
Abstract
Background:
The number of children with a life-limiting condition is increasing. The mothers of these children commonly provide extensive care at home for their child and are at a higher risk of poor health than other mothers. The impact of this is rarely explored from mothers’ perspectives.
Aim:
To explore mothers’ accounts of their physical and mental health, experiences of accessing healthcare and who they think should support their health.
Design:
Qualitative semi-structured interviews were conducted and analysed using thematic analysis.
Setting/participants:
Thirty mothers of children with a life-limiting condition were recruited via three UK children’s hospices and social media.
Results:
Mothers felt that their health concerns could be misunderstood by professionals, describing untimely and inappropriate support that failed to recognise the nature of caring for a child with a life-limiting condition. This led to mothers’ reluctance in addressing these concerns. Mothers felt unable to prioritise their own needs, relative to those of their child and worried about who would look after their child if they did become unwell. They described stress as a result of battles with services rather than as a result of caregiving. Mothers valued feeling recognised as caregivers, which made it easier to look after their health alongside their child’s. Hospice support was particularly valuable in this respect.
Conclusions:
A more unified system that recognises not only the unique set of challenges presented to mothers caring for a child with a life-limiting condition, but the value of palliative care services in supporting these mothers, is required.
Mothers of children with a life limiting condition are more likely to experience physical and psychological health problems than other mothers.
Understanding the health of these mothers is important in its own right, as well as in ensuring that they feel able to care for their child.
Mothers’ health and wellbeing was closely linked to how well they felt their child’s needs were being addressed.
Health and wellbeing problems were more often linked to ‘battles’ with service provision, rather than as a direct result of caregiving.
Mothers’ felt that their unique experiences as caregivers to children with life-limiting conditions could be overlooked, leading to the offer of untimely and inappropriate support and treatment.
Recognising the specific consequences of providing complex and often life-saving care to a child, who the mother knows will eventually die, is important when supporting mothers’ own health and wellbeing.
In order to fulfil mothers’ support needs, provisions must recognise mothers as individuals and as caregivers, in addition to acknowledging the relationship between maternal health and the needs of their child.
A more cohesive and understanding system is required to enable mothers to seek support for their own health alongside feeling supported in providing their child’s care.
Introduction
The number of children with a life-limiting or life-threatening condition is increasing. Latest figures show a prevalence of 66.4 per 10,000 in England in 2017/18, which is estimated to increase to between 67.0 and 84.2 per 10,000 by 2030. 1 This includes conditions for which there is no cure and from which a child or young person will eventually die, such as Duchenne Muscular Dystrophy, in addition to conditions for which treatment may be possible but can fail, such as cancer. In paediatrics, palliative care begins at diagnosis and is delivered alongside other treatments. 2 Consequently, these children may receive palliative care for long periods of time, often over the course of many years. 1
The parents of these children usually assume an extensive caring role including the management of ventilation support, 3 gastrostomy feeding 4 and multiple medications. 5 Further, parents are often required to balance additional responsibilities such as managing busy appointment schedules, offering advocacy, negotiating complex decision making, supporting education, providing transport, alongside fulfilling family and social responsibilities. 6 These responsibilities are ever present, particularly for mothers, who are most likely to be their child’s primary caregiver. 7
Current evidence tells us that mothers of children with a life-limiting condition are more likely to experience poor physical and psychological health outcomes than other mothers, including back problems, heart problems, arthritis, anxiety and depression. 7 However, information about the impact of such conditions, as well as how – and by whom – mothers feel that their health concerns should be best managed, is rarely discussed in the literature. This re-emphasises the need for further research on appropriate physical and psychological support for these mothers, 8 also highlighted in National Institute for Health and Care Excellence (NICE) guidelines. 9 This is important not only for mothers themselves, but in ensuring that they feel able to care for their child. This study addresses this gap by exploring mothers’ accounts of their mental and physical health; their experiences of accessing healthcare; and views on which services should support their own healthcare needs.
