
Abstract
Background:
Heart failure has high mortality and is linked to substantial burden for patients, carers and health care systems. Patients with chronic heart failure frequently experience recurrent hospitalisations peaking at the end of life, but most prefer to avoid hospital. The drivers of hospitalisations are not well understood.
Aim:
We aimed to synthesise the evidence on factors associated with all-cause and heart failure hospitalisations of patients with advanced chronic heart failure.
Design:
Systematic review of studies quantitatively evaluating factors associated with all-cause or heart failure hospitalisations in adult patients with advanced chronic heart failure.
Data sources:
Five electronic databases were searched from inception to September 2020. Additionally, searches for grey literature, citation searching and hand-searching were performed. We assessed the quality of individual studies using the QualSyst tool. Strength of evidence was determined weighing number, quality and consistency of studies. Findings are reported narratively as pooling was not deemed feasible.
Results:
In 54 articles, 68 individual, illness-level, service-level and environmental factors were identified. We found high/moderate strength evidence for specialist palliative or hospice care being associated with reduced risk of all-cause and heart failure hospitalisations, respectively. Based on high strength evidence, we further identified black/non-white ethnicity as a risk factor for all-cause hospitalisations.
Conclusion:
Efforts to integrate hospice and specialist palliative services into care may reduce avoidable hospitalisations in advanced heart failure. Inequalities in end-of-life care in terms of race/ethnicity should be addressed. Further research should investigate the causality of the relationships identified here.
Patients with chronic heart failure experience frequent hospitalisations increasing at the end of life.
Hospitalisations of chronically ill patients lead to a disruption of the highly valued continuity of care, burdensome and unnecessary treatments and a significant risk of adverse events.
We found high/medium strength evidence that palliative or hospice care was associated lower risk of hospitalisation for all causes or heart failure.
Our systematic review provided high strength evidence that black/non-white ethnicity is a risk factor for all-cause hospitalisation.
Meaningful evidence could only be gathered for few factors leaving abundant room for further research, especially on personal and psychosocial factors.
Palliative and hospice care initiatives should target patients with advanced chronic heart failure to reduce unnecessary hospitalisations at the end of life.
This research draws attention to the at-risk group of black/non-white populations for hospitalisations in patients with heart failure and thus can raise awareness among health professionals and policy makers to address racial and ethnic minority disadvantages in end-of-life care.
Our findings could inform the development of supportive interventions for high-risk patients and may help service providers and policy makers allocate limited resources.
Background
Chronic heart failure is highly prevalent and a major cause of morbidity and mortality worldwide. 1 Heart failure represents the leading cause of hospitalisation for people over 65 and constitutes the leading disease in terms of health care costs in many countries.2,3 The prognosis for heart failure remains poor. After diagnosis, approximately 50% of the patients die within 5 years4,5 while mortality in advanced heart failure is even higher.
Heart failure patients in their last months of life are often highly symptomatic,6,7 with unpredictable exacerbations of breathlessness that can be particularly challenging to manage in the community. 8 Accordingly, hospitalisations are not only very common in chronic heart failure but peak towards the end of life.9 –11 During the last 6 months of life, as many as 80% of patients with heart failure are hospitalised. 12
Hospital admissions can represent a crisis intervention that results in improved patient-related outcomes.13 –15 However, admissions also provoke a disruption in continuity of care, which is particularly important to patients with chronic conditions.16,17 They may also involve intensive resource use, burdensome treatments, unnecessary interventions and expose patients to a considerable risk of hospital-acquired adverse events.18 –20 International data show that whilst half of the patients who die from heart failure do so in hospital, 21 most patients with terminal heart disease wish to be cared for and die at home or in an inpatient hospice. 22
Given the adverse outcomes of heart failure hospitalisations, guidelines, position papers and end-of-life care strategies all advocate for a reduction in hospital admissions for patients with refractory heart failure.4,23 –26 In order to achieve this goal, it is imperative to first understand the determinants of hospital admissions in heart failure patients. Several studies have examined one or more factors associated with hospital admissions,27 –31 but this body of evidence has never been synthesised. To address this gap, we aimed to systematically identify and synthesise factors associated with hospitalisations in people with advanced chronic heart failure.
Methods
Design and review question
This was a systematic review reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. The review question was: ‘what factors are associated with hospital admissions in patients with chronic heart failure approaching the end of life?’ The primary outcome measure was all-cause hospitalisations and the secondary outcome was heart failure hospitalisations, both assessed as numbers of hospitalisations, rate of hospitalisations, time spent in hospital, or time to first hospitalisation. The review was not registered and the protocol was not published in advance.
Eligibility criteria
We conducted a systematic literature review of studies that reported original data examining at least one factor associated with hospitalisations in patients with a diagnosis of advanced chronic heart failure (including heart failure with reduced left ventricular ejection fraction and heart failure with preserved ejection fraction). Experimental, quasi-experimental, as well as observational study designs were considered for inclusion. Case reports, case series, reviews and qualitative studies were excluded. Unpublished studies (i.e. conference abstracts, dissertations and presentations) were considered if they met the study design criteria.
In order to characterise the target population with advanced chronic heart failure and the associated limited life expectancy as well as possible, we applied complex eligibility criteria.
