
Abstract
Background:
Acceptance and Commitment Therapy is a form of Cognitive Behavioural Therapy which uses behavioural psychology, values, acceptance and mindfulness techniques to improve mental health and wellbeing. Acceptance and Commitment Therapy is efficacious in treating stress, anxiety and depression in a broad range of settings including occupational contexts where emotional labour is high. This approach could help palliative care staff to manage work-related stress and promote wellbeing.
Aim:
To develop, and feasibility test, an online Acceptance and Commitment Therapy intervention to improve wellbeing of palliative care staff.
Design:
A single-arm feasibility trial of an 8-week Acceptance and Commitment Therapy based intervention for staff, consisting of three online facilitated group workshops and five online individual self-directed learning modules. Data was collected via online questionnaire at four time-points and online focus groups at follow-up.
Setting/participants:
Participants were recruited from Marie Curie hospice and nursing services in Scotland.
Results:
Twenty five staff commenced and 23 completed the intervention (93%). Fifteen participated in focus groups. Twelve (48%) completed questionnaires at follow-up. Participants found the intervention enjoyable, informative and beneficial. There was preliminary evidence for improvements in psychological flexibility (Cohen’s d = 0.7) and mental wellbeing (Cohen’s d = 0.49) between baseline and follow-up, but minimal change in perceived stress, burnout or compassion satisfaction.
Conclusion:
Online Acceptance and Commitment Therapy for wellbeing is acceptable to palliative care staff and feasible to implement using Microsoft Teams in a palliative care setting. Incorporating ways to promote long-term maintenance of behaviour changes, and strategies to optimise data collection at follow-up are key considerations for future intervention refinement and evaluation.
Keywords
Working in palliative care involves a high degree of emotional labour and potential for stress.
Acceptance and Commitment Therapy is effective in workplace stress management interventions.
Online Acceptance and Commitment Therapy consisting of self-directed learning resources and facilitated online sessions is feasible to deliver and acceptable to palliative care staff.
Challenges to retention of participants post-intervention delivery to evaluate longer terms impacts are identified.
The RESTORE intervention needs to be refined and then evaluated with a larger sample to assess effectiveness and cost-effectiveness.
Training palliative care staff to apply individualised Acceptance and Commitment Therapy based strategies in their own lives may help them to manage the emotional impact of their work.
Communities of practice may be needed to help sustain this work.
Background
Palliative care work is generally viewed as rewarding, bringing meaning, and purpose to professional care staff.1–3 However, alongside positive experiences, stress, distress and burnout are common.4–6 Some stressors are typical of those identified across healthcare settings such as unmanageable workloads, shift work, staff shortages and lack of training on specific issues. 6 Additional stressors specific to palliative care include regular exposure to death, loss and grief. This can include caring for a dying person of a similar age or background; caring for a dying child or person with dependent children; caring for a person with a complex physical condition; managing uncontrolled symptoms and breaking bad news.6–8 Balancing the rewards associated with palliative care work with the emotional challenges is an ongoing task.
The COVID-19 pandemic led to increased stress, distress, and burnout across the health and social care workforce,9–12 including palliative care13–16 and exacerbated the need for healthcare staff support internationally.13–17 A considerable proportion of the healthcare workforce experienced mood and sleep disturbances, raising concerns about risks to mental health. 9 In palliative care, staff encountered rapidly changing clinical roles; new modes of service delivery, reduced staffing and increased patient numbers; coupled with risk of infection and limitations in personal protective equipment.13,14 Many palliative care staff felt overwhelmed by the need to support families through telephone or video platforms due to social distancing measures; and remote consultations concerning sensitive and emotive end-of-life care concerns were challenging.15,16 Supports needs of staff increased, and the 2020 Nursing Standard-Marie Curie survey revealed that 45% of respondents reported insufficient support at work to manage grief and emotional stress, up from one-third in 2019. 17
Interventions to support wellbeing in palliative care staff are needed now more than ever. A systematic review prior to the COVID pandemic identified nine intervention studies to improve palliative care staff wellbeing including music therapy, a stress reduction programme, art therapy, a sleep intervention and a psycho-existential intervention. 18 Evidence for the effectiveness of any particular intervention was inconclusive, and the authors concluded that more theory-driven development of psychosocial interventions to improve staff wellbeing were needed. 18 Acceptance and Commitment Therapy is used in hospice settings, 19 but has not previously been evaluated as an approach for improving wellbeing in palliative care staff. Outside of palliative care, there is a growing evidence base that ACT is effective in improving general and work-related distress compared to a control condition, though overall quality of evidence is low. 20 High quality research that seeks to design and further evaluate interventions, including ACT, to promote wellbeing amongst palliative care staff are warranted.
We propose an Acceptance and Commitment Therapy based psychological intervention to help palliative care staff to manage work-related stress and distress.21,22 Acceptance and Commitment Therapy is an empirically supported form of Cognitive Behavioural Therapy which uses behavioural psychology, values, acceptance, and mindfulness techniques to improve mental health and wellbeing by increasing psychological flexibility. 21 Psychological flexibility refers to the ability to act mindfully, guided by our values. 23 Acceptance and Commitment Therapy differs from traditional behavioural and cognitive interventions in that, rather than teaching methods of suppressing or challenging thoughts, it encourages greater awareness and acceptance of both positive and negative internal events. This promotes ‘opening up’ to unwanted inner experiences, when doing so is helpful in pursuing what is important to the person. Previous research identified common responses to workplace stressors in palliative care staff including emotional suppression, over-identification with patient suffering, and neglect of self-care behaviours.2,6 These kinds of responses are typically targetted by Acceptance and Commitment Therapy. Acceptance and Commitment Therapy is efficacious in treating stress, anxiety and depression in a broad range of populations, including occupational contexts where emotional labour is high.22,24–26 It may be especially suited to promoting palliative care staff wellbeing because it supports being present in the face of distress, being open to initiating difficult conversations, and acting in a way that is underpinned by values.2,27 It may also reduce unhelpful responses such as self-doubt, rumination, and over-identifying with patients and families. 2
Our aim was to develop, and feasibility test an Acceptance and Commitment Therapy intervention to improve wellbeing of staff working in palliative care settings. Given the rapid emergence of digital interventions in palliative care, 28 combined with the flexibility and scalability of an online intervention format, and the need to replace in-person with remote interventions during the COVID-19 pandemic, an online intervention was designed. We chose RESTORE (Research Evaluating Staff Training for Resilience) as the study acronym, as it reflected the aim of maintaining and restoring workplace mental health and wellbeing. The research questions were:
What is the experience of palliative care staff undertaking online Acceptance and Commitment Therapy and is it acceptable and feasible?
