
Abstract
Background:
Delirium is common and distressing for patients receiving palliative care. Interventions targetting modifiable risk factors in other settings have been shown to prevent delirium. Research on delirium risk factors in palliative care can inform context-specific risk-reduction interventions.
Aim:
To investigate risk factors for the development of delirium in adult patients receiving specialist palliative care.
Design:
Systematic review and meta-analysis (PROSPERO CRD42019157168).
Data sources:
CINAHL, Cochrane Database of Systematic Reviews, Embase, MEDLINE and PsycINFO (1980-2021) were searched for studies reporting the association of risk factors with delirium incidence/prevalence for patients receiving specialist palliative care. Study risk of bias and certainty of evidence for each risk factor were assessed.
Results:
Of 28 included studies, 16 conducted only univariate analysis, 12 conducted multivariate analysis. The evidence for delirium risk factors was limited with low to very low certainty.
Potentially modifiable risk factors:
Opioids and lower performance status were positively associated with delirium, with some evidence also for dehydration, hypoxaemia, sleep disturbance, liver dysfunction and infection. Mixed, or very limited, evidence was found for some factors targetted in multicomponent prevention interventions: sensory impairments, mobility, catheter use, polypharmacy (single study), pain, constipation, nutrition (mixed evidence).
Non-modifiable risk factors:
Older age, male sex, primary brain cancer or brain metastases and lung cancer were positively associated with delirium.
Conclusions:
Findings may usefully inform interventions to reduce delirium risk but more high quality prospective cohort studies are required to enable greater certainty about associations of different risk factors with delirium during specialist palliative care.
Delirium is common and distressing in patients receiving palliative care.
Studies of multicomponent interventions targetting modifiable delirium risk factors have reported delirium risk reduction in other settings.
There is uncertainty about which delirium risk factors to address in patients receiving palliative care.
A number of studies have examined delirium risk factors for patients receiving palliative care but the overall evidence is limited with low to very low certainty.
Potentially modifiable risk factors reported to be positively associated with delirium included opioids and lower performance status, with some evidence of association for dehydration, hypoxaemia, sleep disturbance, liver dysfunction and infection.
The evidence for several risk factors commonly targeted in preventative interventions in other settings was mixed or reported in a single study only.
There is a need for more high quality prospective cohort studies to enable greater certainty in the association of different risk factors with delirium.
The limited evidence may be used to inform interventions to reduce the risk of delirium in the palliative care context.
Introduction
Delirium is a distressing condition that is common in patients with advanced illness and associated with serious adverse outcomes.1–3 It is a manifestation of underlying and multifactorial pathophysiological abnormalities and is characterised by acute and fluctuating disturbances in attention, awareness and cognition.4,5 Multicomponent interventions targetting modifiable risk factors reduce the risk of delirium by around one in three cases during hospitalisation.6,7
Systematic reviews suggest that although many risk factors for delirium are common across different patient populations and settings, their types and strengths of association vary. Reviews in older hospitalised patients 8 and Intensive Care Units 9 both found strong associations with older age, dementia and illness severity, but other significant risk factors differed and some were setting-specific, such as mechanical ventilation in intensive care. Vasilevskis et al. 10 and Ahmed et al. 8 have highlighted this variability between clinical settings and patient populations. Therefore, it is important to identify specific delirium risk factors, and the strengths of their association, for patients receiving palliative care. For example, palliative care patients’ risk of delirium may be increased due to factors related to advanced disease and multi-organ dysfunction 11 and their frequent exposure to iatrogenic risk factors such as opioids. However, to our knowledge, no systematic review of delirium risk factors in patients receiving palliative care has yet been reported. 12
Synthesis of evidence on potentially modifiable risk factors is important to inform the design of interventions to reduce the risk of developing delirium. The term, ‘potentially modifiable’ is used in this review as the modifiability of some delirium risk factors in the palliative care context may vary, depending on factors such as the patients’ illness trajectory and goals of care. This evidence may also be used, in conjunction with that on non-modifiable risk factors, to develop predictive models of patient groups most likely to develop delirium. 11
This systematic review aimed to investigate risk factors for delirium in adult patients receiving specialist palliative care and address the research questions:
What possible risk factors for delirium have been measured in studies of adult patients receiving specialist palliative care?
What is the strength of association of identified risk factors with delirium incidence or prevalence in adult patients receiving specialist palliative care?
Methods
The protocol is registered on PROSPERO on 11.11.2019 (CRD42019157168). 13 The review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 14 Review guidance specific to observational studies of aetiology also informed its conduct. 15 The definition of a risk factor as, ‘A factor that is causally related to a change in the risk of a relevant health process, outcome or condition’ 16 was used.
Eligibility criteria
Eligibility criteria were framed according to PECO (Participants, Exposures, Comparators, Outcomes) criteria. 15 Eligible participants were adult patients (⩾18 years) receiving specialist palliative care services, including in-patient care in a hospice or hospital palliative care unit, palliative care consultation teams and specialist out-patient and community services. Studies needed to report the association of a possible risk factor with delirium incidence or prevalence, or data permitting its calculation.