(a) Marked limitation of physical activity with heart failure symptoms at rest or minimal exertion (NYHA class III or IV)
(b) Stage D according to ACC/AHA guideline (refractory symptoms at rest despite guideline-directed medical treatment or refractory heart failure requiring specialised interventions)
(c) receiving (specialist or generalist) palliative care or hospice care or deemed suitable for these services by the publication’s research team or treating physicians according to their own criteria (e.g. risk assessment by means of the Gold Standards Framework Prognostic Indicator Guidance)
(d) Estimation of a prognosis of less than a year (either by clinical assessment e.g. use of the surprise question or identification as being in their last year of life by retrospective analysis of data 1 year prior to death)
(A) Studies with patients with acute heart failure/decompensation of heart failure or early disease or hospitalised patients not meeting other inclusion criteria than (a)
(B) Studies on patients undergoing or anticipating specialised cardiological interventions or operations (such as mechanical circulatory assist devices, heart transplant, cardiac resynchronisation therapy)
(C) Studies evaluating specific medical interventions or disease-focused interventions (e.g. medication, therapeutic interventions such as pleurocentesis) or operations (e.g. mechanical circulatory assist devices, heart transplant etc.)
(D) Studies specifically excluding patients meeting markers of advanced disease (any inclusion criteria as defined above under (a–d))
(E) Studies with patients in mixed stages of chronic heart failure with less than 75% of patients meeting at least one inclusion criteria under (a–d))
Studies reporting on mixed populations in terms of disease or heart failure stage were included if the results of the subpopulation relevant to our review were reported separately.
For controlled trials, no specific comparator was required. However, to enhance accuracy of our results, we set preconditions for control groups. Studies that did not characterise comparison samples or used undefined matching criteria were excluded. Propensity-matched studies were included if matching criteria of the artificially constructed control group seemed reasonable with respect to eligibility criteria, for example a comparison between patients with chronic heart failure receiving specialist palliative care or standard care, with indications of equivalent disease severity. Before-and-after studies were only considered for analysis if baseline characteristics met eligibility criteria.
Search strategy and study selection process
We searched five electronic databases (MEDLINE, EMBASE, CINAHL, PsycINFO, Cochrane Library) from inception to October 2018 using a combination of title/abstract keywords and MESH-terms (see Supplemental Data). The search was updated in September 2020 resulting in a total search period from inception (Medline 1946, EMBASE 1974, CINAHL 1937, PsycInfo 1806, Cochrane Library 1996) to September 2020. We restricted the search to publications in English, French, Italian, German and Spanish. Additionally, searches for grey literature (opengrey, Dart Europe Etheses), and hand-searching of the references of included papers were performed. Finally, citation searching of included studies on Scopus was done (on April 28th 2021). Ongoing research was looked for using clinicaltrials.gov. Authors were contacted if eligibility criteria matched but reporting lacked essential information for inclusion. Two authors (A.Z. and A.P.) independently screened all titles and abstracts to select eligible studies. Full text was retrieved if any uncertainty about eligibility remained. Disagreements on inclusion between A.Z. and A.P. were resolved through discussions.
Data collection process
For each included study, detailed information was extracted using a standardised data form including first author, year of publication, country of origin, population characteristics, sample size, factors studied, statistical analysis, results, association with primary and secondary outcomes and quality score.
Quality assessment and strength of evidence
Quality of individual studies was assessed using the validated Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields (QualSyst) tool, which has been used effectively in similar systematic reviews evaluating factors associated with health care use.32 –34 Double quality assessment was performed by a second author on a randomly selected subsample of 10% of all articles (six articles). Interrater agreement was high ranging between 81% and 95% (mean 89%, SD 0.05%), so a double quality assessment of all articles was not considered necessary.
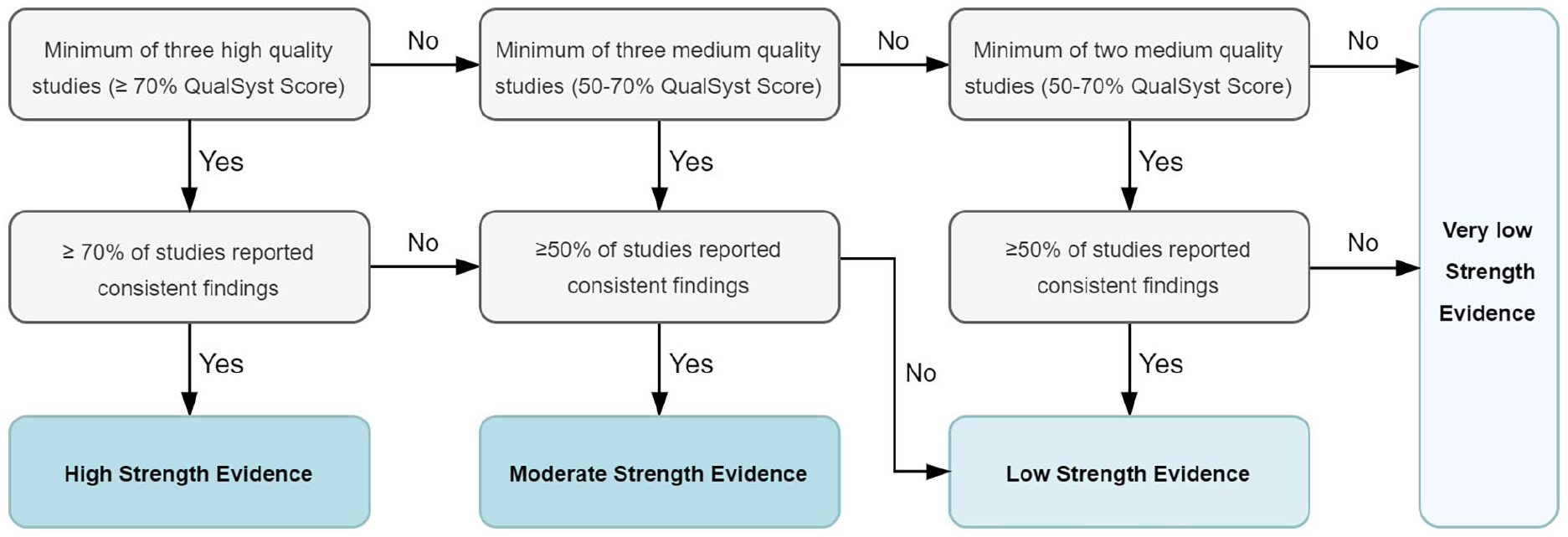
Based on previously published methods, 33 three categories of quality were assigned to the papers according to the allocated summary outcome QualSyst scores (‘low quality’ <50%, ‘medium quality’ 50%–70% and ‘high quality’ ⩾70%).
