
Abstract
Background:
Across the developed West, a significant proportion of older people die in hospital It has been argued that an acute hospital setting is not well equipped to support dying well. A palliative approach, which involves recognising and alleviating suffering, might lead to improved quality of care. Yet suffering is an intangible and contested phenomenon and little is known about people’s actual experiences of suffering in this clinical setting.
Aim:
To examine the context of end-of-life care for older people in an acute hospital setting, particularly focusing on the experience of suffering.
Design:
An observational study, using an ethnographic approach. Data analysis was inductive and iterative. Reflexive analysis included observations and inferences from a participant-observer perspective. Over a period of 3 months in 2016, 186 h of observations of clinical care were carried out.
Settings/participants:
The study was carried out on a 30-bedded acute older peoples’ hospital ward in the United Kingdom. Participants included 11 patients and 33 members of staff and visitors.
Results:
Patient suffering was influenced by a range of factors. Delays in recognising and acknowledging dying often led to treatments that were burdensome or futile, exacerbating patient suffering. This was frequently associated with clinical decision-making that did not take into consideration long term concerns such as prognosis or quality of life. Environmental factors in the physical clinical setting such as noise and smell also exacerbated suffering. Finally, aspects of interpersonal interactions, such as paternalistic attitudes or ineffective communication, affected patient experience.
Conclusion:
Acute care for older people in hospital was shaped by an overarching ideology of rescue which predicted and dictated the process of care. Suffering was not restricted to the direct experiences of life-limiting illness but was also associated with the experience of receiving care in an acute hospital setting. Avoiding or minimising iatrogenic suffering is an essential component of compassionate care.
Failing to identify the end of life can inhibit the provision of compassionate palliative care
Suffering often goes un-noticed, particularly in older people with cognitive impairment
The suffering experiences of older patients in hospital are compounded by the influence of the clinical care setting
There are obstacles to timely identification of dying that directly impact on patient suffering
There is a need for staff to recognise the impact of the environment and context of care on patient suffering, and respond appropriately
Suffering needs to be viewed as a broader aspect of patient experience, not solely linked to experiences of terminal illness
Background
Hospital remains a common place of death in those over 65 years in technologically developed countries, with a high proportion of these people having cognitive impairment, as well as complex co-morbidities. 1 The quality of end-of-life care in hospital is variable and has been the subject of a number of recent reports and investigations.2,3
Improving end-of-life care in hospitals is a global priority, and a key priority for research in the UK. 4 Suggestions to enhance the care quality cite the development of a ‘culture of safety, compassion and learning that is based on cooperation and openness’ 5 and recommend developing insight into the link between culture and compassionate care. Reports highlighting a compassion deficit, however, may only address part of the issue, as poor care may also result from failing to see suffering 6 rather than from a lack of compassion per se.
A central principle of palliative care is to respond to, minimise or alleviate suffering. 7 Suffering is a complex human experience with no agreed definition8–10 yet it is broadly agreed that it constitutes a core concern for people living with life-limiting illness. 11 Older peoples’ suffering at the end of life is frequently ignored, particularly in those with cognitive impairment.12–14 This has been brought into sharper focus since this study was conducted, as families have been unable to visit and spend time with dying loved ones in hospitals and care homes due to the covid-19 pandemic.
Previous research suggests that failing to emotionally engage with hospital patients can lead to a disproportionate emphasis on physical needs, such as pain.15,16 Furthermore, literature often defines suffering in the context of symptom burden from disease and less is known about suffering associated with experiences of healthcare itself. Existing evidence is largely built upon interviews with relatives or professionals 17 or retrospective case note study 18 rather than through direct observation. Observational research offers a window into the experiences of those who are facing the end of life. If more is known about suffering, then changes that enable compassionate care can be optimised.
Methods
Research aim
Our aim was to address the lack of knowledge about suffering of older people in hospital care at the end of life by providing a detailed ethnographic description that could inform improvements in care. Specific objectives were to:
Explore the experiences of patients at the end of life
Identify and describe factors that influenced these experiences
Describe the cultural, environmental and clinical context of care
Posit connections between the context of care and the suffering of patients
Design
The study was underpinned by a constructivist epistemological position. Sensory ethnography enables proximity to the subjective experiences of those at end of life.The design was informed by the principles of sensory ethnography, 19 with observations attending not only to what was seen and said but also to what was perceived by other senses, such as smell and hearing. This yields rich descriptions of the physical and sociocultural environment to provide the reader with a rich reconstruction of the context of care.
