
Abstract
Background:
Palliative care is characterised by heterogeneous patient and caregiver populations who are provided care in different health systems and a research base including a large proportion of observational, mostly retrospective studies. The inherent diversity of palliative care populations and the often inadequate study descriptions challenge the application of new knowledge into practice and reproducibility for confirmatory studies. Being able to define systematically study populations would significantly increase their generalisability and effective translation into practice.
Proposal:
Based on an informal consensus process by active palliative care researchers challenged by this problem and a review of the current evidence, we propose an approach to creating more comparable cohorts in observational (non-randomised) palliative care studies that relies on defining the study population in relation to a fixed, well-defined event from which analyses are built (‘anchoring’). In addition to providing a detailed and complete description of the study population, anchoring is the critical step in creating more comparable cohorts in observational palliative care studies. Anchoring can be done with respect to a single or multiple data points, and can support both prospective and retrospective data collection and analysis.
Discussion:
Anchoring the cohort to reproducible data points will help create more comparable cohorts in palliative care whilst mitigating its inherent heterogeneity. This, in turn, will help optimise the generalisability, applicability and reproducibility of observational palliative care studies to strengthen the evidence base and improve practice.
Keywords
Palliative care is a referral-dependent specialty, with a research base that comprises a large proportion of observational studies.
Lack of agreed referral criteria contributes to the heterogeneity of population(s) served by palliative care, while the often inadequate descriptions of study populations or settings contribute to the variability in patient and caregiver data presented to clinicians.
Collectively, this limits the uptake of new research knowledge into practice and the ability to conduct meaningful confirmatory studies in palliative care.
The question is ‘how do we create more comparable cohorts from observational data in palliative care research?’
We propose that a critical step in creating more comparable cohorts in observational palliative care studies is to define the cohort in relation to fixed, well-defined events for the analyses (‘anchoring’).
Anchoring the cohort to reproducible data points will help mitigate the inherent heterogeneity of populations in palliative care, as well as help to optimise the applicability (by clinicians) and reproducibility (by researchers) of observational palliative care studies to improve clinical practice and strengthen the evidence base.
Introduction
There are fundamental challenges in palliative care that limit the uptake of new research knowledge into practice and the ability to conduct meaningful confirmatory studies:
1) palliative care is a referral-dependent specialty, yet without agreed referral criteria; and
2) its research base comprises a disproportionately large percentage of observational studies, yet with often inadequate descriptions of the populations or settings in which the studies were conducted.
The lack of standardised referral criteria contributes to the heterogeneity of population(s) served by palliative care, while the often inadequate study descriptions contribute to the variability in patient and caregiver data presented to clinicians. This creates challenges for clinicians to confidently compare study populations with the population that they serve and assess applicability of findings, and for other researchers to replicate studies in a meaningful way – both basic tenets of scientific research. 1
The challenge of palliative care as a referral-dependent specialty
Palliative care encompasses a wide range of care settings, models of care 2 and funding streams. 3 Palliative care is characterised by many entry points to access the service across settings, with differing times from referral to death (or discharge) for each service.4,5 Around the world, palliative care serves diverse patient and caregiver populations, with profiles directly influenced by local determinants relating to the:
recognition of palliative care needs (reflected in the timing of referral in relation to the diagnosis of a life-limiting illness or death; source of referral; clinical and sociodemographic profile of people referred; diagnoses of those referred);5 –7
services provided (reflected in mechanisms for initiation and acceptance of referrals); 5
disease burden (due to life-limiting illnesses prevalent in each community/region/country).8–11
Access to services can also vary. Fewer than 60% of people with serious, life-limiting illnesses access specialist palliative care services 12 in high income countries.8,13,14 Access is even lower in low- and middle-income countries.10,11
Attempts to standardise referral criteria for palliative care have been made but are not universally agreed upon nor always relevant to particular patient sub-groups or health service settings.15,16 The lack of agreed national and international referral guidelines 17 creates patient and caregiver cohorts that are much less homogeneous in palliative care than in most other clinical disciplines. 18 Differences in life expectancy, age, cognition, functional status, comorbidities and symptom profiles are all reflected in the populations referred to specialist palliative care services.11,19 These variations limit the comparability of people with palliative care needs in both research (generalisability 18 ) and clinical practice (applicability 20 ), thus limiting the impact of much of the research that is undertaken.