Studies that included only risk markers per se (non-causal predictive factors e.g. educational level) were excluded. Eligible studies needed to report delirium diagnosis using Diagnostic and Statistical Manual (DSM) or International Classification of Diseases (ICD) diagnostic criteria or a diagnostic cut-off score on a validated assessment (diagnostic or screening) tool. Studies needed to compare occurrence of delirium in those exposed and not exposed to the potential risk factor.
Study designs eligible for inclusion included prospective and retrospective cohort studies, case-control, cross-sectional studies and randomised controlled trials. Case studies, case series, qualitative studies, opinion pieces and reviews were excluded. Studies published from 1980 onwards were included (when delirium was first included in DSM-III). 17 No language restrictions were imposed. Abstracts were excluded if no full text was available.
Study retrieval and selection
The following databases were searched: CINAHL, Cochrane Database of Systematic Reviews (CDSR), Embase, MEDLINE and PsycINFO. The search strategy was developed with a Health Sciences Information Specialist. Key terms were: ‘Palliative Care’ and ‘Delirium’. A validated search filter for palliative care was used with minor adaptations. 18 Delirium search terms were derived from recent relevant reviews.12,19 The search was conducted in June 2019 and updated in April 2020 using the full search and screening strategy (Supplemental File 1). A final rapid update (March 2021) was conducted using an accepted method 20 (single reviewer, MEDLINE only, as it was the source of 83% of included studies in previous searches). Reference lists of included studies, relevant reviews identified through the search and delirium guidelines were examined for additional eligible studies.
Search results were screened in two stages: title and abstract and full text screening, using Covidence software. 21 Two reviewers independently screened each result (IF, RW, JB, AH, PL) using Google Translate for non-English papers. At full text stage, reviewers selected a reason for exclusion from a hierarchical list. Where needed, translators, contacted through the Centre for Reviews and Dissemination (University of York), assisted in clarifying eligibility and enabling data extraction and risk of bias assessment. Disagreements were resolved through discussion to reach consensus or consultation with a third reviewer. When no full-text paper could be found, study authors were contacted.
Data extraction
Relevant data were extracted by one reviewer (IF) using a pre-piloted data extraction table in Excel 22 and checked by a second reviewer (RW) (See Supplemental File 2 for data extraction items). Delirium occurrence was recorded as: point prevalence (delirium at a time point, such as admission); period prevalence (delirium on admission and during study period); or incidence (new cases during study period).
Risk of bias assessment
Validity and risk of bias were assessed independently by two reviewers (IF, GR, RW) using a modified version of the Quality in Prognosis Studies (QUIPS) tool. 23 The following domains were assessed: study participation; attrition; risk factor measurement; confounding measurement and account; outcome measurement; analysis and reporting. Consensus on ratings was reached through discussion. QUIPS assessments were conducted only in relation to study data relevant to this review, therefore they should not be interpreted as assessments of the studies’ overall risk of bias per se. This informed decisions about whether study results should be included in meta-analysis; the narrative synthesis of results; and the GRADE (Grading of Recommendations Assessment, Development and Evaluation) 24 ratings of the evidence for each risk factor.
Data synthesis
Clinical and methodological heterogeneity were assessed to decide whether to conduct meta-analyses. Studies evaluating the same risk factor were assessed to determine the extent of variability in relation to participants and settings; measurement of the risk factor and delirium outcome, including type of delirium occurrence; study design; risk of bias; and whether only univariate or multivariate analysis was conducted. 25 Statistical heterogeneity was assessed using the I2 statistic. 26
The principal summary measures used in the review were odds ratios (95% confidence interval (CI)) for dichotomous risk factors and mean differences (95% CI) for continuous risk factors. 27 Data were transformed to present a common statistic across studies where possible.
Revman software 28 was used to conduct meta-analyses using a random effects model (DerSimonian and Laird inverse variance) due to heterogeneity between studies. 25 Where studies provided only the odds ratio and 95% confidence interval, the log odds ratio and standard error was calculated for all studies in the comparison and generic inverse variance was used for meta-analysis. 25 Forest plots were used to present the results. Subgroup analyses were conducted to explore heterogeneity in relation to the type of delirium occurrence measured (point prevalence, period prevalence, incidence).
