
Abstract
Background:
People with diagnoses of intellectual disability or serious mental illness have higher mortality rates due to physical comorbidities; better understanding is needed to guide best practice in provision of palliative care for these populations.
Aims:
To identify multivoiced perspectives, drawn from lived experience of: what works, and what does not, in palliative care for people with intellectual disability or serious mental illness; challenges in, and opportunities to improve, palliative care.
Design:
A systematically constructed qualitative meta-ethnography. Protocol published (PROSPERO: CRD42021236616).
Data sources:
MEDLINE, PsychINFO, CINAHL PLUS and Embase used without date limitations. Papers published in English, containing qualitative data on palliative care provision for people with a diagnosis of intellectual disability or serious mental illness were included. Global five-point strength score applied for relevance/quality appraisal.
Results:
Familiarity (of location, people and/or things) is important for good palliative care. Assumptions and misunderstandings about the role of mental capacity assessment to appropriately involve the patient in decision-making are common. Adapting training for palliative care staff to address concerns and beliefs about mental illness is one of the methods that helps avoid diagnostic overshadowing. Proactive identification of service arrangements to meet needs of persons with personality, psychotic, delusional and bipolar affective disorders will help optimise care.
Conclusions:
Evidence, including the voices of people with intellectual disability or serious mental illness is urgently needed to guide efforts to improve their access to and experience of palliative care. More evidence is especially needed to understand, develop and implement best practice for people with psychosis, bipolar affective disorder, mania and personality disorder.
Individuals with intellectual disability or serious mental illness have high rates of mortality due to physical comorbidities.
These populations have specific needs that should be met to provide optimum palliative care and maintain optimum mental healthcare at the end-of-life.
While research exists describing the problems these populations face, little is known about how to improve care for them.
By focusing on lived experiences of patients/service users, carers and healthcare professionals this paper synthesises existing evidence into multivoiced perspectives on what works, does not work, plus challenges and opportunities for improvement.
Assumptions and misunderstandings about the role of mental capacity assessment to appropriately involve the patient in decision-making are common, while adapting training for palliative care staff to address concerns and beliefs about mental illness helps to avoid diagnostic overshadowing.
Professionals need help to work across divides between physical and mental healthcare services, so people can receive palliative care in familiar locations and/or from familiar people.
A significant research deficit exists regarding provision of optimal palliative care to people with psychosis, personality disorders, bipolar affective disorder and depression.
Assessing capacity may be optimally achieved by involving professionals across specialities and organisations.
Proactive identification of service arrangements for care needs of persons with serious mental illness will help optimise care.
Introduction
Serious mental illness typically incorporates psychosis including schizophrenia, delusional disorders bipolar affective disorder, depression and severe personality disorders. 1 These populations have a higher risk of physical comorbidity, with mortality rates due to physical illnesses being two to three times higher than the general population. 2 Reasons are multifactorial and include late presentation, delayed diagnosis, insufficient treatment, pharmacological interactions of antipsychotic medication and associated unhealthy lifestyles (including poor diet, high smoking rates, excessive alcohol consumption and lack of exercise). 3 People with intellectual disability share this high mortality rate.4,5
Inequities in palliative care provision are likely to be accentuated for people with psychiatric diagnoses. 6 In the United Kingdom, the NHS mandate promotes parity of esteem between mental and physical healthcare, with similar legislature existing in other countries. 7 Despite this, patients with serious mental illnesses are often excluded from palliative care research8,9 and an inability of services to make ‘reasonable adjustments’ for those with intellectual disabilities has resulted in poorer outcomes. 10
There is limited evidence to guide rectification efforts for these disparities. This study sought to synthesise available first person perspectives on these issues and identify the current state of the evidence (e.g. gaps and uncertainties).
Methods
Aim
This qualitative meta-ethnography seeks to identify multivoiced perspectives, drawn from lived experiences of what currently happens and what should be happening for such patients by asking:
What can we learn from synthesis of existing first-person perspectives about care of adults living with an intellectual disability, psychosis, bipolar affective disorder or personality disorder who also require palliative care for a physical illness?
We sought to establish what is perceived to work/not work, what are the challenges and opportunities for improved care and where more research is needed.
Study design and conceptual orientation
This is a systematically constructed review using meta-ethnographic methods to synthesise findings. 11 We utilised the PRISMA model for systematically constructing reviews and the eMERGe standards for meta-ethnography. 12 A protocol was registered with PROSPERO (Record ID 236616). 13
We systematically constructed literature searches to comprehensively search existing evidence for first person experiences and perceptions – bringing together patient/service user, carer and healthcare professional voices. Given many study designs were likely to provide useful first-person perspectives we used the Joanna Briggs systematic search framework of population (by diagnostic group of intellectual disability or serious mental illness), concept (palliative care) and context (care settings). 14 This avoids undue focus on studies of interventions or only those with comparators (initial scoping searches demonstrated that such studies were rare).
