
Abstract
Background:
Age-related complex medical conditions have been commonly reported among adolescents and young adults with advanced life-limiting illness. There is increasing interest in exploring their palliative care needs and end-of-life experiences.
Aim:
This scoping review aimed to explore the available literature about providing palliative and end-of-life care to adolescents and young adults with advanced life-limiting illnesses.
Design:
Scoping review. This review was registered on Open Science Framework (https://doi.org/10.17605/OSF.IO/SPTD7).
Data sources:
Electronic databases (MEDLINEALL, Embase, Emcare, Cochrane Central Register of Controlled Trial CENTRAL, Scopus, PsycINFO, Cochrane Database of Systematic Reviews), Google Scholar and reference lists were searched up to October 2021. We included studies reporting on adolescents and/or young adults with advanced life-limiting illnesses. There were no limitations concerning location, type of illness or study design.
Results:
We identified 51 studies published between 2002 and 2021. Most studies were published in the United States (n = 34, 67%), and nine studies (18%) reported exclusively on patients with non-malignant illnesses. Two thirds of the identified studies were case reports and retrospective chart reviews (n = 33). Three main topics were identified: Physical symptom burden (n = 26, 51%), Psychological and social needs (n = 33, 65%), and end-of-life care (n = 30, 59%). Twenty-six studies (51%) were focused only on one topic, and the age range used to identify adolescents and young adults varied based on the study location.
Conclusion:
The findings of this review shed light on the different palliative care experiences and knowledge gaps related to adolescents and young adults as an underserved and vulnerable patient population. Further research needs to be dedicated toward palliative care programs tailored for adolescents and young adults.
Palliative care integration is associated with better quality of life and improved end-of-life care
Clinical guidelines recommend the early integration of palliative care to standard medical care.
The availability of palliative care support designed for adolescents and young adults is still limited.
Complex symptom management burden, and high psycho-social needs are characteristic for adolescents and young adults with advanced life-limiting illness.
Many adolescents and young adults with advanced disease have late or no access to palliative care consults before end of life
High-intensity medical care at the end-of-life is more common among adolescents and young adults with hematological malignancies, and results in poor quality of end-of-life care.
There is a lack of global collaboration to support the palliative care needs of adolescents and young adults with advanced disease
Research on how to improve adolescents and young adults’ access to palliative care services is urgently needed.
Introduction
Patients with life-limiting illnesses face many challenges due to the physical burden of their illness, treatment side effects, and the social and psychological burden of living with their disease. 1 Palliative care, as defined by the World Health Organization (WHO), is an approach that aims to improve the quality of life of patients and their caregivers. 2 It aims to support patients with life limiting illnesses,3,4 by providing physical, functional, spiritual, and psychosocial support.5,6 Randomized controlled trials and meta-analyses in adults have demonstrated that early palliative care integration leads to better quality of life, lower acute health care utilization, and improved advance care planning.7,8
Adolescents and young adults have unique medical, psychological, social, and supportive care needs that differ from those of children and older adults.9,10 Within palliative care, there is no consistent international age range defined for adolescent and young adults. In North America, the age range is defined as being from 15 to 39 years old. 11 There are different causes of disease-related mortality among this age group, but cancer remains the most common,12–14 with increasing annual incidence since 1992.14,15 Other life-limiting diseases that occur in the adolescent and young adult age group include cardiac diseases, liver cirrhosis, cerebrovascular diseases, and human immunodeficiency virus (HIV). 14
Despite clinical guidelines and recommendations for early palliative care referrals, 16 the integration of age-designated palliative care programs, provided by medical teams with special training in palliative care for adolescents and young adults, remains limited. 17 Research on the palliative care needs of adolescent and young adults is also still developing, with scarce available data.
Scoping reviews, as a structured evidence synthesis process, serve to identify the scope of the literature on a certain topic, rather than to produce a synthesized answer to a specific question. 18 Our scoping review aimed to explore the current data relevant to the palliative and end-of-life care of adolescents and young adults diagnosed with advanced and life-limiting illnesses. The primary objective was to delineate the existing knowledge regarding palliative and end-of-life care for adolescents and young adults. The secondary objectives were to identify the different age ranges used to define adolescents and young adults as described in the relevant studies, and to explore the level and timing of palliative care integration for adolescents and young adults through examining referral patterns to palliative care.
Our aim was to describe the extent and nature of research on this topic, in order to better understand the specific palliative care needs of adolescents and young adults, improve palliative care service provided to this population, highlight any gaps in the literature, and identify opportunities for future research.
Methods
Summary
The protocol for this review was previously registered on Open Science Framework (https://doi.org/10.17605/OSF.IO/SPTD7).
This review used the five-stage method previously outlined by Arksey and O’Malley, 19 with recommendations proposed by Levac et al. 20 First, the research questions were defined and stated as objectives. Second, relevant studies were identified through a comprehensive search of electronic databases. Third, appropriate studies were selected from the search results. Fourth, the data were charted to describe the basic parameters of selected studies. Fifth, data were synthesized through summarizing the results.
Research questions
The primary research question framing this scoping review was: what are the palliative and end-of-life care needs and experiences of adolescents and young adults with advanced life-limiting illnesses? The secondary research questions were: What are the age ranges used to identify adolescents and young adults? What are the referral practices to palliative care related to adolescents and young adults, with respect to referral frequency and timing?
Search strategy
In collaboration with the University Health Network information specialist at Princess Margaret Cancer Centre, an extensive literature search was conducted from the databases’ inception to 21st October 2021, in Medline ALL (Medline and Medline Epub Ahead of print and In-Process & Other Non-Indexed Citations), Embase, Emcare, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, and PsycInfo all from the OvidSP platform, and Scopus from Elsevier.