Narrative synthesis was used when meta-analysis could not be conducted. Studies examining each possible risk factor were grouped, their characteristics tabulated, and a common statistic presented across studies where possible. Potential moderator variables, including measurement of the risk factor and delirium outcome, were examined and a narrative interpretive summary was produced. 29
GRADE assessment
The GRADE approach, 24 with guidance on its adaptation for reviews of prognostic factor research,30,31 was used to assess the certainty of the body of evidence for the association of each risk factor with delirium. Downgrading of the level of certainty was based on assessment of five domains (risk of bias, inconsistency, indirectness, imprecision and publication bias) and upgrading was based on large effects or exposure-response gradient. 24
Results
Study selection
Twenty eight studies reported in 30 articles were included (Figure 1). Three studies were each reported in two articles32–38, two studies were reported in one article. 39
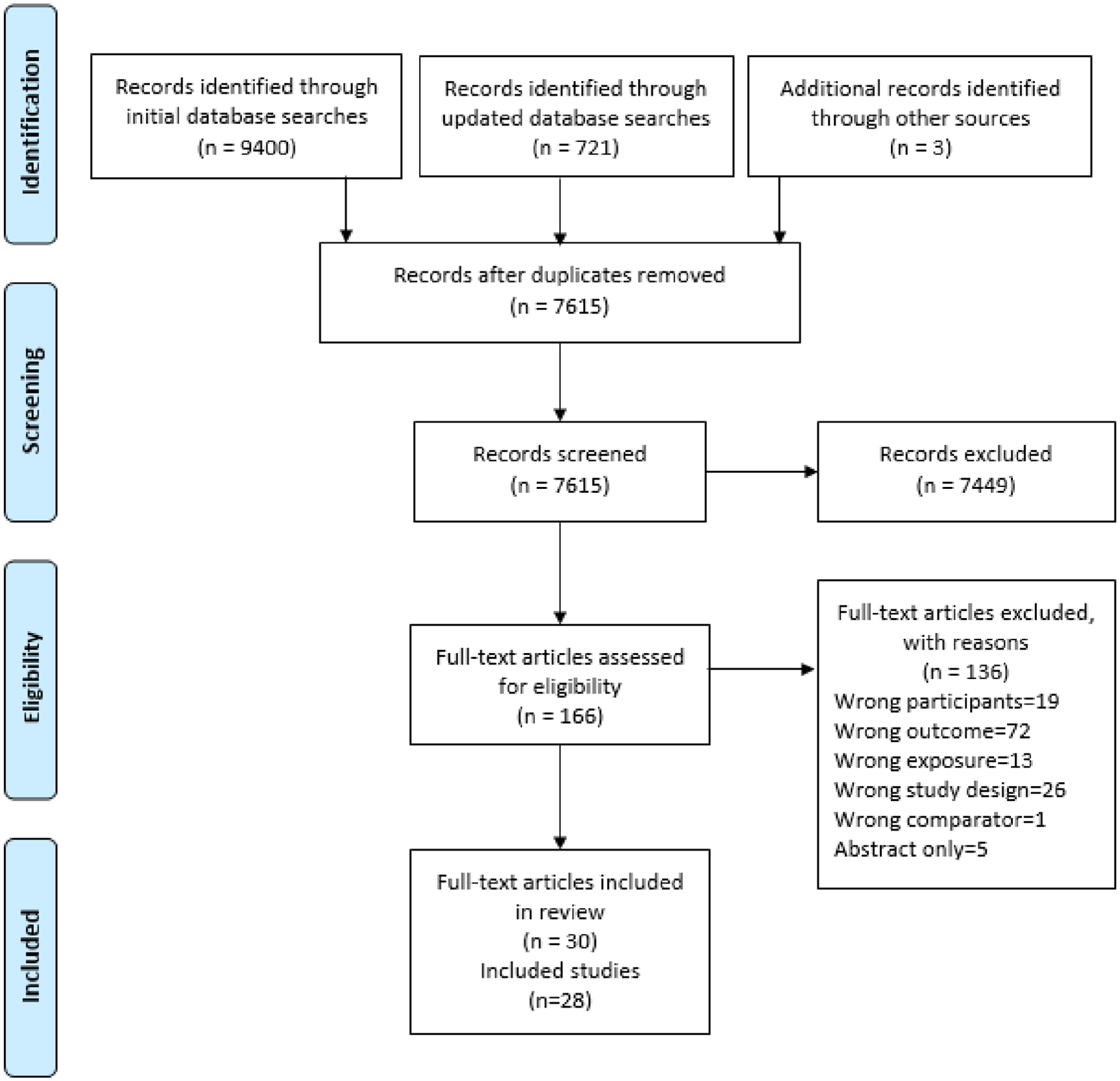
PRISMA diagram.
Study characteristics
Supplemental File 3 shows detailed study characteristics.
Included studies were from the USA (n = 7),37,40–45 Japan (n = 4),46–49 Italy32,33,50 and Spain (each n = 3),51–53 Canada,54,55 South Korea56,57 and the UK 39 (each n = 2) and Taiwan, 58 Germany, 59 Mexico, 60 Turkey 61 and Switzerland (each n = 1). 62 Twenty five studies were reported in English; two in Spanish52,53, one in Japanese. 47
Most studies included inpatient specialist palliative care units in hospitals (n = 21)32,37,39,41,42,44,46,48–53,55–62 or hospice (n = 5).33,39,47,51,54 Three studies each included palliative care consultation teams40,45,49 and palliative care community services33,41,43
In 23 studies, all participants had a primary cancer diagnosis,32,33,37,40–42,46–62 three studies included cancer and non-cancer diagnoses39,43,44, two studies did not report diagnoses.39,45 Participants in 24 studies were in the late stages of illness (e.g. advanced or terminal cancer),32,33,37,39–42,46–62 while in the remaining four studies participants’ stage of illness was unclear.39,43–45
In 14 studies, only cross-sectional data was eligible for the review.32,33,39,41,42,44,47,48,50,51,56,57,60 There were two prospective43,49, one retrospective 45 cohort studies (measuring delirium incidence); eight other prospective studies52–55,58,59,61,62, three retrospective chart reviews36,37,40 (measuring delirium period prevalence). Sixteen studies conducted only univariate analysis (for the data eligible for the review)37,39–42,44,48,51–55,57,58,60,61 and 12 also conducted multivariate analysis.32,33,39,43,45–47,49,50,56,59,62
Risk of bias within individual studies
Table 1 presents the ratings for the QUIPS risk of bias domains for individual studies.
