
Abstract
Background:
Advance care planning in dementia includes supporting the person and their family to consider important goals of care. International research reports the importance of psycho-social-spiritual aspects towards end of life.
Aim:
To develop a multidimensional international palliative care goals model in dementia for use in practice.
Design:
International Delphi study integrating consensus and evidence from a meta-qualitative study. The Delphi panel rated statements about the model on a 5-point agreement scale. The criteria for consensus were pre-specified.
Setting/participants:
Seventeen researchers from eight countries developed an initial model, and 169 candidate panellists were invited to the international online Delphi study.
Results:
Panellists (107; response 63.3%) resided in 33 countries. The model comprised four main care goals: (1) Comfort ensured; (2) Control over function maintained; (3) Identity protected and personhood respected and (4) Coping with grief and loss−person and caregiver supported. The model reflects how needs and care goals change over time with the progression of dementia, concluding with bereavement support. The first version of the model achieved a consensus after which it was slightly refined based on feedback. We did not achieve a consensus on adding a goal of life prolongation, and on use of the model by people with dementia and family themselves.
Conclusion:
A new palliative care goals model for people with dementia and their families includes relationship aspects for use by professionals and achieved a consensus among a panel with diverse cultural background. The position of life prolongation in relation to palliative care goals needs further research.
Keywords
A white paper from the European Association for Palliative Care (EAPC) presented a care goals model for people with dementia covering changes of the goals of life prolongation; maintenance of functioning and maximisation of comfort towards death.
Advance care planning discussions have gained momentum also for dementia, and recent Western and Asian studies indicated the relevance of psycho-social and spiritual care goals in addition to physical care goals.
A newly developed multidimensional palliative care goals model adds psycho-social-spiritual goals such as: identity protected and personhood respected; coping with grief and loss – person and caregiver supported.
While the EAPC care goals model did not achieve a full consensus in the original Delphi study, the new multidimensional model did.
The study highlights remaining controversy around life prolongation as a goal of care for persons with dementia.
The model may broaden the perspective of healthcare providers to consider goals of care that may change as dementia progresses, focusing on care goals that are important in maintain good relationships and connectedness.
The model aims to promote communication on how important each goal is in the context of advance care planning and how the goals can be achieved for individuals.
Further research is needed into how to apply the model in practice and how the goals relate to a care goal of life prolongation.
Introduction
Dementia is a progressive condition with people becoming increasingly dependent upon long-term care, while behaviour often changes and decision-making capacity decreases.1,2 This can affect the person’s relationships with their family and the community,3–5 and a palliative care approach including early initiation of advance care planning and continuous communication about care goals is recommended.2,3,6,7 Living with a progressive disease, often for years, implies that prioritised goals of care likely shift over time. 8
A dementia-specific care goals model was developed in a Delphi study by the European Association for Palliative Care (EAPC) reported in the EAPC white paper on palliative dementia care. It presented goals of ‘prolongation of life’ decreasing in priority towards the end of life, the goal of ‘maintenance of function’ remaining relevant and gradually prioritising ‘maximisation of comfort’9,10 (Figure 1(a)). However, the model achieved only a moderate consensus, with criticism, for example, that families were not included in the model (unpublished finding, personal communication).
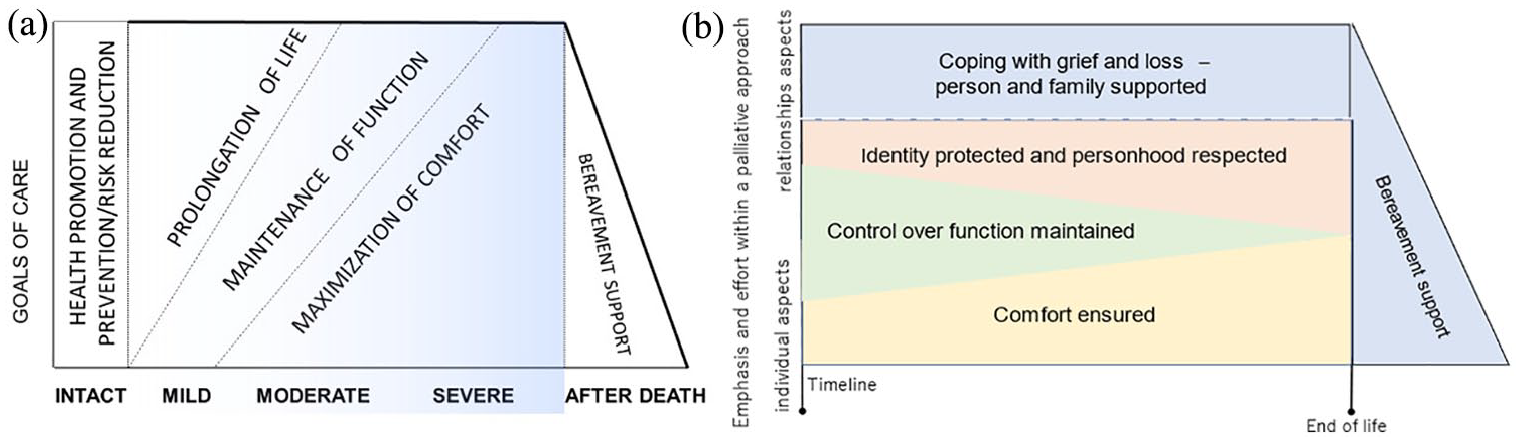
Existing (a) and newly developed final (b) models of dementia care goals. (a) A previous model - dementia progression and suggested prioritising of care goals in the European Association for Palliative Care dementia white paper. The goals of maintenance of function and maximisation of comfort are compatible with palliative care which aims to improve quality of life (van der Steen et al. 10 Copyright by the Authors. Reprinted by permission of SAGE Publications, Ltd.) (b) A model of palliative care goals towards the end of life for people living with dementia and family to support prioritising and detailing of effort to achieve individual care goals that contribute the most to quality of life until the end of life.
Since the EAPC care goals model was published in 2014, caring for people with dementia and models of care have become more of a global topic.11–13 Whereas the EAPC care goals model focuses on medical goals of care, studies from diverse countries have emphasised the importance of psycho-social-spiritual needs.14–16 Our eight-country meta-qualitative study showed that a good end of life with dementia in Western, Southern and Asian countries included multidimensional concepts such as: Care for caregivers; Identity being preserved; and Being connected. 17 Other studies from Western and Asian countries also support the importance of relationships such as providing compassionate care, and respecting personhood and dignity for people with dementia.18–21 Therefore, expanding of current care goals models for use in care planning is timely and relevant. In addition, international models can support communication about values and concepts that risk being overlooked in individual countries.
