
Abstract
Background:
Digital legacy refers to the online content available about someone following their death. This may include social media profiles, photos, blogs or gaming profiles. Some patients may find it comforting that their digital content remains online, and those bereaved may view it as a way to continue bonds with the deceased person. Despite its growing relevance, there is limited evidence worldwide around the experiences of palliative care professionals in supporting patients to manage their digital legacy.
Aim:
To identify palliative care healthcare professionals’ experiences of supporting patients receiving palliative care in managing digital legacy as part of advance care planning discussions.
Design:
A constructivist grounded theory approach was used to understand healthcare professionals’ experiences of managing digital legacy. Semi-structured interviews were carried out.
Setting and participants:
Participants were 10 palliative care healthcare professionals from across the multidisciplinary team working in a hospice in the North-West of England.
Results:
Four theoretical categories were found to revolve around an emergent theory ‘understanding the impact of digital legacy’ which describe the experiences of palliative care healthcare professionals managing digital legacy as part of advance care planning. These were ‘accessing digital legacy’; ‘becoming part of advance care planning’; ‘impacting grief and bereavement’; and ‘raising awareness of digital legacy’.
Conclusions:
The emerging theory ‘understanding the impact of digital legacy’ offers insight into the knowledge and experiences of healthcare professionals working in a palliative care setting. Digital assets were viewed as being equally as important as physical assets and should be considered as part of advance care planning conversations.
Keywords
The use of digital technologies to create personal content is increasing, meaning that people are creating digital content which will be left following their death.
Evidence suggests that palliative care healthcare professionals have little knowledge and understanding of digital legacy, which might be limiting their confidence to open conversations in this area.
Digital legacy has been used to support grief and bereavement through platforms such as social media, digital photographs and online gaming platforms.
Palliative care healthcare professionals believe that managing digital belongings is as important as managing physical belongings.
Palliative care healthcare professionals require education to improve their knowledge and understanding of digital legacy.
Digital legacy should become part of advance care planning conversations.
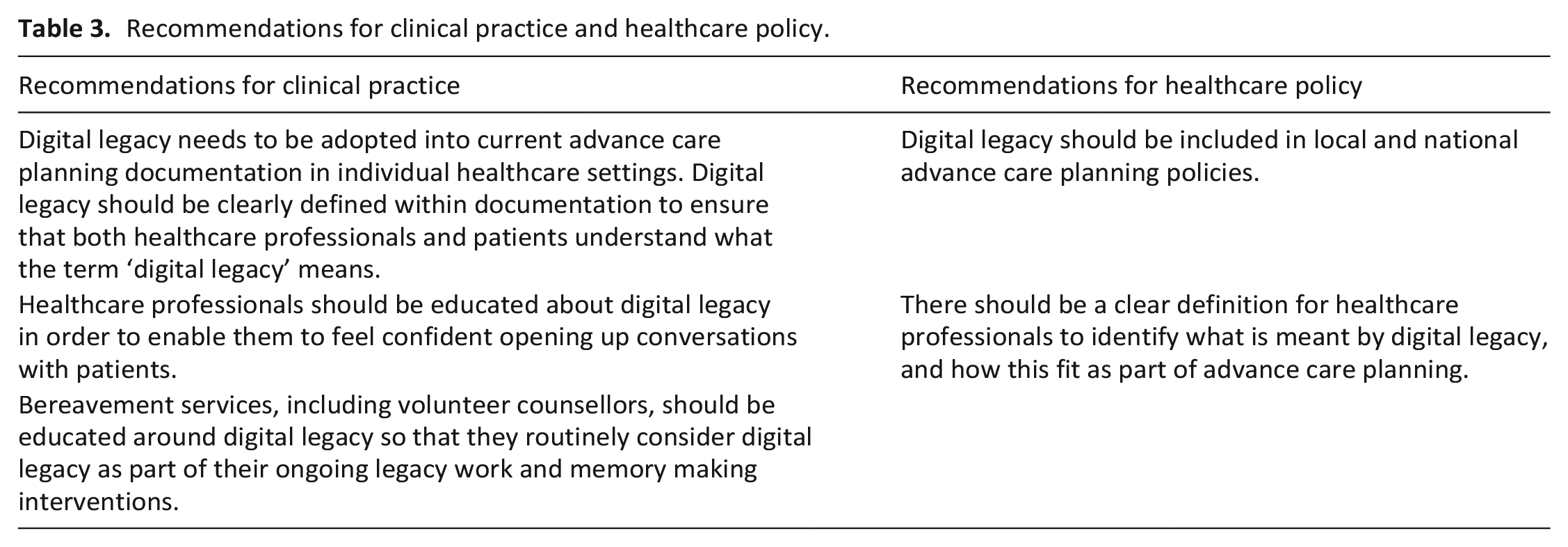
Digital legacy should be included in local and national advance care planning policies, and should be explicitly mentioned in advance care planning documentation.