QUIPS results.
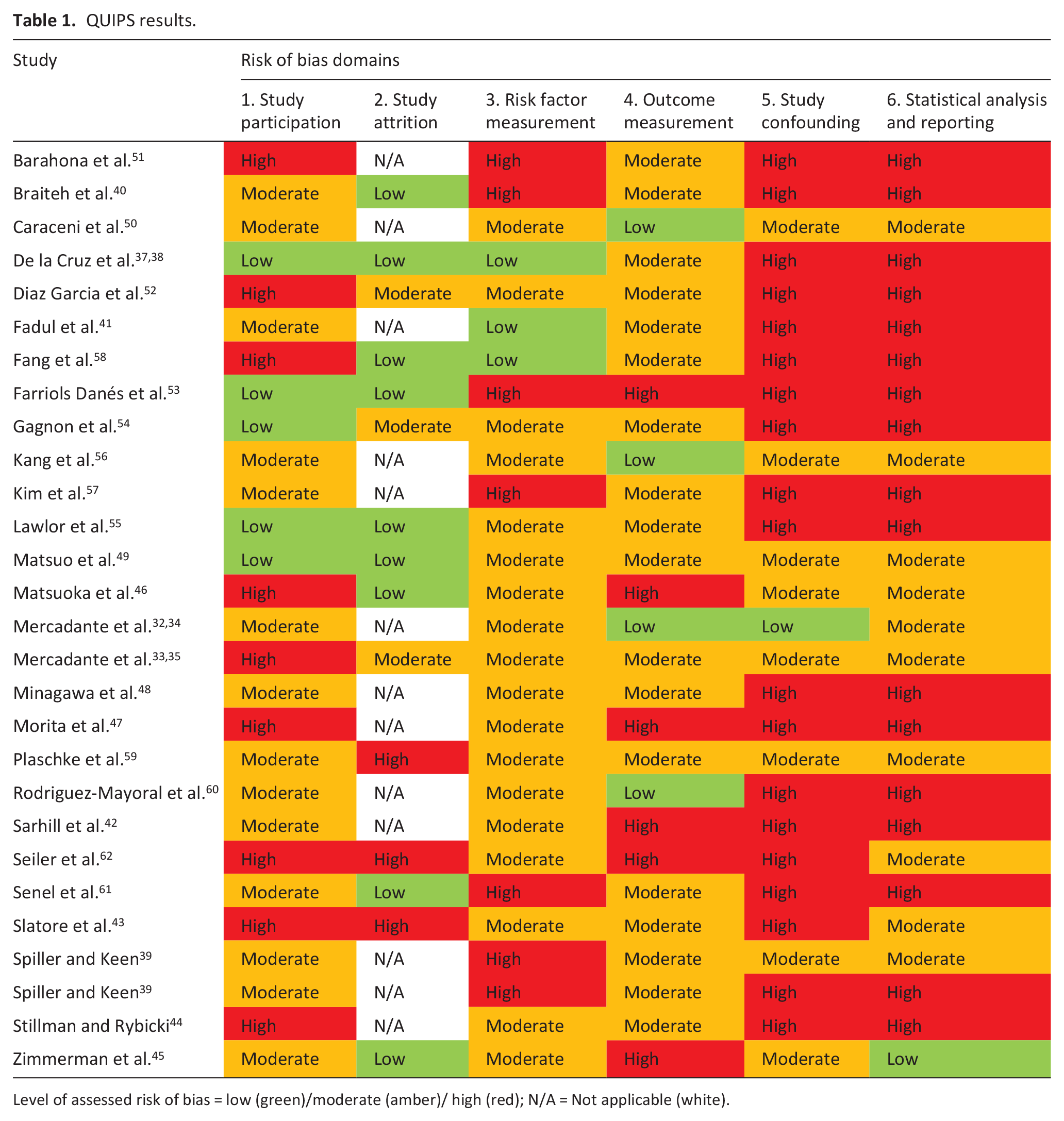
Level of assessed risk of bias = low (green)/moderate (amber)/ high (red); N/A = Not applicable (white).
Several studies excluded patients at high risk of delirium such as those with dementia/cognitive impairment (five studies46,52,56,59,61) and severely ill/dying patients (seven studies32,33,42,46,48,52,56).
Routine data on risk factors were often used and their measurement not clearly defined. The timing of exposure in relation to outcome measurement was unclear in many studies (cross-sectional or measuring delirium period prevalence).39,47,57,59,61,62 All included studies used validated delirium assessment tools or criteria but the methods and frequency of assessment were variable.