Synthesis of results
We derived data on all-cause hospitalisations (primary outcome) and heart failure hospitalisations (secondary outcome) including numbers of hospitalisations, rate of hospitalisations, time spent in hospital, or time to first hospitalisation. Primarily, relative measures (e.g. relative risk, odds ratios or hazard ratios) or for continuous variables differences in means with their 95% confidence level and level of significance were extracted. A positive association for factors and outcomes was reported if there was a statistically significantly increased likelihood of hospitalisation (p < 0.05), a negative association if there was a statistically significantly decreased likelihood of hospitalisation (p < 0.05), and no association if there was no statistically significant effect (p ⩾ 0.05). Factors were merged if a combination was considered feasible (e.g. black and non-white race, BMI and weight, systolic blood pressure and mean arterial pressure).
All studies fulfilling eligibility criteria were included in the analysis. For each variable, strength of available evidence across all studies was graded using an algorithm based on Bone et al. 33 (Figure 1). To assess the overall strength of evidence, the number of studies, their QualSyst scores and the consistency of results across studies were considered. If the same number of studies was found for opposite directions of association, the association was deemed inconclusive. Due to heterogeneity of study populations, methodological differences and summary outcome measures pooling of results in terms of meta-analysis was not considered feasible and findings are presented narratively.
Results
Study selection
Through database searching, a total of 15,534 records were identified. Additional searches described in methods identified another 3786 records. After removal of duplicates and title/abstract screening, full text screening was performed on 664 articles. Three studies were identified by reference searching of included and relevant articles27,36,37, one additional study was included from citation searching. 38 No relevant ongoing studies were identified. Finally, 54 articles were selected for inclusion. The selection process is displayed in the PRISMA flow chart shown in Figure 2.
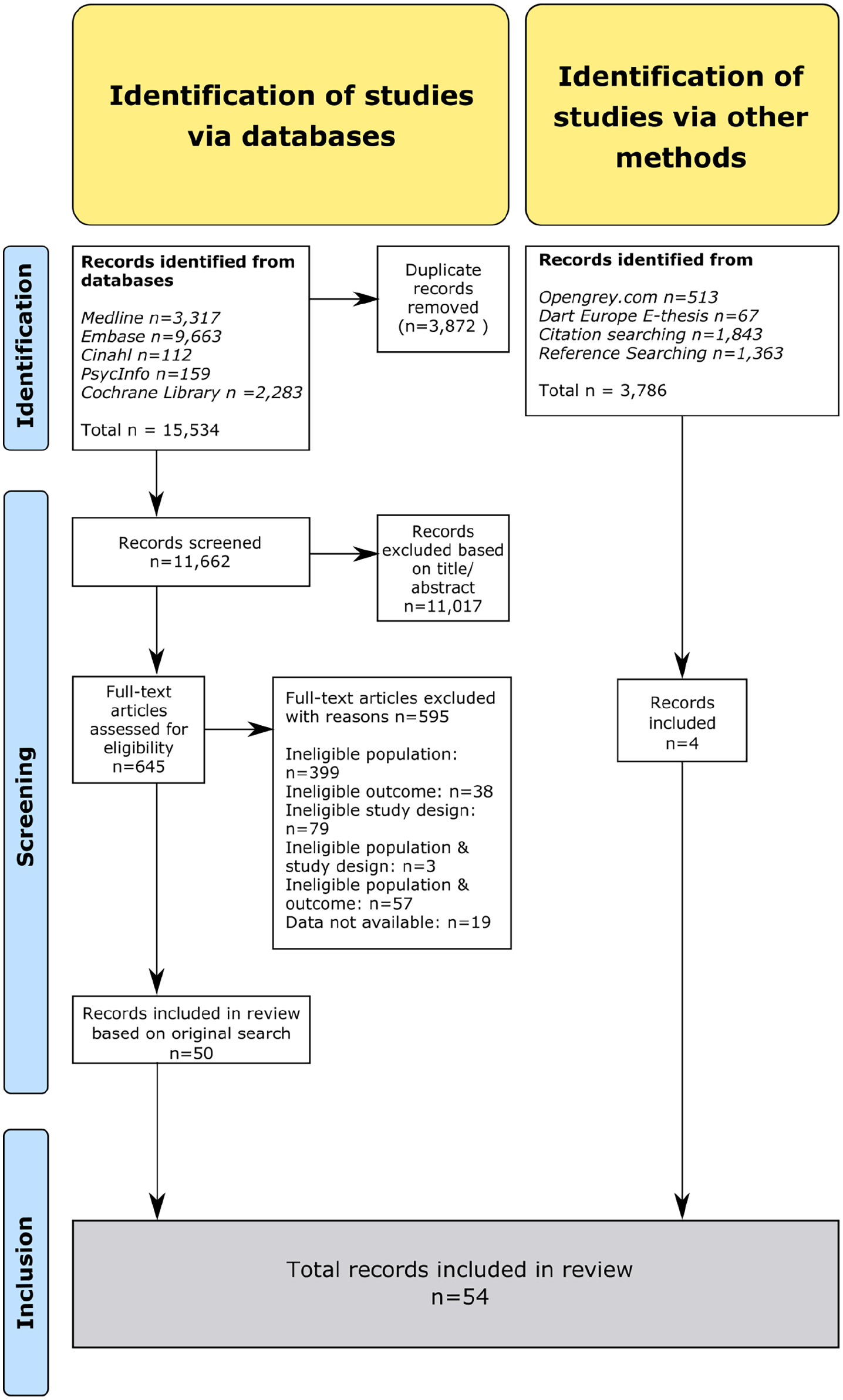
PRISMA flow chart of the study selection process.