Is there preliminary evidence that online Acceptance and Commitment Therapy leads to improvements in psychological flexibility, wellbeing and stress?
What are the barriers and facilitators to implementing online Acceptance and Commitment Therapy for palliative care staff and what are the implications for future evaluation?
Methods
Design
A single-arm feasibility trial of an online Acceptance and Commitment Therapy -based intervention for staff providing palliative care for terminally ill adults. We used convergent mixed methods to address the research questions. 29 A convergent design allowed us to combine the results of both qualitative and quantitative data analysis in order to obtain a more complete understanding of the impact of the acceptability, feasibility and potential impact of the intervention. The study protocol was registered (https://doi.org/10.1186/ISRCTN14313559) and published. 30
Setting
The study was hosted by Marie Curie Scotland. Marie Curie is the largest independent provider of end-of-life care and the largest charitable provider of hospice-based care in Scotland (https://www.mariecurie.org.uk). Two Marie Curie hospices, located in Edinburgh and Glasgow, provide short-term inpatient hospice care and outpatient services for terminally ill people and families in surrounding areas. Across Scotland, the Marie Curie Nursing Service (MCNS) provides palliative care to people in their own homes. The intervention was delivered to staff participants online via Microsoft Teams. Participants could choose to take part in their personal time or during working hours, or both.
The original study was designed as an in-person intervention, to be delivered over 2.5 days (two full days and a follow up) at the Edinburgh hospice. However, the study was put on hold due to the COVID pandemic. Subsequently, in consultation with the hospice management team, it was redesigned for online delivery and also opened to staff at the Glasgow hospice and Marie Curie Nursing Service.
Participants
Participants were recruited from two Marie Curie hospices and from the Marie Curie Nursing Service in Scotland. As this was a feasibility study, sample size was not formally calculated. 31 Based on prior experience, resources available and the format of the intervention, we judged that a sample of 30 would be sufficient to enable a decision about feasibility to be made. Eligible participants were health and social care professionals providing direct support to terminally ill patients and their families. This included nursing and medical staff, allied health professionals, social workers and healthcare assistants. Staff who had previously undertaken Acceptance and Commitment Therapy were excluded.
Participant recruitment
The research team held an online information session with service managers across Marie Curie. The study was promoted via hospice newsletters, posters and internal chat forums. Invitation letters were shared with staff by their service managers. Interested staff completed an online consent form prior to participating.
Intervention design and content
Content
The RESTORE intervention was developed by the research team. The content was informed by previous interventions delivered by the team for health professionals in other settings, as well as research on occupational stress, wellbeing, self-compassion and resilience in palliative care.2,22,32,33
Format
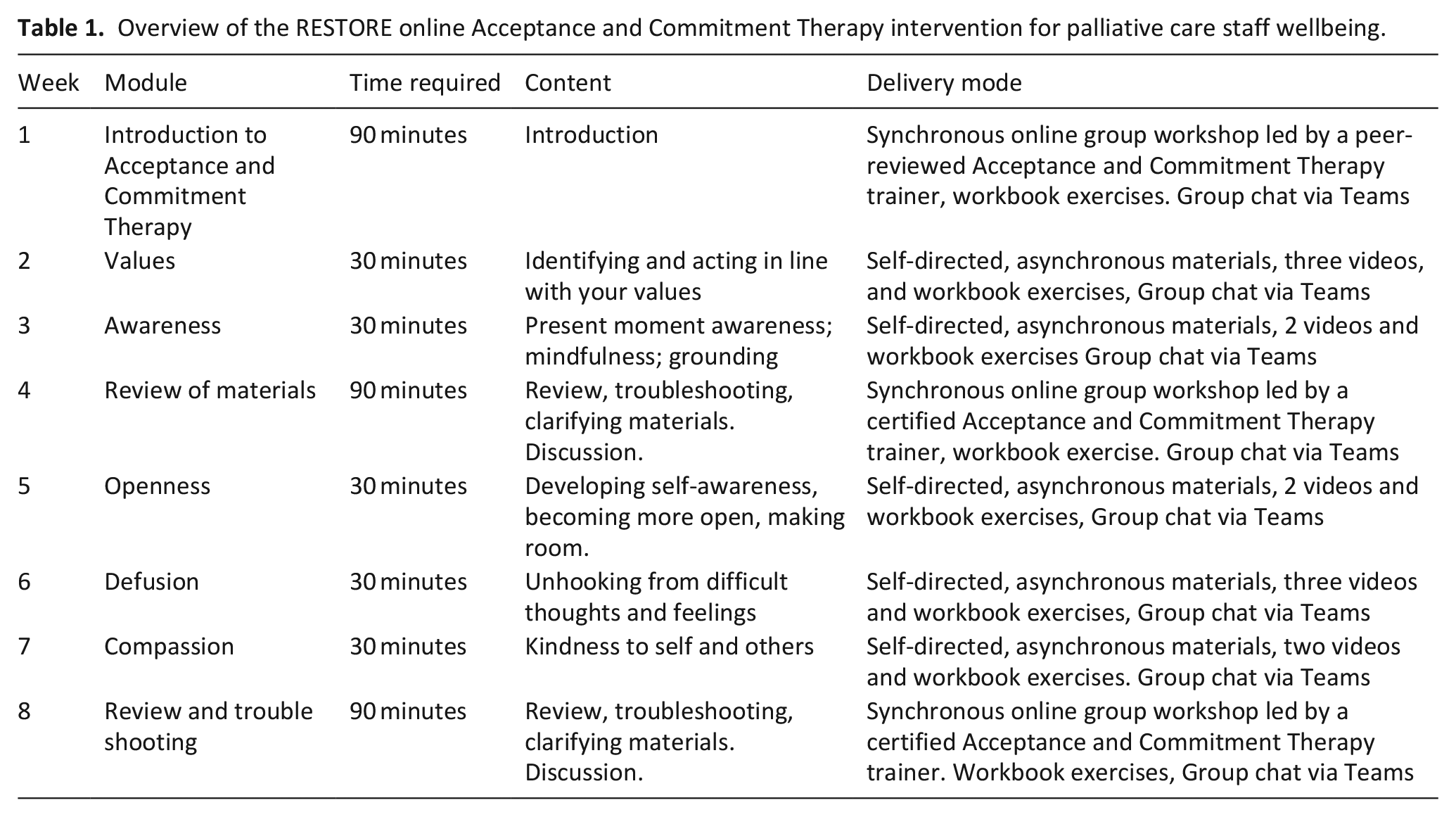
Intervention format was guided by the format of previous interventions developed for related populations including patients,34,35 and dementia care staff 36 and by advice from the host organisation in terms of what format might work best given clinical demands for staff (i.e. flexible format with some self-directed content). The intervention consisted of eight modules delivered via Microsoft Teams over an 8-week period, including three facilitated online group workshops and five self-directed, e-learning modules (Table 1). Participants received a workbook outlining the content for each week. The RESTORE manual and workbook is available on the ISRCTN registry: https://doi.org/10.1186/ISRCTN14313559.