Healthcare professionals should be educated about digital legacy, and there should be a clear definition for healthcare professionals to identify what is meant by digital legacy, and how this fits as part of advance care planning.
Professionals offering bereavement and pre-bereavement services, including social workers and volunteer counsellors, should be educated around digital legacy so that they routinely consider digital legacy as part of their ongoing legacy work and memory making interventions.
Background
Global developments in technology have meant that we are seeing a rapid growth in the progress and use of technology in our day to day lives. 1 This has included an increase in internet access 2 and smartphone use worldwide. 3 These developments have accelerated since the COVID-19 pandemic. 4 With greater access to the internet many people, across all age groups, are spending time creating and broadcasting their own online content using platforms such as You Tube, Instagram, Tik Tok and Snapchat.5,6 It is predicted that by 2100 4.9 billion Facebook users will have died. 7 This emphasises the importance of more discussion around digital death, with potential future issues surrounding access to these accounts (e.g. in relation to hardware updates, financial security of social media groups and data storage costs). 7
Digital legacy can be described as the digital information that is available about someone following their death. 8 This can include social media profiles, email accounts, photographs, websites and gaming profiles.
It is vital for palliative care healthcare professionals to understand digital legacy, and how digital content is managed after death or bereavement. Consideration of digital legacy could be a part of advance care planning. Advance Care Planning (ACP) is defined by the National Institute for Health and Care Excellence (NICE) 9 as an opportunity for people to plan their future care and support, while they have the capacity to do so. Advance care planning can lead to enhanced care through better understanding of patient’s wishes and improved communication between patients and healthcare professionals.10,11 However, healthcare professionals must be well educated in order to feel comfortable and confident in engaging with advance care planning discussions.12–15 This includes understanding the impact early advance care planning could have on digital memory making. 16
While advance care planning is a key issue in palliative care internationally,9,17,18 little is known about what health care professionals understand about digital legacy. Furthermore there is a lack of evidence to support the use of digital legacy as part of advance care planning conversations.
Methods
Aim
To explore palliative care professionals’ experiences with discussing and addressing digital legacy in advanced care planning.
Study design
Constructivist grounded theory was used. This allowed us to identify categories pertinent to digital legacy and to develop a theoretical model to link their relationship. The approach also draws upon the researchers own experiences whilst constructing theories from the data, and is influenced by symbolic interactionism; a recognition that individuals can act in response to how they view their situations and use symbols in everyday life to make sense of their world. 19 Reporting of the study followed the Standards for Reporting Qualitative Research checklist. 20
To ensure research rigour we used four criteria to demonstrate trustworthiness 21 : (i) credibility was demonstrated through regular research team meetings and discussions with palliative care colleagues to discuss themes emerging from data; (ii) dependability was demonstrated through the use of constructivist grounded theory methods which provide a rigorous, transparent approach to data analysis; (iii) confirmability was demonstrated through participant validation and (iv) transferability was demonstrated by providing a good understanding of healthcare professionals’ experiences of managing digital legacy to enable others to compare and critique the findings. The lead researcher (SS), a hospice research nurse, was known to the participants, and consideration of how this might impact on data generation and interpretation was considered throughout. A reflexive stance was maintained by using field journals and writing memos, continually reflecting on the research process and holding regular meetings with the research team to discuss developing themes.
Study setting
The study took place in a hospice in the North-West of England, a specialised healthcare facility providing care for individuals in the advanced stages of a terminal illness or approaching the end of their lives. The hospice provides a variety of services including a 15 bedded inpatient unit, day services, outpatient clinics, community outreach, patient and family support and bereavement services.
Sampling and recruitment
Purposive sampling was used to ensure variation in experiences, such as profession and number of years’ experience working at the hospice. Theoretical sampling was used to explore emerging themes by both adding new interview questions and sampling for specific participant characteristics. Recruitment took place between February and March 2022. The study was introduced at the weekly hospice education meeting, giving potential participants the opportunity to ask questions and express interest in taking part. Study adverts were placed around the hospice, and an email was sent to all hospice staff outlining the inclusion and exclusion criteria for the study.
Data collection
Over a period of 2 months semi-structured interviews were carried out with palliative care healthcare professionals. Participants received written information prior to the interview and provided written consent. Interviews were held face to face in a meeting room at the hospice, or virtually via Microsoft Teams at the participants request. All interviews were audio recorded. Interviews lasted between 35 and 60 min, and participants were informed that they could pause or discontinue the interview at any time. Each interview began with a background to the study and a definition of both digital legacy and advance care planning. An interview guide was used to encourage continuity but was also used flexibly to allow participants to talk freely about their experiences (Appendix 1). Open questions were used, and the interview schedule was adapted throughout the course of data collection to reflect emergent themes and concepts (Table 1). Field notes and reflections were written throughout the interview process to help make sense of data during the analysis phase.