This study aimed to develop a multidimensional international palliative care goals model specific to dementia based on evidence and consensus among a Delphi panel of experts. A secondary aim was to explore if support for the model varied with panellists' characteristics.
Methods
We performed a Delphi study to develop a multidimensional palliative care goals model, aimed at achieving consensus among experts on the model and its potential use. Delphi studies are based on evidence and consensus in developing of content, multiple rounds of anonymous evaluation, with feedback to the panellists after each successive round.22–24 An online Delphi study allows input from experts from diverse geographical locations in a transparent manner. 22 We used five rounds with input alternating between an international project team of researchers, 17 and a Delphi expert panel (Table 1). This Delphi study was embedded in a larger Delphi study on advance care planning in dementia with surveys conducted in 2021–2022. 25
Methods to develop and refine a palliative care goals model specific to dementia.
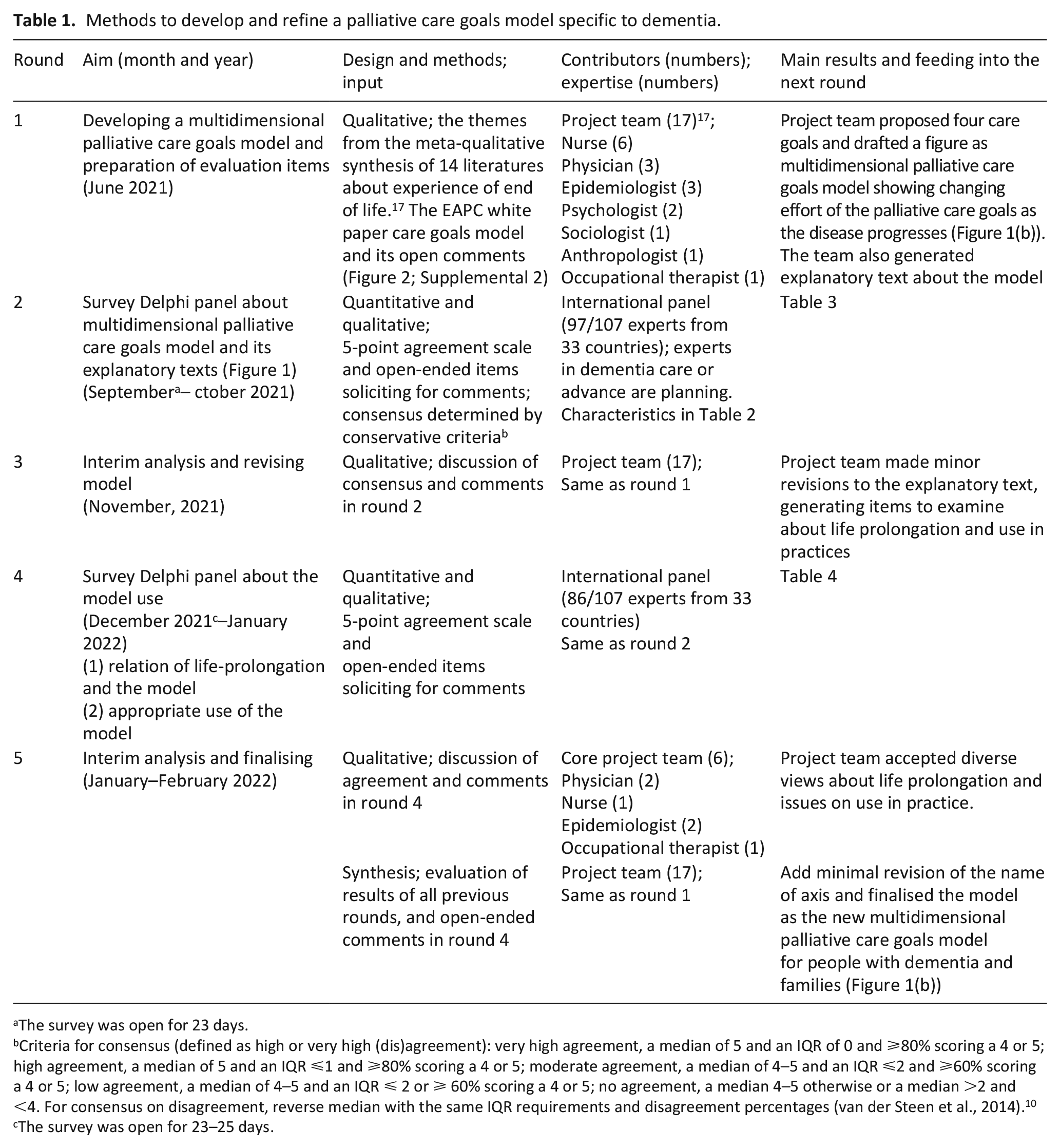
The survey was open for 23 days.
Criteria for consensus (defined as high or very high (dis)agreement): very high agreement, a median of 5 and an IQR of 0 and ⩾80% scoring a 4 or 5; high agreement, a median of 5 and an IQR ⩽1 and ⩾80% scoring a 4 or 5; moderate agreement, a median of 4–5 and an IQR ⩽2 and ⩾60% scoring a 4 or 5; low agreement, a median of 4–5 and an IQR ⩽ 2 or ⩾ 60% scoring a 4 or 5; no agreement, a median 4–5 otherwise or a median >2 and <4. For consensus on disagreement, reverse median with the same IQR requirements and disagreement percentages (van der Steen et al., 2014). 10 cThe survey was open for 23–25 days.
Delphi expert panel members
The inclusion criteria were: (1) expertise in advance care planning, dementia care or advance care planning in dementia more specifically, through practice, policy, research or clinical experience and (2) ability to complete online surveys in English.
Sampling and recruitment
Potential Delphi experts were identified via research and clinical networks, and from relevant publications in PubMed. We aimed for diversity in terms of expertise, continent of residence and occupation, with the aim of recruiting approximately 100 participants.
Round 1: Developing a multidimensional palliative care goals model and preparation of evaluation items
The project team of 17 researchers from eight countries, who had conducted the meta-qualitative study on a good end of life with dementia 17 developed an initial model (process of development in Figure 2).
