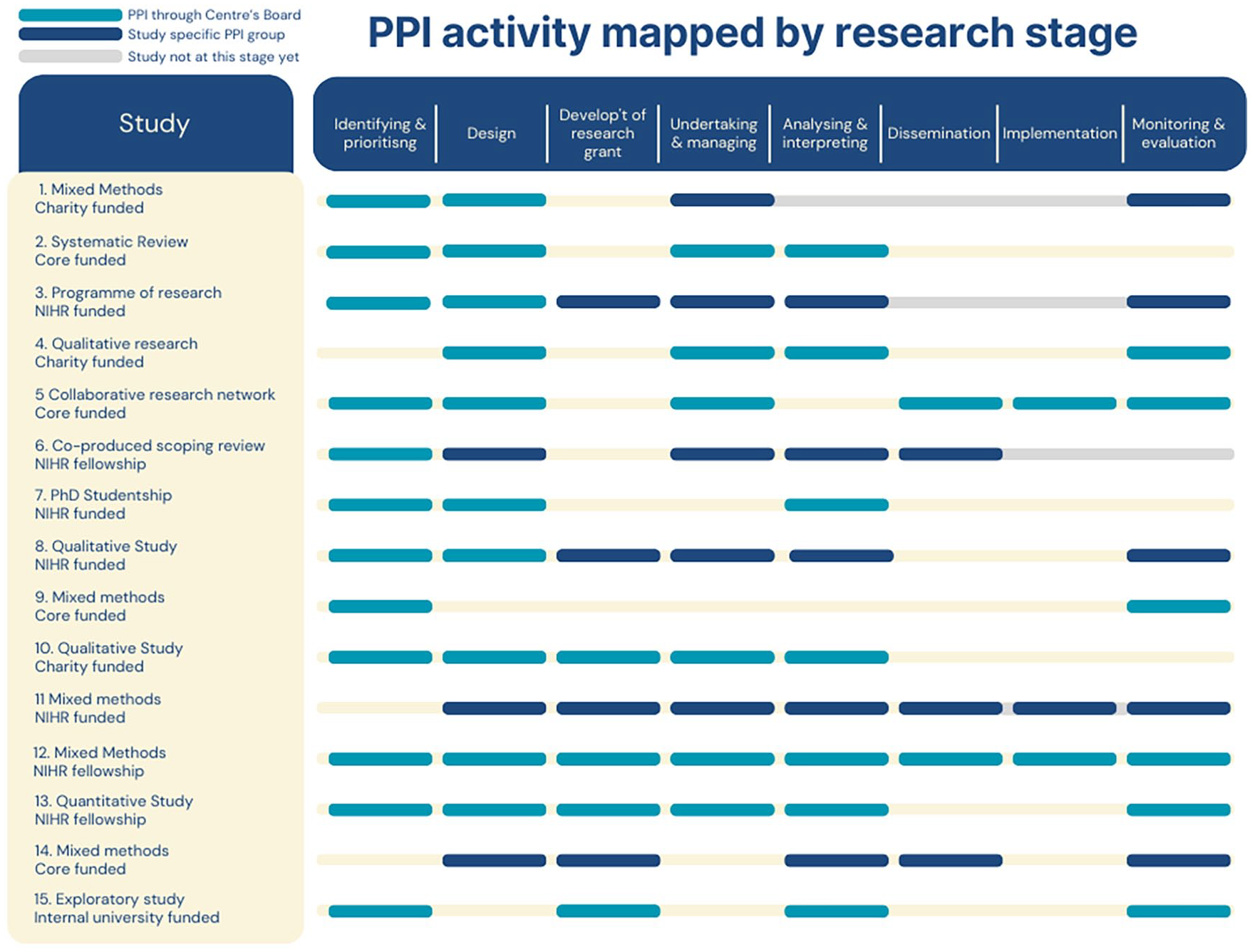
PPI activity mapped by research stage.