Sixteen studies included only univariate data on the association between risk factors and delirium, so made no adjustment for confounding.37,39–42,44,48,51–55,57,58,61 Many of the studies which conducted multivariate analysis had adjusted for some, but not all, important potential confounding factors.39,43,45–47,49,50,59,60,62
Several included studies selectively reported results, including six studies which only reported multivariate analysis results that were statistically significant.39,49,50,56,59,60
Potentially modifiable risk factors
Additional forest plots for study results included in meta-analyses are presented in Supplemental File 4. Due to heterogeneity between studies, most results could not be combined and are tabulated in Supplemental File 5.
Medications and treatment risk factors
Regarding opioid dose (n = 5), two studies54,56 reported higher mean opioid dose in the delirium group and one 57 reported a higher median dose, although these results were not statistically significant. Morita et al. 47 reported that higher opioid use (cut off unclear) was significantly associated with delirium and Mercadante et al. 33 reported a statistically significant correlation between opioid dose and delirium on admission.
All three studies examining ‘opioid toxicity’32,39reported a statistically significant positive association with delirium.
In univariate analysis, Şenel et al. 61 reported a statistically significant positive association between polypharmacy (more than three drugs) and delirium period prevalence (unadjusted OR 26.39, 95% CI 12.70, 54.82).
Physiological risk factors

Forest plot: ESAS lack of appetite and delirium point prevalence (mean difference).
One study each reported statistically significant associations of numbness 47 and pressure sores 62 with delirium.
Symptom risk factors
(Reported in order of ESAS, except loss of appetite reported in nutrition-related risk factors above)

Forest plot: ESAS pain score and delirium point prevalence on admission (mean difference).

Forest plot: ESAS sleep disturbance and delirium point prevalence (mean difference).
Behavioural disorders
Association of smoking, 56 alcohol misuse 32 and substance use disorder 62 with delirium were examined in one study each and no statistically significant associations were found.