Examples of interview questions.
Data analysis
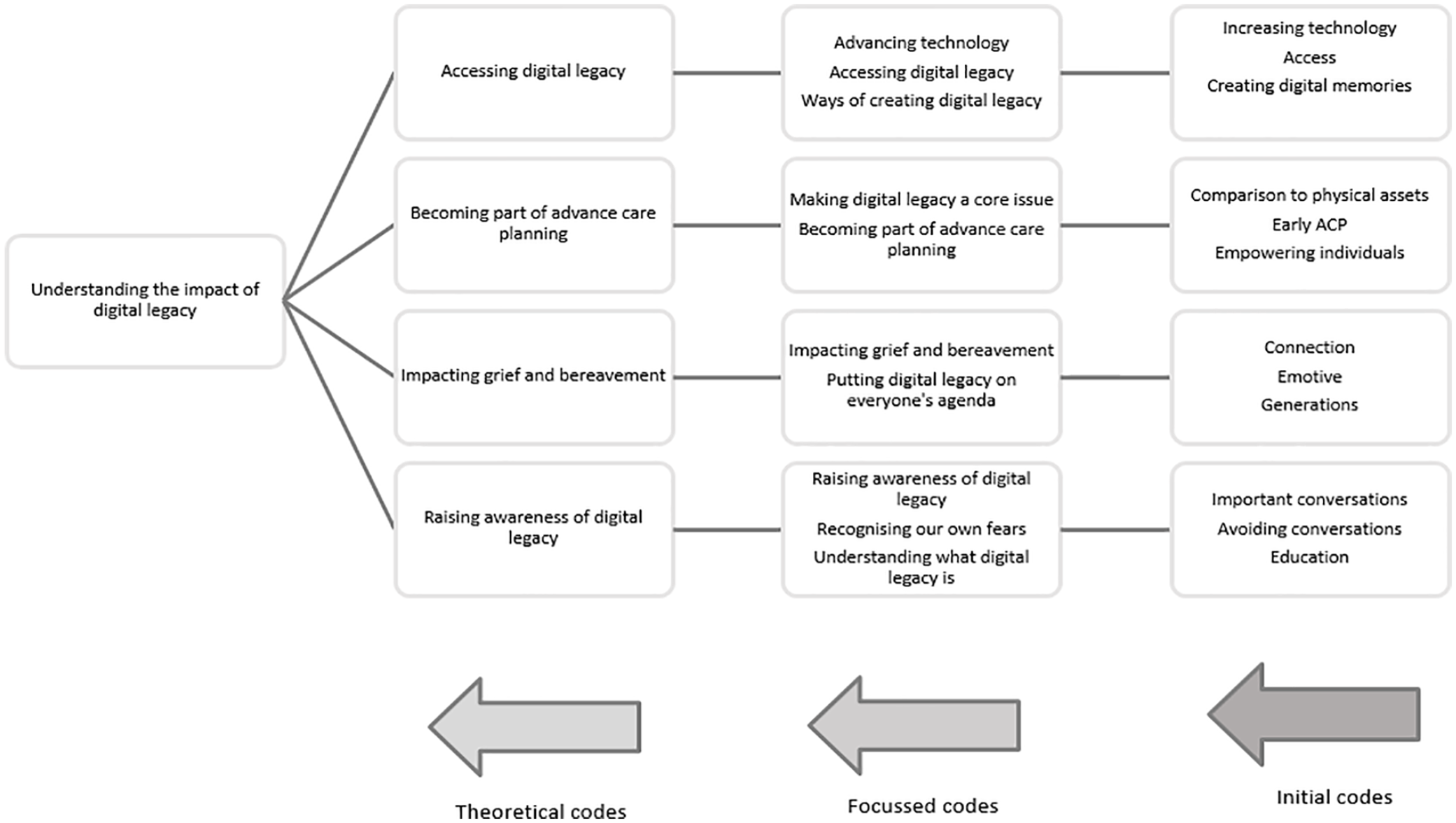
Recorded interviews were transcribed verbatim by SS. Consistent with constructivist grounded theory, data collection and analysis were iterative and ongoing, allowing emerging theories to inform subsequent interviews and sampling of participants. Transcripts were exported to Nvivo 1.4 22 for in-depth analysis. Inductive analysis was used with line-by-line coding of participants’ interviews allowing codes, categories and themes to be generated from the data (Appendix 2). Constant comparison was used throughout the data analysis process to understand the relationships between emerging codes and themes. 23 Coding was carried out by SS, and regular meetings with KH were conducted during data collection and analysis to discuss initial findings, evaluate data and challenge emerging ideas.