PPI involvement tended to be concentrated in the ‘design’, ‘undertaking & managing’ and ‘analysing & interpreting’ phases of a research study, with less involvement at ‘dissemination’ or ‘implementation’ stages.
Six of the 15 studies reviewed had funding to support a study-specific PPI group. Regular meetings with the study team enabled PPI activities to be embedded and have influence throughout the research process. Members of these groups were also on the Study Steering Committees, providing strong monitoring and oversight.
For studies without a specific PPI group, the Board provided input. This usually occurred at the beginning to discuss study aims, design and recruitment strategies and again when initial findings were available. The existence of the Centre’s core-funded Board enabled nearly all studies to have input from PPI-partners at the very early stages of a study.
PPI input was not always feasible or appropriate at all stages. For example, one study had been funded through a commissioned call, and had therefore already been prioritised for funding. Several studies included in this evaluation were still ongoing at the time of the evaluation and so had not reached later stages, such as dissemination.
The review of PPI logs found clear examples of the impact of PPI on the research itself, including shaping the research design, selecting outcome measures, influencing the approach to recruitment and data collection and assisting in interpreting findings. However, there was an inconsistency in language and level of detail in the logs. Data was insufficient to measure the impact of PPI on the research. To learn what had worked and when, it was helpful to understand the types of activity happening and their impact. Figure 2 shows case examples of PPI activity and its impact at each research stage.
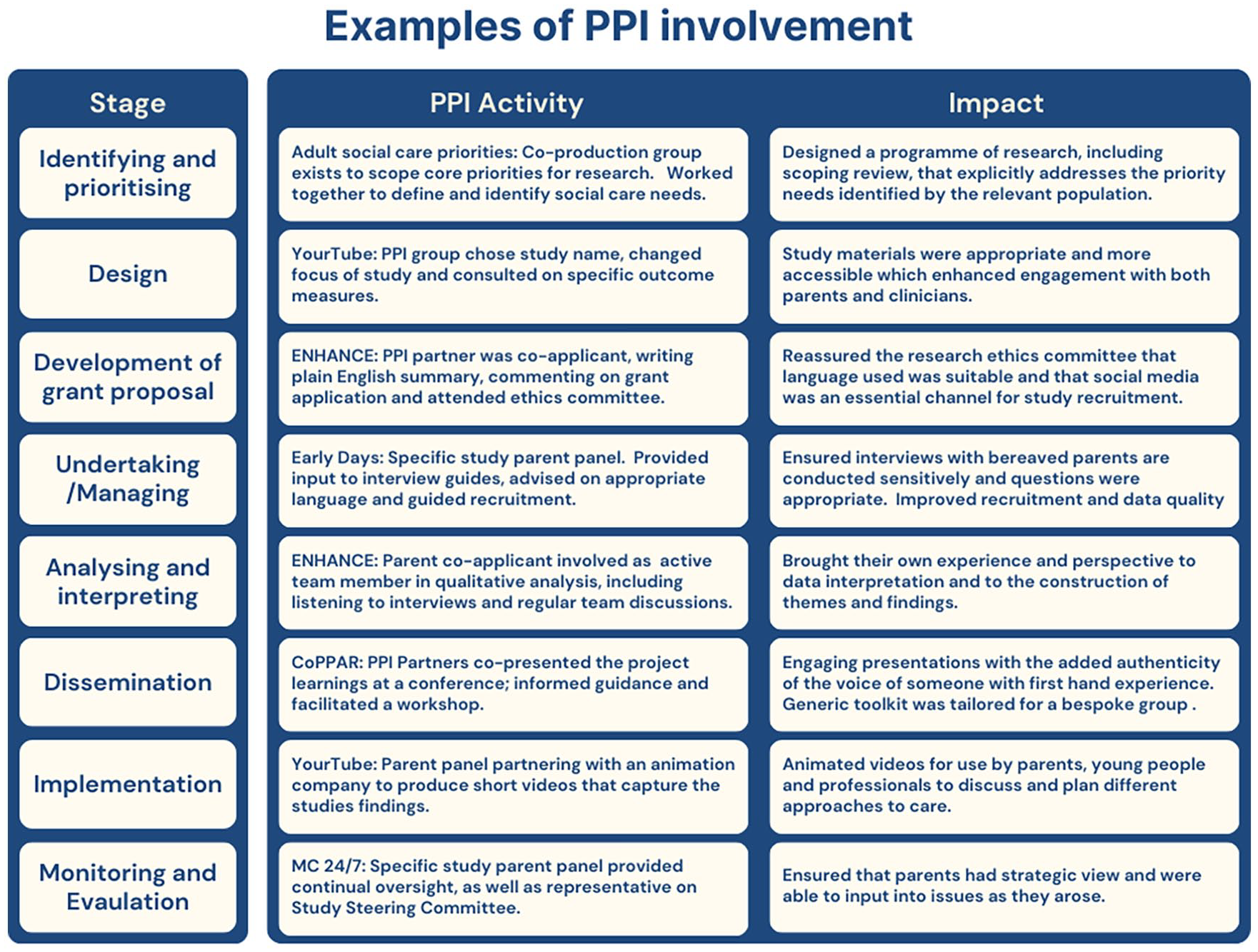
Examples of PPI involvement.
Stage 2: Qualitative exploration of PPI-partner and researcher experiences
Four PPI-partners were interviewed by video (average length 47 min), and eight completed an anonymous survey. All respondents were members of the Board and four had also been part of study-specific PPI groups. They were a mix of bereaved parents and parents of children with life-limiting conditions. Nineteen researchers, all with experience of working with both the Board and study-specific PPI group were invited to an online focus group, of which 12 participated, including the Centre’s PPI lead (JH) and co-ordinator (AP). Detailed participant characteristics are not available as the survey was conducted anonymously and small sample sizes may lead to identification. Where participant quotes are presented below, these are identified as either PPI-partner survey [S] or interview [IV] data or as researchers [R].