Search terms included “pain management,” “symptom management,” “symptom prevalence,” “psychosocial needs,” “hospice,” “end-of-life,” and “palliative care.” Where available, both controlled vocabulary terms and text words were used. Where applicable, the search was restricted to the English language, human studies, adolescents and “young adults and adults” based on each database indexed age group. The indexed age group was from 13 to 44 years for Medline, and 13 to 64 years for Embase, Emcare, and PsycInfo. (Supplemental Appendix- Medline ALL search).
Google Scholar and reference lists from included scoping and systematic review studies were searched by the research team to identify additional relevant studies.
Study eligibility criteria
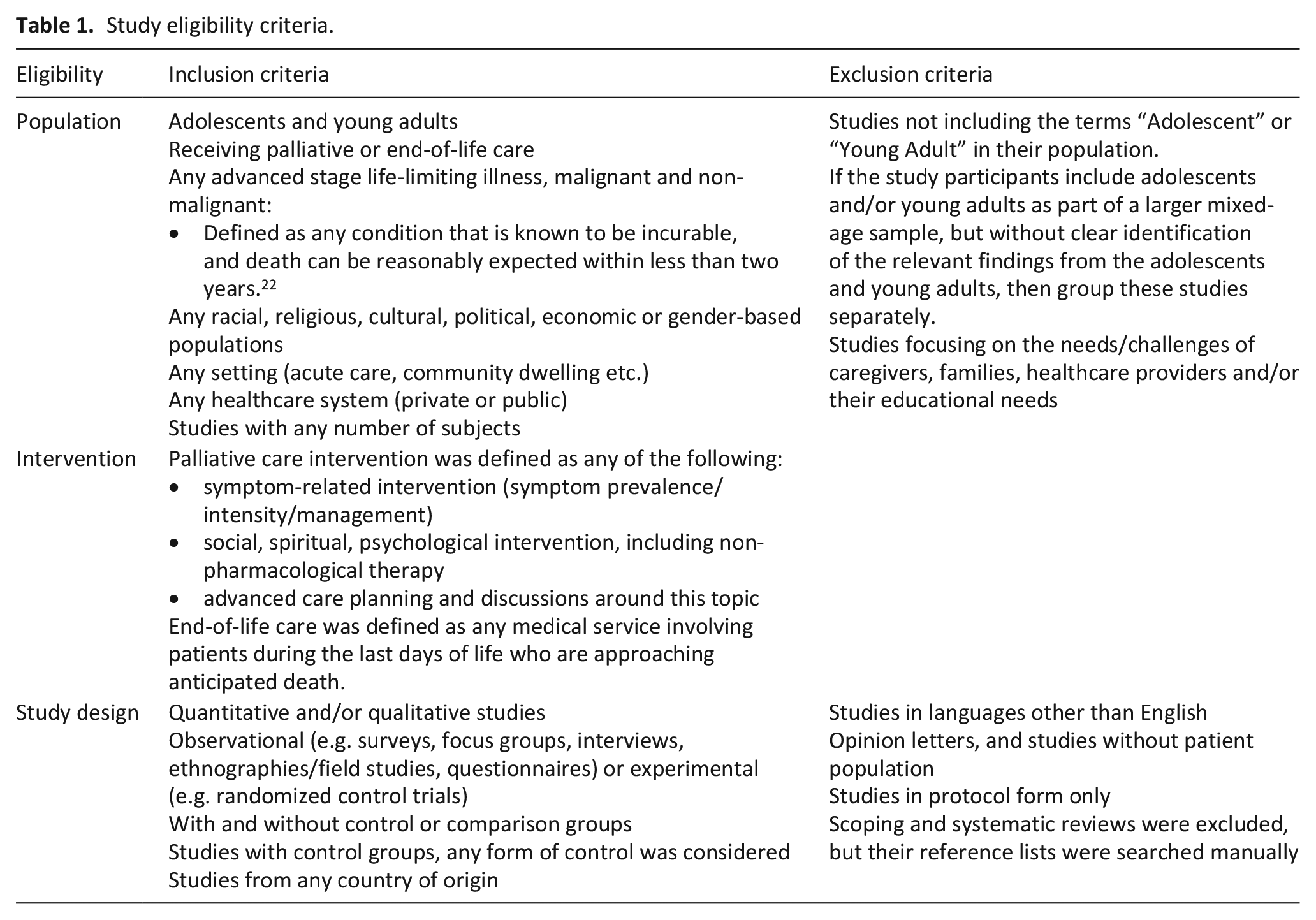
The inclusion and exclusion criteria for this review (Table 1) followed the Joanna Briggs Institute Reviewers’ Manual for scoping review methodology. 21 We included studies that reported on adolescents and young adults who were receiving palliative or end-of-life care for any advanced life-limiting illness, 22 including cancer and end stage organ failure. As the definition of the age range of adolescents and young adults varies among countries, only studies addressing the terms “Adolescent” and/or “Young Adult,” regardless of the age range, were included. There were no limitations related to study location, design, or sample size. Studies were excluded if adolescents and young adults were not specifically identified within the study participants or if the focus was on the needs of caregivers, families, or healthcare professionals rather than on patients themselves.
Study eligibility criteria.
Articles were independently reviewed in-duplicate by two of four reviewers (MA, JA, RC, NS), during Level 1 title & abstract and Level 2 full text screening. A calibration exercise of 20 articles was conducted before each screening level to ensure sufficient agreement (at least 80%) between the investigators. Disagreements were resolved by discussion and subsequent consensus of the two reviewers. If consensus was not reached, a third investigator (AA) was involved to determine whether the study met the criteria for inclusion.
Data extraction and synthesis
Data extraction was performed in duplicate by two of four reviewers (MA, JA, RC, NS), with a third investigator (AA) involved to settle any disagreements. Data from each included study was documented using standardized forms, created and approved by all reviewers. The extracted data included: first author, year of publication, study type and design, study population, sample size and the age range used, type of the advanced illness, palliative care referral patterns (if available), and key findings. Data synthesis, including identifying key findings domains, and highlighting the gaps in knowledge, was completed by the reviewers. The final results are presented as tables and detailed descriptions.