Study characteristics
We included 54 publications reporting on 40 studies. All articles were published in English, 30 studies originating in North America, two in Asia (Israel and Hong Kong), five in Europe and three studies were international multicentre studies. There was a great diversity of sample sizes, ranging from 40 to 396,024 patients. After subtracting obvious population overlap, a total of 1,226,186 participants was included in our analysis. The proportion of women ranged from 0% to 61%. A wide variety of factors and their association with hospitalisations were assessed. The included variables were combined into 10 individual-level factors (nine sociodemographic and one personal factor), 39 illness-related factors, 11 service level factors and seven environmental factors. All-cause admissions were assessed in 41 records, heart failure hospitalisations in 28 records with follow-up periods ranging from 30 days to 4 years. An overview of all included studies can be found in the Supplemental Data.
Quality assessment
Overall, the quality of the studies was rated as high, with 46 of a total of 54 studies rated as high quality, achieving a summary score of 70% and higher, four studies rated between 50% and 70% (medium quality) and four studies were of low quality (below 50%).
Synthesis of results
After reviewing the results, we grouped 67 factors into (i) individual-level (socio-demographic and personal) factors (e.g. gender), (ii) illness-level factors (e.g. comorbidities), (iii) service-level factors (e.g. models of care) and (iv) environmental factors (e.g. geographical variations) to facilitate reporting. An overview of all identified factors, their associations with the primary and secondary outcome, and the strength of evidence is presented in Tables 1 to 4. Factors supported by moderate and high strength evidence are additionally summarised below.
Overview of individual-level (sociodemographic and personal) factors and evidence of their associations with all-cause and heart failure hospitalisations.
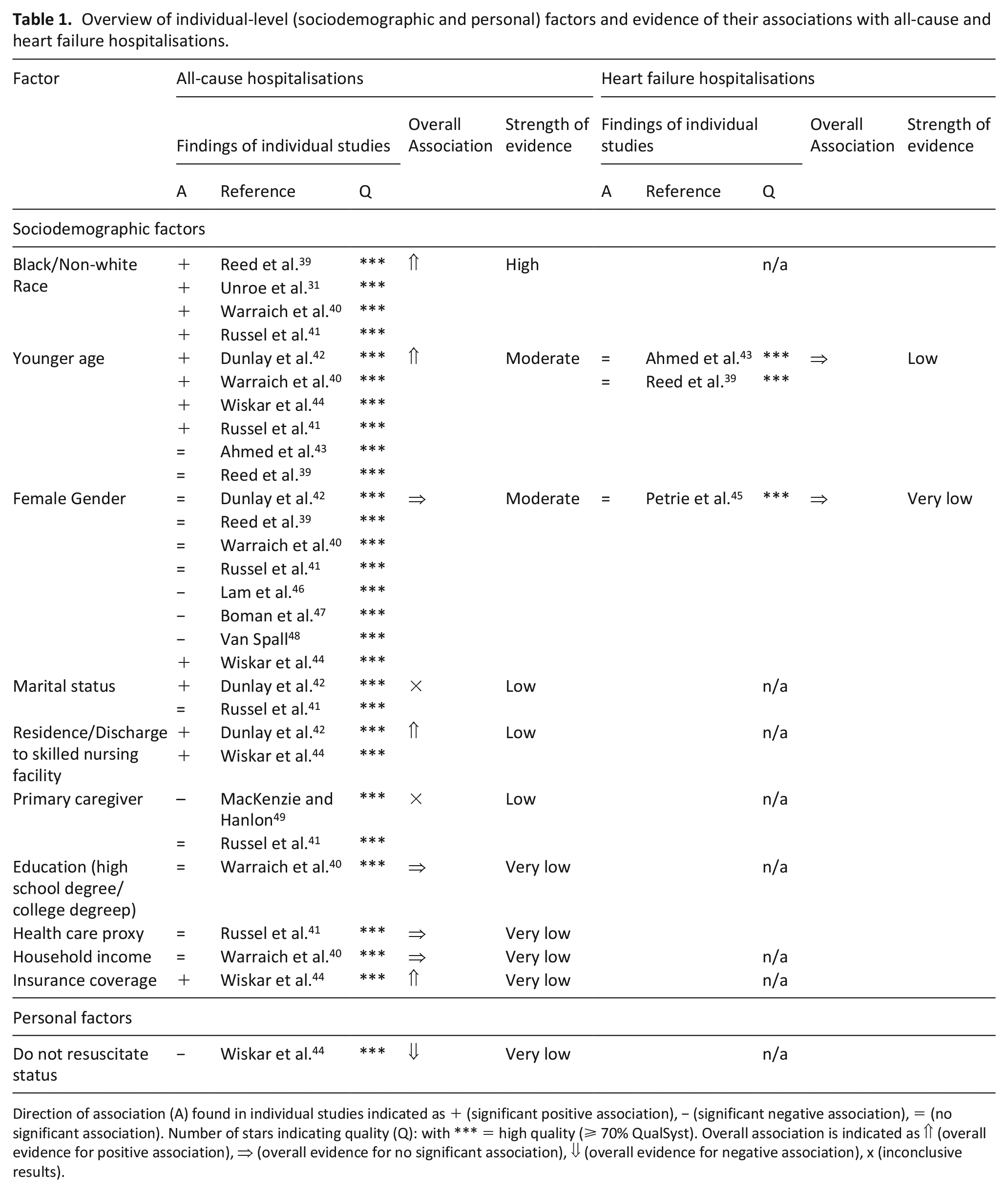
Direction of association (A) found in individual studies indicated as + (significant positive association), − (significant negative association), = (no significant association). Number of stars indicating quality (Q): with *** = high quality (⩾ 70% QualSyst). Overall association is indicated as ⇑ (overall evidence for positive association), ⇒ (overall evidence for no significant association), ⇓ (overall evidence for negative association), x (inconclusive results).