Participants were given the opportunity to discuss the developing themes. Two participants were involved in these discussions. A consensus was reached to cease data collection at 10 interviews as theoretical categories had become saturated, and new data was not providing insight or new properties to the categories. 19
Findings
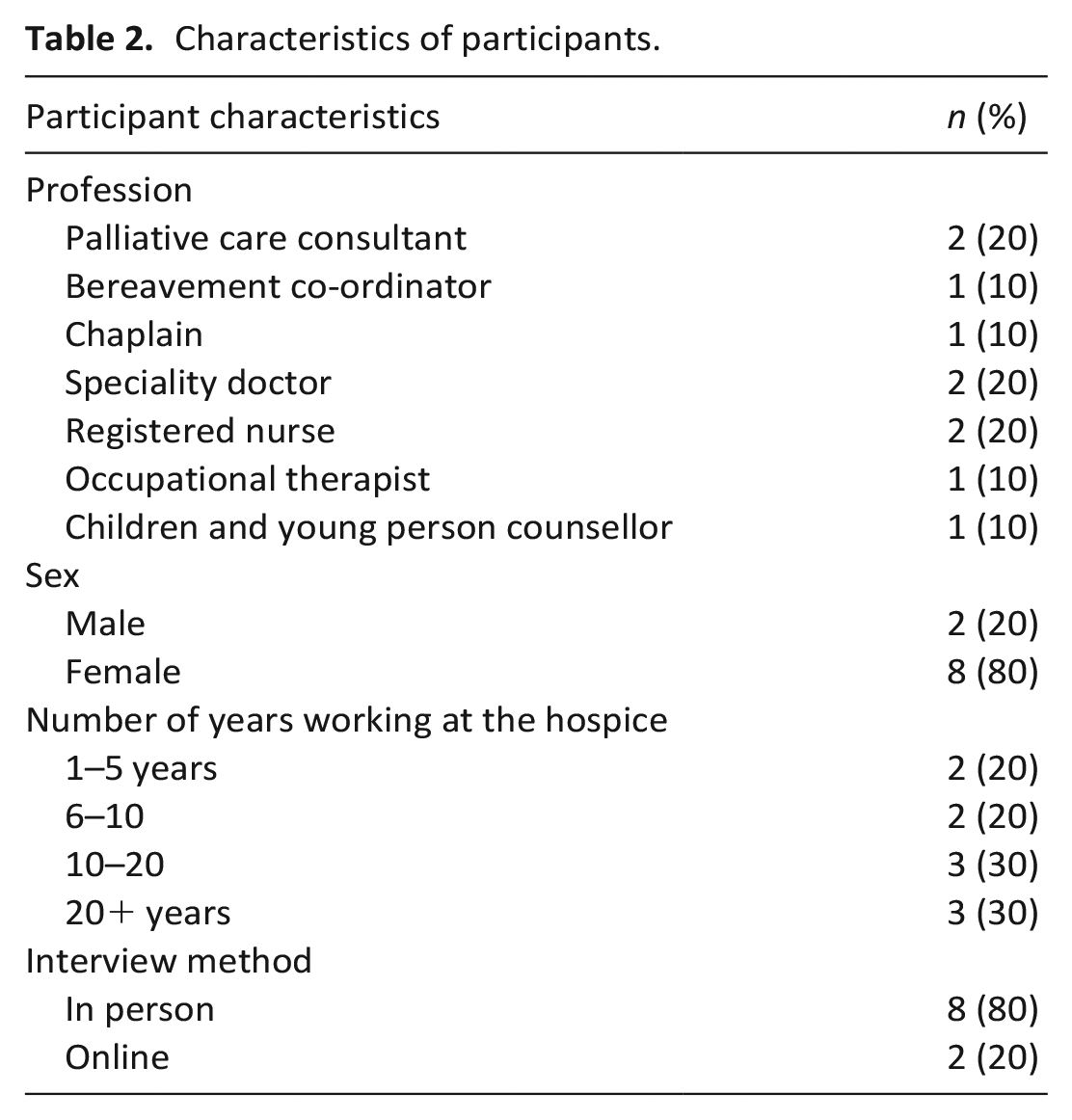
Ten (n = 10) healthcare professionals from across the multidisciplinary team were interviewed (Table 2). Those who chose not to take part reported issues around lack of time to participate in an interview.
Characteristics of participants.