Overview of the RESTORE online Acceptance and Commitment Therapy intervention for palliative care staff wellbeing.
Facilitation
Online workshops were delivered by a Senior Academic Clinical Psychologist with extensive training and experience in Acceptance and Commitment Therapy (DG). DG is also a Peer Reviewed Acceptance and Commitment Therapy Trainer and Fellow of the Association for Contextual Behavioural Science (a mark of quality and fidelity of Acceptance and Commitment Therapy knowledge and skill). Workshops were also facilitated by a research psychologist (AF).
Homework
Participants were asked to complete ‘homework’ each week. For example, to practice a brief mindfulness exercise or try out different strategies to ‘unhook’ from unhelpful thoughts.
Adherence
To facilitate adherence, participants were sent weekly reminders to alert them that the new module content for that week was available.
Intervention fidelity
Intervention fidelity was not formally assessed. However, in the live sessions, the second facilitator (AF) took a monitoring role, ensuring that all elements of the sessions were covered as planned in an Acceptance and Commitment Therapy consistent way.
Research data collection
number of participants recruited (target: 30).
number of participants completing intervention (target: two-thirds of those who commenced the intervention), this measure also reflected intervention acceptability.
number who completed the outcome measures (target: two-thirds of those who commenced the intervention).
number of participants who took part in post-intervention focus groups/interviews (target: 50%–75% of participants commencing the intervention).
Quantitative data collection
Five key outcomes were assessed prospectively at four time-points via online survey (https://www.onlinesurveys.ac.uk): before the intervention, mid-way (week 4), on completion (week 8) and 1-month post-intervention (follow-up). Further detail is available in the protocol. 30 The questionnaire was designed such that all questionnaire items needed to be completed before moving on the next page, thus minimising missing data.
Qualitative data collection
Online focus groups (MS Teams) were held approximately 1-month post-intervention (November 2021) and explored participant’s perspectives regarding acceptability, feasibility, and potential effectiveness (See Supplemental Information). All participants were invited to take part. Focus groups were facilitated by an experienced qualitative researcher (BS), not personally known to participants. Participants who dropped out were invited to share their reasons in a brief interview.
Quantitative data analysis
The main outcomes were feasibility related (recruitment, attrition, retention and evaluation completion); as such, this study was underpowered to detect statistically significant improvements in the non-feasibility outcomes (e.g. stress, quality of life, wellbeing). However, we did conduct paired sample t-tests to explore any changes in outcomes between baseline and follow-up for participants who completed both measures. We were most interested in evidence in change in outcomes from baseline (pre-intervention) to follow-up (1-month post-intervention). We calculated effect size (Cohen’s d) to illustrate the size and direction of any change that might be anticipated in future studies.
Qualitative data analysis
Focus groups were transcribed verbatim prior to analysis. Qualitative data analysis was undertaken by AF and BS guided by the framework approach using NVivo 12. 32 AF undertook the initial coding, developed and applied the analytical framework and summarised the data. BS, who had facilitated the focus groups, provided additional support at the data interpretation stage.