The challenge of observational palliative care studies
The number of clinical trials in palliative care that can directly influence the care offered to patients has increased steadily in the last two decades, overcoming questions about their appropriateness and feasibility in this setting.17,21,22 However, observational studies continue to dominate in the evidence base.7,23,24 Though unable to assign causality to outcomes, 25 observational studies are able to leverage existing funding data 26 (e.g. Medicare) and data routinely collected by healthcare services. Often though, these studies may present an incomplete picture of the study population because they might lack detail on the services’ profiles and processes, the clinical and sociodemographic descriptors of the population(s) served or the disease burden of the region or country in which the research is based. 9 These studies also often report on the patient population seen by a particular specialist palliative care service, 26 which may vary widely from populations seen by other palliative care teams, even in the same city or country. 9 As such, the variability of their data severely restricts comparisons between studies, their replication 1 in subsequent research and applicability in clinical practice or health policy.
Ways forward that are methodologically sound
If observational studies are to be used as a major source of the evidence base and inform clinical practice (and some of these studies will be generating the best level of available evidence for the questions they are posing), it is important to ensure the participants within these studies are being characterised in a way that facilitates such comparisons. Being able to define systematically study populations would significantly increase their applicability and more effective translation into practice. The fundamental question is ‘
Our proposal builds on examples of observational studies that have been successful in achieving more comparable populations by their approach to analysis. The examples from the evidence base were selected by the authors through informal consensus. It is hoped that the suggested approach to resolving issues of heterogeneity in observational (as well as quasi-experimental; henceforth collectively referred to as ‘non-randomised’) palliative care studies will be discussed and further refined in future research.
Why population descriptors are not enough: a worked example
In observational studies in palliative care, describing the population at the point of entry to the study (even with well-defined eligibility criteria) is insufficient for proper comparisons of the study cohort.21,25 Lack of agreed referral criteria means people will be entering and re-entering services provided by palliative care at multiple time points when put in the context of their illness. Most often, the point of referral to palliative care cannot be replicated in studies conducted in other centres (e.g. due to differing service, funding and patients’ characteristics), 27 so the different time points of referral will create heterogeneity in the data for the population being studied, almost certainly negating any chance of applying the study’s findings or replicating it meaningfully in another service.
As an illustration, consider a hypothetical cohort study with prospectively collected data on functional status 28 for two populations from two different services, with median times from referral to death of 28 days (population A) and 49 days (population B), respectively. The two patient cohorts will have two different trajectories, D0–D28 and D0–D49 (where D0 in both cases is the day on which referral occurred and D28 and D49 are the times of death for each population, respectively). In analyses, data could be aligned with the time of referral as D0 or with the time of death as D0. In this context, given the differences in the time of referral to death (4 weeks follow-up for service A and 7 weeks follow-up for service B), if the alignment is with:
time of referral (Figure 1(a)), there will be marked differences at D7, D14 and D21 (the time points of interest) between what is reported for populations A and B (in this case, functional status). This will generate very different results and make aggregating those outcomes meaningless. The two populations will not be comparable in research, and it would be difficult for the reader to replicate the study or apply its findings to their own service setting.
time of death (Figure 1(b)), data collected at the same time points of interest D7, D14 and D21 for populations A and B will potentially be more comparable and increase the likelihood that the findings can be reproduced because the result would create a more homogenous population.
One might argue that providing a detailed description of populations A and B in Figure 1(a) and (b) will mitigate some of the challenges created by the different time points of the referral. However, the data collected for the two populations at the time points of interest for the analysis will remain different when analysed from referral. A good description is essential but not sufficient to create a more comparable population and, therefore, generate more informative findings.

(a) Anchoring the analysis at time of referral for two different patient cohorts A and B to create a combined study population C shows that the two populations over 4 weeks from time of referral are demonstrably different. Using improvised data, the graphs present hypothesised trajectories where x axis is time (in days) and y axis is functional status (Australia Karnofsky Performance Scale (AKPS) 28 ) and (b) anchoring the analysis at time of death for two different patient cohorts A and B to create a combined study population D shows that the two populations over 4 weeks from time of death backwards are more comparable. Using improvised data, the graphs present hypothesised trajectories where x axis is time (in days) and y axis is functional status (Australia Karnofsky Performance Scale (AKPS) 28 ).