Performance status, illness severity and prognostic assessments
Eighteen studies reported that lower performance status was strongly associated with delirium, using either Karnofsky Performance Status (eight studies) 32,33,44,48,50,53,59,60; Eastern Cooperative Oncology Group (ECOG) Performance Status (seven studies)37,39,46,49,56,57,60 or the Palliative Performance Scale (five studies).47,49,51,52,61 One study 61 reported a statistically significant positive association between immobilisation and delirium period prevalence in univariate analysis.
Two studies found no significant difference in Charlson Comorbidity Index scores.52,62 One study 45 found no statistically significant association between illness severity (APACHE III) and delirium incidence; while one study each found that admission for end of life care 32 and higher palliative prognostic index scores 61 were associated with delirium.
Non-modifiable risk factors
Additional forest plots for study results included in meta-analyses are presented in Supplemental File 6. Results are tabulated in Supplemental File 7.
Age
(n = 18). Meta-analysis of mean difference in age reported by nine studies suggested that participants with delirium were on average 3.08 (95% CI 1.01, 5.16) years older than those without delirium (Figure 5).32,33,44,53,55,56,59,61,62 This was higher in studies measuring delirium point prevalence (5.62 years, 95% CI 2.97, 8.27 years). Unadjusted odds ratios from six studies45–47,49,50,62 and adjusted odds ratios from four studies33,45,46,56 report either a small association of older age with delirium or no significant association.
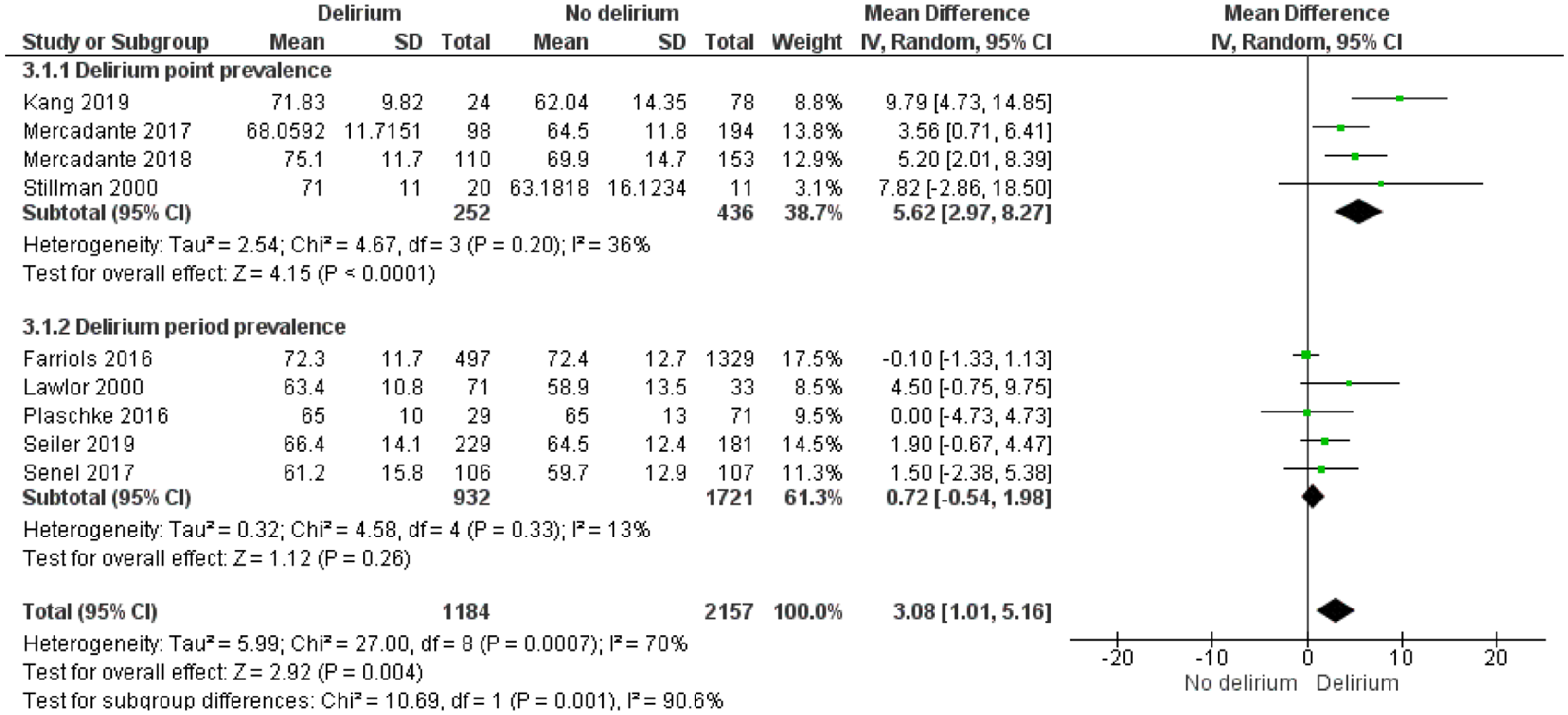
Forest plot: age (years) and delirium (mean difference).
Sex
(male/female) (n = 18). The summary unadjusted odds ratio from 15 studies suggests that male palliative care patients were slightly more likely to have delirium than female patients (OR 1.39, 95% CI 1.23, 1.57) (Figure 6).32,33,37,44,50,52–59,61,62 Results of three further studies not included in meta-analysis were consistent with this.46,48,49
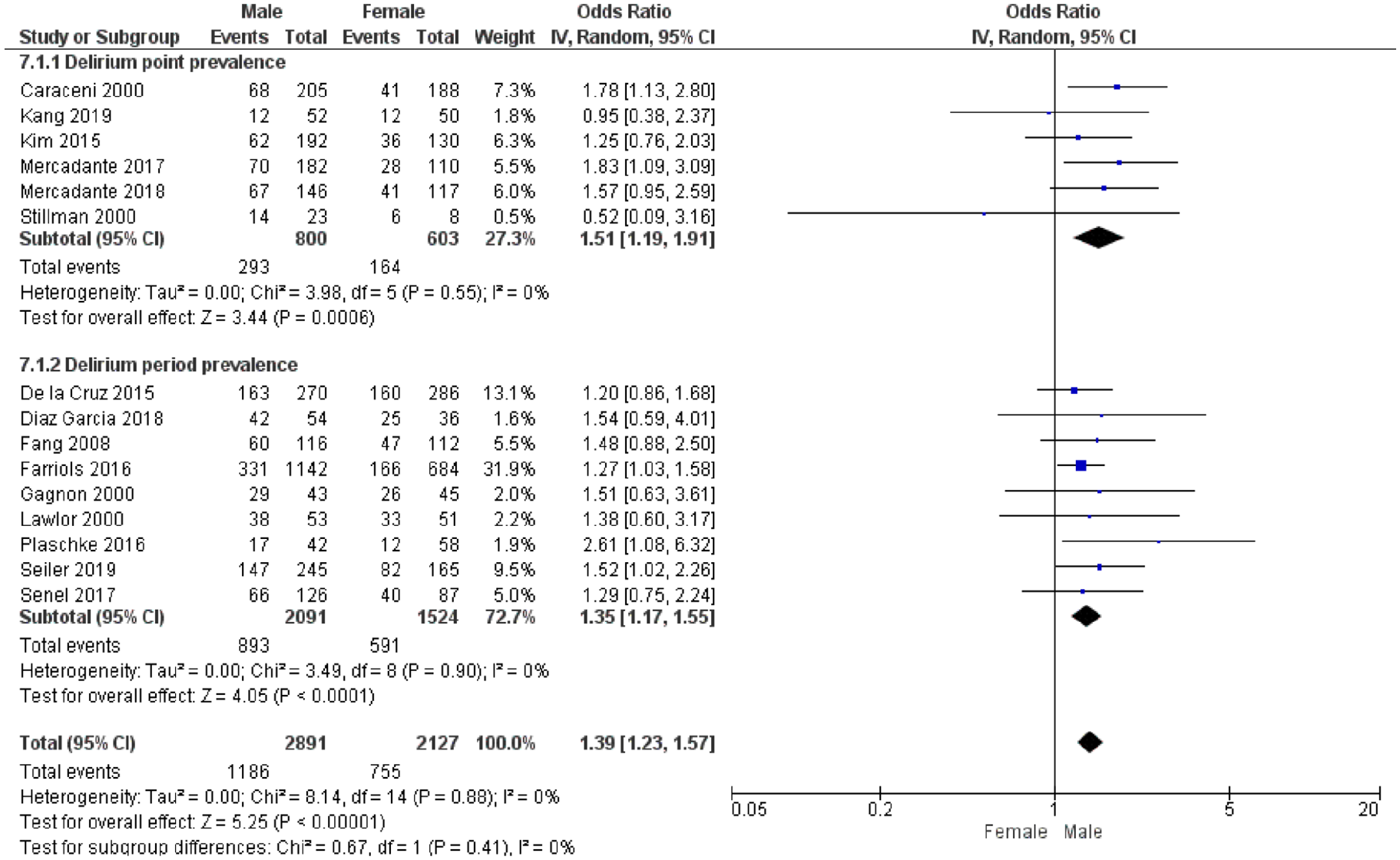
Forest plot: sex (male/female) and delirium (unadjusted OR).