Setting
The study was carried out on a 32-bedded acute ward providing care for older people in a medium-sized urban hospital in the North of England.
Population
Inclusion criteria for patients were that they were thought by staff to be in the last weeks of life. They were identified through discussions with the clinical team. There were no exclusion criteria. In keeping with the ethnographic method, the field observation included all people within the ward, irrespective of role. However, the specific focus for the study was those identified as being in the last weeks of life. However, patients were not observed if they had an acutely unstable clinical condition. All ward staff, visiting staff and visitors were potential participants, although as the specific focus of the study was the activity surrounding those patients approaching the end of life, many visitors and staff were not observed as they did not have direct interaction with these patients.
Sampling
As the focus for this study was on those patients in the last weeks of life, the key informants were those patients and the staff and visitors who interacted with them. Other members of staff were observed where it was decided that this would add to insight into the culture of the ward.
Recruitment
Information sheets were provided by LG to potential patients and written Informed consent was obtained from patient and visitor participants after 24 h. Where a patient did not have mental capacity to consent, consultees were approached to discuss and agree their participation. 20 Staff were informed about the study via meetings, talks, posters and information sheets and were included unless they opted out using a brief form. Ongoing consent was established at each contact.
Data collection
LG adopted a participant-observer role, supporting staff with fundamental care of patients. Periods of observation ranged from 4 h to a full shift, and included early, late and night shifts. To build a deep understanding around suffering of patients at end of life, a focus was selected at the start of each period of observation based on the discussion at nursing ‘handover’, for example, a decision that needed to be made about nasogastric feeding, or issues that were emerging from the ongoing observations which required further exploration; for example, when a staff nurse mentioned that a doctor was seeking to ‘rescue’ a patient, the idea of clinical decision-making became an intentional object of study. Contemporaneous field notes were taken, describing observations of care on the ward in real time and further reflexive notes were made off site afterwards. Informal interviews with participants, documents, patient notes and characteristics of the physical environment relevant to the focus were used as additional data sources. All identifiable characteristics were altered in this report, and patient names anonymised.
All data were collected by LG between May and August 2016.
Ethics
Ethical approval was given by Leeds West Research Ethics Committee (REC Ref: 14/YH/0166 IRAS ID: 149772 Jan 2015). Concerns included issues of consent and capacity, and potential for harm through impact of observation on dignity. Further details on how these were addressed can be found in the thesis. 21
Data analysis
Field notes were kept in shorthand, then typed up. Data were analysed using an iterative, inductive approach during the field work, to inform lines of enquiry for subsequent observations. EverNote™ was used to manage the data, as themes developed. Braun and Clarke’s 22 method of thematic analysis guided the process Excerpts were tagged with codes and aggregated into overarching or subordinate themes. Re-reading of field notes allowed patterns to be identified and connections posited to draw inferences between patient experiences and the context of care.
A reflexive approach was adopted in keeping with the participant-observer role. As the first author was an experienced palliative care nurse this was an important means of identifying any preconceptions. Two approaches to identifying bias were taken. In the first, a series of workshops was held with seven ‘experts-by-experience’ from a service user research group within the University. In the workshops, anonymised extracts from field notes were used as prompts for discussion. Workshops were audio recorded and the discussions reviewed to identify additional interpretations and perspectives on the primary data. Secondly, samples of data were discussed with doctoral supervisors (JO, AC) to inform coding and emerging themes.