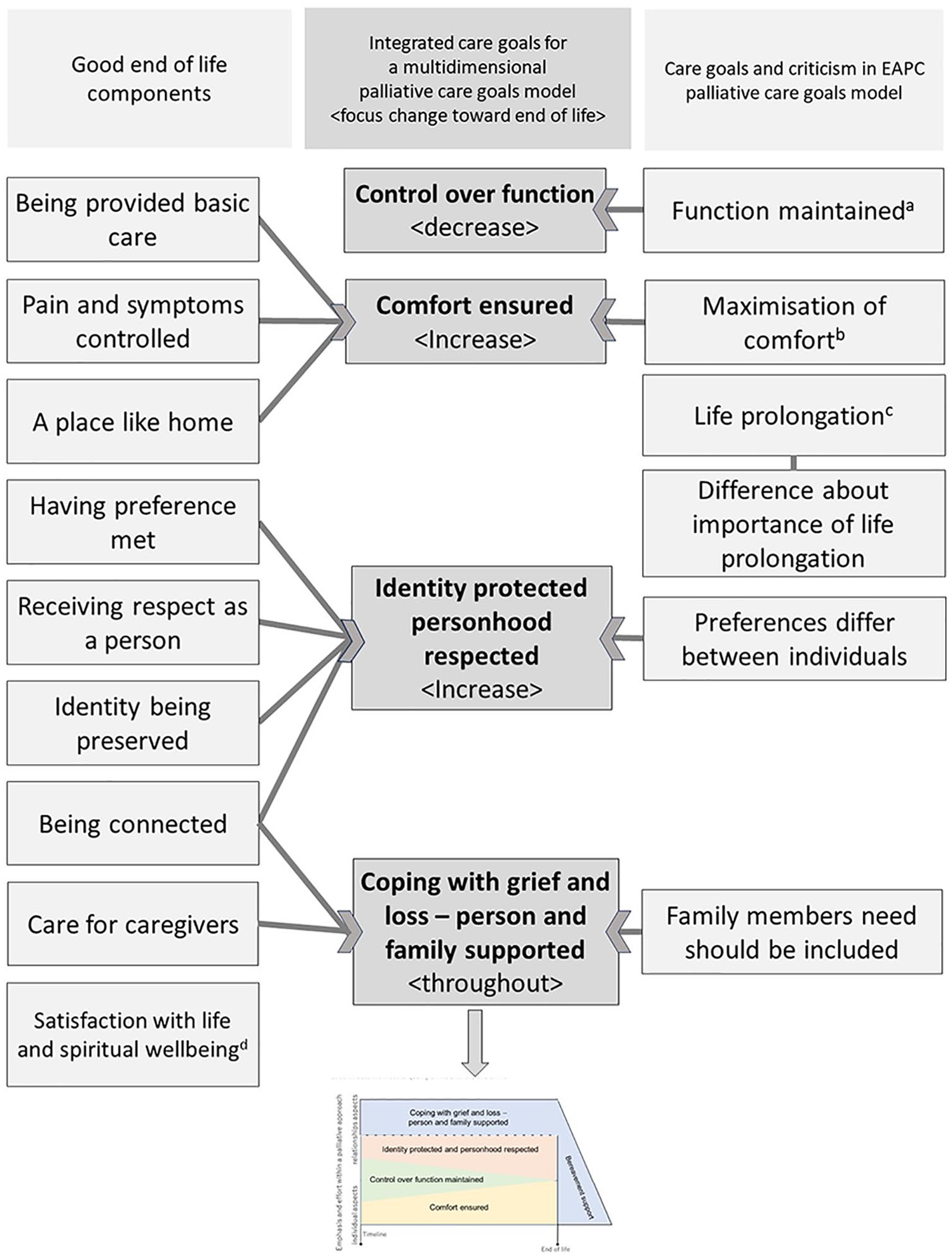
A process of development of an international multidimensional model.
The initial model was based on a previous eight-country meta-qualitative study in which the project team synthesised qualitative interview and observational data about experiences at the end of life of 121 people with dementia and 292 families. 17 The data had been collected during 2009–2020 in the UK, Ireland, Portugal, Germany, the Netherlands, Canada, Brazil and Japan.14,16,26–36 The synthesis process identified nine important components towards end of life 17 shown in the left column of Figure 2.
Based on the components, the project team discussed possible palliative goals of care that meet five criteria that were formulated during our discussions to consider the characteristics of appropriate care goals: (1) relevant to persons with dementia and family caregivers in different cultures–whether more individual or relationship centred–and in particular towards the end of life; (2) preferences tend to differ between individuals − therefore, cannot be taken for granted and needs to be discussed for each individual; (3) require appropriate effort by professionals and family caregivers to set feasible and achievable goals; (4) require variable effort over time indicating the notion of dynamic goals; (5) can involve trade-offs with other, competing goals of care which necessitates prioritisation.
Additionally, we reviewed panellists’ comments regarding the Delphi study for the EAPC white paper in dementia (Figure 1(a)). There were comments on the lack of inclusion of family members’ needs, preferences differing between individuals not being visualised and different importance attached to the three goals and change over time, in particular the goal of life prolongation. From these two sources (the meta-qualitative study and the earlier Delphi study), the team considered several drafts to present the care goals and also developed accompanying explanatory text.
Round 2: Survey Delphi panel and interim analyses
In September 2021, the potential panellists received an email inviting them to join the panel. An online pilot test was conducted with Leiden University Medical Center researchers on advance care planning in dementia. The online survey was developed with Castor Electronic Data Capture (EDC) System for Clinical Research Trials (Amsterdam, New York).
The evaluation items covered the proposed palliative care goals model, explanatory text, alternative formats for listing the goals of care and a comparison with the EAPC white paper care goals model (Figure 1(a)). We used statements that had been used to evaluate the EAPC white paper care goals model, 10 including those with reverse phrasing, such as ‘the interpretation of the model is problematic.’ The Delphi panellists rated levels of agreement on 1–5 agreement scales: strongly disagree (1); moderately disagree (2); neither agree nor disagree (3); moderately agree (4); and strongly agree (5). Based on median, inter-quartile range (IQR) and percent agreement, the consensus criteria (footnote to Table 1) were defined a priori with the same conservative criteria as previously used with the model in Figure 1(a). 10
Round 3: Interim analysis and revising the model
The results from Round 2 were tabulated and discussed in an interim analysis to inform revisions. A priori criteria for consensus including ‘high’ or ‘very high’ (dis)agreement are shown in Tables 3 and 4. 25 JTS and MaN summarised the comments from panellists using Microsoft Excel and proposed amendments to the project team. Unresolved issues were included in the next round.
Round 4: Survey Delphi panel about the model use
All panellists received the results of Round 2, and we presented a revised model and additional questions based on the work undertaken in Round 3. The questions solicited after the model’s usefulness in the panellists’ own countries, and a goal of life prolongation related to the condition of the person with dementia.