Ethics and governance
The intervention was originally designed for in-person delivery and sponsorship approval was obtained from the University of Edinburgh on 18 February 2020. However, due to the COVID pandemic, the study was suspended in March 2020. In consultation with the hospice management team, the intervention was redesigned for online delivery in 2021. Sponsorship approval for the redesigned study was obtained from the University of Edinburgh Research Governance Office on 7/4/21; ethical approval was obtained from the University of Edinburgh Clinical Psychology Research Ethics Committee on 20/5/2021 (Ref: CLPS021s); and approval from the Marie Curie Research Governance Committee in Scotland was obtained on 15/6/2021. Full details on the management of personal data, data transfer, data storage and confidentiality are described in the study protocol. 30
Results
Sample characteristics and feasibility outcomes
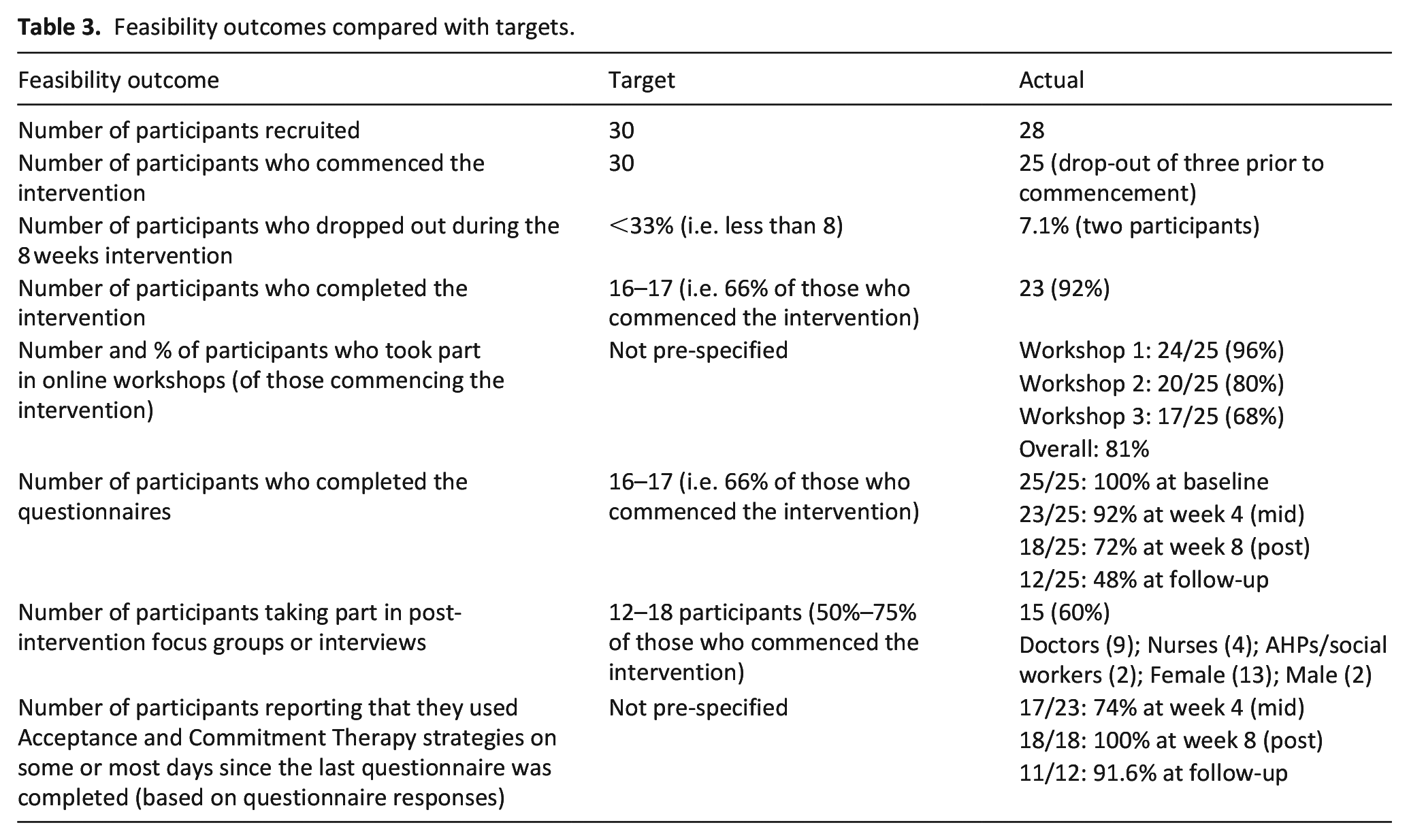
Twenty-eight participants were recruited (Table 2), just under our recruitment target (Table 3). The sample was predominantly white female, aged between 25 and 54 years. Professionally they were mostly doctors and community or inpatient nurses, with over 5 years’ experience in palliative care. Prior to the intervention, three dropped out, and did not complete baseline measures, with the following reasons given: changed circumstances (n = 1); sick leave (n = 1) and no information (n = 1). Nearly all of those who commenced the intervention completed it: only two dropped out, citing sick leave (n = 1) and personal reasons/lack of time (n = 1). Questionnaire completion fell over the course of the study with just 48% completing questionnaires 1-month post-intervention. Focus group participation was affected by annual leave, sick leave and work patterns, but was in line with target. Overall, 15 participants took part in a focus group at follow-up (13 female and 2 male). This included nine doctors, four nurses and two allied health professionals or social workers.
Participant characteristics.