Findings
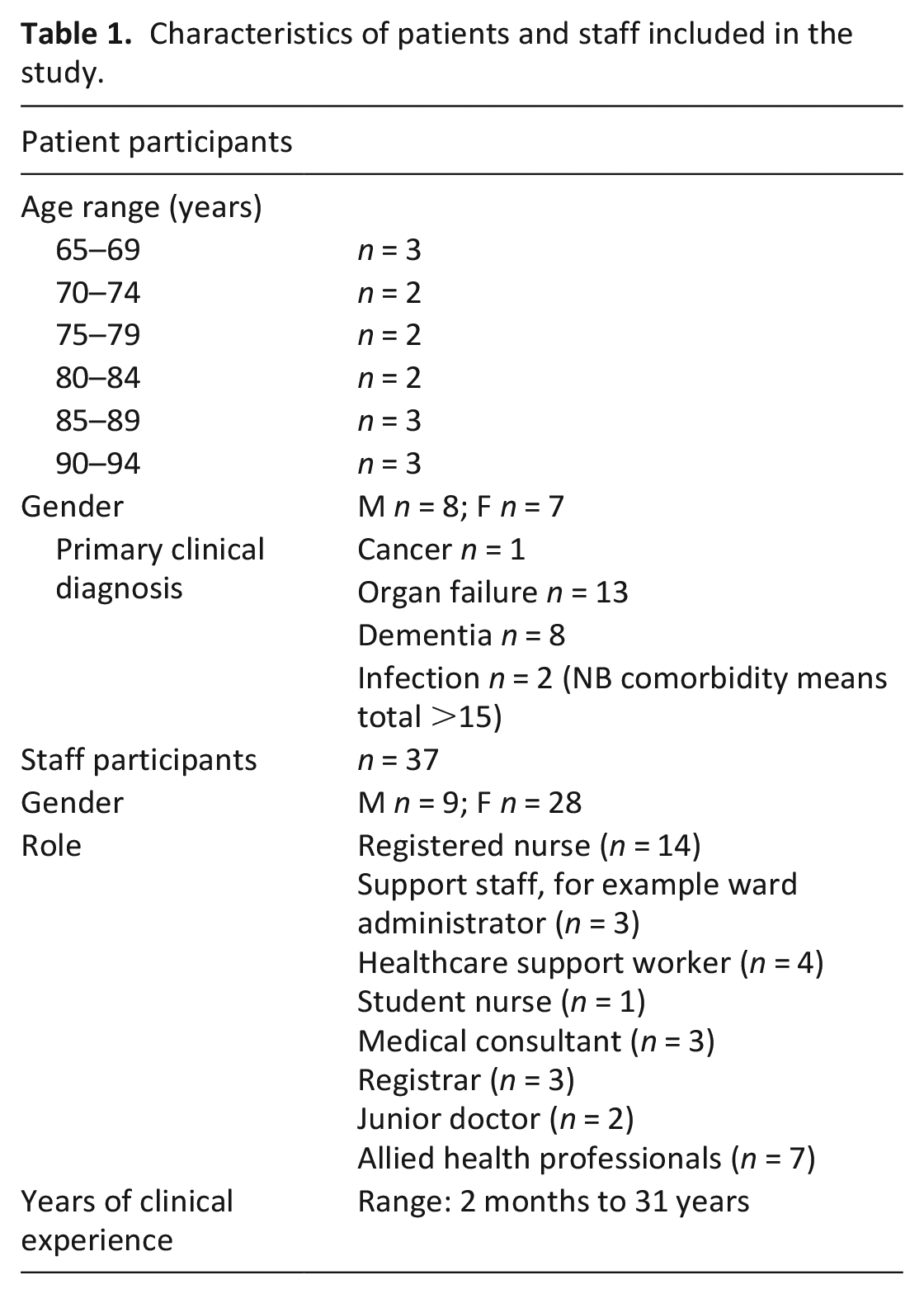
Fifteen patients out of a total of 19 approached participated. 37 staff were observed and none opted out. 4 visitors were also observed, and spoken with. The patients had a range of clinical diagnoses, including chronic obstructive pulmonary disease, dementia, cancer, renal and heart failure. Thirty-seven staff and visitors participated (See Table 1).
Characteristics of patients and staff included in the study.
Themes
Most patients experienced symptoms such as breathlessness, pain or fatigue which caused suffering directly related to their illness, and this was frequently recognised by the clinical team. However, an additional burden of suffering was also observed which was less commonly recognised. This included physical and psychosocial suffering which appeared to be related to the context of care, rather than directly to illness. This suffering is described as iatrogenic since it arose from the context and process of caregiving, rather than through the patients’ clinical condition. 23 Three broad categories of iatrogenic suffering were observed: interventional, interactional and environmental.