Round 5: Final analysis and conclusion of the study
As in Round 3, we analysed the panellists’ evaluations and comments. A core project team (KHD, LS, EIOV, MaN, TN and JTS) discussed whether a further round would be helpful.
Secondary analysis
To examine if panellists with specific characteristics were more likely to agree with the model and other items, we compared the following subgroups of panellists (a) European versus non-European residence; (b) medical professionals as responsible for medical treatment and endorsing care plans versus other professionals; (c) expertise in advance care planning in dementia specifically versus no such expertise specifically; (d) those with personal experience with advanced dementia care versus those without such experience personally.
Ethical considerations
Model development was part of the meta-qualitative study approved by the Graduate School and Faculty of Medicine Kyoto University (R1924-1), 25 April 2019. The advance care planning in dementia Delphi study protocol included evaluation of the model and was declared exempt from the Medical Research Involving Human Subjects Act by the Medical Ethical Committee Leiden Den Haag Delft, the Netherlands (N21.105). The protocol was registered at the WHO International Clinical Trials Registry Platform; NL9720, 7 September 2021. Confidentiality of individual responses was ensured by processing of coded data.
Results
Round 1
The initial model formulated by the project team consisted of four care goals, ranging from the individual level to the level of relationships and connectedness: Comfort ensured; Control over function; Identity protected personhood respected; Coping with grief and loss - person and family supported. To illustrate the changing emphasis on these four goals as dementia progresses, we created a model (Supplemental 2) and explanatory text (Figure 1). Several models were considered, including one that only listed the four care goals, one including life prolongation as a goal and one that emphasised comfort at the end as in the EAPC model. Delphi items were developed to rate the agreement level to the models and to invite open comments.
Round 2
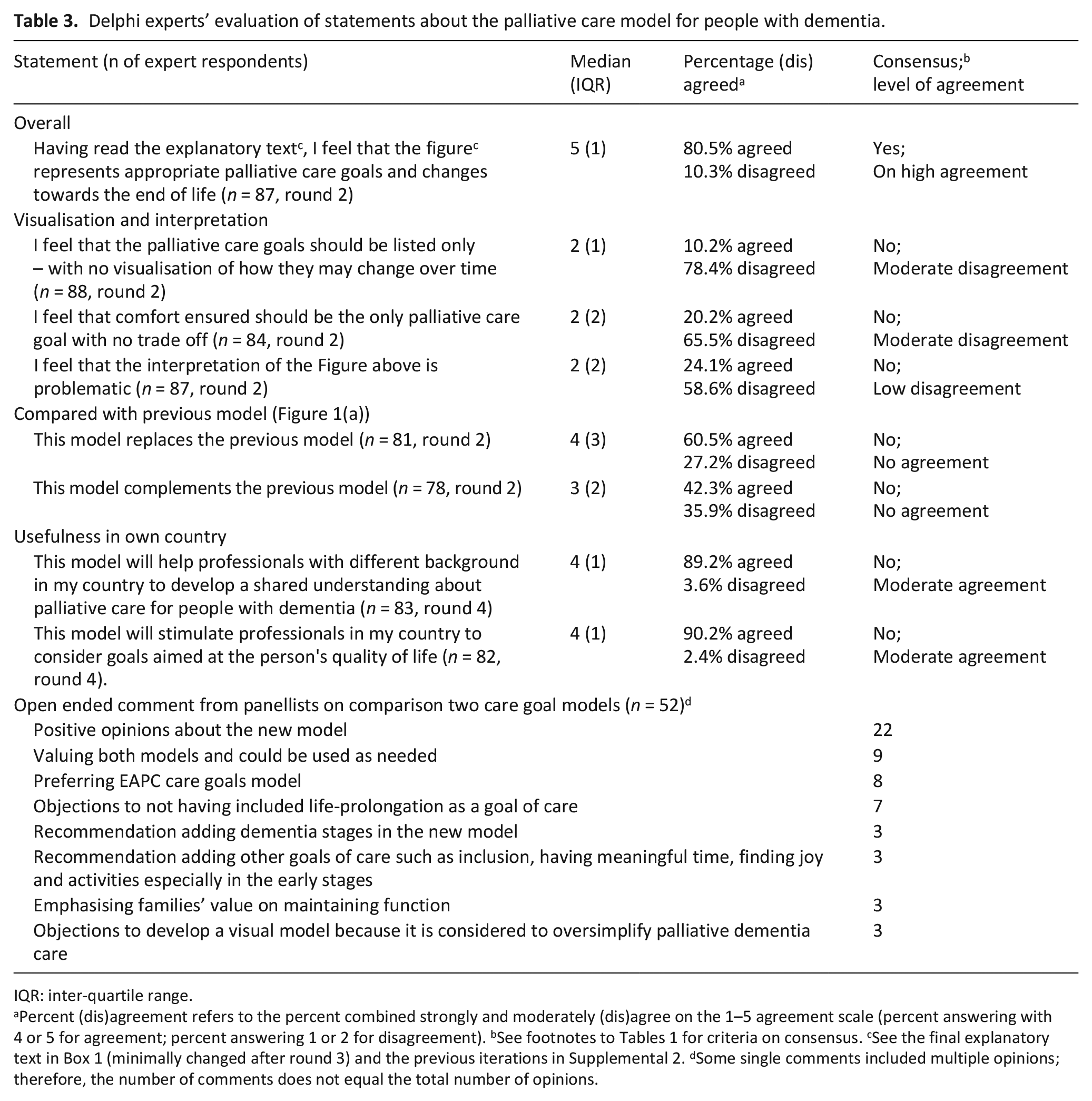
On September 2021, experts of dementia care and advance care planning were invited via email. Of 169 experts reached, 107 (63.3%) from 33 countries participated (response from Europe, 67.0%; from elsewhere, 58.7%). Half of respondents were medical professionals (53/107). Over half (60/104 − some missing values) had expertise in advance care planning in dementia specifically, and 72 out of 102 had personal experience (Table 2). Table 3 shows that the first iteration of the model achieved a consensus on representing appropriate palliative care goals and changes towards the end of life (80.5% agreed, median agreement rating 5, IQR 1). Two items that showed moderate disagreement were: (1) Not offering a visualisation of changes over time (10.2% agreed, 78.4% disagreed; median 2, IQR 1), and (2) Comfort should be the only palliative care goal with no trade off (20.2% agreed, 65.5% disagreed; median 2, IQR 2).
Delphi expert panellists’ characteristics.