Overview of Illness-related factors and evidence of their associations with all-cause and heart failure hospitalisations.
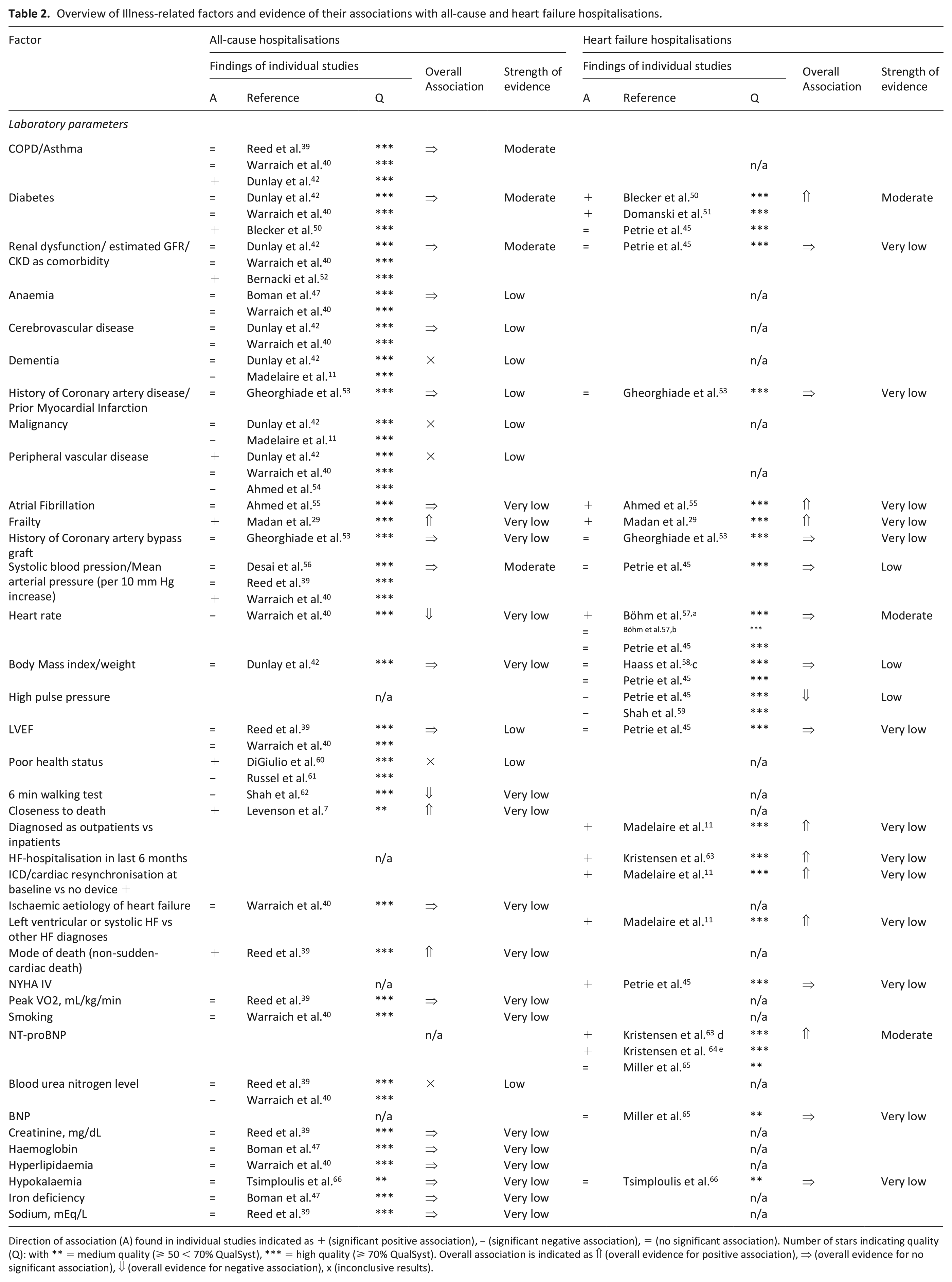
Direction of association (A) found in individual studies indicated as + (significant positive association), − (significant negative association), = (no significant association). Number of stars indicating quality (Q): with ** = medium quality (⩾ 50 < 70% QualSyst), *** = high quality (⩾ 70% QualSyst). Overall association is indicated as ⇑ (overall evidence for positive association), ⇒ (overall evidence for no significant association), ⇓ (overall evidence for negative association), x (inconclusive results).
Overview of service-related factors and evidence of their associations with all-cause and heart failure hospitalisations.