Interventional iatrogenesis
Where dying was not recognised or acknowledged, patients frequently underwent interventions that subsequently transpired to have been unnecessary or burdensome. Some of these took place very close to the point of death. This appeared to be related to the default position of the medical staff that any deterioration was presumed reversable in the first instance and to the challenges in identifying when a patient was approaching the end of life. Medical staff attributed this to uncertainty resulting from co-morbidities and the resulting clinical complexity, and the challenges in assessment of patients with cognitive impairment. Nursing staff reported that identifying dying was hampered by unclear communication within and between members of the multidisciplinary team, particularly nurses and doctors, regular and locum or on-call staff, and staff and families. The point at which there was agreement that a patient was dying was typically late, sometimes just hours or minutes before death.
Excerpt 1 provides in-depth account of how clinical uncertainty led to a tilt towards investigation and intervention; how this was compounded by the families’ wish to prolong life and ultimately to a death that was arguably avoidably difficult.
Excerpt 1 (from reflection on field notes) Thursday - Ellen - unconscious when admitted. Suspected brain stem stroke or seizure. She had experienced seizures in the past, but usually recovered within a matter of hours. This time she had been unresponsive for over a day. She had stage IV heart failure and end-stage renal failure. Doctors - absorbed with the task of trying to diagnose the cause of her unconsciousness. The question of whether it was a stroke or a seizure was significant because it impacts upon the likely reversibility of her condition, and hence her prognosis. First day of admission she underwent a battery of tests and scans - inconclusive. Saturday - Anne and Fiona, her daughters, became concerned that Ellen seemed to be becoming weaker; “She hasn’t eaten since she came in”. Requested review with regards to whether she might need a feeding tube. Regular dietician was not available, so she was seen by the on-call, who was given the history from Ellen’s daughters and the nurse. That day a nasogastric tube was sited, and pump feeding was commenced. Monday: Ellen very different. Still mostly unconscious, began to open her eyes and make twitching movements in response to certain stimuli. Daughters took this as a sign of recovery - affirmed their earlier assertions that she needed to have a feeding tube. But when she opened her eyes, they usually rolled back in her head, and were unfocused. Swelling worsened - legs shiny, taut, huge. Makes small retching sounds, her neck occasionally twitches – is she trying to lift her head? Monday evening - began to vomit, syringe driver with antiemetics sited in one of the few areas of her body that was not swollen with fluid. Feeding continues via tube. Over the next two days - frequency of vomiting increased; often tensed her muscles and tried to lean forwards. Sinews on her neck protrude with effort. Veins swollen against her white throat. Her face - smooth and unlined when admitted - became pinched, pale and furrowed. Although at times she seemed almost awake, she was unable to communicate with her family. When she heard the sound of Anne’s voice she would frown, try to turn her head, but then her eyes would again roll back and she would disappear back into her state of diminished awareness. Sunday - after much discussion between the team and Ellen’s family, the feeding tube was removed. Sunday evening - Ellen died; one daughter present.
In this example, Ellen was dying from heart and renal failure, complicated by a cerebral event. The medical staff put their efforts into trying to understand the nature of the cerebral event, putting Ellen through many tests. Although mostly unconscious and apparently dying (in the view of nursing staff), the staff nonetheless put a feeding tube in place, apparently to satisfy her family that she wasn’t going to starve. Ellen then had 4 days of suffering before the tube was removed and Ellen died.
During this time, brief, informal staff interviews shed light on perceptions of Ellen’s situation. Clinicians were uncertain if she had experienced a seizure or stroke, but the decision on the presenting diagnosis gradually became less important as her heart and renal failure worsened. Seeking clarity on her initial diagnosis and adjusting medications was seen as a distraction from the overall picture. Nursing staff expressed concerns that Ellen was dying but could not clearly articulate their reasons. A senior registrar was unsure if Ellen would recover and felt they lacked authority to make a definitive diagnosis of dying. They suggested Ellen’s family was not ready to hear the news and waiting until the right time was mentioned by multiple participants.