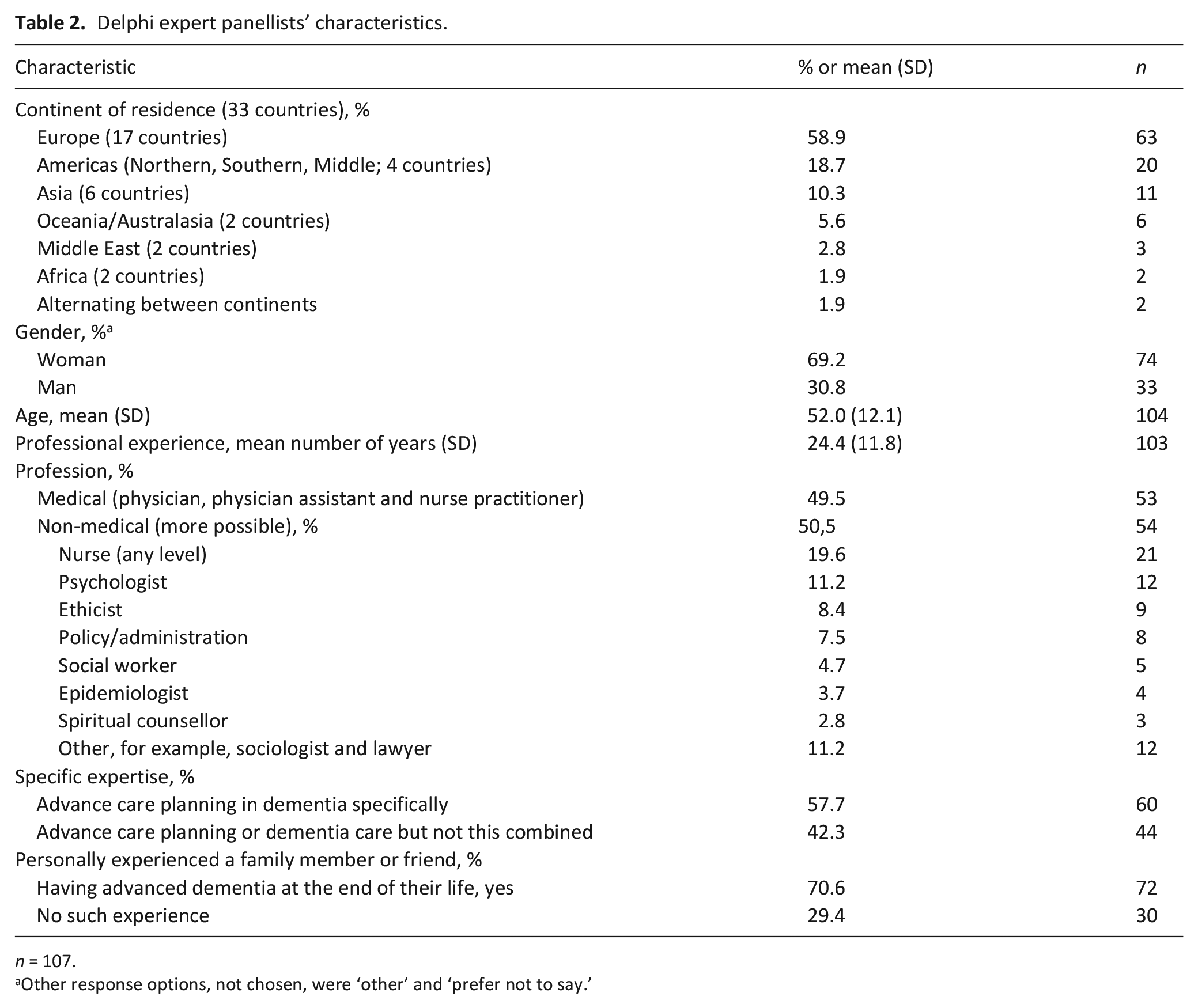
n = 107.
Other response options, not chosen, were ‘other’ and ‘prefer not to say.’
Delphi experts’ evaluation of statements about the palliative care model for people with dementia.
IQR: inter-quartile range.
Percent (dis)agreement refers to the percent combined strongly and moderately (dis)agree on the 1–5 agreement scale (percent answering with 4 or 5 for agreement; percent answering 1 or 2 for disagreement). bSee footnotes to Tables 1 for criteria on consensus. cSee the final explanatory text in Box 1 (minimally changed after round 3) and the previous iterations in Supplemental 2. dSome single comments included multiple opinions; therefore, the number of comments does not equal the total number of opinions.
Final version of the explanatory text that complements the care goals model. a .
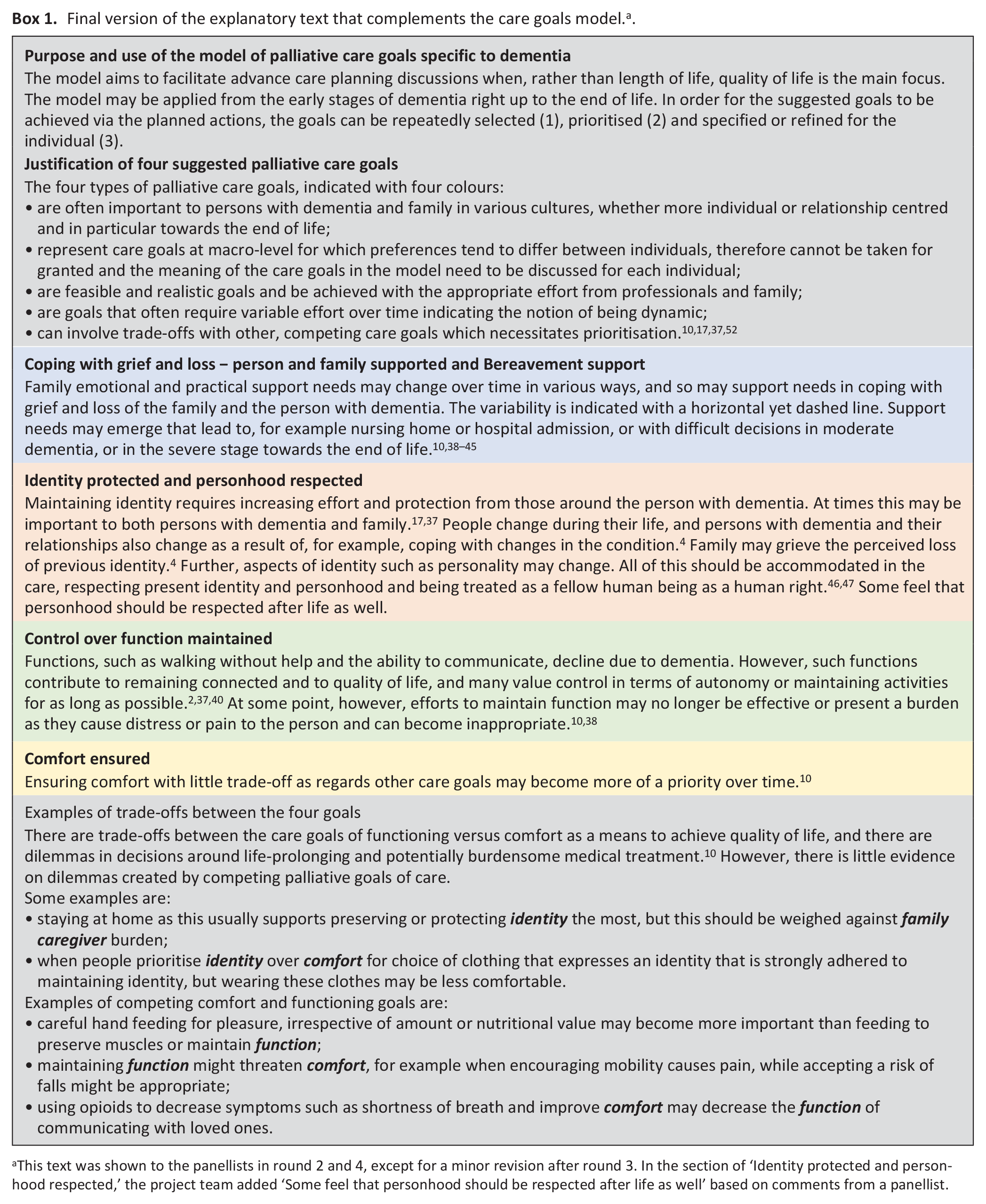
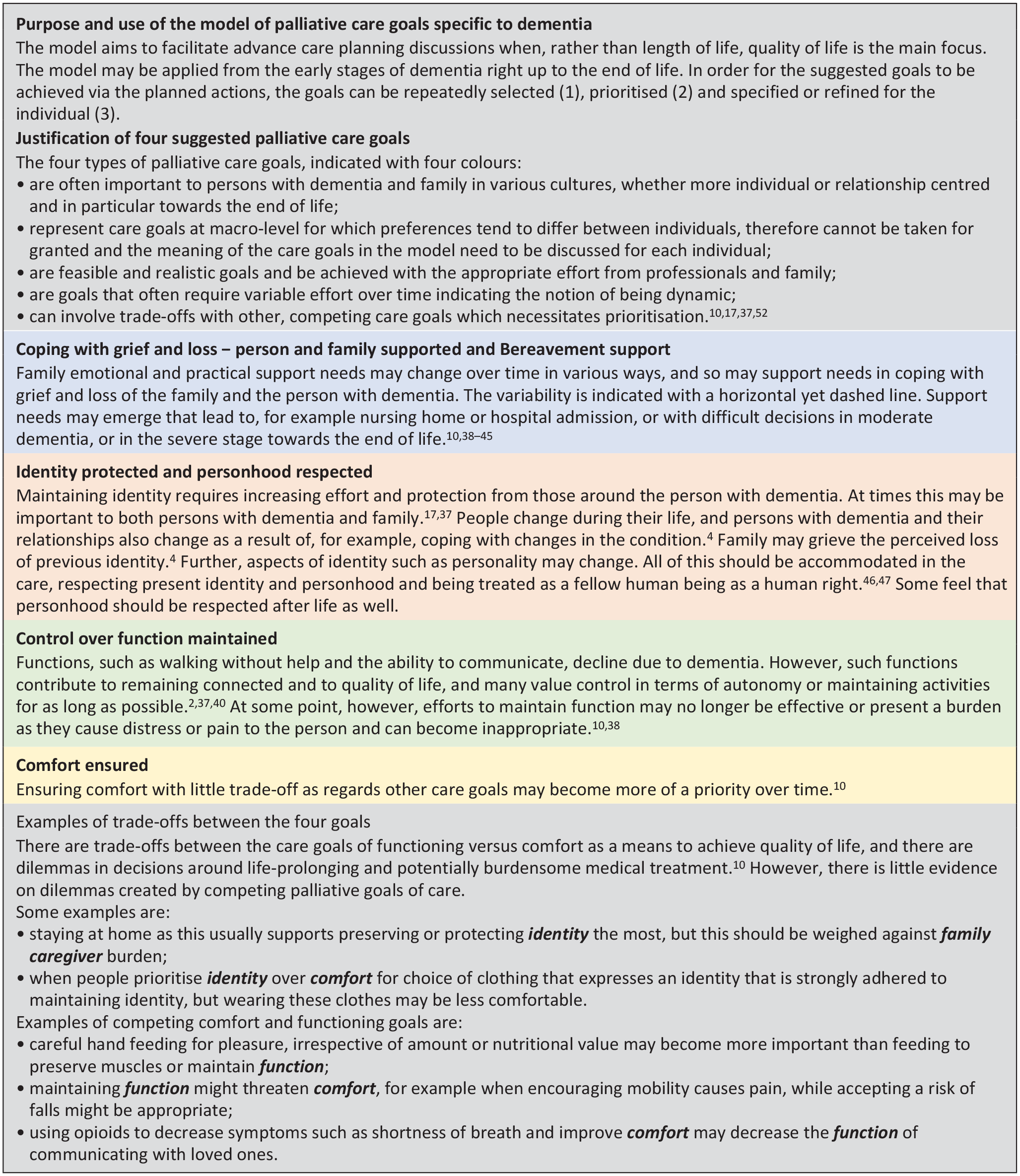
This text was shown to the panellists in round 2 and 4, except for a minor revision after round 3. In the section of ‘Identity protected and personhood respected,’ the project team added ‘Some feel that personhood should be respected after life as well’ based on comments from a panellist.
A total of 53 comments were made regarding comparing the new models with the EAPC care goals model of Figure 1(a). Of these (Table 3), 22 commented in a generally positive way, preferring the new model, while 8 preferred Figure 1(a), and 9 suggested both models are valuable and could be used as needed. Further, nine comments objected to omitting life prolongation as a goal of care (from Portugal, two; Netherlands, two; USA, Czech Republic, UK, Switzerland and Spain each one). In addition, three participants recommended adding dementia stages as in Figure 1(a) and two emphasised spiritual concerns after death.
Round 3
Reviewing the panellists’ feedback, the project team made minor amendments. We added the label ‘After death’ on the timeline and to the explanatory text, ‘Some feel that personhood should be respected after life as well’.