Results
A total of 66,425 records were identified through searching the electronic databases, grey literature, and manually searching the references including the relevant scoping and systematic reviews (Figure 1: PRISMA diagram). No relevant abstracts were identified in the grey literature. After removal of duplicates, 34,938 abstracts were screened, and 144 full articles were assessed for eligibility. Ultimately, 51 studies, including 57,116 patients from the adolescent and young adult age group, were included.
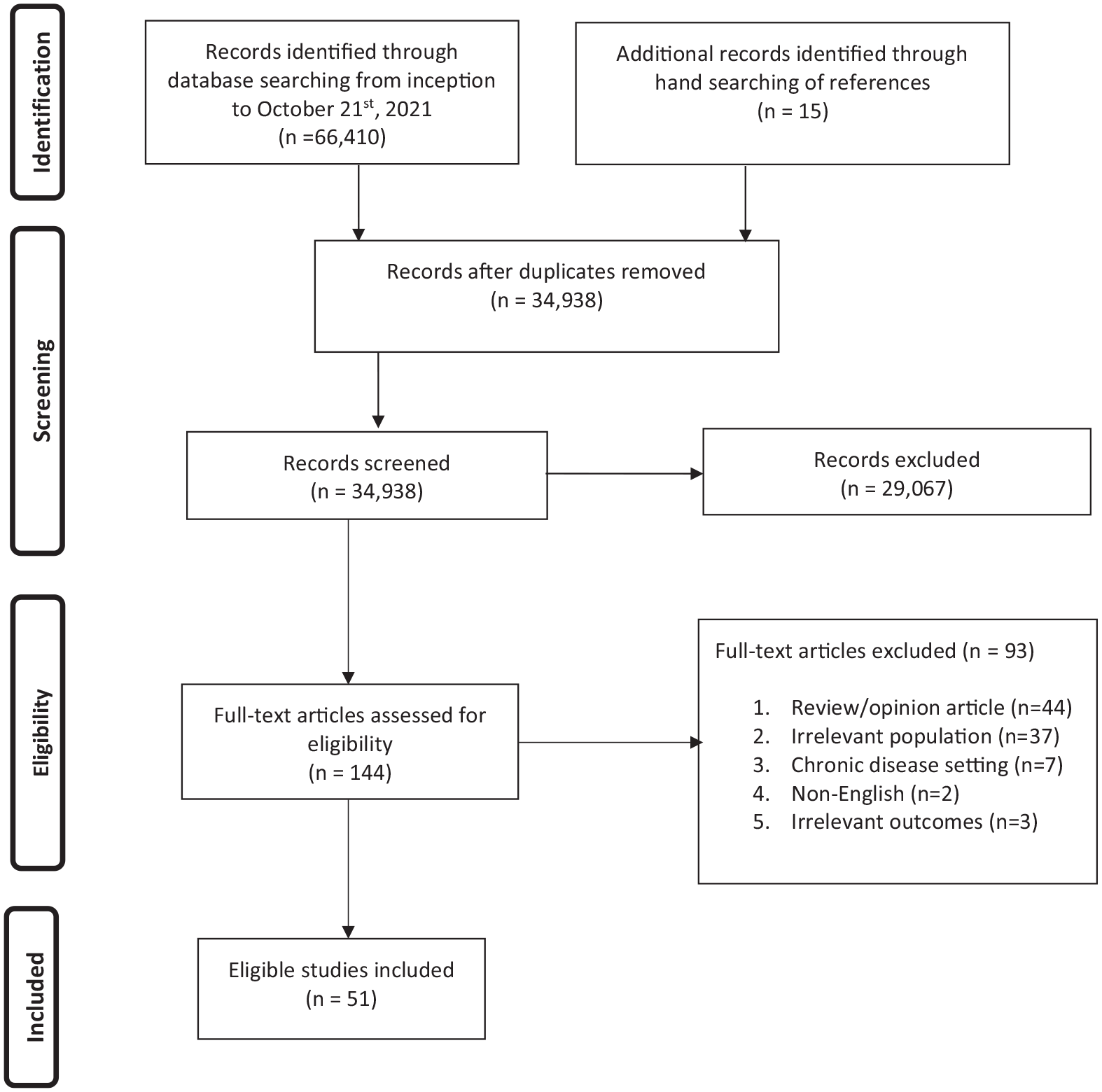
PRISMA flow diagram.
The general characteristics of these studies are summarized in Table 2. Most of the studies were published in the US (n = 34, 67%), and we were unable to identify any relevant studies published before 2002. The majority were quantitative studies (n = 24, 47%), or case reports (n = 15, 29%). Most reported exclusively on adolescents and young adults (n = 44, 86%) and included exclusively patients with cancer (n = 42, 82%). However, four studies included only patients with non-malignant advanced illnesses (HIV/AIDS in three,23–25 and cystic fibrosis in one 26 ). Five studies included patients with both malignant and non-malignant advanced illnesses.27–31
General characteristics.