Three main themes with subthemes were developed from the data: Clarity of processes and purpose; balanced relationships created a safe space; and mutual respect and value for PPI. These themes highlight what is working well within the Centre’s approach to PPI and the opportunities to improve.
Clarity of processes and purpose
Most PPI-partners had a clear understanding of PPI and why they were involved. As a group of parents of children with life-limiting conditions, and bereaved parents, there was a common awareness that their role was to share the ‘realities’ of their experiences of caring for, or trying to receive care for, a seriously unwell or dying child, in order to inform paediatric palliative research. However, there was less clarity around the strategy and operation of the Board. It was recognised that researchers accommodated PPI-partners’ needs and circumstances when planning meetings. This theme mostly arose from the PPI partners data and was less reflected by the researchers.
Understanding of the Board’s remit
For the PPI partners there was uncertainty around the long-term position of the Board, and it was suggested that communication around its strategy and remit could be better, especially being clearer that the Board was there to input into research rather than have a direct influence on care delivery.
Something I would value, and I wonder if it would be useful, is just really laying out the purpose of the group in a really simple way. And that it is purely about research. [Partner IV3]
Fundamental to many of the PPI-partners’ motivations for participating was a drive to use their experiences to improve care for other families. However, for some, there was a feeling of disconnect and powerlessness, and they were not confident of the impact their input was having in practise or at a policy level.
Whether that research leads to policy, as devastating as it may be, we can’t change that. I think sometimes we often drift into conversations around policy ‘cause it’s what we all want to be there for. [Partner IV3] And whether the research made a difference on a macro level? That’s out of our hands really. [Partner IV4]
Transparency of processes
Both PPI-partners and researchers mentioned that the way the board operated could be clearer and that it would be helpful to have introductory training or induction. One PPI-partner suggested there should be ‘welcome pack.’ Researchers appreciated the opportunity to meet the Board members before returning to present to or consult with the group.