Additionally, having already achieved a consensus on the model, the project team decided to move on to projected implementation and consult the panel's opinion on the applicability of this model, who and in which place of care it would be appropriate to use it. Other statements referred to panellists’ degrees of agreement on usefulness of the model and the position of life prolongation in their own country, and to applicability of the model depending on comorbidity, care settings and appropriate users of the model.
Round 4
Table 4 shows that there was no consensus on the inclusion of life prolongation in this model, irrespective of comorbidities. Diverse views on life prolongation surfaced from 28 panellists’ comments. Six panellists commented that life prolongation should always be included in the model for its usefulness in practice. In contrast, 12 others would not include life prolongation because ‘it should not compete with other care goals’ (10 panellists) or ‘it is just beyond the scope of this palliative care goals model’ (two panellists). Ten other panellists did not clearly express an opinion on whether to include it, but commented it should be considered: when the person with dementia wishes (four panellists); at an early stage of dementia (three panellists); when the person has heart failure because it is not part of advanced dementia (two panellists); when medical intervention is helpful but may threaten other goals (one panellist).
Delphi experts’ rating of statements about life prolongation and applicability of the care goals model.
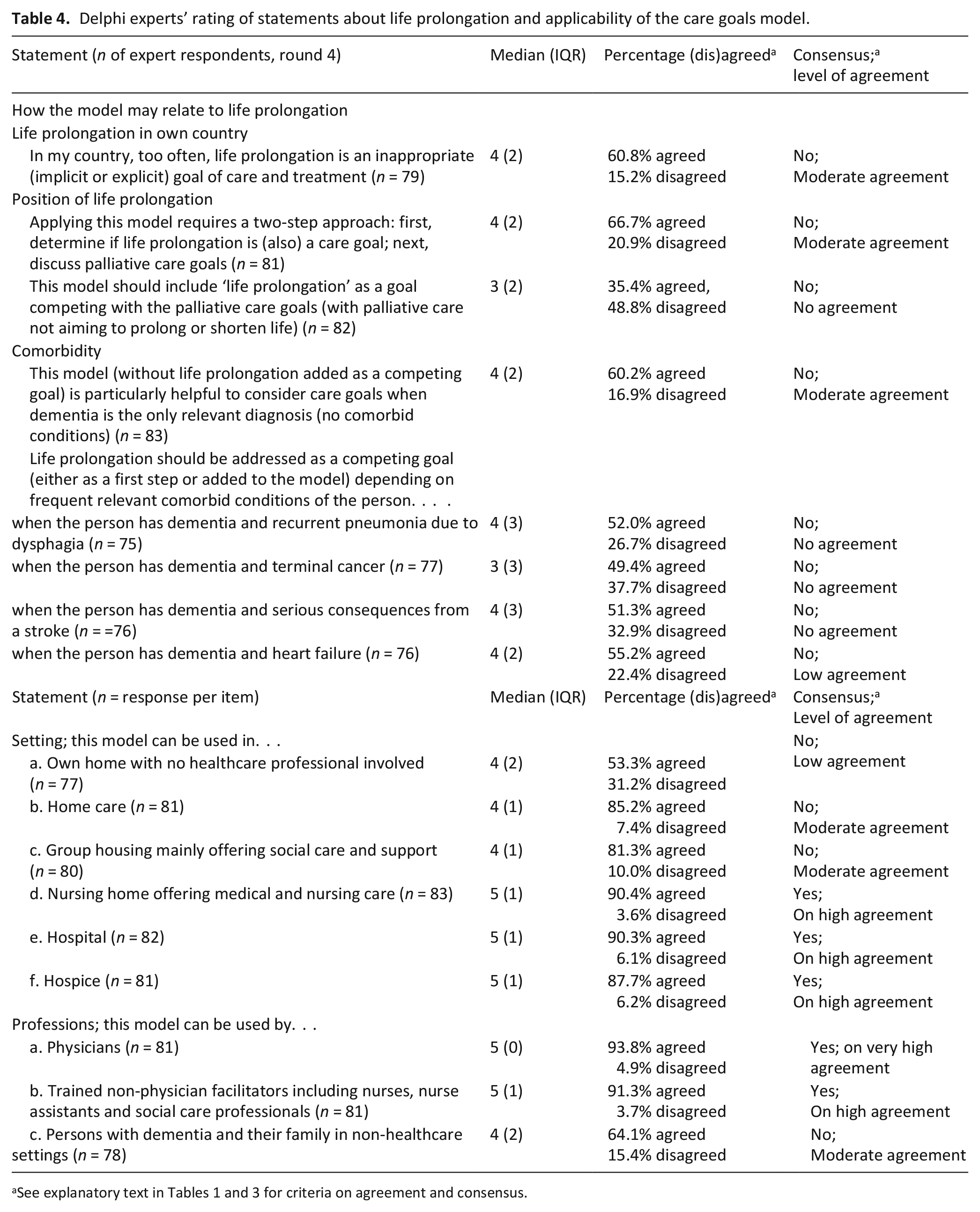
As for applying the model (Table 4), there was a consensus (high agreement) that the model could be implemented in nursing homes, hospitals and hospices. As well as a consensus with very high agreement on its use by physicians, there was a consensus with high agreement that it could be used by other trained healthcare professionals and social care staff.
There was no consensus on using the model in home care with no healthcare professional involved, which was consistent with the lack of consensus on the use of the model by persons with dementia and their families in non-healthcare settings. Suggestions included that a lay version with plain words would be needed if the person with dementia and their family were to use it on their own. Other comments referred to a need to clarify the labelling of the axes.
Round 5
The core project team discussed various issues and whether any new issues had appeared in Round 4 from panellists’ comments that would necessitate another round.
In summary, the main points raised and addressed were the following: (1) the X-axis label of ‘emphasis and effort’ was moved to the Y-axis so that the X-axis represented time only; (2) The lack of consensus in Round 4 among the panel on the position of life prolongation was also reflected within the project team; and (3) team discussions did not result in new insights which could feed into a next round. We agreed to accept the diversity in opinions on the position of life prolongation and decided to not proceed with a further survey round.
Subgroup consensus
The subgroup analyses (Supplemental 1) indicated that the model as presented the first time did not achieve a consensus in the subgroups of medical professionals, those with expertise in advance care planning in dementia specifically, and those with no personal experience. We found other subgroup differences, across the four subgroups, in consensus on the two statements about usefulness in the country of the panellists. The level of consensus about the use of the model in a home care setting differed across all four subgroups. Panellists from Europe did support the use of the model at home, as did panellists from non-medical professions, and no experience in advance care planning in dementia specifically or personally. In contrast, as in the total group, none of the items on life prolongation as a goal achieved a consensus among any of the subgroups.