Four theoretical categories were developed relating to the emergent theory: (i) accessing digital legacy, (ii) becoming part of advance care planning, (iii) impacting grief and bereavement and (iv) raising awareness of digital legacy. These themes revolved around the core category ‘understanding the impact of digital legacy’ (Figure 1), explaining how palliative care healthcare professionals described their experiences of digital legacy.
The emergence of the core category ‘understanding the impact of digital legacy’.
Accessing digital legacy
Participants spoke from both professional and personal experience to highlight issues around accessing digital legacy, which included the volume of information stored on devices, concerns around protecting data and the damaging effect of not being able to access digital belongings could have in bereavement.
Devices such as mobile phones, tablets and laptops were considered a ‘holding space’ for digital belongings. These were described as carrying an abundance of personal and sentimental information such as online banking accounts, email accounts, music libraries, social media accounts, photographs and videos.
I guess it depends how much information you store on these devices doesn’t it? And whether it’s like. . . if you talk about someone’s phone or something with their lifetime’s supply of messages to the friends and family. I mean that’s a wealth of information that’s quite personal isn’t it? (Mike, Specialty Doctor)
There was concern around the protection of data, particularly in relation to social media accounts. This stemmed from an awareness of privacy concerns, bad press surrounding social media, and a limited understanding of who has ownership of any content posted on social media sites. This lack of understanding led to questions around not only how to access such personal information, but also if there was a limited time in which accounts could be accessed before being de-activated.
With YouTube I’m not sure with the digital legacy side of it how far, how long somebody’s page can sort of stay on. Anne (Bereavement Co-Ordinator)
All participants believed that patients receiving palliative care should consider access to digital belongings as a vital aspect of managing digital legacy. This included consideration around passwords and biometric recognition to access devices. This was deemed important for managing both monetary and sentimental digital belongings.
And actually those things are really important aren’t they, because when someone does die then the practical aspects of financial things can be quite tricky to manage if you don’t have those passwords and access and all that. (Mike, Specialty Doctor)
Participants also recognised the importance of family members and friends being able to access sentimental assets such as photographs, videos and music which might be stored on a device such as a mobile phone, and the potentially damaging effect losing or being cut out of accessing these could have.
You like to look at photographs to remember people, we like to listen to songs. . . songs are really emotional, aren’t they? So I think there’d be lots of power in that. . . and getting cut out of it and not having access to it could be quite damaging, couldn’t it? (Mo, Registered Nurse).
Participants all agreed that they are not currently discussing access to digital legacy with patients receiving palliative care or their loved ones. Yet, they believed that it was the responsibility of healthcare professionals to initiate these conversations, as part advance care planning.
Becoming part of advance care planning
Participants felt that advance care planning was a ‘natural place’ for digital legacy conversations. Some acknowledged that there were some barriers to advance care planning conversations due to fear and a lack of confidence amongst some healthcare professionals. Digital legacy was perceived as potentially helpful in initiating these difficult conversations.
It could be helpful for staff as well because it could get them over that hurdle, and the lines of communication. . . It’s just opening that conversation in a gentle way, because you can talk about the fact that we all have things in our phone and. . . you know, so I suppose it is a gentle way into advance care planning, isn’t it? Maybe it might be good for staff. (Mo, Registered nurse)
Participants believed that initiating conversations around digital legacy could be empowering to patients. For instance deciding what happens to their digital belongings is something that patients might still be able to do, even if their physical ability had deteriorated.
But perhaps if they have got things. . . It does give them the opportunity to think ‘well what should I be doing about this now?’ So they. . . they have got autonomy to do what they want with that, with perhaps possibly without them involving other people. (Joyce, Consultant in palliative care)
Some participants suggested that nominating a person to manage digital legacies following death would be useful. It was considered important for patients to identify a relative or friend who would be capable of handling their digital belongings as part of advance care planning.
And I suppose if you nominate somebody to have some degree of responsibility for your digital legacy, then you are choosing that to be a particular person. So much like, I imagine, you would only make a power of attorney somebody who you would trust to make the right decisions for you. (Claire, Speciality doctor)
Many participants recognised that digital legacy conversations should be an individual choice, as they had experiences of caring for terminally ill patients who had no interest in technology and used it rarely meaning that they might not want to consider digital legacy as an essential part of advance care planning.
There’s two camps. So there’s the ones that are tech savvy and okay. And there are the ones like my mum and dad that have got a Nokia. And yeah, if you mentioned anything technical at all, they just look at you like ‘no!’ (Patricia, Registered nurse)
Good timing of digital legacy conversations was deemed is essential in order to allow time to plan given the volume of digital content that an individual may have, and equally to allow opportunities to create new digital memories when the patient was well enough to do so.