Overall, we suggest that the data show that the investigations and the feeding tube created iatrogenic distress and suffering for both Ellen and her family. This position appears to have been related to a lack of holistic clinical consideration of the prognosis. Despite her having advanced heart and renal failure, medical staff did not acknowledge that Ellen was approaching the end of her life. Had this been recognised, staff would also have needed to speak frankly and openly with the family about Ellen’s prognosis but this was side-stepped with a rationalisation of it not being timely for the family.
Other informal conversations with staff also suggested that where there was any possibility, even very remote, that a patient’s condition might be reversible, care frequently defaulted to an approach to care characterised by multiple clinical investigations and interventions. We term this the ‘rescue’ approach to care, as its primary goal is the reversal of deterioration. Some of the resulting interventions, notably intravenous hydration, were not considered beneficial to the patient, as in the following excerpt.
Excerpt 2 (informal interview) Rachel (nurse) reflecting on what happens when someone is dying but the doctors have not yet changed treatment: “There was a man in that middle bay; he was a youngish man with a family. The doctors pumped him so full of fluid even though he had no output, he literally ballooned, there was fluid on his lungs, his skin was breaking down, it was just awful. It was over the weekend that it got really bad - none of the on-call doctors wanted to make a decision to stop because they were frightened about going against the consultant’s orders; they don’t want to overrule a consultant decision.”
The subject of dying was either avoided in conversations between staff and patients or families or alluded to in opaque ways. This appeared to make it more likely that families and patients would actively pursue investigations and treatments, even where these were likely to be futile or burdensome. The perception of ‘something being done’ appeared to be preferable to standing back from treatment: Excerpt 3 (from fieldnotes) Jane (Ellen’s daughter): “She seems to have got worse” Dr Frank: “She’s been here 11 days and obviously we didn’t know why. We passed her NG tube to make sure she got nutrition. She is being monitored and the usual path is improvement. When not improving we look for a specialty to come and help us - like last week when we got Dr X from the Stroke Team. So, we use different specialties for different things. We saw her today again and we don’t think she is improving so we are wondering if we should get people from palliative team to make her more comfortable. . .” Jane: “What will palliative care do?” Dr Frank: “Comfort” Jane: “But that’s what you are doing anyway. . .” Dr Frank: “We are involving another specialism, we stop unnecessary treatment, prescribe meds if she’s in pain”
In excerpt 3, we see the doctor pursuing a convoluted path to telling Jane that her mother is not recovering. In some respects, she is trying to break the bad news gently by using phrases like ‘we are wondering if’ but on the other hand, this obscures her message by making it sound as if her mother may still have hope of recovery especially as she has just said that most people improve. The doctor does not mention death or dying directly and the euphemism of ‘comfort care’ in place of ‘end of life care’ only leaves Jane confused.
Interactional iatrogenesis
The quality of interactions impacted on patient experience. Suffering could be worsened through interactions that were uncompassionate, objectifying or patronising (see excerpt 4).
Excerpt 4 (reflection on fieldnotes) ‘Florence’ - in a side-room because of having an E Coli infection and frequent bouts of diarrhoea. Unable to use the commode, wears incontinence pad, her room smelt of faeces. On one occasion, a doctor asked one of her colleagues if there was such thing as a disposable stethoscope because she didn’t want to use hers to do an abdominal examination. When her colleague told her there was not, she made a visible sign of disgust, in full view of the patient. I, the doctors and nurses were all wearing nitrile gloves and plastic pinafores, in accordance with the Infection Control procedures for patients with this infection. Over a period of several days, Florence gradually withdrew from interacting with the healthcare team, other than to ask for pain relief which she did with increasing frequency, until - according to her medical notes - an assessment by the palliative care team was requested “for psychological aspects of pain”.
Initially, Florence’s isolation was physical, being in a side room, cared for by people wearing personal protective equipment. Subsequently, however, greater distance was created by the interactions described above. Her objectification as an object of disgust was manifested through the nonverbal communication of staff. Other examples of interactional iatrogenesis were observed in the care of people with cognitive impairment. These interactions included ignoring, or using paternalistic or infantilising expressions (see excerpt 5).