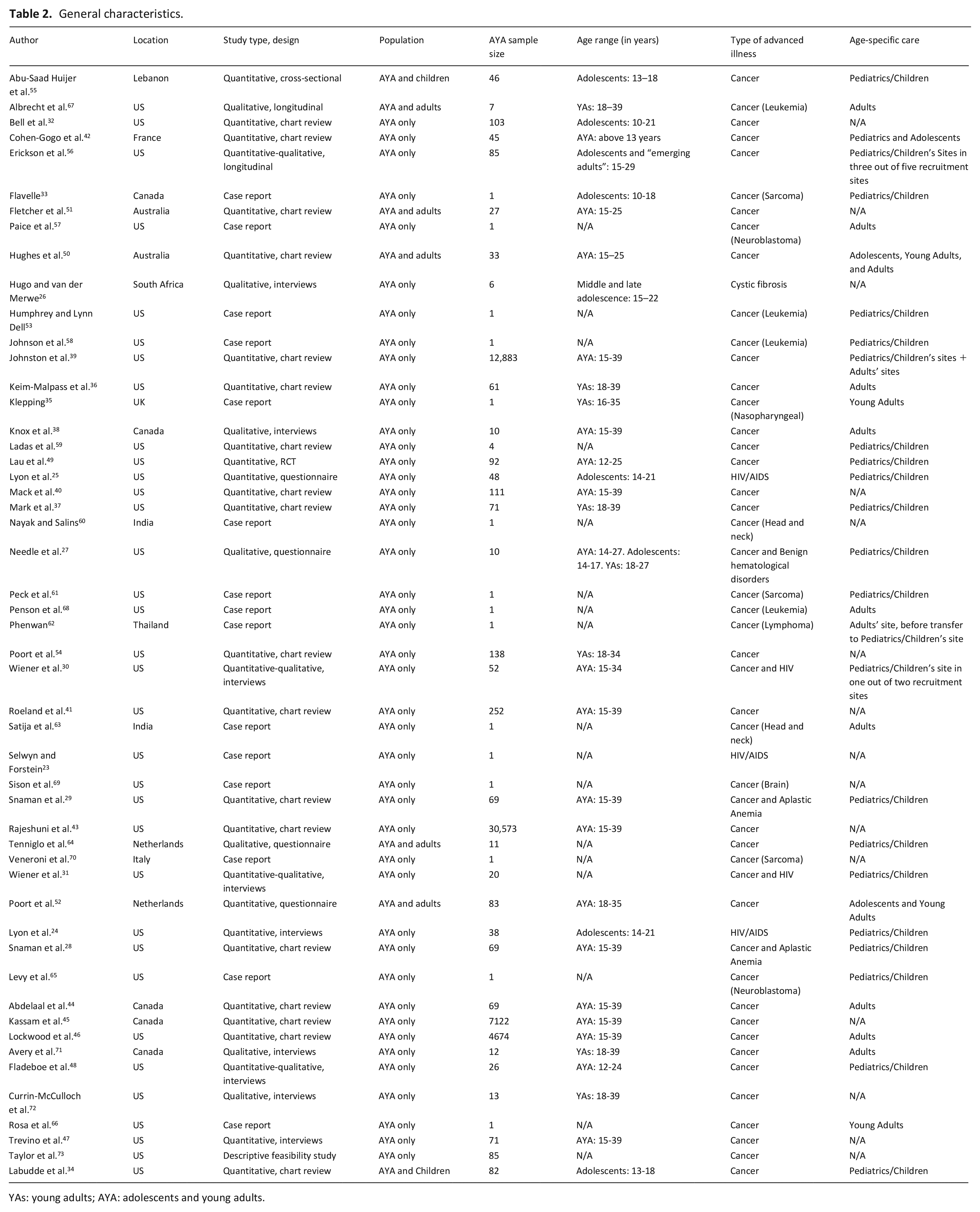
YAs: young adults; AYA: adolescents and young adults.
Definition of age range
An age range was not defined in 17 studies (33%). In the remaining 34 studies, 19 different age ranges were defined: six for adolescents; four for young adults; and nine different age ranges for the studies that included adolescents and young adults.
The age used to define adolescents ranged from 10 to 22 years26,32–34;the age used to define young adults ranged from 16 to 39 years35–37; and the age used to define adolescents and young adults ranged from 13 to 39 years.38–42Most studies originating from Canada and the US used the age range of 15–39 years old28,29,38–41,43–47; however, other age ranges were also reported in US studies, including 12–24, 48 12–25, 49 14–27, 27 and 15–34. 30 Two studies published in Australia used a range of 15–25 years,50,51 a study from the Netherlands used 18–35, 52 and a study from France defined only a lower limit of 13 years. 42
Race/Ethnicity
The correlation between race/ethnicity and palliative and end-of-life care was documented in seven studies.24,34,39,41,43,47,49 Patients of white race stated higher social support, 47 were more likely to receive palliative care, 41 and less likely to die in a hospital. 43 African-American patients expressed higher interest to continue active treatments even if their physical ability was to decline. 24 Patients of Hispanic ethnicity were more likely to die in a hospital, 43 and had higher hospital bed utilization in the last year of life, compared to non-Hispanic ethnicity. 39 The use of a resilience promoting intervention had a higher response in finding benefit among non-white patients, compared to white patients. 49 In one study, there was no difference in the number of palliative care opportunities across racial and ethnic groups. 34
Palliative care referral practices
Twelve studies contained information on referral practices to palliative care among adolescents and young adults.28,29,34,36,37,41,44–46,51,53,54 The time between palliative care referral and death was reported in five studies,34,36,37,44,51 with the mean time ranging from 12.8 days 36 to 94.4 days, 51 and a median time of 53 days, 51 62 days, 34 5 months, 44 and 318 days. 37 One study reported the median time between cancer diagnosis and palliative care referral was 144 days among hematological malignancies, and 458 days among patients with neurological malignancies. 46 Palliative care referral during the last month of life varied between 7% of the adolescents and young adults in one study, 37 17% in another, 54 and 68% of the patients who received a stem cell transplant (compared to 77% in patients who did not receive a stem cell transplant). 29 One study reported that 18% of adolescents and young adults had palliative care referral during the last day of life, 36 whereas in another up to 43% of patients had no palliative care involvement. 54 Patients with hematological malignancies were less likely to receive referral to palliative care or hospice.36,41,45
Domains of palliative care needs and experiences
After analyzing the key findings of the 51 studies, three domains were identified related to the palliative care needs and experiences of adolescents and young adults: physical symptom burden (n = 26, 51%),26,28,29,32–35,40,42,44,46,50,52,53,55–66 psychological and social needs (n = 33, 65%),26,28,29,31–33,35,38,40,42,44,46–50,53,55,57,58,60–64,66–73 and end-of-life care (n = 30, 59%).23–25,27–32,34–37,39–45,51,53,54,58,60,62,65,66,68 The three domains were all presented in 13 articles (25%). Twelve articles (24%) discussed two domains, and 26 articles (51%) focused on one domain only.