Especially if. . . I think it depends when it’s [the digital memory making] done. So if like, I capture somebody who is quite well even though they’re dying, and they can talk with a strong voice and they don’t get their words muddled and they are like they were. . . then I think that’s very different to if we try doing it with somebody who is very, very frail maybe a bit confused and gets very tired doing it. (Daisy, Chaplain)
Impacting grief and bereavement
Digital memories, such as videos and voice recordings, were described by participants as being more emotive than a physical photograph. Many healthcare professionals shared their own personal experiences, particularly relating to grief and bereavement.
Maintaining a connection following the death of a loved one was viewed as important, and digital memories could play a role in achieving this. Videos, photographs, social media accounts and music libraries could all be used for this purpose.
And when speaking about that when I’ve worked with these young people they see that (social media) as still a point of contact for the parent that’s died, ‘I’ve still got that part to be able to keep of Mum that’s not going away’. (Sadie, Children and young person counsellor)
Participants recognised that grief is a process that will affect individuals in a different way, and that each person will find different ways to cope. Some spoke about how feeling close to a person through digital memories following their death might help them to cope with the loss.
I suppose (if you can access their digital media) you would still feel like you’re close to that person. And if you can access their Spotify list and the music that they liked to listen to. . . or, and the photographs, and the posts and things that they. . . it’s what interests someone else. And I suppose it’s part of. . . not so much keeping them alive. . . But going through that process of letting go isn’t it? It’s, it’s something that would get you through I think because it’s something that you can go to, isn’t it? And it’ll get you through (Mo, Registered nurse).
Participants also recognised how maintaining a connection, through digital memories such as photographs and videos, could help a person to cope in grief.
You know, you’ve had this massive horrendous loss but. . . it brings so much more, you been able to hear, being able to see just mannerisms of being alive, you know, and so the digital is what brings that life in so much more, than a picture or a letter. . . although there is so much that you can get from that isn’t there. But actually physically on a screen seeing somebody and hearing them seeing them and those unseen, you know the way that they. . . I don’t know flick their hair or whatever it is. Erm so for her (my friend) it has been like a real comfort. And she has been trying to get anything where she can just see him and hear him because everything is. . . . She’s now clinging on to. . .just to, just help her through. (Laura, Occupational therapist)
Participants recognised an increase in grieving online, which was described as both a positive and negative experience. Some spoke of a generational divide, with a perception that younger people find more comfort in being able to express their grief through social media.
A few things did pop into mind with regard to the young people that I’m working with after the death of a parent and how, I don’t know, my experience of it - through Facebook and Instagram and how they hold the accounts for the parents. . So when it comes to Mother’s Day, birthday’s anniversaries, they post on there. . . So that has been put in place, which is really interesting because I think my experience of digital legacy is around preparing and somebody to be able to put that in place. (Sadie, Children and young person’s counsellor)
Raising awareness of digital legacy
Participants spoke about raising awareness of digital legacy through staff education and through awareness-raising at a societal level.
Many participants felt that it was not necessarily within their remit to advise on how to manage digital legacy, yet they believed they should initiate conversations with their patients.
I think we should be. . . . If it’s been raised as becoming much more common, much more popular. So, therefore, we, we need to be inclusive of people and just to, as I say, raise awareness really with the patients and the families that these could be things, they may want to think about and may want to talk about. (Joyce, Consultant in palliative care)
One participant recognised that it is often the responsibility of the healthcare professional to explore all aspects of care and that this is seen as an important part of clinical practice.
So you know, people don’t necessarily come and tell us about their religious needs or directly ask about nutrition and hydration. But we know that those are important things that we (healthcare professional’s) should talk about in the consultation. (Graham, Palliative care consultant)
By just opening up these conversations it was felt that patients would be given opportunities for managing digital legacy which could have a positive effect on both their own and their loved ones lives.
Yeah, I think it could be really beneficial, especially in the hospice environment. If you know, we were just raising that awareness over it and I think so many people would really appreciate that. . . and to just simply open that discussion with the patient and family and say, ‘you guys have a chat about it, I’ll go and make a cup of tea’, you know, it’s about those really lovely unique conversations that likely wouldn’t have happened. I think it could be a lovely sort of introduction to the way we work. (Anne, Bereavement Co-Ordinator)
Most participants admitted that they did not feel confident in knowing exactly what digital legacy was, but that speaking about it as part of the interview process had given them a greater insight. They felt it was important for healthcare professionals to feel comfortable in starting these conversations with patients and families, and that education could lead to digital legacy being discussed more frequently.