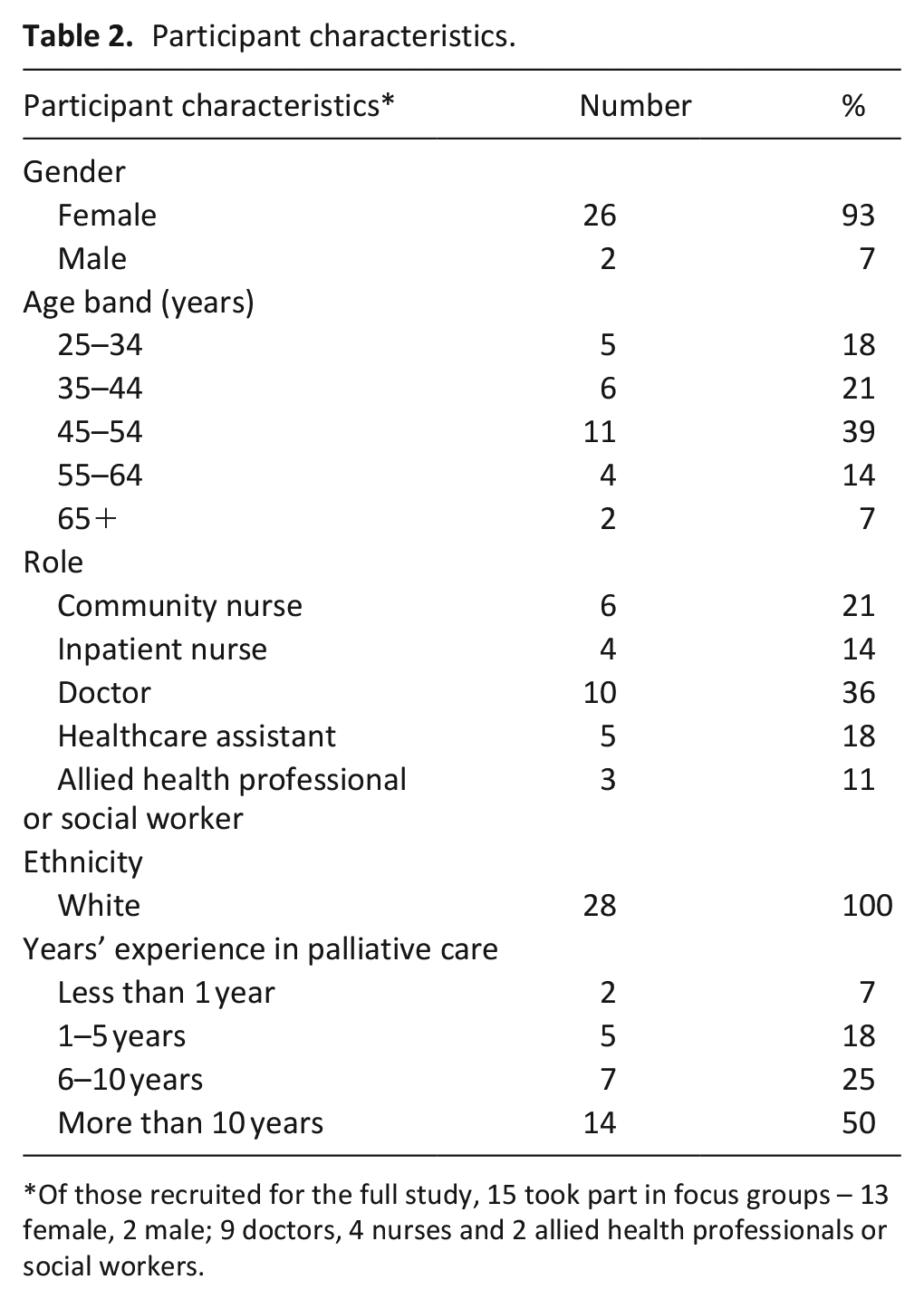
Of those recruited for the full study, 15 took part in focus groups – 13 female, 2 male; 9 doctors, 4 nurses and 2 allied health professionals or social workers.
Feasibility outcomes compared with targets.
Staff perspectives on acceptability of the intervention
Participants reported that RESTORE provided a positive experience overall. They found it to be enjoyable, informative and beneficial. Participants valued the opportunity to step back and reflect on how they approach challenges in everyday life.
“I really enjoyed it and you know, quite a lot of the techniques that they were showing us and asking us to do I found really helpful in allowing yourself some space and time to think, or to clear your mind. . .”. (FG 5, P3)
The structure, format and mode of delivery was acceptable to participants. The blended approach, consisting of a mix of online self-guided and facilitated sessions, was acceptable and highly valued. The online group sessions allowed participants share experiences with colleagues, seek clarification and engage with the materials on a deeper level.
“I definitely wouldn’t have got as much just going through the material without that ability to hear other people’s reflections and stories, and the challenges. . .. “(FG4, P1)
The self-directed modules allowed participants to engage flexibly with the content and created opportunities to reflect personally on the material:
“. . .good balance with the self-work that you needed to do. . . I think if it had all been face-to-face sessions I wouldn’t have got so much out of it because you really do need to work through it” (FG4, P2)
The workbook helped participants stay on track each week and provided dedicated place for note-keeping that could be referred to even after the intervention had been completed.
“It was really helpful to have the workbook as well. I think you know it wasn’t just about you doing your own notes, the workbook running alongside it was really good” (FG5, P3)
Participants noted the high quality of facilitation of group sessions. The online aspect did not impede the ability of participants to feel they were in a safe space and open-up about their experiences.
“It was really well facilitated, you know like there’s all these problems where everyone talks at the same time or who knows when to speak, but the facilitation of it was really good and putting your hand up when people wanted to speak like yeah it was much better on Teams than I thought it was going to be. (FG2, P1)”
Preliminary evidence for intervention effectiveness
There was no difference in baseline outcome measure scores for the participants who completed outcome measures at follow-up (n = 12) compared to those who did not (n = 13). (Supplemental information file). For the 12 participants completing questionnaires at follow-up, we found preliminary evidence for improvements in psychological flexibility (Cohen’s d = 0.70), particularly valued action (Cohen’s d = 0.83) and openness (Cohen’s d = 0.66) (Table 4). There were increases in defusion between baseline and follow-up (Cohen’s d = 0.64), but only small or minimal changes for engagement and awareness. There were improvements in overall wellbeing (Cohen’s d = 0.49), but only a small reduction in stress (Cohen’s d = −0.34). There was little change in burnout or compassion satisfaction, though secondary trauma scores fell between baseline and follow-up (Cohens d = −1.03). At baseline, participant scores were high on compassion satisfaction, and low on burnout suggesting floor and ceiling effects. 42 No participant met the threshold for burnout at baseline, thus improvements on these outcomes were unlikely.