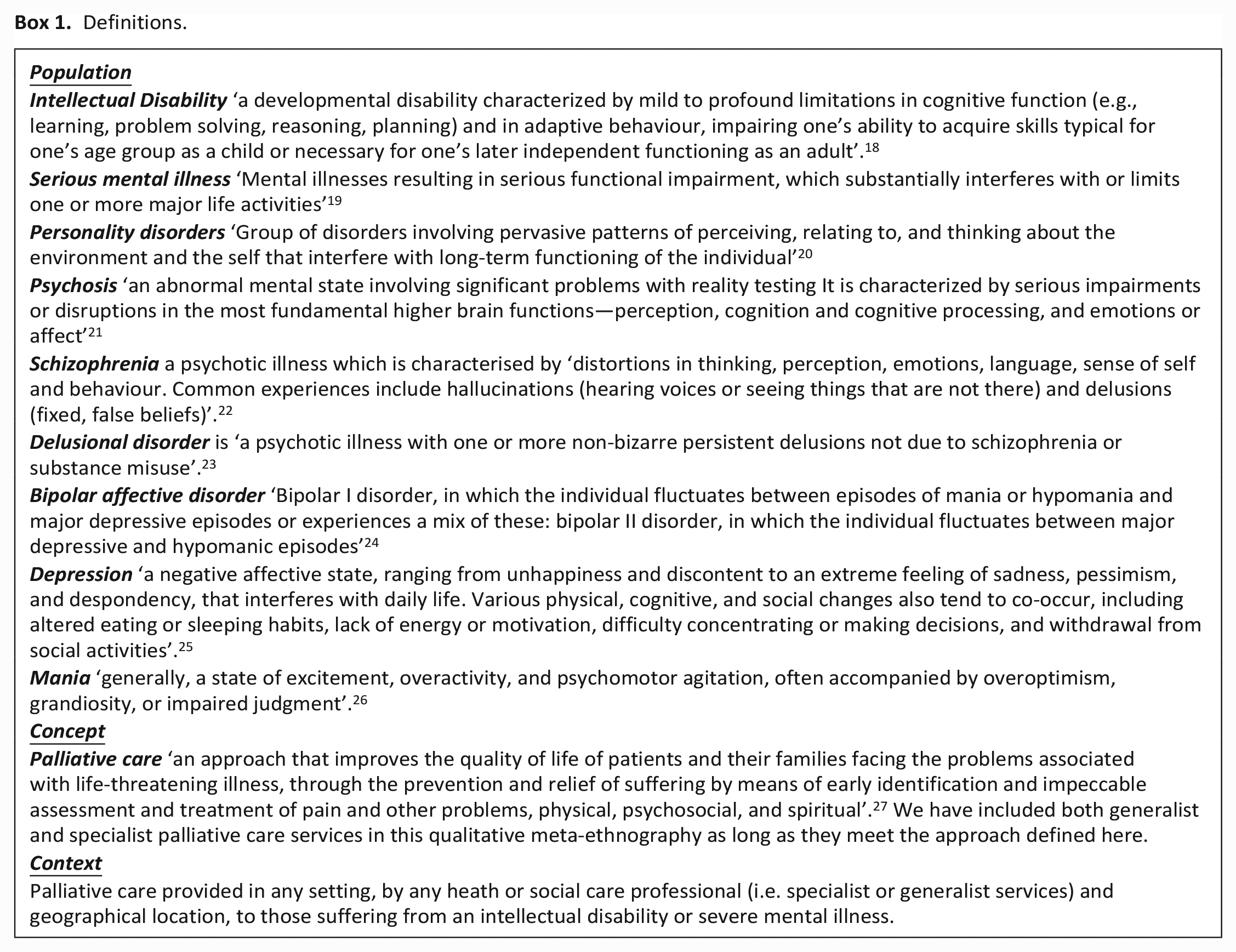
Box 1 defines our search parameters within the population, concept and context framework. Serious mental illness definitions vary within literature, operationally and clinically.15,16 All definitions include psychotic illnesses. We chose not to include substance use/drug induced psychosis or eating disorders as these populations have distinct clinical and contextual features compared with included disorders.
Definitions.
Meta-ethnography is a synthesis method for analysing and interpreting qualitative studies to answer focused questions and develop new insights. 17 We sought to understand what could be learned from first person narratives in existing literature (i.e. the experiences of people giving or receiving palliative care when provided through first order data, i.e. direct quotations), but also to identify relevant second order data (commentary, whether descriptive or interpretative from the authors of work included in the review) so we could establish where specific gaps in understanding the perspectives and experiences of people lie.
We conducted our synthesis using steps described by Noblit and Hare 11 : (i) develop a question (as above), (ii) search and select studies (conducted systematically using the ‘PCC’ format of population, concept and context, (iii) read studies (to identify first/second order data and consider content of each), (iv) determine how studies are related (looking for themes, with attention paid to consensus/diversity), (v) translate studies into each other (tabulating), (vi) synthesise translations (through team discussion) and (vii) express the synthesis (as discussed in this paper).
Search strategy and study selection
The search strategy is summarised in the Supplemental Files: Figure 1 (PRISMA flowchart) and Table 1 (Search strategy). As serious mental illness is not a recognised specific search term in medical literature databases, we searched using specific diagnoses with relevant ICD-10 codes (see Box 1 and Supplemental Table 1). We sought but did not identify any proven search threads for serious mental illness in established review databases such as Cochrane.
MEDLINE, PsychINFO, Embase and CINAHL plus were searched without date limits. The initial search was conducted in February 2021 (following which alerts were set to identify articles published while conducting our analysis, with formal updates in January and October 2022 plus a final update completed 19th February 2023. Two independent reviewers screened records at each stage (title, abstract, full text). Differences were resolved by discussion with a third reviewer. References of all included papers and all reviews of original research were examined to capture further studies.
Inclusion criteria
(1) Qualitative or mixed method studies (if qualitative data extracts were included in the source publication) meeting aforementioned definitions. Case study and review papers were included as second order data if these otherwise met the inclusion criteria. Review papers were included as second order data if meeting new content in the review met our inclusion criteria.
(2) Participants aged 18 or older.
(3) Any setting where healthcare is provided: including home, care homes, hospitals, specialist institutions for serious mental illness, intellectual disability or palliative care.
Exclusion criteria
(1) Less than 18 years of age.
(2) Diagnosed with other or no mental illnesses.
(3) No qualitative data or first-person narrative included.
(4) No English language version available.
(5) Poor quality (see below).