Excerpt 5 (fieldnote) Roland: tall, thin, distinguished, has dementia, continuously walks these corridors. Does not like shared bay so won’t stay there – man in bed opposite calls out and disturbs him. R (to me): “Will you come into my room and tell me what you see out of the window so I know which way to go?” (We walk) As we navigate the corridor, he tells me he was looking for his friend John. We sit down together on the plastic covered seating halfway down the corridor and he continues: “He’s not in this graveyard here, he’s in that graveyard there. We’ve been friends for 51 years and now in five years’ time I’ll be dead, I shouldn’t be surprised. All I want is some cash and half an hour to go and visit him on my birthday. I haven’t gone home because there’s a lunatic in my room swearing and shouting. Look, I haven’t even got shoes on.” Three nurses walk past and he stops talking to follow them with his eyes. “All three of them said they’d help but none of them did. They don’t have the power. Fifty-one years. I want to be able to go down the road and feel gracious, feel free. I’m not expecting fees, I just want to be able to say, “Hello John, how are you settling down? I know your wife died, but. . .” we grew up together for 90 years.” “It sounds like you were a bit like brothers”, I tell him. “We were, yes we were. I fail to understand why people can’t say, “Oh, all we’re doing is taking this bloke by the hand and talking for a couple of minutes and then pulling back. . .” His head turns and he looks at my shirt, “It’s no good talking to you, you’ve no authority to help me.” More nurses walk past and he tries to get their attention. They are avoiding eye contact and speeding up slightly as they go past. We sit together for around twenty minutes. “I’m just looking to see him say ‘bye, I’m glad to see you’, that’s all.” He stands up and leaves, walks across to the Clean Utility Room. Hannah (SN) is coming out through the door as he approaches. “This is a sterile room, sweetheart, and only staff can come in. Have you got one of these?” (She shows him her NHS lanyard). He stares. “Why don’t you go and find your shoes?” she suggests. He turns and walks away.
Embedded in Roland’s suffering was a sense of lost identity. He was continuously searching and dealing with his nagging sense he needed to get his shoes on and go and find his longstanding friend. He could not fully understand that he was in hospital but he indicated that he felt ignored as staff failed to listen and help him. While he probably needed staff to listen and understand and walk with him most of his interactions on the ward were functional or involved him receiving instruction or admonishment from staff. Another example occurred a few moments later (see excerpt 5).
Excerpt 5 (cont’d) R is following Lucy, a healthcare assistant, down the corridor: R: “Can you show me?” L: “Right, just take a seat for me because we are going to be busy with dinners soon and the nurses with meds”
In this excerpt, the health care assistant completely ignores Roland’s words and instead uses the sort of language one would use to a child of ‘take a seat for me’ in giving him an instruction to sit down and leave her alone.
Interactions could cause distress where they lacked authenticity (see excerpt 6).
Excerpt 6 (fieldnotes) John, a physiotherapy assistant, comes into the room. “Hello, my name is John”, he says to Vincent. “I know your bloody name is John”, Vincent retorts, “You were only here this morning”. “I know”, John shrugs, “we have to say that. It’s policy.”
Vincent’s anger arose because the introduction by name had the paradoxical impact of worsening, rather than enhancing, a sense of personalised care. The origin of this ‘policy’ was a plea by a patient to healthcare professionals to introduce themselves by Walter, 24 so as to avoid confusion and encourage person-centredness. Yet subsequently her message was bureaucratised and, in this case, although it appears the physiotherapist knew Vincent was well oriented, he failed to personalise care by persisting in re-introducing himself.
Environmental iatrogenesis
The physical environment, and how it was experienced, appeared to exacerbate suffering. Background noises impacted patients because of their intensity. Sometimes, the meaning or interpretation of sounds appeared to cause distress. The sounds of confused patients were commonplace yet frightening for patients who did not know the source of the cries. At other times, sounds evoked a particular response, as in excerpt 7.