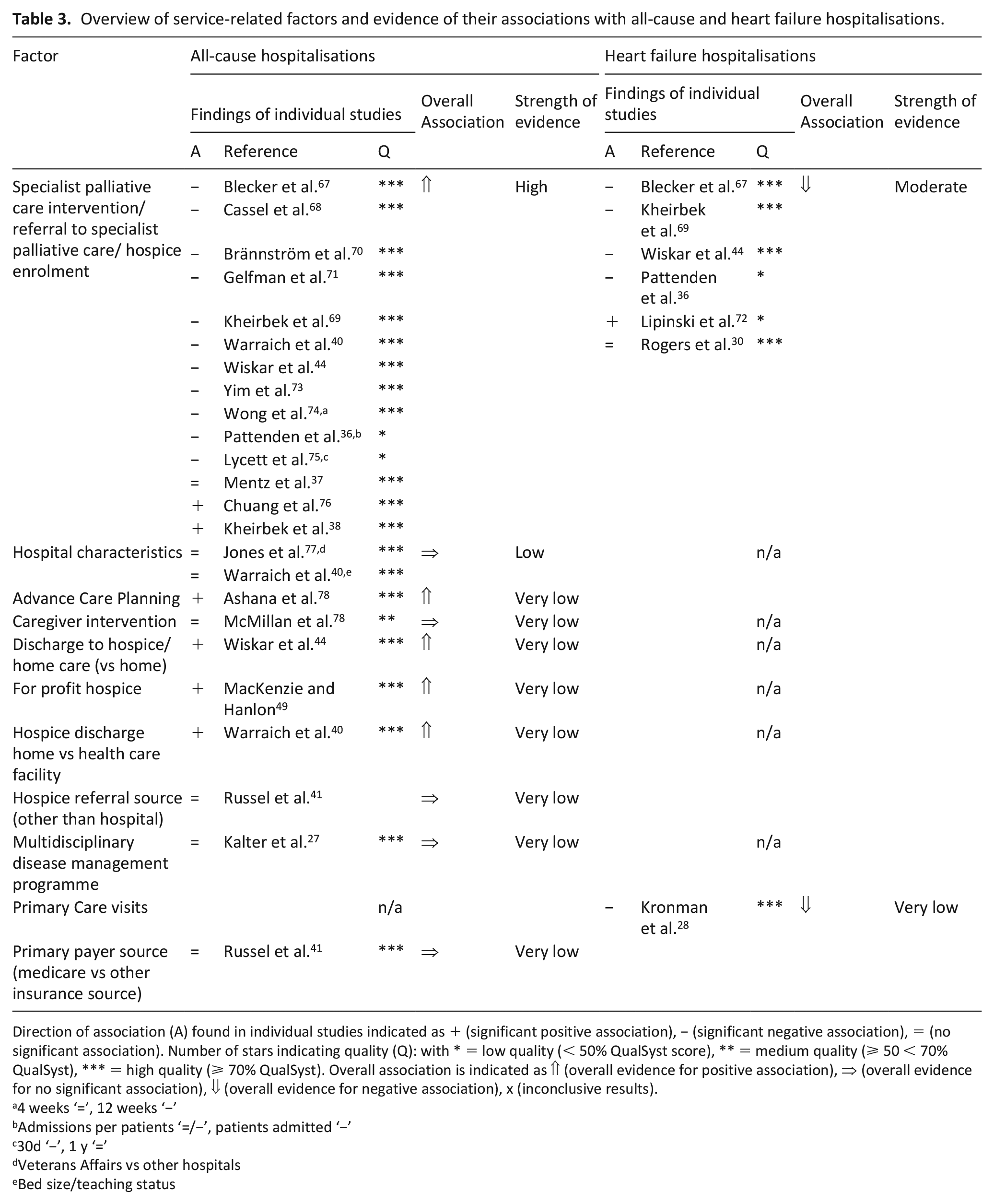
Direction of association (A) found in individual studies indicated as + (significant positive association), − (significant negative association), = (no significant association). Number of stars indicating quality (Q): with * = low quality (< 50% QualSyst score), ** = medium quality (⩾ 50 < 70% QualSyst), *** = high quality (⩾ 70% QualSyst). Overall association is indicated as ⇑ (overall evidence for positive association), ⇒ (overall evidence for no significant association), ⇓ (overall evidence for negative association), x (inconclusive results).
4 weeks ‘=’, 12 weeks ‘−’
Admissions per patients ‘=/−’, patients admitted ‘−’
30d ‘−’, 1 y ‘=’
Veterans Affairs vs other hospitals
Bed size/teaching status
Overview of environmental factors and evidence of their associations with all-cause and heart failure hospitalisations.
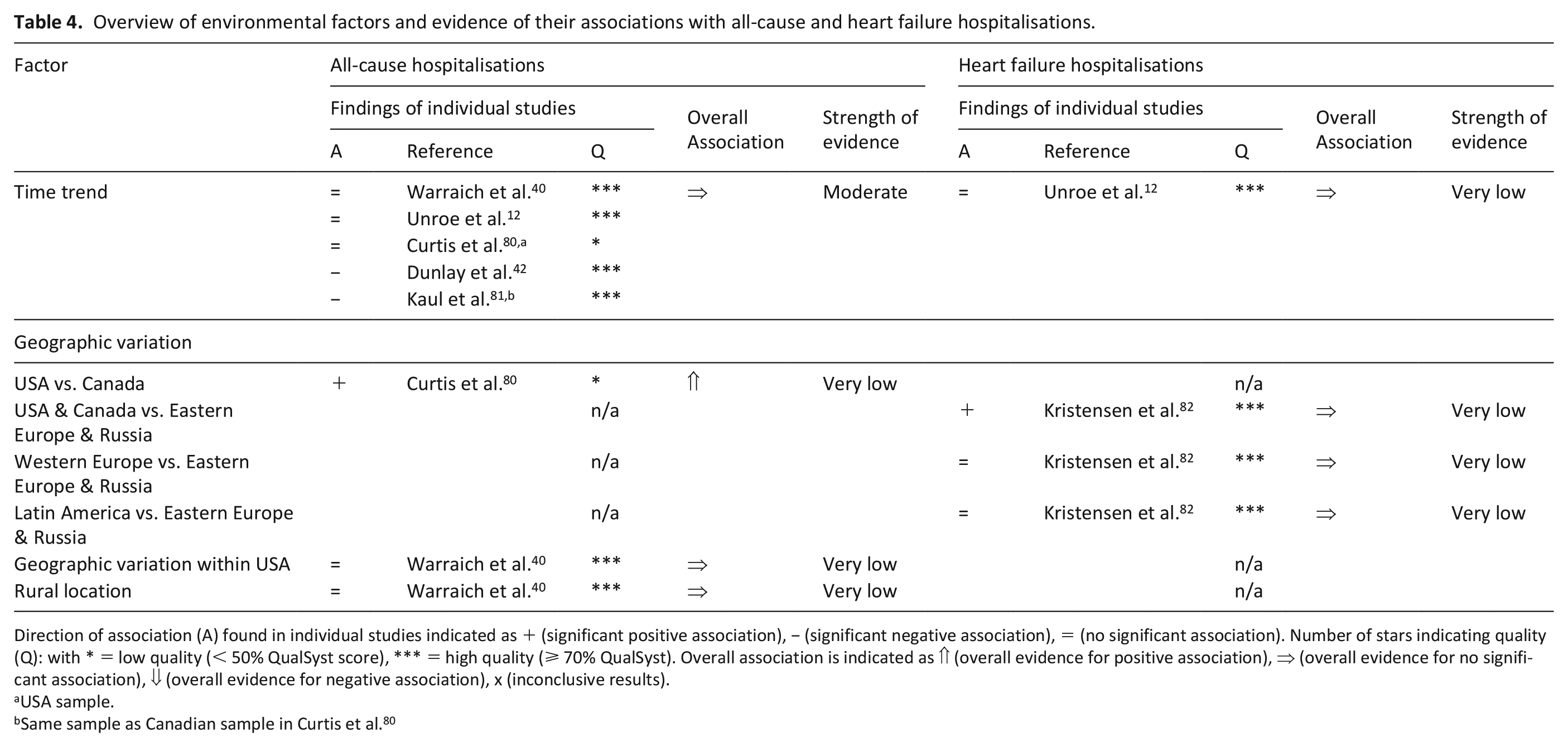
Direction of association (A) found in individual studies indicated as + (significant positive association), − (significant negative association), = (no significant association). Number of stars indicating quality (Q): with * = low quality (< 50% QualSyst score), *** = high quality (⩾ 70% QualSyst). Overall association is indicated as ⇑ (overall evidence for positive association), ⇒ (overall evidence for no significant association), ⇓ (overall evidence for negative association), x (inconclusive results).
USA sample.
Same sample as Canadian sample in Curtis et al. 80
Individual-level factors (see Table 1)
We found high strength evidence of an association between black or non-white race and all cause hospitalisations.31,39 –41
There was moderate strength of evidence for an association between younger age and all-cause hospitalisations.39 –44
Furthermore, we found moderate strength evidence for an equal risk of all-cause hospitalisations for both genders: there was with no significant association in four high quality studies39 –42, three studies found a negative46 –48, one high quality study found a positive association for women. 44
Illness-level factors
A wide range of illness-level factors (Table 2) including comorbidities, clinical variables and laboratory parameters were assessed, as shown in Table 3, however, few factors were significantly associated with all-cause or heart failure hospitalisations. There was a lack of consistent evidence, weakening the inferences that could be drawn.
Service-level factors
Nevertheless, we identified moderate strength evidence that none of chronic obstructive pulmonary disease (COPD), asthma, diabetes, renal failure or increased systolic blood pressure were associated with all-cause hospitalisations (Table 3).