Methods
This was an exploratory qualitative study in which semi-structured interviews and open-ended questions were used to explore mothers’ accounts of their physical and psychological health, their experiences of accessing healthcare and how they think their health should be supported. We drew on an interpretivist/constructivist paradigm 10 to explore how mothers made meaning of their lived experiences whilst recognising the importance of researcher experience and background in such interpretations. The study was reported following the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 11
Participants
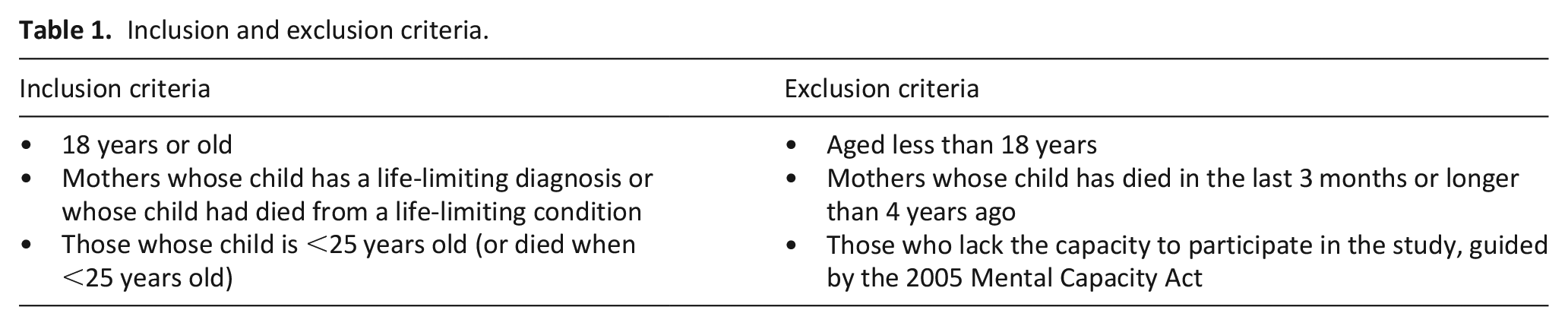
Mothers of children with a life-limiting condition were included if they met the criteria defined in Table 1.
Inclusion and exclusion criteria.
Sample
Mothers of children with a life-limiting condition or whose child had died from a life-limiting condition were eligible for the study. Purposive sampling was undertaken by healthcare professionals during consultations, meetings and visits, as per the study inclusion criteria.
Recruitment
Participants were recruited through three UK-based children’s hospices and social media (Facebook, Twitter) between November 2020 and June 2021. If eligible, healthcare professionals provided mothers with the study information, following which potential participants gave written consent for their details to be passed onto a researcher. The study team contacted all participants who completed a consent-to-contact form to discuss the study, check eligibility and book an interview if appropriate. The study team received 39 consent-to-contact following which Potential participants who saw the advertisement on social media were directed to contact the study team directly, following which the same steps as above were followed.
Data collection
Interviews took place between November 2020 and July 2021. The topic guide (Supplemental Material) was developed from the literature, refined with patient and public involvement (PPI) and through piloting. It included topics such as the exploration of mothers’ own health concerns, ease of access to healthcare for themselves, ways in which they look after their own health and suggestions on which services should look after their health. Semi-structured, audio recorded interviews were carried out by two female researchers (VF, LF), separate from the clinical setting, who hold interview training and experience and were not familiar to participants prior to the study. Following verbal or written consent, interviews were carried out on the telephone or via video call, depending on participant preference. We were unable to conduct face-to-face interviews due to the COVID-19 pandemic. Probes and additional questions were used for clarification and deepening of understanding. Interviews were audio-recorded, transcribed verbatim and anonymised prior to analysis. Field notes were also taken during the interviews.
Analysis
Interview data was organised, managed and coded in NVivo and analysed using thematic analysis. 12 The stages of thematic analysis were followed; (1) familiarisation through repetitive reading; (2) generation of initial codes; (3) theme development; (4) reviewing of themes; (5) defining and naming the themes; (6) writing up and summarising themes. The aim of thematic analysis is to identify patterns and themes in qualitative data 13 and the steps of thematic analysis were followed in an inductive and iterative manner. Coding was inductive and conducted by one researcher (VF) with frequent discussions with the research team to optimise trustworthiness.
Ethical considerations
Research Ethics Committee approval was granted (reference 20/NE/0164) on 2nd July 2020. Informed consent was provided by participants and monitored throughout the interview process. There was a procedure in place for any participants who became distressed during interview which involved taking a break from or stopping the interview if required. Follow-up telephone calls were offered to participants 24–48 h after interview to check whether they had any questions or concerns after the interview. The procedure for any participants who were distressed during the follow-up call was encouragement to seek support from an appropriate professional such as a member of staff at the children’s hospice from which they were recruited for the study.