Quality appraisal
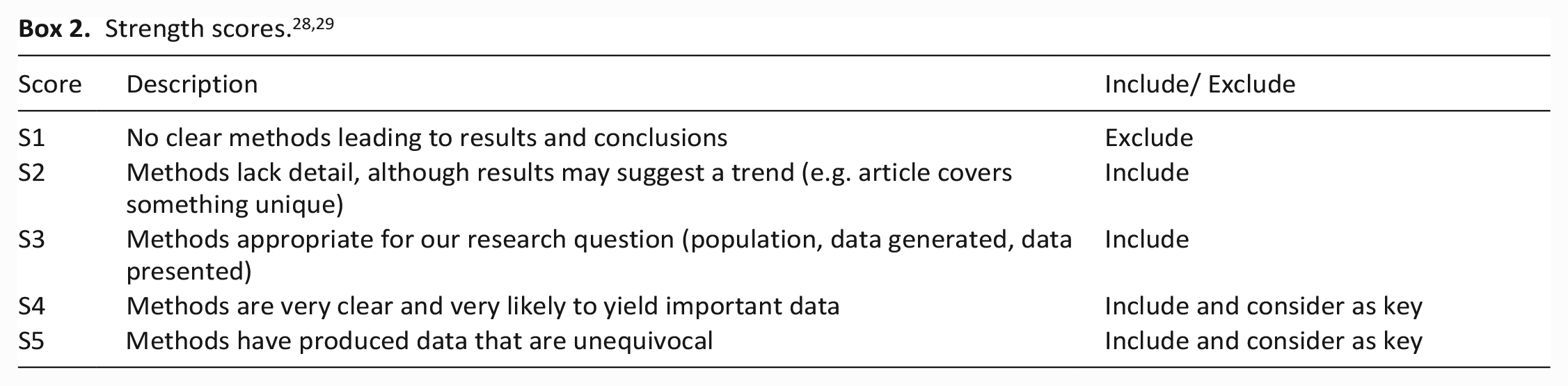
We did not automatically exclude papers on the basis of quality. Drawing on precedent in health professionals’ education research, quality of papers was assessed using a five-point strength score (Box 2) by two independent reviewers. This was appropriate to our goal of understanding the current ‘state of evidence’.28,29 Strength scores were allocated according to the reporting of the methodology and results; study type did not automatically influence the score. When scores differed, the lower score was chosen. No scores had a difference of more than one. Papers scoring S1 were excluded as these were not of a quality to meaningfully incorporate into our synthesis.
Data analysis
Following the process of meta-ethnography described by Noblit and Hare, 11 first and second order data were extracted and thematically analysed using our research question as a framework (see Supplemental Files Table 3: Data mapping to research questions and identification of themes). As a team we developed and refined our analysis; extracting, coding, identifying themes, discussing ideas and concepts relevant to our review questions and systematically comparing across studies. Primary outcomes were: challenges faced while providing palliative care to this population; and opportunities for improvement. Secondary outcomes (any other aspects of care experiences) were also noted.
Results
Table 2 (Supplemental Files) details included studies. Fifty-eight papers met our eligibility criteria. Of these, 38 discussed palliative care for persons with intellectual disability, nine for persons with serious mental illness (not further defined), five discussed depression, and six for persons with psychosis. No papers specifically examined the diagnoses of bipolar affective disorder or personality disorder although these diagnoses may have been included in papers which did not define serious mental illness.
Most studies were conducted in Europe, especially the UK (n = 18), Holland (n = 12) and Ireland (n = 6). Seven papers were from the U.S.A and nine from Australia. None were conducted in Asia or Africa.
Regarding quality, most studies were graded S3 or S4 (n = 44). Twelve were S2 and none S5. Two papers were determined to be S1 and so excluded from the analysis.30,31
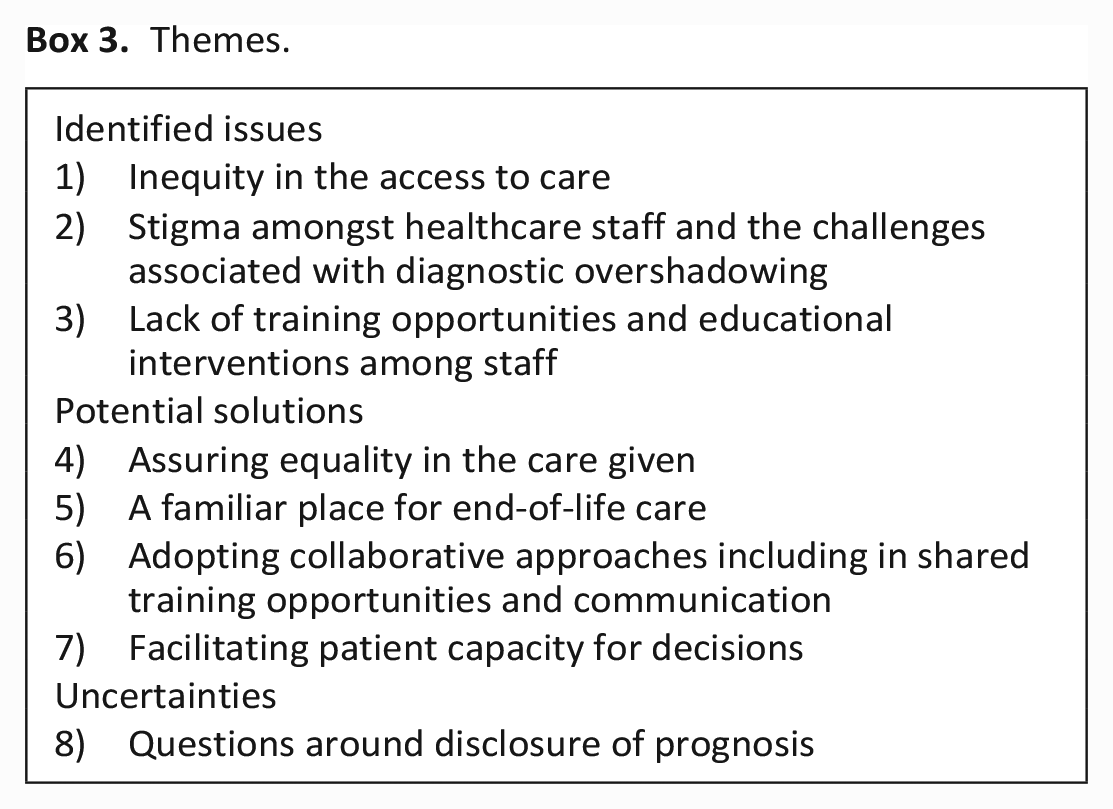
Supplemental Table 3 maps the data to our research questions, namely: what works and what doesn’t; what are the challenges, and opportunities for improvement in care. When possible, we present themes (see Box 3) with identification of how these applied by diagnostic group. We summarise in our discussion the areas where either an absence of evidence or conflicting evidence prevents even tentative conclusions about best practice and/or how to improve care being drawn.