In terms of the secondary outcome, there was moderate strength evidence supporting a positive association of diabetes with heart failure hospitalisations.45,50,51 Furthermore, there was moderate strength evidence that higher heart rate was not associated with heart failure hospitalisations. Lastly, our review provided moderate strength that higher levels of NT-proBNP increased the risk of heart failure hospitalisations in advanced chronic heart failure.
We found high strength evidence that specialist palliative care interventions, referral to specialist palliative care and hospice enrolment are associated with a lower likelihood of all-cause hospitalisations. Eleven studies including nine high quality studies40,44,67 –71,73,79, two low quality studies36,75 consistently reported a lower likelihood of all-cause hospitalisations in patients receiving these interventions. In contrast, two high quality studies found a higher likelihood of all-cause hospitalisation in the intervention group compared to propensity-matched controls.38,76 Only one high quality study yielded no significant association between the factor and all-cause hospitalisation. 37 Heart failure hospitalisations were examined in six studies,30,36,44,67,69,72 which overall found moderately strong evidence of a lower likelihood in patients being provided with specialist palliative or hospice care compared to controls receiving usual care.
An overview of other service-level factors and their association with all-cause hospitalisations and heart failure hospitalisations is presented in Table 4.
Environmental factors
Environmental factors assessed in the included studies comprised time trends (changes of hospitalisations over the years) as well as geographic variations and are displayed in Table 4. Five studies12,40,42,80,81 examined time trends in different settings in North America providing moderate evidence for no association with all-cause hospitalisations.
Discussion
Our systematic review provides the first synthesis of the association of individual, illness-related, service-level and environmental factors with all-cause and heart failure hospitalisations in patients with advanced chronic heart failure. Our findings add to the understanding of the complexity of factors influencing hospitalisations in the population of advanced heart failure. However, two factors in particularly stood out offering compelling evidence: (i) specialist palliative and hospice care proved to be protective, while (ii) black or non-white ethnicity was found to be a risk factor for hospitalisation.