Outcome data from baseline to follow-up.
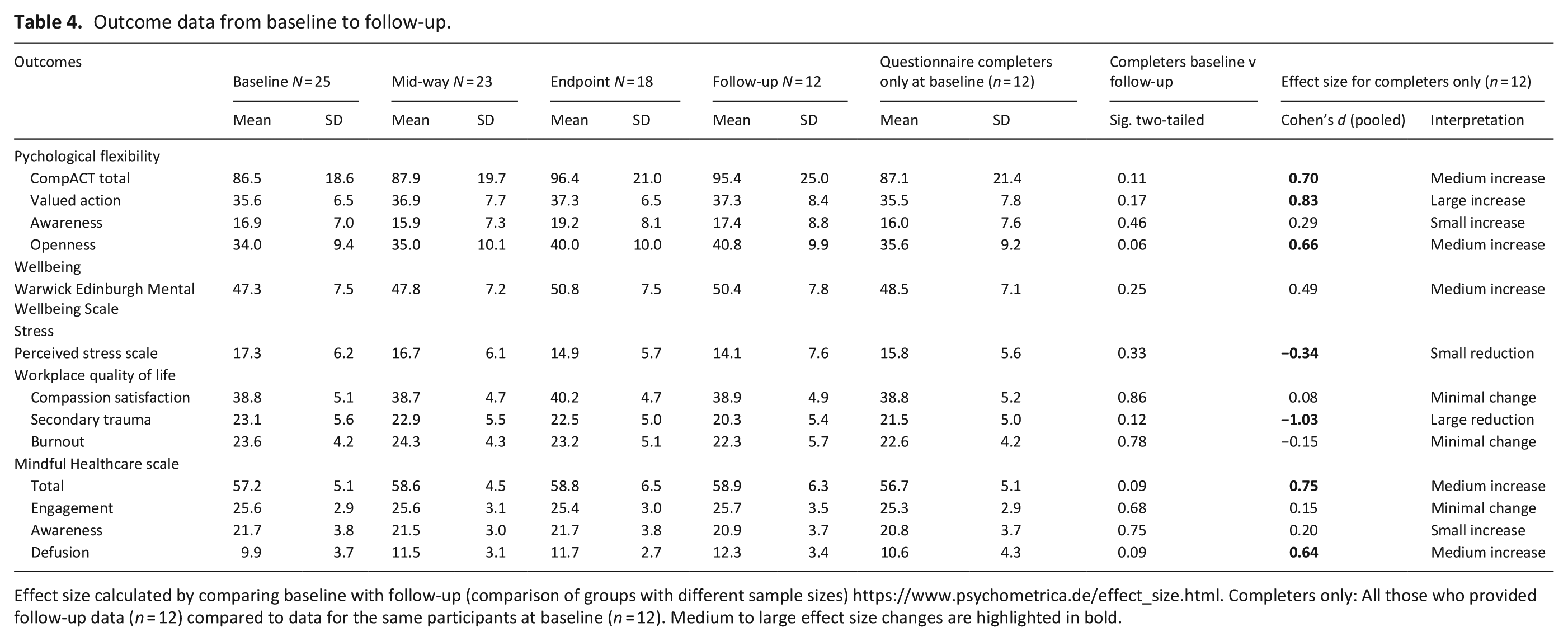
Effect size calculated by comparing baseline with follow-up (comparison of groups with different sample sizes) https://www.psychometrica.de/effect_size.html. Completers only: All those who provided follow-up data (n = 12) compared to data for the same participants at baseline (n = 12). Medium to large effect size changes are highlighted in bold.
Preliminary evidence for effectiveness could also be interpreted in the qualitative data. No negative impacts were reported. Participants reported that they became more aware of their thoughts, emotions and feelings:
“I suppose one of the themes that ran through it was you’re not necessarily your thoughts and you don’t have to buy into them or to live by them, you can just notice them. So, all really helpful concepts. . .(FG5, P1)
Participants developed strategies to ‘unhook’ from unwanted thoughts and feelings and valued the practical nature of the exercises.
“I think probably the most helpful things [were] the kind of practical tips . . . ways to break those anxious thoughts or negative thoughts on a day-to-day basis” (FG3, P3)
The present moment awareness exercises helped participants to slow down, connect with the present moment, relax and unwind.
“I remember one day in work it was just chaotic . . .I sat down and my head was still buzzing, like I just couldn’t concentrate on anything. But then actually when I started sitting. . . eating, and reflecting on that, it definitely made a difference”(FG2, P2)
The self-care component highlighted the value of reducing self-criticism and creating opportunities to look after oneself.
“. . .I’ve started to be kinder to myself in those situations than I was before. . .”.(FG4, P2)
Barriers and facilitators to intervention engagement
Common barriers to engagement with the intervention were (i) time constraints and (ii) staff wellbeing not seen as a priority. For instance:
I have struggled to find the time to engage as much as I would have liked. I think setting aside dedicated time when I am able to devote my full attention to it in a quiet space has been difficult. . .. (QT1, P17).