Results
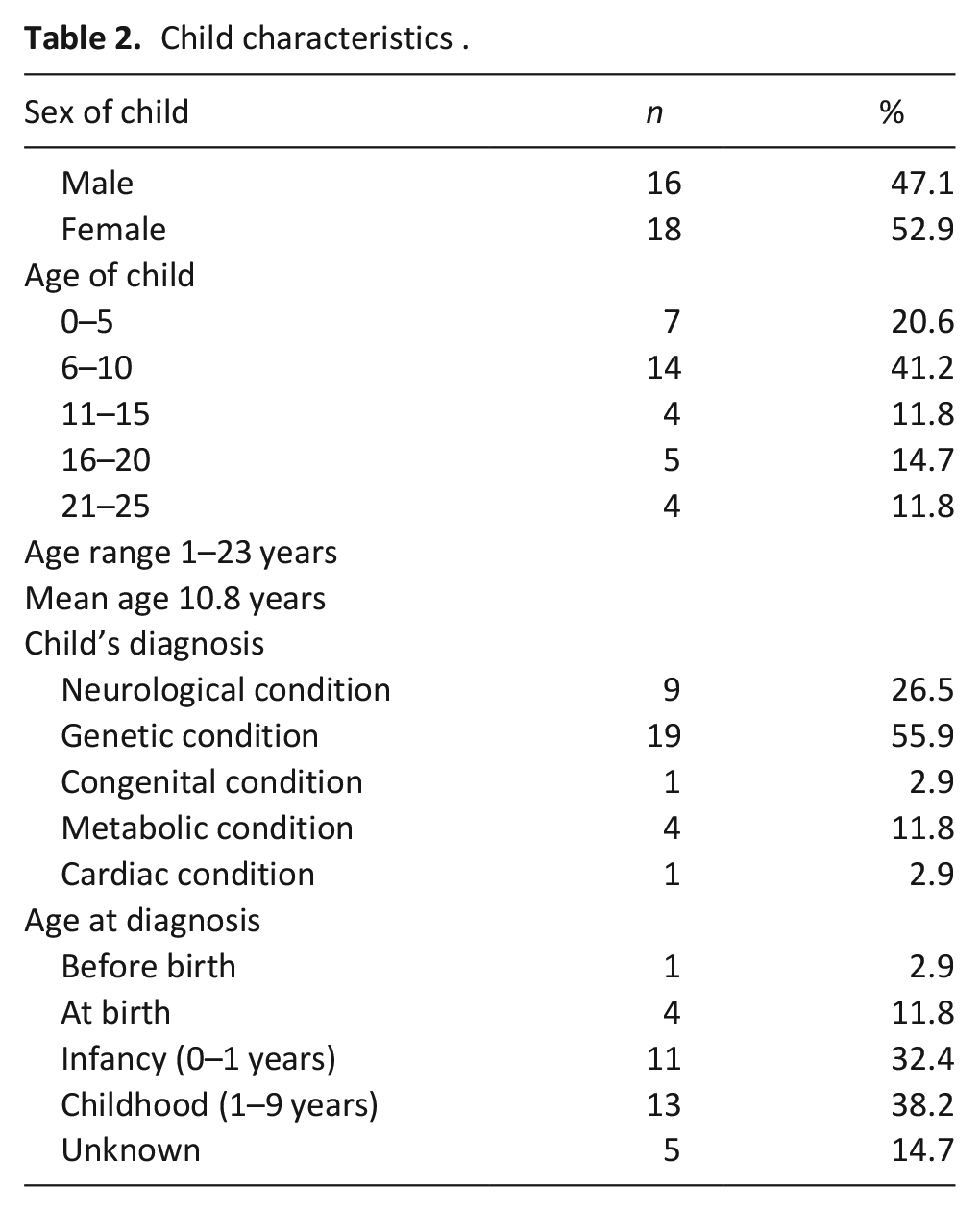
Thirty participants completed interviews, 24 of which were recruited via hospices and six via social media 39 consent-to-contact forms were received from hospices, meaning that 15 mothers decided not to participate in the interview after providing their details. For some this was due to a lack of time to participate and for others, contact was lost. Mothers were aged between 32 and 60 and resided across the UK. Some mothers had more than one child with a life-limiting condition meaning that the mothers of 34 children were interviewed. Child characteristics are provided in Table 2.
Child characteristics.