Excerpt 7 (fieldnotes) Vincent - waiting for medical investigations of his anaemia. Doctors querying myelodysplasia, a precursor of myeloma. Test is a bone marrow biopsy - drilling into his pelvis to extract a small tissue sample which is examined under a microscope for abnormal cells. His room is positioned midway down the corridor, opposite a utilities cupboard where maintenance workers are rerouting some wiring. This involves a certain amount of hammering, and drilling. Also heard is the continuous sound of Sheila from the room next door "No! No!!" and Lilian, a little further down, screaming "They've taken my eyes". The drilling continues today. I only notice this noise when I sit beside him; the sound enters my field of awareness and I realise I have just been thinking about his biopsy. I cannot separate the two – the thought of the procedure as his bone is drilled, and the sounds of the engineers at work. I recall how just the sound of the dentist’s drill used to make my teeth ache. When the procedure is explained to Vincent the doctor raises his voice over the sound of the drilling. "No, thank you very much", Vincent says, glancing at me and looking fearful.
Staff appeared to be used to the physical environment, exhibiting less sensitivity to noises and smells. In response to the noise described in excerpt 7, staff members simply raised their voices when the drilling increased in volume. However, observation of Vincent shows the distress on his face. It seems possible that this is linked not only to the thought of the procedure but also to the connection I found hard to avoid, as the observer, between the sounds of drilling and the description of the drilling involved in the proposed biopsy.
Excerpt 8 describes the multisensory nature of the ward as perceived by the researcher: Excerpt 8 (fieldnotes) Macerator in the dirty utility room chews up cardboard commode pans & effluent contents and flushes them away, opening like magic to reveal a still-gleaming yaw. Trolley wheels rattle - the newsagent trolley w/ papers, chocolate, drinks and sweets. Smell in V’s room – is it old tobacco, stale urine, illness? - can’t quite capture the nature of the latter. His breath, I think, and an acrid smell that comes from his skin. Slippers frayed and worn, slightly damp and cold to touch. I take them off his feet: the smell hits the back of my throat.
The physical layout of the ward meant that activities of daily living such as eating, defaecating and sleeping took place in proximity or in the same location; for example, a commode would be wheeled away from a bedside to be replaced by a bed table and a bowl of food. Where patients did not eat, this was frequently ascribed to their condition, side effects of medications or overall deterioration, rather than because of how appetising (or otherwise) the experience of mealtimes was. Again, staff appeared less impacted by these concerns; one nurse was informing me about what she planned to have for lunch whilst simultaneously wheeling a commode filled with faeces towards the sluice.
Discussion
Main findings
This study aimed to provide insight into the context of end-of-life care on a single hospital ward for older people. The excerpts illuminate a number of key themes relating to suffering at the end of life.
The suffering experienced by patients was much broader than that related to their physical disease. Suffering was not only related to physical symptoms but also to a range of ways in which patients interacted with other people and with their environment. These aspects of suffering appeared to go unnoticed by staff, perhaps because the healthcare team are accustomed to the processes, sounds, sights and smells and potentially desensitised to the impact on patients.
What this study adds?
This study proposes a relationship between attitudes towards end-of-life care and the conditions that create iatrogenic suffering. Even when the prognosis of imminent end of life was fairly certain, given multiple comorbidities and ongoing deterioration, the default position was to investigate and treat rather than to prioritise comfort and natural dying, creating interventional iatrogenesis. This was particularly prominent where there was uncertainty regarding diagnosis or prognosis. This affirms previous research findings that have suggested that prognostic uncertainty impacts on the likelihood of physicians discussing end of life care with patients and families 25 Further, we surmise that this is related to doctors’ altruistic determination to save lives which forms the bedrock of their identity. For medical staff in particular, a death may feel like a failure in their professional practice. 26 From our observations and interviews, nurses seemed more likely to acknowledge iatrogenic suffering and imminent death. This may be related to their greater exposure to patient suffering as they provide 24-h care. Possibly, as they do not carry the overall responsibility for major treatment decisions but do carry responsibility for day-to-day care, they may be more able to see a holistic picture of patients’ prognosis. This difference in perspectives could be usefully harnessed in multi-disciplinary discussions where medical staff might actively seek the views of nurses on this issue.