And so I do think, yeah, educate healthcare professionals around. . . and it’s not, it’s just about reassurance, they don’t have to know all the answers, but just feel comfortable sitting with somebody and exploring that with them could be all they need (Anne, Bereavement Co-Ordinator)
Many described the need for a change in societal attitudes and the importance of people considering their digital legacies before they are diagnosed with a terminal illness.
Yeah, maybe it’s an add-on thing that we need to look at nationally on a bigger scale. Because it is for all of us, it’s a reminder that we’re not here forever. . . we’re all gonna die, we don’t really know when. And it just serves us a reminder, doesn’t it? And there’s nothing wrong with that. I think it’s a helpful conversation, isn’t it? (Mo, Registered nurse).
Some participants spoke about the role children and young people might play in ‘normalising’ digital legacy conversations. This was mainly due to their confidence and awareness of using technology in their everyday lives.
I think I’d say for my generation there’s probably. . . we still have to think about these things a little bit more because we’re not, you know, it’s not second nature is it to. . . but I think the kids. . . Oh, I sound old, kids these days. . . but it’s part and parcel of life, isn’t it? (Mike, Specialty doctor)
Digital legacy was considered a ‘current’ issue which might be appealing to younger generations, it was considered to be a topic which could be discussed with young people in schools as an introduction to discussions around death and dying.
Definitely and, you know, even going into schools and talking about that. . . could it be a project? Could it be an open discussion around young people to say ‘what are your thoughts on digital legacies?’ If somebody, you know, died unexpectedly or even if you have months to plan, would it be something that you would want to be put in place for your future self? (Sadie, Children and young person counsellor).
Discussion
Our findings demonstrate that for digital legacy conversations to take place between healthcare professionals and patients there was a need to raise awareness around digital legacy within palliative care. By raising this awareness through education, digital legacy conversations could become a part of advance care planning leading healthcare professionals to discuss issues around access of digital belongings and suggest ways to create digital memories (Figure 2).
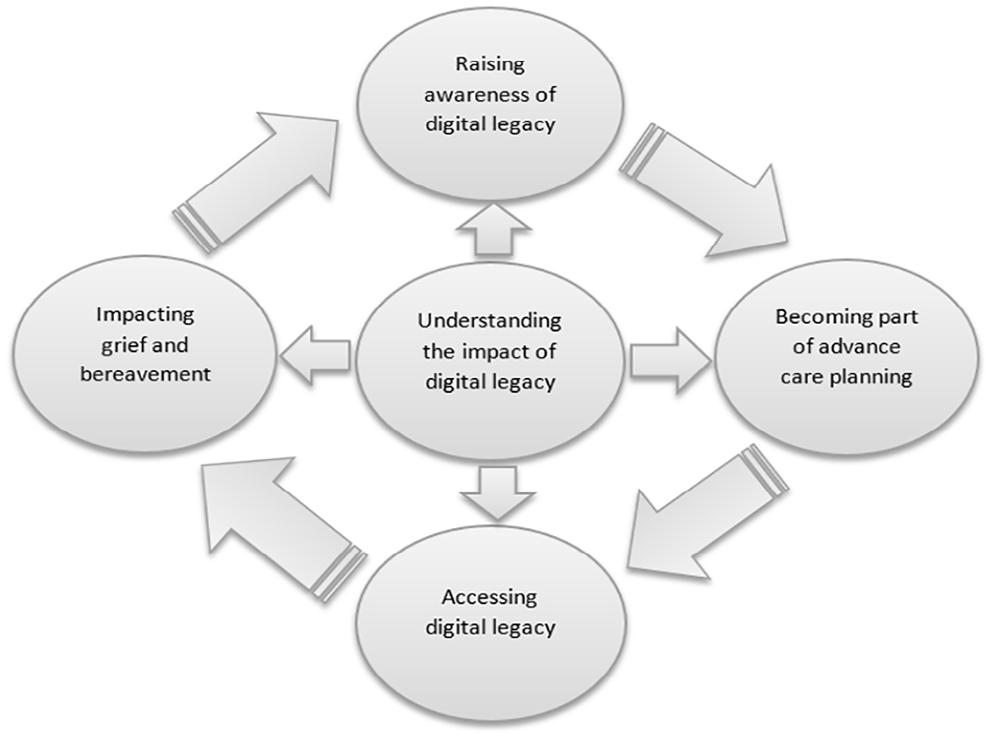
Understanding the impact of digital legacy.
Most patients will possess a broad and varied range of digital belongings by the end of their life. This is new for many healthcare professionals, and a recent survey study of hospice staff showed that the vast majority have never discussed digital legacy with their patients. 24 In the present study, as interviews progressed many participants realised that their own devices held a lot of important information, particularly sentimental data such as photographs and videos. Some participants spoke of the need to arrange this data and consider how their loved ones would access it as they wouldn’t want it to be lost following their own death. This is consistent with previous research which revealed that losing access to digital memories presented bereaved relatives with a ‘fear of digital death or a second loss’.