Interview length ranged from 27 to 102 min (average 63 min). Four analytical themes were identified from the analysis. These themes describe experiences surrounding mothers’ own health and wellbeing and those of accessing support for themselves.
The unique experience of parenting a child with a life-limiting condition: A need for understanding
This theme describes the unique experience and associated complexities of caring for a child with a life-limiting condition. Mothers felt that their experiences could go unrecognised, reflected in what they regarded as a paucity of appropriate support and understanding from services. This was demonstrated, for example, by difficulties in accessing timely support through their GP, which was often attributed to first needing to prioritise their child’s needs.
‘It had reached points where I couldn’t even stand in the last 8 months but it has been virtually impossible to get a GP appointment. Because I have to phone to renew [child’s] medication, if I can get through to reception, that’s my priority. It has taken 28 phone calls on occasion to get through to anybody’ [Mother 2].
As well as some physical health concerns, mothers described their experiences of anxiety, depression and post-traumatic stress. The onset of these symptoms could be sudden and unexpected.
‘I went from coping with everything to just not. . .I had zero energy. Just the thought of telling somebody what had happened to [child], I just couldn’t bear it. I realised that it was depression. That was very unfamiliar to me’ [Mother 25].
Poor access to timely healthcare, was often followed by inappropriate treatment or referrals being offered, particularly in the case of mental health concerns; namely, prescriptive therapies with a limited number of sessions, scheduled at times that made it difficult for mothers to attend due to their caregiving responsibilities.
‘I went to the first CBT (cognitive behavioural therapy) appointment. I spent 15 minutes going through everything, past, present and future, and they kind of sat there and their jaw got progressively lower and lower. At which point they literally went ‘I’m going to stop you there because this is well beyond what we can deal with. We’re only given funding for 12 weeks and this is a lot more than 12 weeks of stuff’ [Mother 8].
Some mothers who were prescribed psychological therapies, believed they did not address or recognise the nature of providing complex and extensive life-saving care for a child.
‘I think I struggled with the concept that my thought processes were irrational. I think I kind of looked at our circumstances and thought “to be honest most people would feel a bit crazed” and I really struggled with that’ [Mother 3].
Mothers also expressed particular concern that self-perceived normal reactions to extremely challenging situations were automatically labelled as a mental health concern by professionals. They found this unhelpful and believed such responses failed to recognise the realities of caring for a child with complex needs.
‘I didn’t feel like I did have anxiety or depression. I suppose it is anxiety, but it’s a different anxiety. . .. when your child stops breathing, it’s reasonable anxiety’ [Mother 19].
Mothers’ reluctance to prioritise their own health and needs
The first theme explored difficulties associated with accessing timely and appropriate support, with mothers describing a lack of recognition of their individual needs and a subsequent disengagement in addressing these needs. However, analytically distinct from this first theme was a deeper sense of unwillingness to prioritise their own needs, both in terms of healthcare and general support. This theme is broken down into three sub-themes contributing to this reluctance; a lack of trust in others’ ability to care for child, worries about judgement from others and a need to be strong for others. This is summarised in Figure 1.
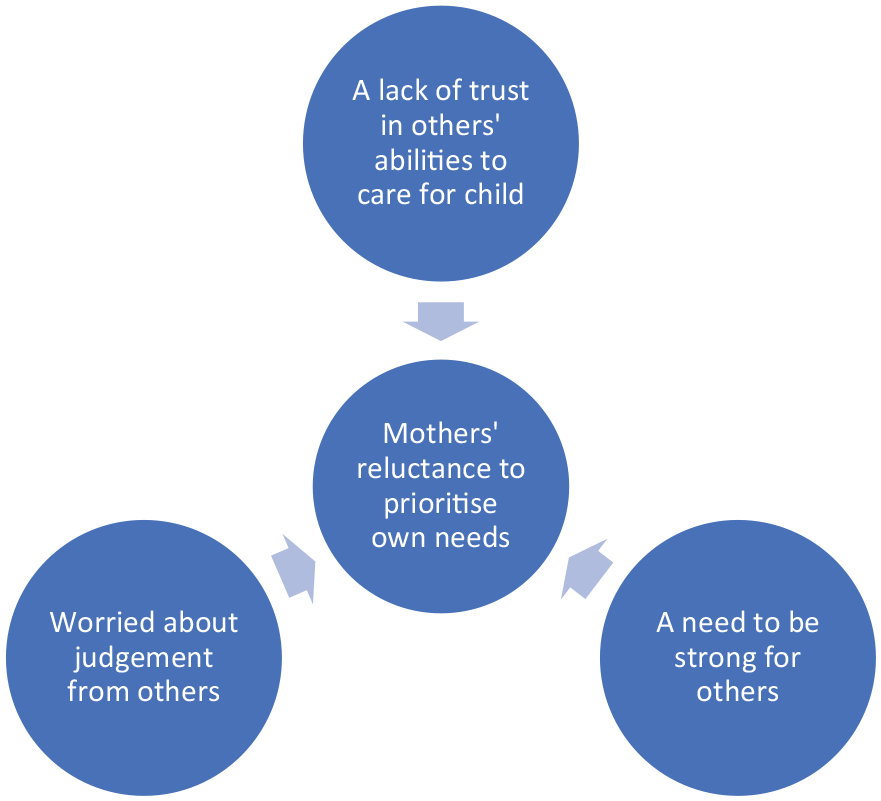
Factors contributing to mothers’ reluctance to prioritise own needs.