Creating more comparable cohorts in observational palliative care studies: a proposal
Prospective clinical trials have eligibility criteria that mean that the study population is well defined, regardless of the time in the disease trajectory when they are referred to palliative care services. In a randomised controlled trial, having established eligibility, there is also a finite anchor point from which subsequent outcomes are measured – the moment of randomisation, in the context of an intervention being delivered in a controlled manner. Randomisation creates an objective and reproducible anchor point that, in tandem with careful description of the population (through the eligibility criteria) enables clinicians to consider the study’s applicability and researchers to reproduce the study in other settings. When randomisation is not possible or not desirable (because of the nature of the research question), other methods to optimise applicability, comparability and reproducibility are required.
Providing a complete and consistent description of the study population is an obvious first step to ensure the cohort in observational studies is well defined.15,16 A detailed description enables better comparison between study populations as well as comparison with the clinical population to which the findings could be applied, 7 thus providing a helpful reference point for clinicians as they consider the applicability of the study’s findings for the patient and caregiver population(s) they serve. Description of the population is unlikely to be sufficient given that individuals referred to specialist palliative care services differ so greatly as do the service models used to provide care.29,30
We would like to propose that in the context of observational (as well as quasi-experimental) studies the critical step for creating more comparable cohorts is to:
define the study population in relation to a fixed, well-defined event (henceforth referred to as ‘anchoring’).1,31 This event would become the reference point (‘an anchor’) from which the analyses are subsequently built.
Anchoring
The use of fixed, well-defined events in cohort selection and data analyses is the critical step in creating more comparable cohorts in observational studies in palliative care. Importantly, reproducibility of results can only be achieved when well-defined data points are selected as anchors, and the study cohort and outcomes are described and analysed with those anchors in mind. This means selecting data points for which there are agreed definitions (i.e. reproducible criteria), and which are described and illustrated clearly (e.g. by using design diagrams).1,31 In this context, referral to a palliative care service without objective criteria for referral could not be an anchor.