Cancer-related risk factors
Three cancer-related risk factors were examined in this review: lung cancer (n = 12); brain cancer/ brain metastases (n = 12) and metastases (overall) (n = 4). Patients with lung cancer may be slightly more likely to have delirium than those without (pooled OR 1.29, 95% CI 0.99, 1.68) (Supplemental Files 6 and 7).32,33,48–50,52,53,55–58,62
Twelve studies examined the association between primary brain cancer and/or brain metastases and delirium.42,45,47–50,52,53,55,58,61,62 Positive associations were found in meta-analyses of univariate analyses between delirium and primary brain cancer (OR 2.01, 95% CI 0.98, 4.14)52,53,62 and brain metastases (OR 3.16, 95% CI 1.85, 5.40)42,47,48,50 (Supplemental File 6). Seiler et al. 62 found a positive association with primary brain cancer in multivariate analysis (OR 3.63, 95% CI 1.03, 12.77). Three further univariate analyses of brain metastases, from studies not included in meta-analysis,45,49,58, two studies that combined primary brain cancer and brain metastases as a single risk factor,55,61 reported mixed results.
Seven studies reported positive associations bet-ween other neurological/ cerebral risk factors and delirium.39,40,44,46,51,61,62 As these were defined in different ways they could not be combined for meta-analysis. One study each reported a statistically significant association of ‘neurological diseases’ 61 ; ‘cerebral disease’ 39 ; ‘focal neurological deficit’ 44 and ‘myoclonus’ 40 with delirium.
In meta-analysis of univariate data from four studies, presence of metastases (overall) was not associated with delirium period prevalence (OR 0.83, 95% CI 0.66, 1.05) (Supplemental File 6).52,53,55,61
GRADE assessment of the certainty of the evidence for risk factors’ association with delirium
The certainty of the evidence for the following risk factors was graded as low: gender, lung cancer, metastases (overall), primary brain cancer, performance status, opioid use, dehydration, infection and drowsiness. For all other risk factors, certainty was rated as very low (Supplemental File 8). The evidence for most risk factors was downgraded for risk of bias, based upon the QUIPs assessments and lack of adequate adjustment for confounding factors in analysis. The evidence for many risk factors was also downgraded for inconsistency, due to unexplained heterogeneity between study results, and for imprecision of the results. 24
Discussion
Main findings
We found that the evidence from 28 included studies regarding the association of possible risk factors with delirium in adults in palliative care settings was limited, particularly for many potentially modifiable risk factors, and was of low or very low certainty.
In relation to potentially modifiable risk factors, there is evidence of positive associations between delirium and both opioids and lower performance status and suggestive evidence for dehydration, hypoxaemia, sleep disturbance, liver dysfunction and infection. Positive associations with delirium were reported in only one study for each of the following: polypharmacy, sensory impairment, immobility, pressure sores and indwelling catheter use.
There was more mixed evidence about the association of delirium with pain, dyspnoea, anticholinergics, drowsiness, anxiolytics/ hypnotics, steroid use, constipation and nutrition-related risk factors.
In relation to non-modifiable risk factors, the evidence suggests positive associations of delirium with older age; male sex; primary brain cancer or brain metastases and lung cancer.
Strengths and limitations of the review
To our knowledge, this is the first systematic review conducted of risk factors for delirium in palliative care settings. Rigorous review methods were used. Particular strengths were the inclusion of studies that only used validated delirium assessment tools or criteria; inclusion of non-English language papers; screening and risk of bias assessment conducted by two independent reviewers and GRADE assessment of the certainty of evidence for each risk factor. 24
Most included studies were not high quality cohort studies comparing delirium incidence between those exposed/ not exposed to the risk factor. Identifying delirium risk factors was not the primary aim of most included studies. Many provided only cross-sectional data, or measured delirium period prevalence, so timing of risk factor exposure in relation to delirium development was unclear. Little evidence was reported on several potentially modifiable risk factors recommended in delirium risk reduction guidelines.64,65
Delirium can result from a complex interplay between multiple risk factors 5 and this was not adequately accounted for in the included studies which mostly used only univariate analyses. Due to the multiple risk factors for delirium, it is difficult to account for all potential confounding and, as Zaal et al. 9 (p. 69) noted, ‘It is poorly established which confounders should be incorporated in multivariable risk factors models’ for delirium. Multivariate analysis adjusted for some, but not all, potentially important confounding factors. For example, those examining associations between pain and delirium did not adjust for opioid use.