A lack of trust in others’ ability to care for child
Mothers described having an instinct for their child’s needs and felt they were the only ones able to provide adequate care for them. A lack of trust - often based on previous experience – and a fear of handing over complex caregiving responsibilities, meant that it was difficult for mothers to ask for or accept help, whether they felt they needed it or not. This meant that they rarely got a break from caregiving.
‘I don’t trust family to look after [child]. Not that I don’t trust them, I don’t trust their medical ability to cope in a crisis. It’s difficult and incredibly stressful and takes a lot of inner strength to cope with it’. [Mother 25]
This lack of trust in others led to worries that if they did become unwell in the future, or needed some extra help, their child would not be looked after properly. This generated future anxieties and vulnerabilities and may also explain why some ignored initial signs of illness.
‘I can’t even go there yet. Like I didn’t think she had years to come. But, you know, yes, in the bigger picture, I need to be in the full of my health, and I feel quite vulnerable, and I’m really conscious that I don’t have a sense that I can look outwards [tearful], you know. And this is partly me trying to break through that and daring to say it to a doctor, going – I really am terrified of doctors now’. [Mother 17]
Worried about judgement from others
Mothers were also concerned that if they asked for help, they would be judged for ‘not coping’ or else be perceived as a burden to others.
‘I don’t want people to worry about me and if I have a really bad day, I don’t think I’m able to call anybody, I just want to crawl away and wait until it’s over and don’t want to worry people’. [Mother 12]
A need to be strong for others
Mothers also believed that they needed to be strong for other family members. When asked to talk about their own health, mothers frequently went on to talk about what things were like for their child and family. This further highlighted a reluctance to talk about themselves and how closely related their own wellbeing was to that of their child and family.
‘He [partner] struggles as well. If I’m struggling he knows, he just knows I am but I don’t highlight it because I don’t want to set him off. He had a number of issues over the last 10 years, always around [child’s] birthday time’. [Mother 1]
There was, however, a level of recognition that mothers needed to be well to provide the care for their child particularly for those who had experienced issues with their own health in the past. For some this manifested as making sure that some self-care was observed, although as we have seen the demands of care can make this difficult.
‘To be able to look after [child], I need to look after myself. It’s a full-time job and when things go wrong, it happens quickly. So I just need any support I can get and to look after myself so that I can cope when that happens’. [Mother 25]
Stress resulting from battles with services, rather than as a direct result of caregiving
This theme describes mothers’ interactions with services, which they often talked about as ‘battles’ or ‘fights’, ongoing for extended periods of time. The nature of the impact of such battles varied, depending on the type of support that mothers felt they were lacking. It could include anything from access to specific equipment to more general support. For example, lifting a heavy child whilst awaiting appropriate equipment caused back problems and pain.
‘Not having the correct equipment is a big one. Because of COVID things have slowed down. I’ve waited 6 months for a sling. The sling is the most important thing in our house at the moment. We need it. She’s a big girl and as a result of us not having a sling, me and dad have now got back problems. I’ve been waiting months for a hoist. It was like this even before COVID’. [Mother 27]
Financial wellbeing was also an issue for families who had tried to fund equipment themselves. Mothers regarded these ‘battles’, (particularly for equipment), as relentless and difficult to manage, especially when they had to be negotiated alongside other caring demands. They felt that managing many different challenges had an accumulative impact on their wellbeing.