There was concern from participants about their lack of knowledge surrounding what happens to social media accounts following death. With this came a concern that they were also unaware of how long accounts such as social media, email and music streaming would remain active following a persons’ death. Social media accounts can play a significant role in helping the deceased person’s community express their grief, thus ensuring access to such accounts is considered and managed in a timely fashion is essential.
Our findings suggest that discussing digital legacy as part of advance care planning conversations is important. Research shows that when patients have the opportunity to make their wishes known, this helps them feel in control, allowing bereaved caregivers to feel comforted in the knowledge that their loved ones wishes would be respected. 25 Digital legacy was considered to be a gentle introduction to ACP conversations, with some participants suggesting that reaching goals set for digital belongings could be more achievable than some current considerations of patient’s wishes. For example, although preferred place of death is often discussed with patients it is something that cannot always be achieved. 26
Our findings also suggest that digital legacy will not be a priority for all patients, and given the importance of tailoring advance care planning to an individual’s needs, 27 digital legacy may form a significant or minor part of advance care planning discussions depending on the individual.
Digital legacy can play an important role in bereavement, supporting the bereaved person to maintain a connection with the deceased and their community. Participants in the present study believed that digital memories (e.g. videos and social media accounts) could help to maintain a connection with a person following their death. This is aligned with continuing bonds theory, and supports the position that relationships do change after death but do not end, and that continuing the bond with a deceased person can be normal, adaptive and comforting.
Our findings suggest that it is important to raise awareness and knowledge of digital legacy amongst healthcare professionals, as well as a need for change in societal attitudes towards digital legacy. A recent report published by Marie Curie ‘Public Attitudes Towards Death and Dying in the UK’ 28 emphasises the increasing importance of raising awareness of issues related to end of life care, and engaging in these important conversations. As our findings suggest, digital legacy has a growing significance in palliative care both now and into the future.
Limitations
Recruitment to this study was limited to participants from one hospice in the North West of England and therefore the findings may not be generalisable to other healthcare settings. The aim of the study was to develop a theory which could relate to similar settings and therefore it is important to consider how the theory ‘understanding the impact of digital legacy’ might provide the basis for future research in palliative care. It is important to recognise that the participants in the study were familiar with the researcher, which may have influenced the responses they gave. To mitigate this a position of reflexivity was adopted to allow a more pragmatic view of the study and address any potential bias. Field journals and memo’s provided a way of continually reflecting on the research process in order to remain grounded in the data.
Implications for policy and practice and research
Further research is required to examine the views and experiences of patients and carers in relation to digital legacy. Further research is also needed to understand the impacts and challenges of digital legacy in bereavement. Research is required to explore which healthcare professionals should conduct digital legacy conversations, and to understand the limitations associated with this in clinical practice. Furthermore, it is essential that further work is undertaken in specialities outside of palliative care to understand how other areas of healthcare are considering digital legacy. We outline considerations for clinical practice and healthcare policy (Table 3).
Recommendations for clinical practice and healthcare policy.
Conclusion
This study shows the importance of understanding the impact of digital legacy. Considering digital legacy should routinely form part of the advance care planning process and may help to initiate advance care planning conversations. Digital legacy may have value in raising awareness of palliative care amongst younger audiences. Further work needs to be undertaken to explore the impact of digital legacy in all areas of palliative care. Knowledge around digital legacy is limited and it is essential to raise the profile of digital legacy both within healthcare and the wider society for digital assets to be managed effectively.
Footnotes
Appendices
Acknowledgements
We would like to thank the participants for their valued input and participation in this study. We would also like to thank the hospice management and research governance group for supporting recruitment to the study.
Author contributions
SS and KH designed this study. SS collected the data. SS and KH analysed the data. SS drafted the manuscript with the support of KH, AN and AF. All authors provided critical feedback to the manuscript, read and approved the final draft.
Data management and sharing
In order to anonymise data, participants were allocated a unique number during data analysis, and a pseudonym for report writing. Transcripts were typed in word documents and saved on a password protected laptop. Any data held on paper (e.g. consent forms) were stored in a locked cabinet, in a locked office at the research site.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
SS, AF and AN’s roles are funded by Marie Curie. Funding for SS to undertake the Master of Research Health and Wellbeing, which this project was a part of, was obtained through Marie Curie. The open access fees were covered by Marie Curie.
Ethics and consent
This study received ethical approval from Liverpool John Moores University Research Ethics Panel (NAHPGT (MRES) 2100) and was approved by the hospice research governance group. All participants provided written informed consent. This study was not registered in a trials register.