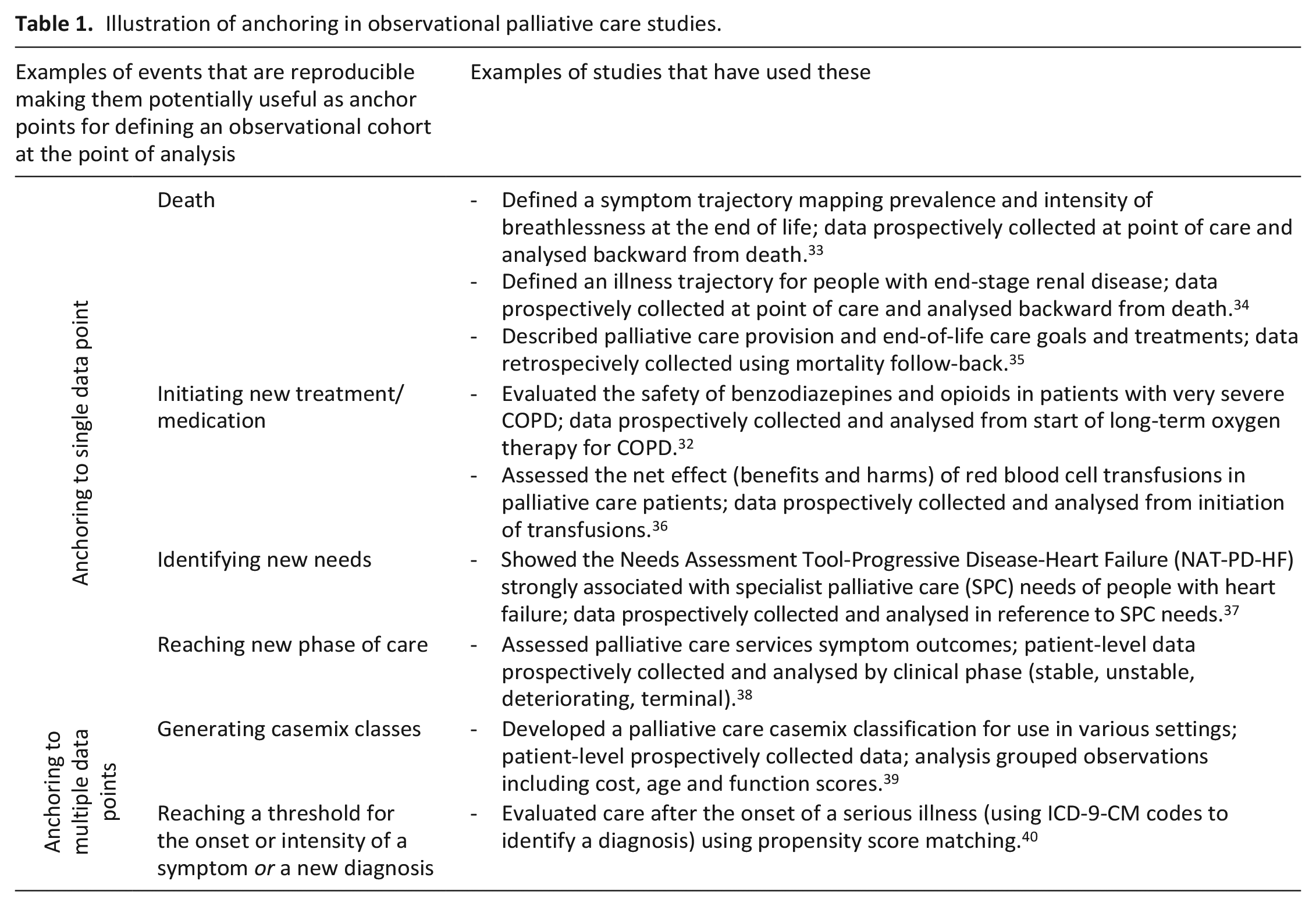
From the study population perspective, anchors will be sentinel events which help ascertain the study entry date to allow replication of those in future studies or application to the population served by a clinician. Although in principle sentinel events can be caregiver and health service related (e.g. demographics and contact with health services, respectively), in most cases, the sentinel events are patient events. These events can be temporal (e.g. time of death) or non-temporal (e.g. reaching a certain clinical threshold such as a level of function). The anchoring can be done with respect to a single data point or multiple data points (including, potentially, propensity score matching). From the analysis perspective, the anchoring can be done retrospectively (e.g. using the date of death and calculating events of interest backwards 27 ) or prospectively (e.g. using the date a treatment is being initiated and calculating events of interest subsequently 32 ). Importantly, the choice of anchors should be guided by the research question. Once the anchor is chosen, a key assumption is that appropriate statistical methods will be used for the analysis to answer the research question.
Some initial examples of potential anchors are outlined in Table 1, with some potential strengths and weaknesses outlined in Table 2. Future work will refine and expand this selection and explore their characteristics and suitability in order to strengthen the evidence underpinning this framework.
Illustration of anchoring in observational palliative care studies.
Potential strengths and weaknesses of suggested anchors for analysis in observational palliative care studies.

NRSs: numerical rating scales; CRSs: categorical rating scales; PROMs: patient reported outcome measures.
Anchoring to a single data point
The study population can be defined with respect to a single event (e.g. time of death; people reaching a particular level of functional decline or frailty; initiation of a particular treatment because a certain clinical threshold (e.g. intensity of pain) has been reached). Similarly to randomisation in clinical trials, such anchors will provide a reference point at which time the cohort is defined (e.g. the initiation of a treatment) and from which outcomes of interest are subsequently measured and analysed (e.g. the person’s response to that treatment), thus helping create a more homogenous study cohort. Some heterogeneity would always remain no matter what steps are taken in the process of defining the cohort, anchoring to a well-defined data point would increase the value of information that can be obtained for readers and strengthening the capacity for translation into clinical practice or conduct of confirmatory studies.