‘I will hold my hands up and say yes, it is hard. But it would be easier if we didn’t have to fight for the help that we need and have to chase people who don’t do what they say they are going to do. It just adds to the feeling of general tiredness and exhaustion really’. [Mother 30]
Mothers highlighted these ‘battles’ when responding to questions about their physical and mental health. They reiterated that their stresses arose from these interactions with services, rather than as a direct result of caregiving. This further demonstrated how closely linked mothers’ wellbeing was, with how well their child’s needs were being addressed.
‘The frustration isn’t medical. The frustration is the network of services. It’s the constant battle and how massively time consuming and frustrating it is’. [Mother 2]
Establishing connections; feeling recognised
This final theme explores the value of feeling recognised, particularly the importance mothers attached to care professionals understanding their situation. Mothers, for example, emphasised the benefit to their wellbeing, of feeling they had established a rapport with professionals involved in the care of their child. Mothers spoke of how such rapport helped mitigate against the stresses associated with providing constant care for their child. It also often helped mothers reflect on and address their own health. Mothers identified hospice support as especially important. They felt able to discuss their own needs with hospice staff, who they believed understood their family and perhaps more importantly, the challenges of caring for a child with complex needs. Mothers expressed frustrations about constantly needing to explain the child’s condition (and needs) to other care professionals. This further explains the value of hospice care.
‘Having counselling through the hospice. . . firstly they have met [child] which makes a difference. . . it’s all one team. . . I know if I had the choice I would always access support through the hospice because it’s such a massive part of everything. You can’t have counselling and not have an understanding of that part of my life’. [Mother 22]
Mothers also specifically valued support offered directly alongside their child’s care, knowing that their needs were being taken into consideration.
‘Yeah so the NICU. . . basically assume that you need it and want it [counselling], so it’s an opt out system rather than an opt in. So the second [child] was born we were assigned a counsellor and within a week she had come to the cot side and introduced herself and said “shall we book a time in another room to sit and talk so we’re not talking around an incubator?”. It should be provided. I say that very strongly, should be provided’. [Mother 23]
This contrasted with mothers’ experiences of support from other professionals. When asked ‘when was the last time that a healthcare professional asked how you were?’, mothers explained that this was not only rare, but carried with it an assumption that they should answer that they were ‘okay’, as there wasn’t time to discuss any issues during their child’s appointments, a failure in recognition that their wellbeing was connected to that of the wellbeing of their child.
‘There’s not the holistic family approach, it’s just focused on [child] and we just have to, you know, do our best, but our wellbeing isn’t really considered’. [Mother 30]
Support and activity groups involving other mothers could also be useful, particularly for generating a shared understanding of experience, alongside practical advice related to getting appropriate equipment and support. However, mothers were keen to highlight that some of the groups they attended included parents whose child had different needs to their own. At times, this created challenges in generating a shared understanding and prompted feelings of isolation.
‘As soon as you come into the special needs world you are suddenly just surrounded by ADHD and autism to be perfectly honest and that’s not us, I have a child who is not even on the autistic spectrum and it’s very hard to access services, it’s very hard to get anybody to think it matters because a lot of people assume if you’ve got a serious child, “Well you must get tons of support” And often we get in many ways the least because we can’t access universal services like after school clubs or even school a lot of the time’. [Mother 17]
Discussion
Main findings
The aim of this study was to explore mothers’ accounts of their physical and mental health and to identify how, and by whom, their own wellbeing should be addressed. Previous research tells us about the types of physical and mental health conditions present in this population7,14 but these conditions have rarely been explored qualitatively. In this study, mothers described a healthcare system that did not accommodate their needs as caregivers. They highlighted how care professionals could misinterpret mental health concerns, failing to recognise the unique nature of caregiving and differentiate between normal and pathological distress. Mothers also highlighted how their wellbeing was mostly affected through conflicts with service provision, rather than as a direct result of caregiving. Some mothers did describe positive examples of support, though this was closely linked to how well they felt their child to be supported. This created a tension, in which the mother strongly identified their needs with that of the child, while also wanting to be recognised and supported as caregiver in their own right. This was not easily negotiated and reflects the complexities of the mothers’ response to their role.