Engagement was more difficult for staff who work shift patterns, or who needed colleagues to cover their regular duties:
“. . .because I was rostered on shift quite a lot of the time when we had the meetings and occasionally it would be too busy, there would be no staff to cover me, so I found that a bit of a barrier”. . . (FG5, P2)
Some participants felt guilty about taking time out for a wellbeing intervention given their current workloads and did not view their own wellbeing as a priority.
Clinical demands resulted in prioritising patient care over staff wellbeing.
“Ultimately the top-down pressure is because of staffing so they can’t get time off the ward because there’s not enough of them to cover. . .certainly though, it [staff wellbeing] would never be seen as a priority. (FG2, P1)
Intervention engagement was facilitated by: (i) senior management support; (ii) protected time; (iii) flexible format and (iv) private space to engage in the intervention:
“We were very much supported by the senior (profession) team to take part in this. . . on the day making sure that . . .the service is covered. . . allowing us to get to sessions. . .” (FG6, 2)
Protected time, or the ability to plan your own time also made participation easier:
“I’m not on the ward all the time, my office is downstairs so I can ensure that time is protected. Like I can work my diary around it. . .” (FG2, P2)
The flexible format allowed participants to engage with the resources in a time that suited them – either in the workplace or at home. Having a private office or home space facilitated full participation in the online sessions. For those working in open offices, this was more difficult due to interruptions, and lack of privacy:
“I actually was working from home so I was removed from the office, no phone calls, no nothing, so that was actually really, really helpful” (FG5, P6)
Future implementation and evaluation
Most participants would have liked more opportunities to consolidate their learning, and allow more time to practice new strategies between workshops:
“It was great but to me actually it felt quite short and quite rushed and not giving me enough time to really consolidate some of the [techniques]”. . .(FG5, P5)
Many reported that they would like a top-up or follow-up session in the future:
‘It might be quite helpful to check in again at 3 months and say ok you know how is everybody and how have you got on?’ (FG1, P1)
Participants viewed the online questionnaires as onerous, with two participants referring to the process as ‘tortuous’!
“I would agree, they felt really long. . .it was a wee bit onerous, definitely”. (FG5, P6)
Although nearly all participants remained in the intervention, just under half (48%) completed the questionnaires at follow up. Despite reminders, questionnaire completion at follow-up was not a priority for staff and was often forgotten with time pressures and clinical priorities:
“it’s not a lack of enthusiasm for wanting to complete the questionnaire itself. . ., it’s just it being lost in a ream of other things. And forgetting, like when it comes through you may be getting emails of other things you need to prioritise in that moment so you see it and you think ‘I’ll go back and do that’ and then you forget to go back and do it” (FG4, P2)
Discussion
An online Acceptance and Commitment Therapy intervention to improve wellbeing was perceived as feasible and acceptable to palliative care staff. Once commenced, retention was good, and participants found RESTORE enjoyable, informative and beneficial. Data collection was feasible during the intervention but challenging at follow-up. Between baseline and follow-up there was preliminary evidence for improvements in psychological flexibility and mental wellbeing. Overall, these findings suggest that online Acceptance and Commitment Therapy shows promise as an accessible and flexible intervention that could support staff wellbeing in palliative care settings. Further intervention refinement and pilot-testing is warranted.
Improvements in psychological flexibility and overall mental wellbeing were not statistically significant. This was to be expected given the low sample size and emphasis on acceptability and feasibility over effectiveness. Many feasibility studies are not powered to detect significant differences in outcomes, rather the focus is on whether the intervention looks promising and can be evaluated. 31 However, the general direction of change was aligned with improved wellbeing, and when combined with qualitative findings we judge that these findings support further intervention refinement and evaluation.
The intervention was acceptable to staff. Despite workload constraints, and intervention delivery during the COVID-19 pandemic (September–December 2021), recruitment was close to target and there was high staff retention, with staff reporting positive experiences and impacts relating to participation. Participants reported examples of increased contact with the present moment, greater likelihood to prioritise self-care and use of techniques to help them step back from overwhelming thoughts and feelings. Similar impacts were identified by dementia care workers, who reported greater present moment awareness, clearer focus on values, and changes in self-care behaviour following an Acceptance and Commitment Therapy intervention. 36
None of our participants were experiencing burnout at baseline pointing to the value of offering online Acceptance and Commitment Therapy as a protective measure, allowing them to develop skills that they could draw on in future challenging situations. Proactively preparing for challenging future situations, both at an individual and organisational level, may help mitigate experiences of psychological distress when a future crisis occurs. 47 Healthcare staff value the opportunity to access psychological support and learn techniques that support wellbeing. Those who have access to such supports feel valued and supported by their employer,48,49 thus organisational-level benefits may accrue when wellbeing interventions are provided.
Our findings provide further evidence that online psychological support is acceptable to palliative care staff. Prior to the COVID-19 pandemic, there was already evidence for the utility of digital health interventions for education and training, with online learning and video-conferencing playing a critical role. 28 Cost-savings associated with reduced travel, alongside greater access to support were identified as benefits of online formats previously 50 and were found to facilitate participation in this study. Previously there was mixed views on the delivery of psychological support online, with some suggesting that face-to-face interventions are better for psychological concerns. 51 However, staff in our study were comfortable discussing psychological issues and felt safe to share their views and experiences in online group session. A recent review showed that online Acceptance and Commitment Therapy improves mental health outcomes including anxiety, depression and psychological flexibility in a range of contexts, especially with therapist guidance. 52 Given the scalability of online formats, continued work to adapt in-person formats for online delivery, so they can be accessed by more people, are essential.