Just before a new member joins a bit of orientation especially around emotional support will be useful. [Partner S5] I guess maybe a little bit more of an introduction into the kind of things that might be discussed that the parents are here to answer your questions and if they don’t want to answer it, they’ll tell you and it’s kind of like an open environment and all of that. So, I think just for new researchers coming in that kind of reassurance about what kind of environment it is. [Researcher R2]
It was also mentioned by both groups that there was not a clear ‘ending’ so it might be hard for PPI-partners to say they don’t want to be involved anymore or they feel their experiences are no longer relevant.
Some Board members became involved in other projects or activities outside of the main forum. A few wanted a better understanding of how these opportunities were allocated, particularly with individual research projects.
I think the one bit that isn’t structured is how you get involved in the kind of additional work that you guys do, and whether and how there are any opportunities to get involved in more or in a different way. [Partner IV1]
Commitment levels were purposefully flexible
Some PPI-partners found it difficult to sustain regular obligations due to their caring responsibilities or other issues relating to being a parent of a child with a life-limiting condition. So, it was recognised by both researchers and PPI-partners that there needed to be flexibility around expectations of commitment to the group. Partners felt able to ‘kind of dip in and out as much as you can and want to and are able to.’ [Partner IV2] I think I was told, “Maybe go along.” You know, if you can't make it, it is fine. You will still get the invites so you can just go to the ones that you can make. That was made perfectly clear, and that is how I found it. [Partner IV1]
Inclusive and accessible meeting arrangements
Partners recognised the efforts made to ensure that any events were inclusive and accessible. Having previously met in person, since COVID-19 meetings are now predominantly online, with annual face-to-face meet ups. For some partners, the move to online meetings had been helpful and felt more inclusive, but for others this was seen as a barrier to engagement.
This having online meetings and maybe occasional face-to-face meetings is a very good combination. The online meetings perhaps lend themselves to different kinds of discussions than face-to-face meetings. In a way, that’s the potential of doing it and being online makes it easier for some of the participants who wouldn’t otherwise be able to come to face-to-face meetings. [Partner IV4] I think since I struggle with Zoom, so since it’s gone a lot onto Zoom, I haven’t engaged as much, I haven’t been able to keep track as easily. Meetings have passed and I have gone, “Oh, that was the meeting.” [Partner IV2]
Balanced relationships created a safe space
A strong theme from both the researcher and PPI data was that establishing and maintaining supportive relationships, and balancing professionalism and vulnerability enabled the Board to become a safe space for everyone.
Continuity enabled solid relationships to form
The continuity and regularity of the Board enabled relationships to develop between researchers and PPI-partners. PPI-partners viewed their interactions with researchers as positive, empathetic and built on mutual respect and found researchers friendly and approachable.
The staff are communicative, friendly, and knowledgeable, making the process simple and kind to the participant. [Partner S8] And you have much more context on the history of their lives and what’s going on and you therefore, you are more comfortable about what you are saying or what you can say than someone you really don’t know so much about their circumstances or what’s happened. [Researcher R4]
Researchers balanced professionalism with openness
Researchers felt it was important to understand the balance between professionalism and friendliness, and that the boundaries were ‘blurry’. As part of building a trusting open relationship with PPI-partners, researchers felt able to be vulnerable and expressed a desire to share personal information about themselves. This was appreciated by PPI-partners.
I find it’s also, in those bits, it’s an opportunity for you to share back little bits of information about you, as well to try and break that power imbalance away. [Researcher R1] We ask about how are you and how’s things and you talk like a human being. You’re not just talking like a researcher. That helps as well. I like that. It’s a very fine balance being professional because we’re still involved in a professional level, but because you treat us on an equal level, it’s easier, I think, to keep this very fine boundary between . . . we’re not friends. [Partner IV4]
Communication was described as open and easy and PPI-partners felt able to email or phone outside of structured meetings and described researchers as responsive, which helped PPI-partners feel they were an equal part of the team.