Physical symptom burden
This domain was presented in 26 articles, and can be further divided into symptom incidence, severity, and management (Table 3). Most articles (n = 15/26, 58%) discussed at least two of these topics, and all three topics were presented in three articles.55,62,63 In eight articles, only one topic was presented (Symptom incidence: n = 7,26,33,34,40,46,52,56 management: n = 1 32 ).
Physical symptom burden.
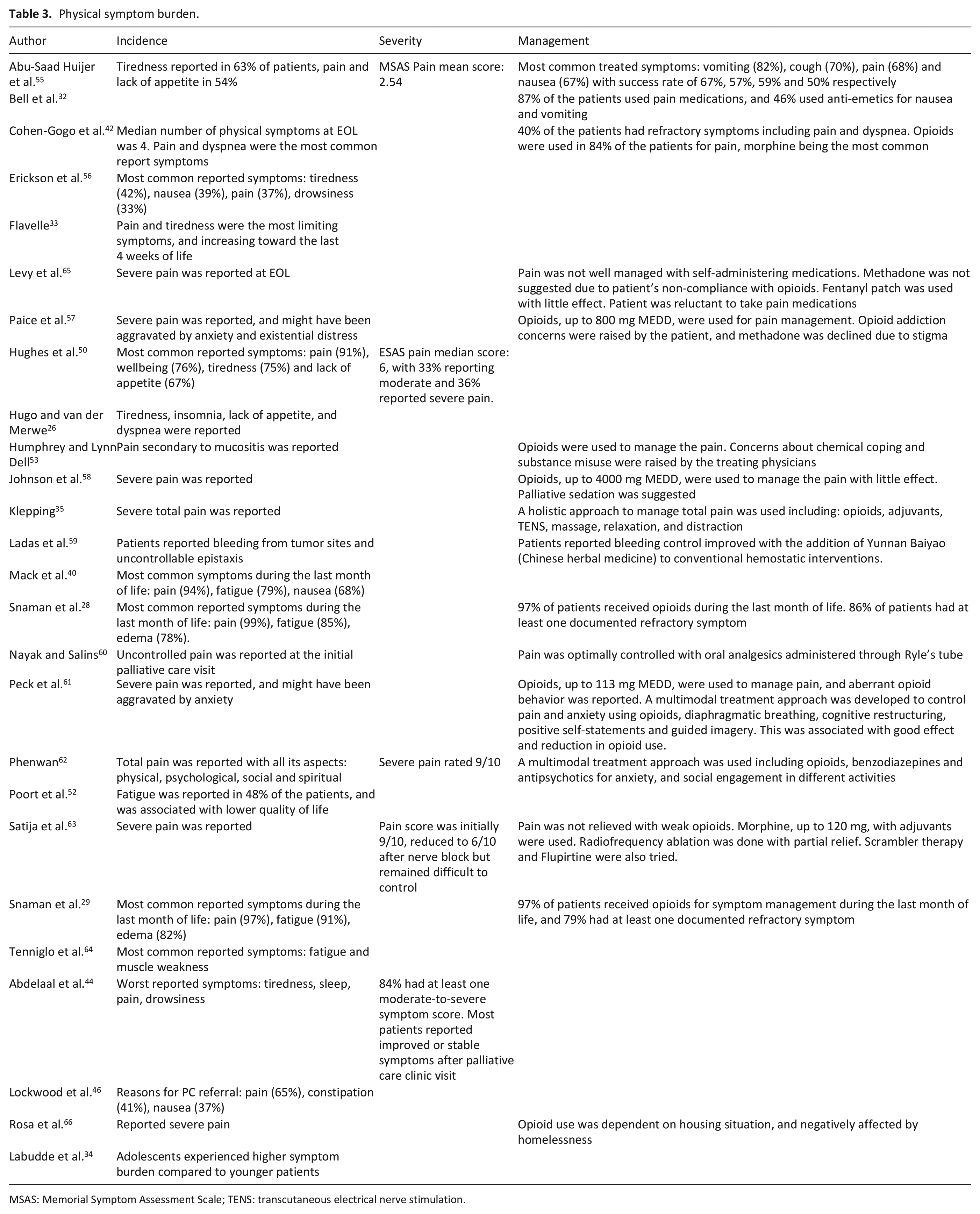
MSAS: Memorial Symptom Assessment Scale; TENS: transcutaneous electrical nerve stimulation.