In the nine papers where a more specific diagnosis for study participants beyond ‘serious mental illness’ was not described we found similar results to the studies that did provide greater diagnostic detail.
Themes.
Identified issues
Inequity in the access of care
There are many challenges to reducing inequities of access of care as summarised by Woods et al:
When these people seek help from health care providers, they may not present in a typical way and a history may be difficult to elicit. Comorbid medical conditions may also be complex. Symptoms of medical and mental health illnesses may not be recognized, leading to undertreatment. As a result, people with SPMI may not have access to cure-oriented treatment in a timely manner, and “palliative care may become the treatment from the time of detection and diagnosis.”. [Second order data
32
]
Across the included studies, collaboration was identified to be of paramount importance for improving access to care, as emphasised by Donald and Stajduhar:
Many authors recommended joint endeavours between palliative care and mental health, whether that was collaborating in treatment teams or providing cross-training and sharing resources [Second order data
33
]
Stigma amongst healthcare workers and the challenges associated with diagnostic overshadowing
Diagnostic overshadowing is ‘the process by which a person with a mental illness receives inadequate or delayed care due to the misattribution of their physical symptoms to their mental illness’.
34
Some studies showed that even psychiatric staff sometimes felt stigma or fear towards patients with schizophrenia; and this continues to be replicated in palliative care as well as in other areas of physical healthcare:
They’re really scared. . .when it comes to someone who has mental illness, ‘specially schizophrenia, they’re really, kinda. . .they don’t want to handle them. I think they’re afraid [First order data
35
]
In the single study we found that included people with bipolar disorder the issue of stigma was particularly evident to nurses:
Almost all of the nurses in both groups discussed the effect of stigma on the delivery of care to this patient population [Second order data
35
]
A specialist palliative care nurse highlighted how patients with depression are also stigmatised
. . .you know when we talk about depression, there is certain stigma. . . I feel depression has a stigma myself. . . [First order data 36 ]
Professionals offering care were conscious of the wider societal issues related to this:
I think depression largely in our society is something that people see as a mark of weakness and a stigma, and often people will defend against admitting depression.’ [First order data
37
]
Other studies also showed that mental illness-related stigma in the healthcare system is a major barrier to treatment, resulting in poorer care quality 38 and impacts help seeking behaviours, leading to decreased access to required care. 39
Diagnostic overshadowing was identified as being one of the key challenges to provision of optimal palliative care. Lack of insight was put forward as a potential reasoning behind this.
A consistent picture of delayed or late diagnosis and diagnostic overshadowing appears in case studies. Complex and enduring mental health problems may contribute to these issues. . . Denial, or a lack of insight, is a possible complicating factor. It is not unknown for persons diagnosed with other serious conditions to deny the gravity of their situation, and for people with pre-existing mental health conditions it appears that this is no different. [ Second order data 40 ].
Lack of training opportunities and educational interventions among staff
We recognise that staff training and education alone will not work. Professionals also need to be supported to apply their learning in a system orientated to facilitating better care. However, existing literature mainly focuses on the lack of training generalist staff.
Distinguishing psychiatric symptoms from physical symptoms was highlighted in many studies as a potential mechanism for reducing the risk of diagnostic overshadowing:
Lack of training in palliative care or mental healthcare, particularly for those outside of mental health or palliative specialties, is a recurrent issue in the literature that inhibits access to palliative care for those with SPMIs [Second order data
33
]
Evenblij et al demonstrate how this can also impact on patients in specialist practice with this quotation from palliative care nurses:
. . .We hadn’t picked up on the signs coming from this lady. . .or not enough. But that was very much to do with the fact that we considered the complaints of pain from a psychiatric point of view rather than as genuine complaints about pain. [First order data
41
]
Home managers providing care for people with intellectual disability were identified as engaging in similar reasoning:
When he was going downhill, people maybe saw it as manipulation. [First order data
42
]
. . .leading to inequalities in care provision:
This problem of diagnostic overshadowing, where symptoms are understood by health care professionals as part of the learning disability rather than part of the person’s illness, was also highlighted in the account [Second order data
43
]
While it is well recognised that diagnostic overshadowing can lead to physical illnesses being attributed to pre-existing mental diagnoses, we also found evidence suggesting a risk of what might be termed reverse overshadowing. For example, in papers considering clinical depression, a lack of training for palliative care staff was identified as a hindrance to diagnosis, and therefore treatment:
. . .we get so much in service teaching and study days on assessing pain, new drugs for pain, etc., but very little on how to assess for depression. . . [First order data
36
]
It can be difficult to separate some depressive symptoms from physical health symptoms due to their illness and hence, an alternate symptom criterion is often required in this population:
The somatic symptoms fatigue and loss of weight or appetite were prominent but often indistinguishable from manifestations of the progressing cancer. Despair, anxiety, and social withdrawal emerged as alternative symptom criteria. . . “, the findings point to a need for a broader understanding of “recurrent thoughts of death or suicidal ideation” in patients with incurable cancer [ Second order data
44
]
Diagnosis of depression by palliative care clinicians can feel like a subjective assessment:
It’s a tricky thing. It’s somewhat person-dependent, in terms of the clinician. I guess, because it doesn’t have a physical or you can’t do a test actually looking for biological abnormalities, to some extent, it remains a, you know, gray area, I suppose. [First order data
37
]
Causal explanations also vary amongst different palliative medicine professionals:
I think it’s part of a biopsychosocial response. . .with people who have got cancer, it’s because of illness. Others see it as a major challenge to their personal integrity as a person, and there is a lot of stress, physically, psychologically, emotionally, spiritually on the body, and I guess depression comes about as an abnormal delay in response to everything that’s happened. [First order data
45
]
Palliative care professionals also report greater uncertainty around help-seeking to support diagnosis and treatment when mental illness is considered than with alternative concerns such as complex pain:
We need more help from the psychiatrists. . .we think nothing of getting an anaesthetist to see the patients, but ponder for so long over a psychiatrist and when they come . . . they really do help and teach us as well [First order data
36
]
This suggests a difference in attitude and/or confidence towards diagnosing and treating mental illness, a point reinforced by other studies where additional issues regarding the ability of palliative care staff to access psychiatric care on behalf of their patients were also seen:
. . .we would do better if I think we knew that particularly for a group of patients who we felt that we were struggling with, that we could actually ask for some more help, so if we could actually have a psychiatrist, for example, who could go out and do a home visit on some of these patients and look at some better strategies, or even to say to us, yeah. . .I do agree with you, I think this person is depressed, or no, I don’t. That second opinion is really quite powerful. [First order data
46
].