So, I feel like it really is a collective, which is really nice, and the power feels really nice in that way. It doesn’t feel very hierarchical. [Partner IV1] We are treated as partners and experts. [Partner IV4]
PPI-partners felt safe and were well supported
As the topics discussed were often emotionally sensitive, researchers felt a keen duty of care for PPI-partners and wanted to ensure they were supported emotionally and practically if needed. They stressed it was important to be aware of any changes in circumstances or if any of the PPI-partners needed additional support. Researchers also recognised they should not shift into gatekeeping, shy away from difficult topics or act paternalistically.
But when you do engage with them, they’re saying we do want to speak, we do want to engage – let us make the decision, don’t protect us without giving us the voice and chance to contribute. [Researcher R3]
PPI-partners agreed and expressed that they did not need protection and are quite capable of engaging in ‘difficult’ subjects.
It is an important area, and one that often gets overlooked or sidelined under the assumption that parents won't want to discuss difficult things. So, I like the fact that difficult things are discussed. [Partner S1]
The connection and sense of community between PPI-partners added to the sense of safety. These relationships had in some cases led to involvement with other PPI activities.
It also feels like a time when we can all just come together and talk about stuff. [Partner IV6]
Ultimately, both groups agreed that a safe space was created where PPI-partners were supported, were able to express themselves authentically, challenge the researchers if necessary and talk openly about difficult topics.
I think I would feel quite comfortable saying oh I am not comfortable with this, or I need support with x, y and z. [Partner IV2] It felt very safe, it felt like they were able to speak very candidly about their thoughts on the research, their input and to challenge us. [Researcher R8]
Mutual respect and value for PPI
Both PPI-partners and researchers respected and valued each other’s involvement with PPI. Both groups felt personal benefits from being involved in PPI, and there was a consensus that PPI played an important role in grounding, shaping and improving the Centre’s research.
Respect for PPI partners’ own experiences
Fundamental to the process was that PPI-partners were bringing the truth and reality of their own experiences and that they felt that their expertise was listened to and valued.
It’s very useful for the researchers because they can tailor the proposal in line with our reality if you like. They make it more potent and in line with real experience. [Partner IV4]
However, it was noted that current Board members were not always representative of all experiences and that more could be done to ensure a broader range and diversity of people. In particular, it was felt that the voices of more young people and men/fathers should be heard. For the researchers there needed to be clarity that PPI-partners are involved to only bring their own experience and this should not be extrapolated.
You’ve got to be very careful to not take one person’s experiences and think that reflects the experiences across a group of people that you’re going to then take that out to. [Researcher R6]
Personal benefits of participating in PPI
The PPI-partners reported satisfaction from being able to put their experiences to use. For some there was clear personal growth and development, including improving skills and confidence. For some parents whose lives are often dominated by their caring duties, involvement in the Board was seen as a potential step into the world of work.
Especially because [. . .] a lot of parents themselves might not be working, so it’s actually a really good work experience, and could open doors for employment for the parents who are not working. [Partner IV1]
There were also reports of a sense of therapeutic benefit, that PPI-partners were able to use the forum to process their experiences through discussion with others.
To help mitigate my own grief by being able to potentially help others who will go through the same, or similar experience. [Partner S8] it’s very therapeutic in that respect. [Partner IV4]
When training was discussed, most PPI-partners responded that they were keen to learn and upskill. Training requests included understanding the research process, research methodologies, specific research topics, IT skills and Zoom training.
For researchers, having the Centre’s Board as a resource enabled them to sense check their personal approach and their ‘practise’. This is particularly important when the research involved working with sensitive subject areas.