Twenty five studies elaborated on the incidence of symptom among adolescents and young adults, whether during the illness trajectory or at end of life. The most prevalent symptoms were pain and tiredness.29,40,50,55,56 Pain was reported among 37%–91%46,50,56 of adolescents and young adults, and the incidence increased up to 99% of the patients during the last month of life. 28 Similarly, tiredness was reported by 42%–75%50,52,56 of the patients, and increasing to 91% at end of life, with lower quality of life.29,52
Although the level of symptom severity was not regularly described in the reviewed studies, many case reports described severe pain in adolescents and young adults,57,58,63 rated at 9 out of 10 in different studies.62,63 Various techniques for symptom management were explained in some studies. However, optimal pain control was rare despite using high opioid doses,57,61,63 up to 4000 mg of morphine equivalent daily dose (MEDD). 58 Concerns around opioid addiction, substance misuse and chemical coping were reported in two case reports.53,57
Total pain was described in three case reports35,61,62 where physical pain was aggravated by anxiety, or social distress. The use of benzodiazepines and antipsychotics, in addition to non-pharmacological interventions such as breathing techniques, were used to manage the pain in patients where opioids alone were not successful.35,61,62
Psychological and social needs
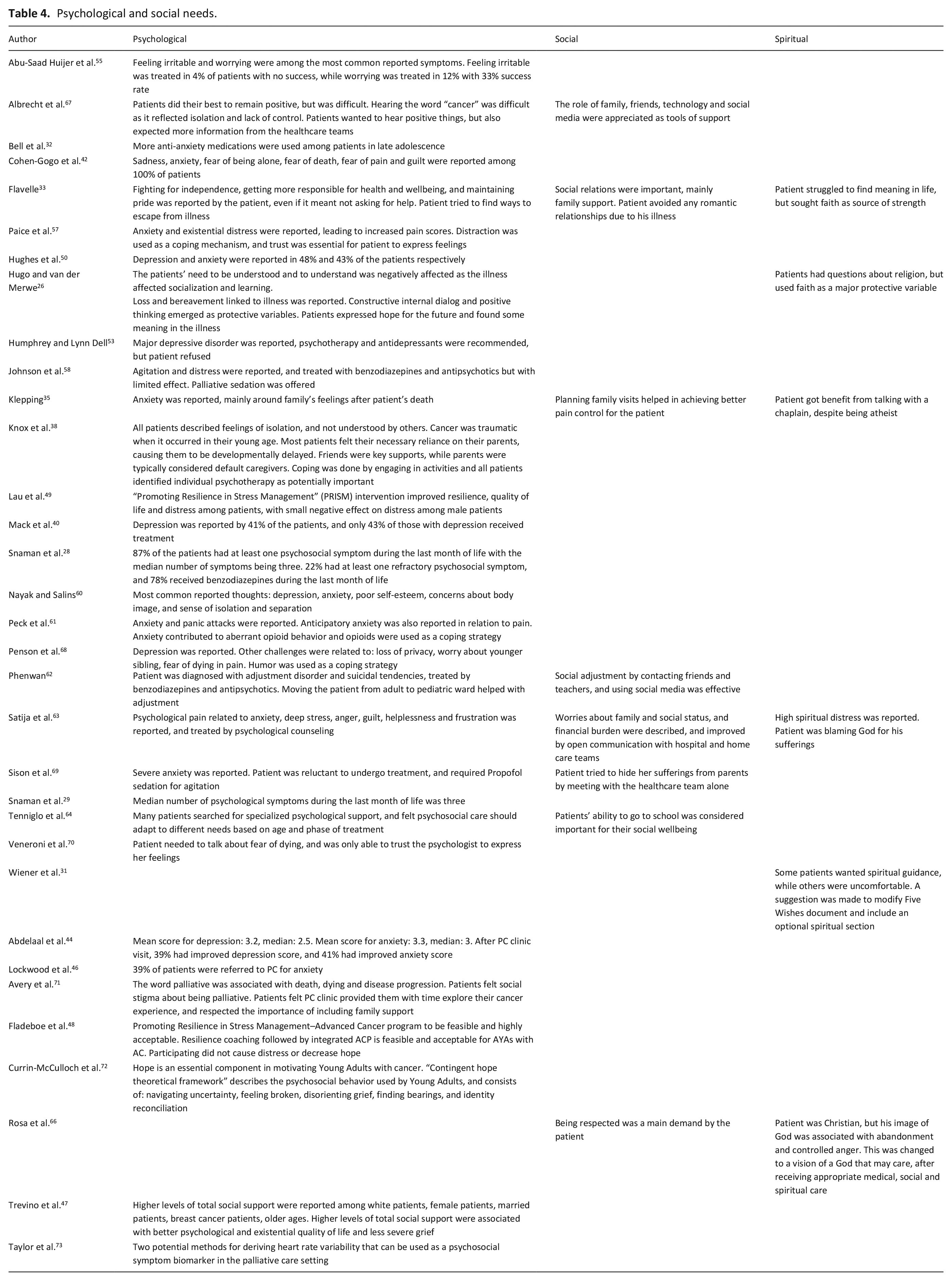
Table 4 summarizes the 33 studies exploring the psychological and social needs for adolescents and young adults. Themes related to psychological symptom burden and adjustment disorders were discussed in 31 studies.26,28,29,32,33,35,38,40,42,44,46–50,53,55,57,58,60–64,67–73 During the last month of life, up to 87% of patients had at least one psychological symptom. 28 Depression and anxiety were repeatedly reported by adolescents and young adults,35,40,53,60,69 in up to 43% and 48% of patients, respectively. 50 The use of benzodiazepines was common, especially toward end of life.28,58,62 However, in the majority of cases, these psychological symptoms were either untreated,40,53,55 or refractory to treatment.28,55
Psychological and social needs.
SDM: substitute decision maker; DNR: do not resuscitate.
Emotional distress was another psychological challenge faced by the patients, and demonstrated in common terms such as “feeling isolated,” “loss of privacy,” and “fear of dying.”38,42,60,67 Patients in these studies used a variety of coping mechanisms including humor and engagement in different activities, such as with peer support groups.38,57,68
Additionally, the importance of social engagement with friends, and the role of family support constituted important coping tools for adolescents and young adults.33,35,62,67 The value of technology and social media was demonstrated as an effective way of keeping patients connected with their peers.62,67 On the other hand, adolescents and young adults in some studies preferred to hide their emotional distress from their parents,69,70 and avoided engaging in personal or romantic relationships during their illness. 33
Spirituality and spiritual needs were explored in six studies.26,31,33,35,63,66 Some adolescents and young adults used their faith as a coping mechanism, despite their struggle to find meaning in life.26,33 However, other patients did not feel comfortable answering questions pertaining to their religious or spiritual beliefs. 31
End-of-life care
Components of advance care discussions and end-of-life care for adolescents and young adults were presented in 30 articles (Table 5). Code status decisions were discussed in 12 articles.25,28,29,34,36,37,40,41,44,51,54,58 While the majority of adolescents and young adults had “Do not Resuscitate” orders confirmed before death,29,36 the median time between this decision and time of death of some patients was as short as two days. 28 A range of 1%–21% of adolescents and young adults had resuscitation attempted before death.29,36,37,44,51 Patients who received hematopoietic cell transplant, or those who were not followed by a palliative care team, were more likely to have resuscitation attempts at the end of life.28,29 In one study, 36%–44% of patients had either late or no discussions around code status, and 40% had no documented discussions around their goals of care. 54
End-of-life care.