Our data showed that both medical and nursing staff put off conversations with relatives about a family member being at end of life, often giving the explanation that it was not being the right time. We suggest this was a rationalisation for avoiding discomfort, not least as it is well established that normative responses to grief frequently entail a degree of denial and disbelief. 14 The avoidance of open discussions about death between staff and relatives seems to have fostered further interventional iatrogenesis. To avoid this, it is essential that staff are skilled in broaching these difficult discussions. There has been a lot of attention given to advanced communication skills in certain specialties such as oncology and palliative care 27 However, our study suggests that this issue still needs to be addressed for staff in this general hospital ward. Given the pervasive (although shifting) taboo in society about talking about death and dying 24 it seems likely this will also be the case in many general hospitals.
Not only was iatrogenic suffering related to treatment interventions but there was also interactional iatrogenesis whereby patients who were very ill or confused were isolated and had little meaningful interaction with staff. Sometimes it appeared that an elderly dying person was a distasteful object to staff who reacted with disgust to some of the associated sights and smells. Talking over a patient is a sign of objectifying the person, apparently failing to register that they may be affected by what is being said. The wider identity of a passive ill person in a bed is perhaps easy for staff to ignore as the patient may not be in a position to actively express any loneliness or need for company. Objectification is one of the dimensions of ‘malignant social psychology’ that was first described by Kitwood in relation to interaction between staff and patients with dementia. 27 This conceptualisation has not previously been applied to understanding the position of older ill people in general hospital care but could usefully be taken forward to help educate staff about interaction that recognises and supports ‘personhood’. Such training could contribute to improved quality of life for older ill people in hospital.
People with confusion due to dementia seemed to be at particular risk of interactional iatrogenesis. We saw example of their attempts at communication ignored by staff who probably saw them as a nuisance. Being ignored is likely to increase restless and distress so detracts from quality of life. The difficulty of nursing patients with dementia on general hospital wards has been widely acknowledged and some studies have noted poor interaction. 28 Care for these patients must go beyond gestures such as introductions by name.
Finally, environmental iatrogenic suffering was evident from observations. The lived experience of being in hospital during a period of illness may impact on a patient’s overall wellbeing beyond their physiological recovery. If suffering is to be ameliorated, then those hospital admissions that are deemed to be necessary should consider the whole experience of hospitalisation for individual patients. The environment of care should be designed not only with clinical convenience and infection control in mind, but the recognition that patients may benefit from a low stimulation care setting. 29
At an educational event, data was presented back to the multidisciplinary team on the hospital ward where data was collected. Many of the scenarios were instantly recognised, and staff agreed about the challenges identified. They suggested it was valuable to hear their work described as a series of narratives where they were able to view the bigger picture, beyond their own interventions. Some found listening to the narratives uncomfortable but nonetheless agreed that it was a useful learning experience. We recommend this approach could be a helpful training exercise for wards and teams. Dementia Care Mapping 30 is an approach built on systematic observation of quality of care which pays particular attention to interaction and this could be adapted and piloted as a tool for raising quality of care to reduce interactional iatrogenesis. At the heart of some of suffering we saw, was discomfort with death and dying. Attention needs to be paid to enabling all staff in general care of the elderly wards to feel more comfortable to recognise and talk about end of life.
Strengths and limitations
This study was a small, single-site ethnographic research project. As such it seeks to present a vivid impression of end-of-life care without making claims regarding generalisability. Potential bias has been addressed by sharing and discussing the findings with Experts-by-Experience, with the ward multidisciplinary team and with doctoral supervisors. The impact of participant observation on the field of study has been debated widely in the literature.29,30 Nonetheless it is hoped that the reflexive approach employed offers an important insight into a poorly researched area. There is a need for patient-centred research methods for understanding the nuanced aspects of care that cannot necessarily be captured using retrospective or proxy methods.
Conclusion
The goal of palliative care is to ameliorate suffering wherever possible. This ethnographic study has demonstrated that as well as being responsive to suffering related to life-limiting illness, healthcare professionals must be sensitive to the potential for iatrogenesis and make efforts to ameliorate the negative impact of the healthcare environment. The potential negative impact of interactions, interventions and environment must be considered, alongside the clinical aspects of care. Future research should focus on obstacles to timely diagnosis of dying, and how this is related to the provision of compassionate care.
Footnotes
Author contributions
LG: main author and principal investigator; JO: doctoral supervisor – critical revisions; AC: doctoral supervisor – critical revisions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was carried out as part of a doctoral study funded by the University of Bradford.