In both cases training was seen as the best way to improve care whether in the context of depression or intellectual disability as shown above or in the context of psychotic illnesses including schizophrenia. Evidence was identified demonstrating awareness of lack of training for palliative care staff:
“. . .. very little to none of the staff had training in schizophrenia” [Second order data
47
]
in managing the symptoms, experiences and behaviours associated with psychosis, so that in turn patients could benefit from appropriate palliative care. Equally mental healthcare staff and patient relatives alike could not always recognise that the patient’s physical health was declining leading to delays in receiving care:
Additionally, family, informal carers and even staff in psychiatric group homes or nursing homes may not recognise the declining health of the person [Second order data
48
]
Even if a decline was identified there were additional risks for patients on medication for psychosis as the potential side effects and pharmacological interactions of psychotropic medications could be confused with other causes of symptoms at the end-of-life:
Many patients with chronic schizophrenia take Clozapine, a pharmacologically complex drug which, when combined with other treatments and medications, can lead to unwanted and possibly dangerous side-effects. It was reported that staff unfamiliar with patients with schizophrenia experiencing physical decline at the end-of-life may not recognise the signs indicating the patient is in distress. [Second order data
48
]
The need for training was also identified in the one study that included data from people with bipolar affective disorder:
I don’t know so much about my bipolar patients. A lot of times . . . I feel like those people you can’t take care of by yourself.. . .. It’s probably their splitting and their personality as far as you know. . . what they say they want, but what they actually do . . . or, um, their unpredictability. [First order data
35
]
Lack of training, or superficial training on palliative care was also identified by staff working in intellectual disability services as a hindrance to good practice:
I remember, you know, when I was training it was – I can even see the section in the book – it was like, maybe two pages. . .. [First order data
49
]
They found it hard to identify the need for palliative care as a result:
The extent in which ID-physicians are able to identify a need for palliative care also depends on experience and knowledge [Second order data
41
]
Potential solutions
Equality in the care given
While our findings above regarding access to care, stigma, diagnostic overshadowing, reverse overshadowing and potential for training strongly point to inequalities in the care received, it was only in the diagnostic categories of intellectual disability and depression that studies focused specifically on equality were found.
A participant working in a specialist palliative care service, highlighted the importance of providing equitable care to people with intellectual disability:
I think . . . it is about equity – in that this is a population who is very vulnerable – and it is about . . . the valuing of human beings and it’s about humanity [First order data
50
]
And others working with this group questioned why this was not always done:
Would a person from the general community be treated the same way? I suspect not, and it gets very hard. [First order data
51
]
Staff working in intellectual disability services described discrimination faced when trying to access medical services resulting in feeling unsupported when delivering care:
We’ve had doctors that have refused service. They said they don’t have time to take on someone with complex medical issues, meaning an intellectual disability. [First order data
51
]
The term “isolation” was chosen as best reflecting the frustration staff expressed in being aware of the existence of support services, but then being unable to access them consistently or when needed. [Second order data
51
]
Specific recommendations to address equity issues included the use of hospital passports 52 specialist intellectual disability liaison nurses, 53 provision of longer appointments 54 and liaison with patients to understand their priorities. 55
In the context of depression there was some evidence that palliative care staff were aware they did not always give equal importance to mental health symptoms:
we just do not ask about it often enough . . . and when we do, we do not let patients know how common it is ¡/ they often think they are the only ones and that they are not coping. . .You know failing in some way. . . [First order data
36
]
Furthermore, it was recognised that people with depression were at risk of getting less attention to their symptoms overall:
People who are depressed are possibly more generally withdrawn and I guess for that reason, possibly, it may be overlooked. [First order data
37
]
A familiar place for end-of-life care
There currently exists no standard on the most appropriate location for providing end-of-life care for persons with a diagnosis of a serious mental illness. Wilson et al looked at the data that evidenced where this care took place and where an individual is most likely to spend their last days. It was found that individuals are more likely to die in care homes, however, no patterns existed when looking at data about other locations:
We found studies that reported associations between serious mental illness and increased likelihood of dying in hospital, decreased likelihood, and no association between serious mental illness and hospital deaths [Second order data
56
]
Care home deaths were more common in patients with serious mental illness, for all causes. One potential explanation for this is, for many people with serious mental illness a care home or similar institutional care setting is their usual place of care, and may be more likely to be their place of death, than the general population, who may be more likely to reside at home until their death or nearer to the end-of-life [Second order data
56
]
For people with intellectual disability the evidence suggests significant benefit from ensuring the patient is within a familiar environment at the end-of-life. Staff working in intellectual disability services recognise this need:
They recognised that there were limited choices offered to this patient group and acknowledged unsatisfactory outcomes when a patient was placed in an unfamiliar environment [Second order data
57
]
Equally staff working in care homes for people with intellectual disabilities were keen to avoid hospitalisation when someone was dying from known irreversible causes:
When death was expected, hospital deaths were seen as being inappropriate and something to be resisted. [Second order data
58
]
One of the reasons given by this staff group for hospital avoidance was the need for one-to-one care:
. . .. They need to have one to one when they’re really poorly. So, I don’t feel hospitals are the place for them. [First order data
59
]
Psychiatrists also identified that flexibility and willingness to consider a change of setting to achieve the best care during a person’s dying phase might ensure their needs were met more fully:
For example, someone in the final stages of life may live and die most comfortably in a hospice setting but have been best served in a mental health setting only days prior. [Second order data
60
]
This was a nuanced issue, however, and nurses considering this question also discussed the importance of the preferences of the person, and those close to them:
. . .they also took into consideration the nature of the illness in view of preference and also the view of patients’ relatives and friends. [Second order data
61
]
While all studies emphasised the importance of a comfortable environment and many considered familiarity to be key there was no consensus as to which environment was most suitable. Choice was considered by some professionals to override technico-clinical markers of quality care:
“Unanimously, participants expressed a commitment to providing end-of-life care at the place of client’s choice” [Second order data
62
]
There was little evidence on this issue for people in other diagnostic categories but two studies of schizophrenia did consider the question of where care should be provided. For this group finding an appropriate location for end-of-life care was considered challenging by palliative care professionals meaning not all the usual options were necessarily open to them:
We’re seeing some dying in hospital because no-one else knows where to put them. A hospice might see schizophrenia and think “hmm a bit hard to manage in the hospice environment [First order data
48
]
It remains unclear where a patient with psychosis can be provided with the best end-of-life care, particularly given difficulties in accessing psychiatric support in some palliative care settings:
Being able to anticipate the patient’s pain and properly and aggressively treat it is crucial for effective end-of-life care. If a patient needs to be hospitalized, a psychiatric/medical unit would be ideal in which both illnesses of the patient can be effectively addressed [Second order data
63
]
Adopting collaborative approaches including in shared training opportunities and communication
Collaboration was viewed by palliative care staff as key to meeting needs in a holistic way, as demonstrated when caring for someone with severe depression:
I think you can’t address emotional things in isolation. . .it goes without saying that we rigorously address the obtrusive physical symptoms, and are obliged then to follow up their emotional pain and their spiritual pain. . .I think holistic care means that we look at the whole person. . .to see if we can relieve their distress in other parts of who they are, and that may mean then that we need to address a depressed state. [ First order data
46
]
While the strongest evidence around collaborative approaches was from people with intellectual disabilities and those offering care to them, there was also some evidence of perceived benefits in practice from adopting a multidisciplinary approach to care for people with psychosis, including schizophrenia. For this later group positive experiences of joint working were reported by palliative care staff: . . .they actually had their dedicated mental health worker as part of that team, so they work collaboratively with the community palliative care service, and their kind of health worker, maybe their GP and family, so again you’ve got this really nice partnership model. [First order data
48
]
Ideally this came as a continuation of joint working earlier in the disease trajectory:
Early psychiatric consultation and communication with the patient’s outpatient mental health team are key strategies to optimize cancer outcomes and enable oncologists to focus on the delivery of quality cancer care [ Second order data
64
]
For people with an intellectual disability, it was possible to consider what collaboration could offer, and what was lacking when it was not present. To ensure collaboration:
Openness to cooperation and sharing’ the care was an important value [Second order data
65
]
This applied between professionals, different healthcare services, staff and relatives:
. . .good working relationships with relatives and paid care staff were the most important contributing factor to ensure an effective process of decision-making. [Second order data
66
]
Palliative care nurses described the importance of everyone’s voice being heard:
Well, yes, we had a good working relationship with the doctor in this period, where we were able to say anything we wanted: what we thought, our feelings about it. And the doctor definitely listened to what we said. . .. [First order data
67
]
When collaboration was lacking, the same level of care could not be provided and learning was potentially lost:
Individual houses and units within the intellectual disability organizations did not appear to share their experiences of palliative care provision with each other, and as a result, there was little organizational-wide learning gained from isolated interactions [Second order data
68
]
The potential for shared training between palliative care and intellectual disability teams was identified in the arena of communication where different tools and approaches were needed:
. . .. Professionals need to provide open invitations for patients with an ID to talk about death using clear and simple language and visual stimuli, such as booklets [Second order data
69
]
and greater attention to non-verbal communication could make a difference:
‘Non-verbal aspects include facial expressions, touch, gestures, interpersonal spacing and posture‘. [Second order data
70
]
Symptoms were just tolerated or expressed atypically as irritability, inactivity, loss of appetite or sleep problems. [Second order data 71 ]
Assessing pain was complicated in those with an intellectual disability:
. . .. are they in pain. . .are they distressed. . .you know it is very difficult to tell [First order data
72
]
Assessing pain and indicators of quality of life is a difficult task for professionals, as described by intellectual disability physicians:
To what extent are they suffering? That’s often very difficult to say, especially if someone can’t communicate [First order data
73
]
Atypical communication methods may hamper palliative care staff, while staff working in intellectual disability services, alongside patient’s relatives, had a better understanding of communication styles. An occupational therapist describes how to understand non-verbal signs:
Communication is a big thing, particularly with residents who are non-verbal and like (name), he started doing things like playing with my clothes or wanting a hug. . .I knew straight away something wasn’t quite right [First order data
74
]
Sometimes specialist palliative care professionals relied on family members to understand the patient’s care needs:
The need to involve family or carers in gaining an understanding of the patient’s emotions or symptoms, in some cases relying on them heavily. It could be difficult to know how to communicate and how much the person understood. [Second order data
75
]
Relying on carers and relatives might help bridge the communication barrier, however, there was a risk staff might become excessively dependent on them:
. . .. However, palliative care staff were commonly over-reliant on carers to meet communication needs. [Second order data
76
]
Literature surrounding communication and assessing symptoms is freely available, but currently there is little empirical evidence of improved clinical outcomes as a result.77,78
Providing support and educating relatives and carers is an important factor, as demonstrated by the patient relative quoted below:
. . . when he first got the diagnosis and we went to that training course [on Dementia and Learning Disability] . . . it just prepared us so much and let us understand what he was going through and why [First order data
79
]
Facilitating patient capacity for decisions
One study provided evidence that people living with psychotic illnesses were concerned about whether they would be allowed to make choices and decisions about end-of-life care:
For each patient to be able to choose his own way of death, with dignity. I want people to let me do my thing, to let me do it my own way, without complaining. I want to decide when my time has come. That they let me spend the rest of my time like I want it with the people I choose. You have to let people make their own decisions, especially when it concerns the end-of-life. [First order data
80
]
However, they are often left out of this process as they are assumed to not have the capacity to participate in decision-making:
Individuals with schizophrenia were reportedly interested in discussions regarding end-of-life care and have the ability to communicate their preferences. However, more often health-care providers associate a diagnosis of schizophrenia with the incapacity to make decisions as a result of their incompetence and emotional fragility, consequently disregarding the need to incorporate patients in end-of-life care conversations [Second order data
81
]
All other evidence around facilitating capacity for decision making came from studies of intellectual disability. In these studies, it is concerning to note that professionals may not be confident, or familiar with established guidance around capacity and consent:
. . ... in practice, staff did not appear to have an agreed-upon way of assessing this, and different team members could have quite different opinions about a person’s level of insight. [Second order data
76
]
While others were concerned that people with learning disability would have little experience of exposure to death and dying and so attempts to involve them in their own care when facing this might cause harm:
I didn’t know that she had the intellectual capacity to take it on and that it could cause more harm. . .. People with longstanding intellectual disability. . .[have] been protected from having discussions about death and dying. . .. all their lives [First order data
82
]
Both of these issues are likely to be factors in a further concern: professionals themselves were not ready and willing to discuss end-of-life issues and felt that someone ‘in authority’ needed to make the decision to tell patients they were dying, although it was unclear who this might be:
Professionals were not prepared to discuss end-of-life issues with the patient because they believed the patient would not understand and they did not know who had the authority to tell the patient directly. [Second order data
83
]
One study did identify it was possible to adapt advance care planning processes to individual needs:
Additionally, professionals found it important to adapt the ACP process to suit the level of understanding and experiences of the person with intellectual disabilities. [ Second order data
84
]
The failure to assess capacity, and if it was established to be absent for particular decisions to follow best practice in decision making for incapacitous patients was problematic not just because of the failure to respect the patient as an individual but also because it was hard for others to trust in decisions. An example of this is illustrated in the concerns raised by emergency medical service providers:
I guess the question for me is always: these are people that don’t necessarily have the capacity to understand what choices are or make their own choices. So, is it the staff that are making the decisions about it? Is it the family? Does it really represent what the person would want? [First order data
85
]
Uncertainties
Questions around disclosure of prognosis
More detailed evidence related to specifically discussing prognosis was only found in relation to intellectual disability, where staff tended to avoid discussions of death and dying in general:
Getting older . . .. I don’t know what I should say to her about that. That she is getting older and she will eventually die? I think that would only make her anxious. [First order data
86
]
He wasn’t really able to. . .he understood he was dying. . . but he wasn’t able to process it or understand it on that level of his wishes. . . [First order data
87
]
while also recognising that failure to normalise death as part of life could have unintended consequences when, for example, in residential care settings people experienced peer bereavements:
Intellectual disability staff commented that service users who experienced the death of a peer often had incomplete understandings of illness and death [Second order data
88
]
In addition, carers, including relatives were sometimes vehemently against disclosure. A father of a client with a moderate intellectual disability described:
If [my son] was to ask us what’s going to happen to me, I think I’d lie. I’d lie for his own good. . . [First order data
89,90
]
Death was a topic we never raised with A. We talked about it indirectly, when others . . . But not with A himself. . .. . .W: He would totally panic. He couldn’t deal with that. [First order data
91
]
Common reasons given to support such nondisclosure include the belief that the patient would not understand, prevention of emotional suffering and distress. These views were not universally held. Some staff in intellectual disability services did feel a duty to inform the patient:
. . .they all have different capabilities, but I think they all have a right to know, and I think it would be quite awful to keep something like that from someone. . . [First order data
62
]
And in this view, they were more aligned to the views of palliative care professionals:
I think each case must be looked at on an individual basis with the needs of the patient and their level of understanding and comprehension kept central to the decision-making process [First order data
90
]
Unlike other themes there was some evidence directly from people with mild to moderate intellectual disability in this area from seven studies, all of which pointed to a desire to understand prognosis and make choices based on this information:
People like us should know what is happening to us because . . . we have choices to make like. . .where to die, how to die, how to be buried. Yah. . .the person who is dying should know everything and people should let them make choices [First order data
92
]
A key concern for primary participants was that they were able to make their own choices and be in control of the decisions being made. [Second order data
93
]
‘The discussions about wishes also seemed to express a deep desire that the person with ID should be in control’. [Second order data
94
]
Open communication, though difficult, was seen as a means to allow individuals to have a better understanding and a feeling of familiarity with their illness. It can often lead to productive conversations as evidenced below:
Communication was not only about sharing information but was also a means to help the person feel familiar with his illness. [Second order data
95
]
Although, communication about the end-of-life can be difficult and takes more effort, time and experience, nurses stated that fruitful conversations about end-of-life issues are possible. [Second order data
96
]
Discussion
This qualitative meta-ethnography provides novel insights for advancing care for people with a physical life limiting illness who have a diagnosis of intellectual disability or serious mental illness. Despite undisputed evidence that these individuals have high rates of mortality due to physical comorbidities, little research has been conducted to understand the experiences of, or to improve palliative care for, these populations. In contrast, there has been considerable research exploring improvement in cancer care, 97 diabetes, 98 cardiovascular health 99 and obstetric outcomes 100 in those with serious mental illness.
All of these populations have specific needs that should be met to provide optimum palliative care and maintain adequate mental healthcare at the end-of-life. Professionals need help to work across divides between physical and mental healthcare services, so people can receive palliative care in familiar locations and/or from people they already know. Assumptions and misunderstandings about the role of mental capacity assessment to appropriately involve the patient in decision-making are common. Adapting training for palliative care staff to address concerns and beliefs about mental illness helps to avoid diagnostic overshadowing and ‘reverse’ overshadowing. People with serious mental illness are at risk of having symptoms overlooked due not only to the misattribution of physical symptoms to mental illness but also because symptoms such as those experienced in severe depression are not given equal priority.