Discussion
Main findings
We have developed a new palliative care goals model for people with dementia and their family based on a meta-qualitative study and a Delphi study. The model demonstrates how people can choose over time from four potentially competing goals of care regarding individuals, family and relationships. These include: Comfort ensured; Control over function maintained; Identity protected and personhood respected; Coping with grief and loss-person and family supported which concludes with ‘bereavement support.’
What this paper adds?
An EAPC white paper from 2014 defined optimal palliative care in dementia and presented a care goals model comprising medical care goals: Maintenance of function, Prolonging life; and Maximisation of comfort. The new model adds psycho-social-spiritual goals at the individual and relational level, and it has been supported by the diverse panel of experts from across the globe. The expert panel also agreed with its use by medical and social care professionals and applicability in other institutional settings.
The exploration of subgroups indicated that those with no medical or no professional advance care planning experience in dementia specifically were slightly less critical regarding the model. The most subgroup differences concerned the use of the models in home care, which may point to cultural, social or national policy differences in the quantity or quality of home care or how it is being organised and funded.48–51
A possible reason why no consensus was reached on including life prolongation to the multidimensional model may relate to the definitions of palliative care by World Health Organization and the international Association for Hospice and Palliative Care, which states that palliative care ‘intends neither to hasten nor postpone death.’52,53 Other possible reasons include that this goal is the most medically oriented, or else how participants define futile treatment in the context of dementia is affected by their personal or cultural perspective. However, issues about prolonging life remain important; for example, when considering whether to withhold the treatment of comorbid, intercurrent disease or whether to use (intravenous) antibiotics to treat pneumonia. Clearly, different people have different perspectives on the meaning of life prolongation and its relevance as a care goal in the use of this model.54,55
In practice, this international multidisciplinary model may broaden the perspective of healthcare providers to consider goals of care that extend beyond mere medical care and that may change over time as dementia progresses. The model may promote a focus on care goals that are important to maintain good relationships and connectedness, which add to positive care experiences for persons with dementia and their family.56,57 Using the model may be combined with existing decision-making tools.58–65 while explaining that the way to achieving the competing goals of care will vary depending on their personal values and preferences.
Of note, the model does not force any decisions to be made in individual cases, nor gives simple answers of care goals in different cultural and social background. To consider individual care goals, the process of communication is still indispensable by actively listening to individual needs with guidance to encourage addressing of specific topics represented in the model. As Davies et al. pointed out, some people do not wish to think about the future and prefer to think about everyday life. Further research may consider how the model may support resilience of the wider networks in the environment around the person with dementia. 66 Understanding diversity in meaning of life prolongation as a care goal is important for the use both of this model and the white paper model that also included it. The usefulness of life prolongation as a goal of care should also be understood from the perspective of persons with dementia and their family to best serve their interests.
Strengths and weaknesses
We did not include persons with dementia and family caregivers in the Delphi panel, but most experts had personally experienced a lived one with dementia at the end of life. The model may not fully capture diversity, also because experts who could not communicate in English were not included. We used rigorous predetermined criteria, that may have led to overestimation of the degree of disagreement between subgroups in our subgroup analysis. In addition, there was no authorisation of the model by an external body (called ‘external validation’ 22 ). Future studies should examine whether the international consensual model is applicable in practice and can improve the quality of care, and living and dying with dementia for those involved in diverse locations across the globe.
Conclusion
A new palliative care goals model for people with dementia and their family with psycho-social-spiritual goals achieved consensus amongst a diverse expert panel. Controversy around life prolongation as a goal of care remained and needs further research.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241234579 – Supplemental material for A palliative care goals model for people with dementia and their family: Consensus achieved in an international Delphi study
Supplemental material, sj-docx-1-pmj-10.1177_02692163241234579 for A palliative care goals model for people with dementia and their family: Consensus achieved in an international Delphi study by Mayumi Nishimura, Karen Harrison Dening, Elizabeth L Sampson, Edison Iglesias de Oliveira Vidal, Miharu Nakanishi, Nathan Davies, Wilson Abreu, Sharon Kaasalainen, Yvonne Eisenmann, Laura Dempsey, Kirsten J Moore, Sascha R Bolt, Judith MM Meijers, Natashe Lemos Dekker, Mitsunori Miyashita, Takeo Nakayama and Jenny T van der Steen in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163241234579 – Supplemental material for A palliative care goals model for people with dementia and their family: Consensus achieved in an international Delphi study
Supplemental material, sj-docx-2-pmj-10.1177_02692163241234579 for A palliative care goals model for people with dementia and their family: Consensus achieved in an international Delphi study by Mayumi Nishimura, Karen Harrison Dening, Elizabeth L Sampson, Edison Iglesias de Oliveira Vidal, Miharu Nakanishi, Nathan Davies, Wilson Abreu, Sharon Kaasalainen, Yvonne Eisenmann, Laura Dempsey, Kirsten J Moore, Sascha R Bolt, Judith MM Meijers, Natashe Lemos Dekker, Mitsunori Miyashita, Takeo Nakayama and Jenny T van der Steen in Palliative Medicine
Footnotes
Acknowledgements
We thank EAPC and the Delphi panellists for their contributions and support in conducting the Delphi study. Also, we sincerely thank Professor Tom Dening, MA, MD, PhD, FRCPsych, Dementia Research, School of Medicine, University of Nottingham, UK, for his help in language editing of this manuscript.
Author contributions
MaN, TN and JTS contributed to acquisition. MaN and JTvdS jointly drafted the article. The core project team members (MaN, KHD, LS, EIOV, MiN, TN and JTS) contributed substantially to interpreting the survey findings and finalising the model. All authors made a substantial contribution to the concept or design of the work, and to analysis or interpretation of the data. Also, all authors revised the article critically for important intellectual content, and approved the version to be published. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was performed with the same expert panel as with EAPC’s ACP Delphi study, but this study was not designed by the EAPC ACP in dementia task force. This separate study was not conducted as part of the remit of the EAPC task force. There are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MaN and TN are supported by the Graduate School of Kyoto University, Japan. JTvdS is supported by a European Research Council (ERC) Consolidator Grant (Agreement ID 771483).
ORCID iDs
Data availability
Part of the data that support the findings of this study are available on request from the corresponding author, JTvdS, for the data provided by panellists who provided informed consent for reuse for other research. There was no consent to provide open access to the data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.