Anchoring to multiple data points
The study population can be defined by anchoring to multiple patient events which can be any combination of individually available data points or, at its most sophisticated, by creating a composite score for the whole sample in propensity matching. A propensity score as a summary of multiple patient-oriented characteristics helps create comparable cohorts ‘to account for observable differences between individuals receiving a treatment [the intervention group] and individuals receiving usual care’. 41 Propensity score is the preferred method for ‘reducing the effects of selection bias on the estimation of treatment effects on outcomes in observational studies’, 25 though caution is needed to counteract a possible increase in random error in such cases. 42 Closest to the quality of evidence generated by a randomised controlled trial, propensity matching creates a composite score for the whole sample, with variables needed to be carefully selected to manage confounders. Although propensity score matching is challenging for palliative care as it requires large numbers of observations to create it, it has been successfully used.40,41,42
Why might anchoring be useful?
The lack of national and international criteria for referral to palliative care services means there is currently no specific clinical threshold for describing the population(s) with palliative care needs. This can be particularly challenging for observational studies which leverage robust, yet diverse datasets from a variety of sources including by palliative care services themselves. Identifying fixed events (anchors) can help define populations in cross-sectional and longitudinal cohort studies and improve the ability to compare like-with-like within the illness or symptom trajectory of a patient cohort. In longitudinal studies, once the anchor is defined, discrete time points can be determined at which to measure the outcomes of interest in individuals and populations. 43 As such, anchorning can help define trajectories for whole diagnostic groups 34 and typology of trajectories, 44 including for symptoms and concerns for people at the end of life.27,45,46
Data can be collected either prospectively (e.g. at point of care) or retrospectively (e.g. from medical records) for each outcome of interest. Of note, hypotheses generated by retrospective analyses ideally should be confirmed with prospective data collection. The analysis can also be done prospectively or retrospectively. Which method of analysis is chosen will have implications for how the cohort is characterised. 47 For example, it is very clear from two papers exploring the same research question (within the same patient cohort) with forward trajectories in one, and backward trajectories from death in the other that what is reported for the cohort is likely to be different – like looking through the opposite ends of a telescope. When looking backward from death, people with end-stage renal disease (conservatively treated, i.e. not on dialysis) seem to be relatively stable then sharply decline in the last 1–2 months before death. 34 When looking forward there is great individual variation in symptom burden in the last 12 months before death, 44 reflecting the wide heterogeneity in where individuals are in their disease trajectory, in part because time of death is not known prospectively. This seems to suggest that retrospective analyses (e.g. from time of death) generate a more homogenous clinical profile of a given patient cohort while prospective analyses delineate individual nuances across that population for the same period of time. When considering which approach to implement, it may be worth exploring both options to map out trends for the population of interest as well as individual trajectories to help support a more personalised treatment and symptom management. Given that people may have a very different end of life, understanding ‘last month’ or ‘last three months’ is not only about trying to reduce heterogeneity, but also about having meaningful clinical insight into what to expect for that person.
In the context of observational data, there will always be residual heterogeneity and, therefore, variance. However, defining the study population in relation to fixed, well-defined events (anchors) may help reduce this variance where it is artefactual, thus creating more comparable analytic sets and clinical populations.
Implications for research
Previous studies have proposed population descriptors15,16 and outcome measures 4 for studies in palliative care. Defining suitable fixed, well-defined events as anchors for cohort selection and analysis that directly link to the clinical and health service profile will provide a useful method to creating more comparable cohorts from observational data and help increase applicability to clinical practice and replicability of study findings. Future work should focus on delineating the most suitable measurement candidates in a well-defined framework.
Conclusions
The challenges posed by the heterogeneity of populations with palliative care needs will vary depending on the research questions, as will the possible solutions. Anchoring the cohort selection and analysis to clearly reproducible data points will help create more comparable cohorts in palliative care whilst mitigating its inherent heterogeneity. This, in turn, will help optimise the applicability and reproducibility of observational (non-randomised) palliative care studies to strengthen the evidence base, and improve practice and policy.
Footnotes
Acknowledgements
The authors would like to thank Ms Debbie Marriott for her expertise and generous assistance in preparing this manuscript for publication.
Author contributions
All authors contributed to the conception, writing and final approval of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by discretionary funds held by the academic team at the Faculty of Science, Medicine and Health at the University of Wollongong, Australia. Professor Fliss Murtagh is a National Institute for Health Research (NIHR) Senior Investigator in the United Kingdom (UK); the views expressed in this article are those of the author(s) and not necessarily those of the NIHR, or the UK Department of Health and Social Care.