For people with intellectual disability there is a consistent body of evidence to support the provision of palliative care in a familiar environment. This might be a familiar location or another environment that has been made familiar, for example, by inclusion of people and things that are familiar and important to the person being cared for. There is also strong evidence of the importance of creating good collaboration between different specialities; and between relatives and staff, by cooperatively working together to allow for a free flow of information and experience and sharing the responsibility of patient care and decision making. Unsurprisingly, given these findings, the evidence also points strongly to the need to increase intellectual disability and palliative care staff training and knowledge on the topics of: effective communication, adapting processes to suit the individual, and pain assessment. Increase knowledge of carers and relatives on the disease and how they can support loved ones, and the support available. Several sources of evidence also support the need to ensure equitable care by making reasonable adjustments at organisational level, and at individual level by involving the person with intellectual disability in discussions surrounding access to care.
The specific challenges experienced in giving and receiving palliative care when people also have serious mental illness, other than were specified in the themes above, were all under-researched. Without better understanding the problems experienced it will not be possible to design meaningful improvements. We suspect it is likely that many of the underlying issues and factors surrounding care identified for people with intellectual disability, such as stigma, lack of inclusion in healthcare discussions and decisions, and professional uncertainty about capacity assessments are likely to also play a part in the other diagnostic groups we considered in this review. Equally it is likely that it may be advantageous to involve professionals across organisations and service boundaries in order to create suitable care and working may also help reduce variation in how capacity assessments are conducted or the mental health act is applied. Some limited evidence including people with psychosis supports this. Proactive identification of service arrangements for care needs for persons with personality, psychotic, delusional and bipolar affective disorders is needed to achieve this and optimise care.
Strengths and limitations
In common with any systematically conducted review our findings are dependent on the identification of existing evidence. By focusing on lived experiences of patients/service users, carers and healthcare professionals this paper syntheses existing evidence, where it exists, into multivoiced perspectives on what works, does not work, plus challenges and opportunities for improvement.
We synthesised first-person evidence from a wide range of participants, however, there was not enough first order data from people in the diagnostic groups we included, to draw meaningful comparisons between groups other than noting there are promising signs of a growing body of evidence to support best practice in palliative care for people with intellectual disability. Even here, first person perspectives are currently lacking. In the other diagnostic groups included in this review the most notable finding is the overall paucity of qualitative research in general and a total lack of patient voices in particular. There is an urgent need to better understand the perspectives of people with psychosis, personality disorders, bipolar affective disorder, and unipolar depression if we are to design and develop palliative care services that can meet their needs, let alone provide good care that is orientated to individual priorities, preferences and choices at the end-of-life.
Heterogeneity of the term serious mental illness and the absence of standardised database search terms for many forms of serious mental illness may have limited our work. We included all study designs and also checked case reports and commentaries/editorials for first person perspectives based on lived experience. It remains, of course, possible that there are other sources of evidence which might be found with further resources. The absence of included papers from Asian or African countries suggests, that there is a lack of evidence internationally and/or cultural and socioeconomic differences may play a role in the way these diagnoses are viewed.
Implications
Our findings have significant implications for both policy-makers and clinicians as well as researchers. The World Health Organisation recognises the need for early, effective and geographically inclusive palliative care, 101 however it is particularly challenging to deliver this to patients with serious mental illness or intellectual disability without a supporting evidence base. In the United Kingdom, policymakers have attempted to enlist commissioners, alongside frontline clinicians, in improving the access to palliative care for those with a serious mental illness. 102 Uptake of these recommendations is generally poor 103 and what clinical teams can practically do to address such issues is often limited. Services are typically delineated between ‘mental’ and ‘physical’ health; an approach which is unhelpful in delivering integrated patient-focused care 104 and emphasises an unrealistic expectation of how people with physical comorbidities present with mental health problems or vice versa (i.e. if serious mental illness precedes significant physical illness). It is important to recognise training and education alone will not work. Our findings strongly suggest an urgent need to support developing better systems to support staff in applying learning. These systems need to provide suitable care environments where professionals are facilitated in multidisciplinary working, and greater collaboration between professionals, patients and their friends/families.
Based on the findings of this work specific areas for further research include:
When caring for people with intellectual disability how can staff best be supported to appropriately judge capacity and consent so patient can be involved in the decision-making process and when capacity is questioned how can decisions made on the patient’s behalf be made without denying the patient a voice in their care?
More research is needed on all aspects of providing palliative care for people with serious mental illnesses including how to address system issues in order to provide the best available place for end-of-life care and redesign services to facilitate integrated care across organisational and service boundaries. Questions about how to practically consider capacity, discuss prognosis and attend to potential medication interactions all also need further research for these groups in order to both support professionals in practice and design effective training to alleviate fear and stigmas as well as improve technico-clinical interventions.
Conclusions
Evidence, including the voices of people with intellectual disability or serious mental illness is urgently needed to guide efforts to improve their access to and experience of palliative care. Addressing the challenge of access to care requires whole system change to facilitate and support healthcare professionals to work across organisational and service boundaries. Without this it will be difficult to generate impact at scale from opportunities for training to mitigate diagnostic overshadowing. Improving practical knowledge of how to appropriately manage questions of capacity and reduce assumptions about capabilities and preferences for information and involvement in care is also essential, and likely to be improved through shared working and experience rather than education alone.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231175928 – Supplemental material for Challenges and opportunities for improvement when people with an intellectual disability or serious mental illness also need palliative care: A qualitative meta-ethnography
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231175928 for Challenges and opportunities for improvement when people with an intellectual disability or serious mental illness also need palliative care: A qualitative meta-ethnography by Nivedita Ashok, Daniel Hughes and Sarah Yardley in Palliative Medicine
Footnotes
Authorship
We confirm that all authors have made a substantial contribution to study design, analysis, and interpretation of data. NA drafted the first version of this article under the supervision of DH & SY as part of a Masters dissertation academic programme. All have critically revised this version for important intellectual content and approved it for publication. All authors take joint responsibility for the article content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent
Not applicable to systemically-constructed reviews of published literature.
Data sharing
Data used in this systematically-constructed review is available through the publishers of each item. Publisher restrictions may apply.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.