I found that process very useful because it just felt like a bit [of an] informal way. . . and I felt like I could very honestly say, “Is this okay to say to someone?” or, “What do you think about this?” Yes, it sounds a really safe way to practise what could be difficult interview, so that was fantastic. [Researcher R1] They really helped me phrase things and it made me a lot more confident to be honest to then go out and interview parents. [Researcher R7]
Grounding, shaping and improving the research
Researchers were clear that input from PPI-partners helped them prioritise research topics that had application and relevance. However, several of the PPI-partners would like more opportunities to shape what is being researched and mentioned it would be good to revisit the research prioritisation exercise carried out when the Centre was established. 24
I think for me it’s really about grounding our research and make sure that what we’re doing really does have relevance in the world, in the real world, and for people having that experience. [Researcher R3]
Researchers were clear that collaborating with PPI-partners had shaped and improved the research process, given helpful perspectives and deeper insight. In particular, the approach to participant recruitment, interviewing about emotional and sensitive topics and communicating findings.
It was really invaluable actually for my research and really changed a lot of the ways I was thinking about it. [Researcher R8] Taking my initial findings and things to them definitely gave some important insights and stuff that I wouldn’t have thought about. [Researcher R4]
Some PPI-partners would like more feedback about the progress of research studies, particularly those they had provided input into.
Hearing of outcomes would be rewarding. [Partner S1] PPI process is genuinely valued by all involved
Researchers were consistent in expressing their respect for the PPI process, that it is ‘critical to everything we do’ [R6] and that they were engaging sincerely and not as a token effort or tick-box exercise.
They [PPI-partners] are part of everything that the Centre does. Really valuable. [Researcher R2]
This was reflected in responses from the PPI-partners who felt their efforts were recognised.
I honestly couldn’t fault the Centre’s approach to PPI and how it really, genuinely is at the heart of everything that’s done [Partner IV2]
Route to impactful PPI
Findings from the review of the Centre’s PPI activities, the qualitative evaluation and a further consultation with the Board provided an understanding of the PPI work undertaken within the Centre, including what has worked well and what could be improved. From this, a route map to implementing successful PPI within the paediatric palliative care research centre was developed. This is shown in Figure 3.
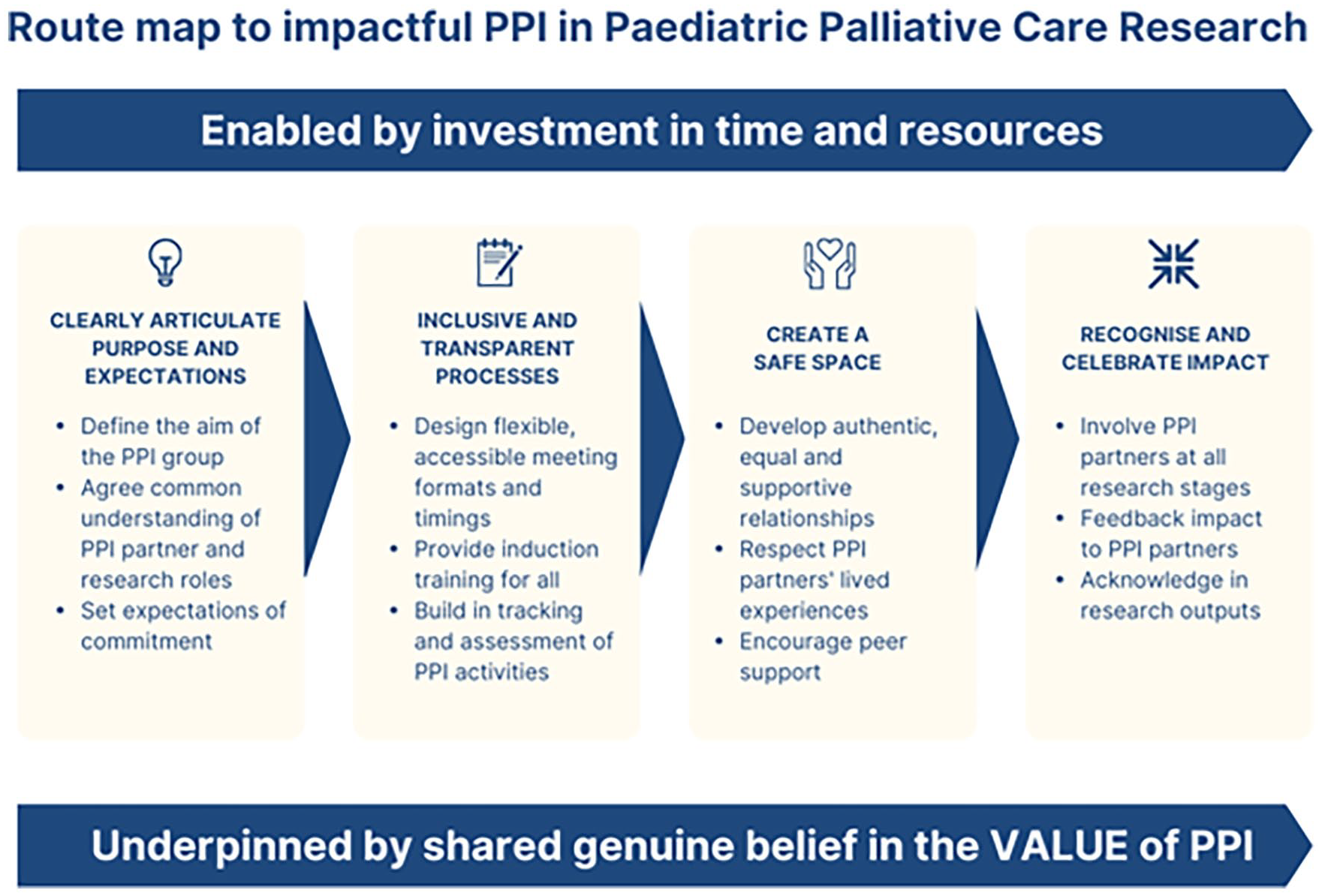
Route map to impactful PPI in paediatric palliative care research.
Discussion
Main findings
This study highlights that PPI has positive personal benefits for both researchers and PPI-partners, in addition to improving the research. To enable successful PPI in paediatric palliative care research, funded time and resources are needed. Long-standing relationships that balanced professionalism, friendliness and support had created a safe space where parents were comfortable sharing their experiences and discussing difficult topics. Researchers and PPI-partners recognised the value of everyone’s contribution and both groups perceived animpact in terms of personal growth.. Researchers were also very clear that collaborating with PPI-partners had shaped and improved their research.