Sustaining the effects of any intervention beyond the course of a research project is challenging. 53 Consideration of longer terms plans for intervention implementation is needed from the early stages of development. 54 Sustainable interventions should have perceived benefits or value to participants; they need to be embedded into the habitual practices of individuals, organisations and systems; and the intervention needs to evolve to fit with individual and organisational needs over time. 53 For successful implementation, clearly communicating the potential benefits of Acceptance and Commitment Therapy who to staff; identifying protected time to participate; and routinely collecting feedback to refine the intervention, will be essential. Leadership and contextual factors also influence sustainability. 53 We had strong senior manager and clinician support, yet there were still context-related barriers to engagement such as shift patterns, time constraints, and prioritisation of clinical priorities over staff wellbeing. Recognition of these tensions, and planning to prioritise staff participation early on, will likely optimise engagement and sustainability over time.
Implications for future intervention development and evaluation
In a follow-up study, the Warwick-Edinburgh Mental Wellbeing Scale43,44 would be most useful to include as a main outcome, given that it showed greater sensitivity to change than the other measures examined. Participants would have welcomed more time to embed the new techniques in practice, so follow-up sessions or peer-support groups to sustain practice in the longer term will need to be built into intervention design. Furthermore, our intervention was delivered by an experienced Acceptance and Commitment Therapy trainer who led the online group sessions; future interventions need to be designed to allow delivery by organisational staff such as a Palliative Care Nurse Specialists, Doctors, Social Workers or Allied Health Professionals. To support upscaling, training for professionals to deliver the intervention will need to be developed and evaluated. Longer-term, there is potential for RESTORE to be adapted to support palliative care staff wellbeing in other countries: even though care systems may differ, the personal coping skills trained in RESTORE are likely to have commonalities across culture. As with any validation to other health care settings, this would require consideration of the intervention-context fit to inform judgements on transferability and decisions on the nature and extent of adaptations required.
Strategies to improve data collection at follow-up will be needed for future studies. In the present study, quantitative data collection fell at the 1-month post-intervention point. The fact that this study was conducted in the midst of the COVID pandemic, with intense pressures on staffing alongside clinical challenges, is likely to have influenced participants ability to prioritise completion of quantitative data at follow-up. Some suggestions to improve data collection at follow-up in the future include: (i) availability of a research nurse or assistant to prompt participants to complete follow-up data; (ii) encourage participants to add prompts to their diaries indicating when data needs to be returned; (iii) reducing the number of data collection points (e.g. removing the mid-study data collection point); (iv) consider incentivising questionnaire completion, for example providing a voucher or entry to a prize draw for those who complete outcomes at the follow-up. (v) Clearly communicate, and reiterate, the importance of the evaluation aspect of the study to participants, which may seen as of less value to participants than the act of taking part in the intervention. While much previous research has examined recruitment issues in palliative care settings, further research on effective strategies to support retention and follow-up beyond the course of an intervention are recommended.
Further research is needed to refine the intervention and evaluate its effectiveness compared with other forms of wellbeing support or no support. The effect of the intervention on outcomes such as stress-management self-efficacy, need also to be explored. 55 If effectiveness is established, there will be a need for an implementation study, examining how to implement and sustain the intervention when delivered in practice, including when it is delivered by non-psychologists. Finally, evaluating this intervention with health and social care workers in other emotionally charged work contexts may be fruitful.
Strengths and limitations
As far as we are aware, this is the first study to examine the use of Acceptance and Commitment Therapy to promote palliative care staff wellbeing. As a feasibility study, it was underpowered to detect statistically significant differences in quantitative outcomes. Yet, the use of mixed methods was a strength, and qualitative data provided strong evidence for acceptability and preliminary evidence of potential impact. As this was a pre-post study, we did not have a control condition, so we do not yet know how feasible it will be to recruit and evaluate participants for an RCT. As this study was funded by a small research grant, intervention fidelity was not independently assessed, and this is recommended in future studies. We collected data at four time-points, but under half completed quantitative measures at follow-up. This may have been due to participant burden as they had been asked to complete questionnaires and participate in a focus group, at a time when COVID-19 was still heavily impacting staffing. In future studies, identifying strategies to ensure data collection at follow-up will be essential.
Conclusion
An online Acceptance and Commitment Therapy intervention to improve palliative care staff wellbeing was acceptable, with preliminary evidence that participation may improve psychological flexibility and wellbeing. Mixed method evaluation was useful in identifying areas for improvement in the structure of the intervention and considerations for future efficacy studies. The data presented here suggest that such studies are worth pursuing.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221143817 – Supplemental material for Feasibility of RESTORE: An online Acceptance and Commitment Therapy intervention to improve palliative care staff wellbeing
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221143817 for Feasibility of RESTORE: An online Acceptance and Commitment Therapy intervention to improve palliative care staff wellbeing by Anne M Finucane, Nicholas J Hulbert-Williams, Brooke Swash, Juliet A Spiller, Brigid Wright, Libby Milton and David Gillanders in Palliative Medicine
Footnotes
Acknowledgements
We are very grateful to Julie Pearce, Chief Nurse Executive Director of Quality & Caring at Marie Curie for support and advice on intervention design and participant recruitment at the early stages of this project. We also thank Jean Lugton, research volunteer at Marie Curie Hospice Edinburgh, for proof-reading and commenting on the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AFs research fellowship is funded by Marie Curie. JS, LM and BL are employed by Marie Curie.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by a Marie Curie small grant (£9804) to AF and DG (7.02.20), and a small grant from the University of Edinburgh (£2177) to support the design and production of the RESTORE workbook (22.03.2).
Data available statement
Given the potential for identification of study participants, full transcripts from qualitative interviews are not available – though further detail can be provided on request. The original protocol for this study had been referenced in this article and is available online. Requests for quantitative data access should be addressed to the corresponding author (AF) and will be reviewed and responded to.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.