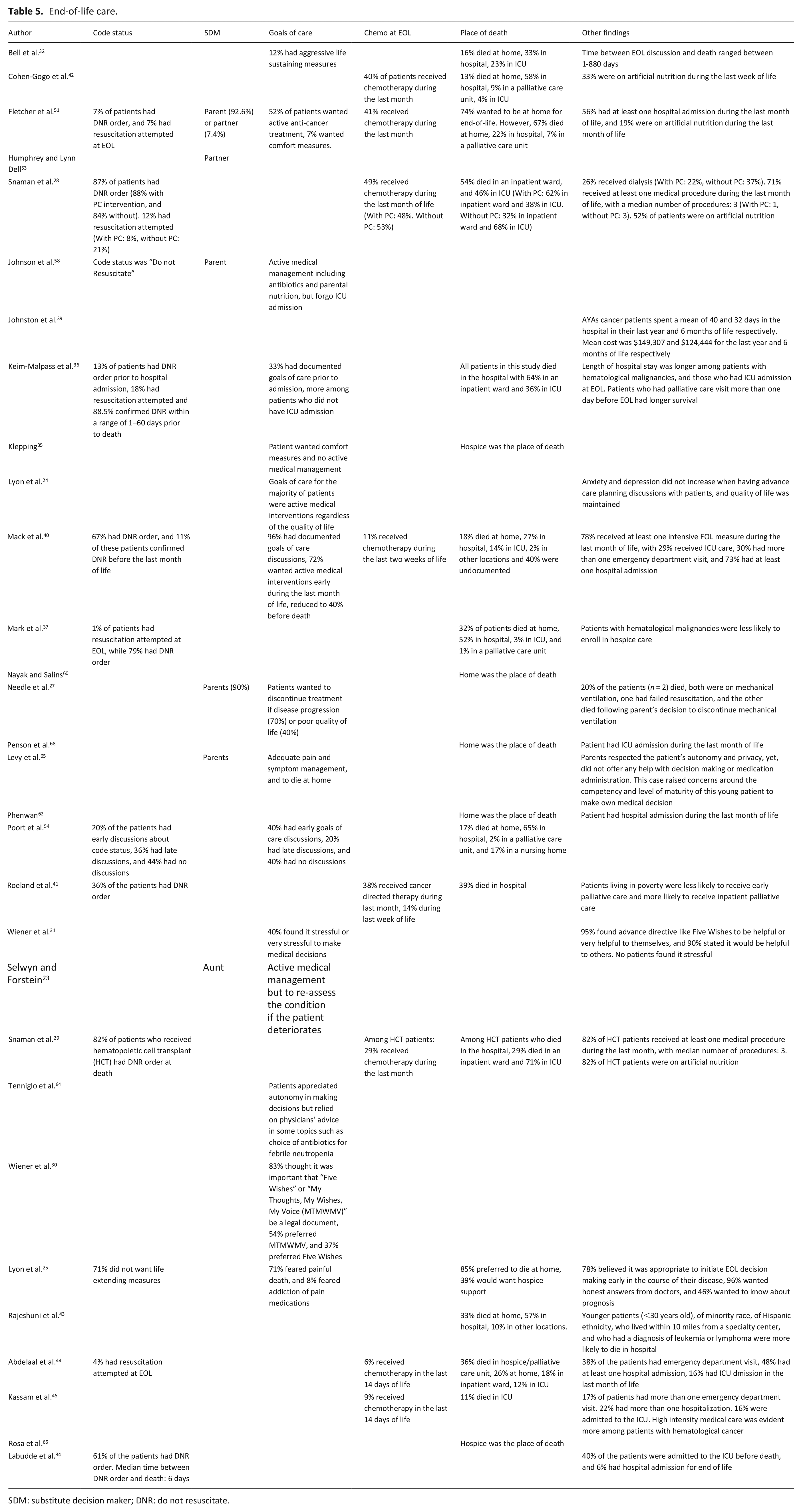
Moreover, some studies showed that the patients’ goals of care were mostly centered around active medical management,23,24,40,51,58 reaching up to 72% of the patients during the last month of life. 40 However, many patients voiced their preference to discontinue treatment and pursue a comfort based medical approach if their prognosis was limited and before death.27,40 Generally, adolescents and young adults felt early discussions around goals of care and end of life were appropriate, helpful and did not affect their quality of life.24,25,31
Despite favoring to make treatment decisions, many adolescents and young adults found it stressful, 31 and preferred to follow the medical teams’ advice. 64 Additionally, opioid use was concerning to some patients, with fears of addiction. 25 The choice of a substitute decision maker was another topic presented in six articles,23,27,31,51,53,58 and up to 93% of patients preferred to have their parents as their decision makers. 51
More than one-third of adolescents and young adults received chemotherapy during the last month,41,42,51 and up to 14% during the last week of life. 41 Similarly, more than 70% of patients received at least one medical intervention during the last month.28,29,40 In one study, 33% of the adolescents and young adults received artificial nutrition during the last week of life. 42
Up to 85% of patients expressed a wish to die at home.25,65 However, inpatient hospital units were the most common place of death, ranging between 22% and 65% of patients.37,40,51,54 Patients with hematological malignancies, who received hematopoietic cell transplant, or who did not have palliative care involvement, were more likely to die in intensive care units (ICU).28,29,32,36
Discussion
This scoping review identified 51 studies that addressed different aspects of palliative and end-of-life care for adolescents and young adults with advanced illness. Most of the studies (n = 45, 88%) were published within the last 10 years, and 67% originated from the US. More than two-thirds of the studies were retrospective chart reviews and case reports. These findings highlight the need for age-specific prospective studies that relate to adolescents and young adults, particularly in countries outside the US and for patients with non-malignant conditions.