However, PPI-partners felt communication about the purpose of PPI activities needed to be more explicit and there was a requirement for more clarity around expectations, roles and processes. It was particularly important for these parents to understand and have flexibility in their commitment.
What the study adds?
This study highlights the importance of consistently recording PPI activities and their impact. The Centre must keep in line with current best practice, for example potentially adopting the recently launched Public Involvement in Research Impact Toolkit (PIRIT) tracking tool, 25 which allows researchers to record public contributions and the difference they make to the research, and maps them against the UK Standards for Public Involvement. 5
Establishing long-term relationships through regular meetings allowed for PPI to be included in most studies particularly at the crucial early shaping stages. However, this requires time and funding to invest in this process; research funding can support study specific PPI activities, but for PPI input in to the early prioritisation, design and the development of grant stages, there is a need for further investment. This was reflected by Wilson et al. 9 who found PPI was more strongly embedded if an organisation had core funding and stability, including a person with a designated responsibility for co-ordinating and facilitating PPI. The end of the Centre’s core funding has emphasised to the research group that it is essential best practice for all PPI costs to be accurately budgeted into funding applications.3,26
Explicitly agreeing the purpose of PPI activities and the role expectations of those taking part is essential. 7 Feedback from the Board when consulted about this study’s findings included potentially defining a ‘role description’ and the importance of induction training. For PPI-partners involved in paediatric palliative care research who may be recently bereaved, or who are juggling intense caring responsibilities for their child, understanding ‘what’s involved’ is particularly important. Reflecting findings from other studies, keeping a flexible approach and mixing meeting formats and timings ensures inclusivity.6,7
Like other research work in this area, 6 the importance of building relationships with PPI-partners and the consideration of emotional support when discussing sensitive topics was highlighted. This study, however, found the balance of power in these relationships also depended on researchers being authentic and open, and if appropriate sharing their personal experiences. This is not always the case in PPI and an evidence synthesis of PPI activities in adult palliative care found research professionals could be reluctant to be involved and open, although in those instances when boundaries were blurred, this was seen to be helpful to the process. 7
While PPI-partners felt confident that their contributions were useful, it was clear that they would welcome more insight on how these had impacted the Centre’s research. This supports the findings of Mathie et al. 27 who highlighted the benefits of feedback to create motivation for further involvement, to aid learning and development, as well as a means of recording impact.