Mothers valued practical and emotional support from care professionals. Hospice support was particularly valued as an environment in which mothers’ own needs could be addressed alongside their child’s needs. However, they demonstrated an underlying reluctance to address their own needs, which was sometimes related to a fear that if they did become unwell, there would be no one else capable of looking after their child. Mothers described a lack of trust in others’ abilities to care for their child, particularly when their child required substantial medical intervention and monitoring. Mothers sometimes played down the challenges they faced, but also believed some care professionals were not especially interested in how they felt. This created an environment in which mothers were unsure about how to express concerns relating to their wellbeing and worries about being misinterpreted when articulating these concerns. This explained their sense of vulnerability when seeking support.
Strengths and limitations
Although recruitment was delayed slightly due to the COVID-19 pandemic, we found that many participants valued the opportunity to share their experiences over the phone or via zoom. Ordinarily, they would not have had the time to take part in the study. Equally, had it been feasible, some participants would have preferred to share their experiences in a face-to-face interview. We recognise that the data was collected during an especially difficult time for these families, particularly those who had been shielding. Recruitment was heavily reliant upon hospice staff, meaning that much of our sample comprised of those who had received support from a children’s hospice, which is not always the case for this population of caregivers.
What this study adds
This study reflects existing research on the impact of caregiving on the health of caregivers, including both psychological and physical health problems. 15 However, existing studies have predominantly focussed on the health of caregivers of children with disabilities or specific conditions rather than on those of children with life-limiting conditions.16,17 We know that parents face many challenges in caring for a child who they know will eventually die18–21 but this has rarely been explored in the context of mothers’ own health seeking behaviour and their own perspectives of how their own health should be supported.
Parent caregivers frequently deal with what they describe as ongoing ‘battles’ with services to get appropriate levels of care and support for their child.6,22 The experience of mothers included in this study was no different and the COVID pandemic had amplified these existing issues further. Navigating a disjointed system and ‘battling’ for support with little or no means of guidance was challenging and overwhelming when considered alongside the challenges of their everyday caregiving responsibilities. This is important when understanding the context of mothers’ psychological health and should be considered alongside mothers’ perceived inadequacies of current support when deciding on appropriate interventions.
The mothers in this study highlighted some limitations of traditional psychological interventions (such as CBT). Considering these perspectives when thinking about more effective support is important. Mothers identified hospice support as being particularly valuable, because they were able to access support alongside their child’s care and from known and trusted professionals. Gaining support and reducing uncertainties through the formation of these relationships was invaluable in ensuring mothers felt recognised in their roles and supported in navigating the system, as well as being allowed the space to reflect upon their own health and needs. This reflects current literature that highlights the value of hospice respite and strong relationships with professionals in improving psychological outcomes for caregivers.23,24
Conclusions
Through mothers’ accounts of their own health, this study has highlighted the importance of understanding their practical, emotional, physical and social needs more holistically. It is important to recognise that being a parent of a child with a life-limiting condition presents a unique set of challenges that can leave mothers feeling isolated and vulnerable. Mothers’ ongoing ‘battles’ with service provision increased their stress and exacerbated the challenges of caring responsibilities.
Mothers struggled to obtain appropriate and timely support for physical and mental health conditions and often felt that their needs could be misunderstood, demonstrated through limited or erroneous treatment options. Strong relationships and open communication with healthcare staff, who understood their child’s care needs, seemed to mitigate some of these issues. This was made particularly evident through mothers’ experiences of hospice support, which offered them a level of understanding not experienced in other settings. Current inequities in the support received by these families means that not all families that would benefit from palliative care services, have access to them. 25 However, this study, reinforces evidence surrounding the value of such services in supporting families. Given the vital role that these mothers play in the healthcare of their children, the healthcare system should recognise and prioritise the services that these mothers need to stay well.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221122325 – Supplemental material for The health of mothers of children with a life-limiting condition: A qualitative interview study
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221122325 for The health of mothers of children with a life-limiting condition: A qualitative interview study by Victoria Fisher, Karl Atkin and Lorna K Fraser in Palliative Medicine
Footnotes
Acknowledgements
The authors wish to thank the members of the Martin House Research Centre advisory board for their input to this study and to the participants who took the time to share their experiences. The authors would also like to thank Dr Jo Taylor for her contributions to the study.
Author contributions
LF led the conception and design of the study and obtained funding. LF and VF collected the data. VF analysed the data with regular input from LF. VF drafted the manuscript with substantial contributions from LF and KA. All authors approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Victoria Fisher is funded by a National Institute for Health Research (NIHR) Career Development Fellowship (award CDF-2018-11-ST2-002) that was awarded to Lorna Fraser for this research project. This publication presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.