Age range
The age range used for adolescents and/or young adults was not identified in one third of studies. In the remaining studies, the age used to identify adolescents and young adults varied, with an interval from 10 to 39 years old among all the studies. However, this range was widely variable across the studies, and differed according to the country of origin, with North American studies tending to use the interval of 15 39 years,28,29,38–41,43–47 and studies originating in Australia tending to use the interval of 15–25 years.50,51 Indeed, definitions of the adolescent and young adult age group vary internationally, with the United States using a wider age range of 15 to 39 years, the UK uses 13–24 years, and Australia uses 15–25 years. 11 Even within countries, the definition can vary; for example, the National Cancer Institute (NCI) in the United States used the age range of 15–29 years for clinical epidemiology purposes, but favored 15–39 years as a broader range for adolescent and young adult oncology. 11 The differences in the age definition of adolescents and/or young adults across the literature creates discrepancies in identifying palliative and end-of-life experiences of this age group. These findings reflect the importance of defining a global age range for adolescents and young adults with advanced disease, in order to better understand their needs, and to more easily compare and improve the quality of palliative care programs for the adolescent and young adult population internationally.
Complex symptom burden
Symptom control is one of palliative care’s main goals, which aims to improve quality of life.74,75 Adolescents and young adults with advanced illness face high symptom burden, with complex physical and psychological needs.76–78 This complexity is sometimes referred to as total pain, that can be refractory to high opioid doses. 57 Adequate total pain management requires a multimodal approach including pharmacological and non-pharmacological interventions, as well as social and spiritual support.35,62
In addition, adolescents and young adults may express high levels of psychological and social distress, related to their stage of cognitive development, as well as a desire to preserve their privacy, along with worries about body image and financial burden.79,80 The majority of patients included in our review reported multiple psychosocial symptoms, and more than 20% were refractory to treatment. 28 Tenniglo et al. highlighted the demand for specialized psychosocial care for adolescents and young adults, that needs to be compatible with the different needs of the adolescent and young adult age group. 64
Quality of end-of-life care
Some studies in our scoping review observed longer hospital admissions, less palliative care involvement and higher rates of ICU deaths among adolescents and young adults with hematological malignancies.32,36,37,45 Other factors related to the poor quality of end-of-life care included late palliative care referral, receiving a hematopoietic cell transplant, and patients’ financial status.29,36,41
People with cancer within the adolescent and young adult age group had high hospital bed utilization during the last 6 and 12 months of life, with a mean hospital stay of 32 and 40 days respectively. 39 This was associated with high medical expenses and cost more than $120,000 per patient. 39 Earle et al. and colleagues defined criteria for aggressive end-of-life care, which involved the number of admissions to emergency rooms, intensive care units and inpatient hospital wards during the last month, as well as the use of intravenous chemotherapy during the last 2 weeks of life.81,82 Based on these criteria, adolescents and young adults tend to have a high incidence of receiving aggressive care at the end of life, resulting in poor quality of end-of-life care.37,39
Advance care planning
Studies in our scoping review that examined the opinions and preferences toward advance care planning showed that the majority of adolescents and young adults encouraged these discussions, and preferred their early introduction.25,31 There are different age-specific documents, created to help adolescents and young adults plan for their future medical needs, such as “Five Wishes,” “My Thoughts, My Wishes, My Voice,” and “Voicing My Wishes.”30,31 Further adaptation of these documents to match adolescents and young adults’ needs, together with introduction of advance care planning discussions early in the diagnosis and during treatment planning, can help in better understanding these patients’ needs, and improving the quality of their medical care.
Strengths and limitations
To our knowledge, this is the first scoping review to report on the palliative care needs of adolescents and young adults with advanced illnesses, as a distinct age group. We conducted an extensive search of multiple bibliographic databases from inception to October 21, 2021. We also searched through the grey literature and identified studies through hand search of the references. Our inclusion criteria were inclusive to all study designs and types of advanced illnesses, which helped to capture the broad spectrum of evidence within the available literature.
However, our review has limitations. Due to the inconsistent definition of the adolescents and young adults age range across different healthcare systems, we only focused on the studies that specifically addressed adolescents and/or young adults. Further, our search excluded non-English language studies, and would not have included some of the studies that discussed palliative care components, but were not indexed as “palliative care.” Some of the findings in this review were obtained from case reports, and need further evidence to be generalized among the adolescent and young adult population.
Conclusion
This scoping review provides an overview of the available literature related to the unique palliative and end-of-life care needs of adolescents and young adults with advanced illness. The reviewed literature paints a clear picture of disparity for this vulnerable and underserviced population as it relates to their high distress levels, unmet needs and poor quality of end of life care. Our findings show that adolescents and young adults are more likely to experience severe refractory symptoms, and receive intensive medical measures at end of life. Despite the concerns raised by these patients’ families, they are interested in engaging in age-appropriate advance care planning discussions. As such, there is a need for designated palliative care teams, with special age-focused training, to address this population’s complex needs. More prospective research centered around adolescents and young adults is needed, to ensure the provision of high-quality medical care to this age group.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221136160 – Supplemental material for Palliative care for adolescents and young adults with advanced illness: A scoping review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221136160 for Palliative care for adolescents and young adults with advanced illness: A scoping review by Mohamed Abdelaal, Jonathan Avery, Ronald Chow, Nasreen Saleem, Rouhi Fazelzad, Pamela Mosher, Breffni Hannon, Camilla Zimmermann and Ahmed al-Awamer in Palliative Medicine
Footnotes
Authorship
The study design was conducted by MA, AA, JA, PM, and RF. Search strategy and data search were performed by RF. Records screening and data extraction were completed by MA, JA, RC, NS, and AA. MA drafted the manuscript, before being revised by JA, PM, RC, NS, RF, BH, CZ, and AA. All authors approved the final version and are accountable for all aspects of this review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.