This evaluation highlighted the importance of understanding the specific needs of PPI-partners and it was clear that being involved in the PPI had positive benefits for all concerned. The PPI-partners described a range of personal impacts. For some parents who have spent a large proportion of their life caring for a child, involvement in PPI offered a safe opportunity to learn and gain new experiences. This is reflected in a systematic review by Brett et al. 3 focussed on the impacts of PPI on the people involved. However, in addition to the benefits found in that review, many of the PPI-partner participants in this study also found a sense of community and therapeutic benefit from sharing their stories and experience with peers, and in some cases, this helped with processing their grief.
Both parents and researchers felt that PPI was genuinely valued by all involved and that it was not being undertaken as a ‘tick box’ or tokenistic exercise, which can be a danger given the pressure from funding bodies. 28 As evidenced throughout, PPI-partners and researchers see the Board as both partners within the research centre, shaping strategy and direction and as contributors to individual studies. PPI-partners are therefore truly embedded within the research centre. This mutual respect and belief in the value of PPI underpins the route map to conducting PPI in paediatric palliative care research.
Strengths and limitations
This study benefited from strong PPI input into the evaluation including the study design, data collection methods and interpretation of findings. Use of multiple methods of data collection allowed for PPI-partners choose how they contributed and led to a breadth and depth of findings.
Due to established relationships, participants may have been more likely to, or felt obliged to provide a positive reflection. To counter this, topic guides were explicitly designed to elicit more negative experiences and PPI-partners were encouraged to complete the anonymous survey. The study team also sought to challenge their own and each other’s accounts in the interests of improving and developing the Centre’s work.
Conclusion
To enable successful PPI in paediatric palliative care research, funded time and resources are needed. Partner and researcher roles, processes and expectations must be explicitly agreed. Establishing and maintaining relationships ensures a sense of safety for difficult discussions and enables authenticity and vulnerability from all involved. PPI has positive personal benefits for both researchers and PPI-partners, in addition to improving the research.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241266374 – Supplemental material for Evaluating parent and public involvement activities within a paediatric palliative care research centre: Route map to impactful and meaningful engagement
Supplemental material, sj-docx-1-pmj-10.1177_02692163241266374 for Evaluating parent and public involvement activities within a paediatric palliative care research centre: Route map to impactful and meaningful engagement by Laura Barrett, Julia Hackett, Jo Taylor, Andrew Papworth, Gabriella Walker and Lorna Fraser in Palliative Medicine
Footnotes
Acknowledgements
We would like to express our gratitude to the parents and researchers who took part in this study. We are also grateful to the Centre’s Board for the advice, guidance and input though the study.
Author contributions
JT, LF, AP and JH designed the study in partnership with the Board. The data collection was conducted by AP, JH and LB. LB led the data analysis and writing of the manuscript. JH contributed to the analysis and parent advisors gave feedback on initial themes. All authors LB, LF, JT, AP, GW and JH critically reviewed and contributed to revisions of drafts of the manuscript and then read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by True Colours Trust and funded and hosted by the Martin House Research Centre: a partnership between the Universities of York and Leeds, and Martin House Hospice Care for Children and Young People
Research ethics and consent
This study was reviewed and received ethical approval from the University of York Health Sciences Research Governance Committee on 13th May 2022 (HSRGC/2022/508/G: MHRC PPI Evaluation Project 2022).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.