Specialist palliative care interventions were associated with a lower likelihood of all-cause hospitalisations and a reduced likelihood of heart failure hospitalisations in advanced chronic heart failure patients. These findings, supported by high, and moderate strength evidence respectively, build on research highlighting the effect of specialist palliative care for more heterogeneous samples of heart failure patients.83 –85 Indeed, chronic heart failure patients often suffer from palliative care-related problems with substantially higher prevalence of needs in advanced NYHA stages.86,87 For several years, scientific societies of palliative care and cardiology have, therefore, strongly recommended specialist palliative care for this population.4,24,88 –90 But there is still a great disparity of specialist palliative care provision in heart failure compared to cancer patients despite increasing recognition of positive effects on patient-reported outcomes – without impact on mortality.83,84,91 Patients with advanced heart failure are significantly less likely to have clinicians discussing hospice with them, 92 experience more frequent emergency department visits and hospitalisations after hospice enrolment than cancer patients and are admitted to hospice care closer to death. 93 In this context, a variety of barriers to specialist palliative care referrals of heart failure patients have been documented, including misconceptions and confusion around terminology, difficulties of accurate prognostication and uncertainties about referral triggers.94,95 Our systematic review further reinforces the importance of specialist palliative and hospice care for patients with heart failure to reduce unnecessary hospitalisations at the end of life. The results encourage timely integration of specialist palliative care for patients with chronic heart failure and may inform service planning and allocation of resources. However, the effectiveness of well-defined models of palliative and hospice care for advanced heart failure patients need to be further examined in high-quality prospective multicentre studies in order to generate a better understanding of which service elements prevent hospitalisations. Furthermore, qualitative studies could add to a deeper understanding of the mechanisms.
On the level of individual factors, high-grade evidence demonstrated that black/non-white ethnicity is an independent risk factor for all-cause hospitalisations, a finding that aligns with previous evidence of associations of non-white ethnicity with health care use in general heart failure populations,96,97 end-stage heart failure populations 98 as well as throughout other end-of-life care populations.33,99 –101 Reasons for persisting ethnical disparities are multifaceted. Explanations have been sought in differences in comorbidities, cultural beliefs and treatment preferences, distrust of providers, poor access to health care services, lower referral to specialists and barriers to the use of specialist palliative care.97,102 Recently, racial and ethnic minority disadvantage has been flagged as an issue in palliative care offering multiple reasons to explain this phenomenon.103,104 In addition to the occurrence of implicit and explicit racism at the individual and systemic level, psychosocial determinants such as deprivation have been discussed as possible causes. Interestingly, however, a higher prevalence of non-oncological diseases among ethnic minorities has also been implicated to be potentially causal. 103 Existing evidence, indeed, substantiates significant differences of referral rates to specialist palliative and hospice care in non-white patients with heart failure.31,105 Given specialist palliative care is associated with reduced hospitalisations in heart failure, disparities in terms of use of hospice and palliative care for black or non-white people with heart failure may partially explain the higher likelihood of hospitalisations in this population, though this is yet to be corroborated by prospective research. Our results may encourage health care providers to reflect their own biases and to focus on culturally sensitive communication and individualised care. Moreover, we hope to raise awareness of organisations and policy makers to address grievances at the structural level.
While there was strong evidence for the factors of ethnicity and hospice and specialist palliative care, most of the many factors examined in the included studies were of low or very low evidence leaving abundant room for further research. We need to explore more deeply the causality of the identified associations as well as the interplay of factors. Evidence gaps, particularly in relation to psychosocial and personal factors, including preferences, attitudes and understanding of illness, as well as the role of informal carers and the caregiving situation, should be an additional focus for future research.
Strengths and limitations
This systematic review provides a comprehensive overview of the evidence on factors associated with hospitalisations in heart failure patients approaching the end of life, identified and synthesised by rigorous methods. However, there are limitations on study and review level.
Heterogeneity in study designs and outcomes considered, including short-term and long-term outcomes may restrict generalisability of results. A statistical analysis with pooling of effect sizes was thus not possible. Defining advanced heart failure is particularly challenging and little evidence exists regarding criteria indicating end of life for this patient population. Although care was taken in establishing meaningful eligibility criteria, it is conceivable that prognosis for the overall population was incorrectly gauged, leading to an overestimation or underestimation of effects.
Due to the inclusion of studies using register data as well as subpopulations of wider studies there is a possibility of remaining population overlap carrying the risk of over- or underestimating effects.
Use of a language restriction might have introduced language bias possibly excluding data from regions other than North-America and Europe where most of the included studies originated. Therefore, applicability, especially to low- and middle-income countries, might have been limited due to diverse population structures and relevant differences in health care systems across the world.
Conclusion
This systematic review identifies that access to hospice and specialist palliative care is associated with fewer hospitalisations in advanced chronic heart failure. Furthermore, there is strong evidence for the association of black/non-white ethnicity with increased hospitalisations in this population. These findings could foster development of supportive interventions for high-risk patients and could also advise service providers and policy makers in allocating limited resources. In particular, hospice and specialist palliative services should be involved in the care of patients with advanced chronic heart failure to avoid unnecessary hospital admissions at the end of life. It is important to address the disadvantage of racial and ethnic minorities in end-of-life care and to deliver culturally sensitive care in advanced heart failure. Evidence for most factors was low or very low strength, indicating that we still do not understand the full picture of what drives hospital admissions in advanced heart failure. Further research should provide more evidence of factors and a deeper understanding of the causality of the associations found.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221123422 – Supplemental material for Factors associated with hospitalisations of patients with chronic heart failure approaching the end of life: A systematic review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221123422 for Factors associated with hospitalisations of patients with chronic heart failure approaching the end of life: A systematic review by Aina R Zehnder, Anna J Pedrosa Carrasco and Simon N Etkind in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163221123422 – Supplemental material for Factors associated with hospitalisations of patients with chronic heart failure approaching the end of life: A systematic review
Supplemental material, sj-pdf-2-pmj-10.1177_02692163221123422 for Factors associated with hospitalisations of patients with chronic heart failure approaching the end of life: A systematic review by Aina R Zehnder, Anna J Pedrosa Carrasco and Simon N Etkind in Palliative Medicine
Footnotes
Authorship
A.Z., A.P. and S.E. conceptualised and designed the review, A.Z. and A.P. undertook the analysis and interpretation of data, and drafted the manuscript, S.E. revised the draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.