We separately reported the results for those risk factors that are clearly non-modifiable (e.g. age, sex) and those which may potentially be modifiable. However, what is modifiable is uncertain, for example, it might not be possible to modify risk factors such as liver and renal dysfunction and performance status. In palliative care contexts, the modification of many risk factors may not be possible due to factors such as the patient’s stage of illness and their goals of care. 11
Most studies in this review were conducted in in-patient palliative care settings with participants with late-stage cancer, so results may be less generalisable to other patients receiving palliative care services. The definition of the eligible population as patients in receipt of specialist palliative care services could be clearly operationalised to conduct this review. However, it led to the exclusion of some possibly relevant studies, such as those of delirium risk factors for terminally ill patients in the general hospital setting.66,67
What this study adds
Delirium guidelines, not specific to palliative care contexts, such as NICE 64 and SIGN, 65 and systematic reviews of multicomponent interventions,6,7 recommend delirium risk reduction through targetting modifiable risk factors. The evidence from this review suggests positive associations between delirium and opioid use, higher opioid dose and toxicity in palliative care settings. This supports the importance of medication review and use of the minimum effective dose, in line with delirium guidelines.64,65 The limited evidence of associations of other modifiable risk factors with delirium, provides some support for targetting risk factors included in guidelines and interventions from other settings,6,7,64,65 including dehydration, hypoxaemia, sleep disturbance and infection, to reduce delirium in palliative care.
The low or very low certainty of the evidence must be taken into account in drawing clinical implications from our findings. Several potentially modifiable risk factors targetted in guidelines and interventions from other settings,6,7,64,65 including sensory impairments, mobility, catheter use and polypharmacy, were each examined in only one study, which reported positive associations with delirium. A systematic review found these to be statistically significant risk factors for delirium incidence for older hospitalised patients. 8 We found mixed evidence regarding several other risk factors- pain, constipation and nutrition- which are commonly targetted in delirium prevention strategies. This highlights the need for further, high quality research focussed on the association of potentially modifiable risk factors with delirium in palliative care settings.
Although performance status was strongly associated with delirium in this review, it is not a single modifiable risk factor. It could be useful, in conjunction with evidence on other modifiable/non-modifiable risk factors, in developing predictive models of patient subgroups most likely to develop delirium. In relation to non-modifiable risk factors, this review’s results support the association between older age and delirium found in other settings.8,9 Associations between delirium and male sex, brain cancer/metastases and lung cancer were also identified in palliative care contexts. Notably, dementia, which is strongly associated with delirium in other settings,8,9 was only examined by one study in this review. However, as delirium prevalence in palliative care patients is very high (58%– 88% in the last weeks of life), 1 it is arguably more of a priority to develop population-level preventative interventions targetting modifiable risk factors, than to predict subgroups of patients at elevated risk in order to target interventions for them.
In treating an established episode of delirium, modifiable causes are also targetted (in accordance with the patient’s goals of care), to attempt to reduce the length and severity of the episode. A study in an acute palliative care unit found 49% of delirium episodes could be reversed. 55 Although the primary focus of our review was on factors affecting the risk of developing delirium, its findings could also be used to inform further research to identify modifiable factors to target in delirium treatment. Several additional studies have investigated delirium reversibility through systematic investigation of multiple precipitating risk factors in palliative care patients who have developed delirium.55,68–70 Their data were excluded from this review because they did not include a comparator group without delirium, but may be informative in research to identify factors associated with delirium reversibility.
Conclusion
The limited evidence from this systematic review offers some support for the use of interventions that target modifiable risk factors to reduce the risk of delirium for palliative care patients. However, there is a need for high quality prospective cohort studies with more comprehensive and robust delirium risk factor measurement along with adequate adjustment for important confounding factors through multivariate analysis. This will enable much greater certainty in the evidence regarding the strength of the association of different risk factors with delirium, to inform the design of multicomponent interventions to reduce risk of delirium, and clinical decision-making regarding competing risks, in the palliative care context.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211065278 – Supplemental material for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211065278 for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis by Imogen Featherstone, Trevor Sheldon, Miriam Johnson, Rebecca Woodhouse, Jason W Boland, Annmarie Hosie, Peter Lawlor, Gregor Russell, Shirley Bush and Najma Siddiqi in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163211065278 – Supplemental material for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-pmj-10.1177_02692163211065278 for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis by Imogen Featherstone, Trevor Sheldon, Miriam Johnson, Rebecca Woodhouse, Jason W Boland, Annmarie Hosie, Peter Lawlor, Gregor Russell, Shirley Bush and Najma Siddiqi in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163211065278 – Supplemental material for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis
Supplemental material, sj-pdf-3-pmj-10.1177_02692163211065278 for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis by Imogen Featherstone, Trevor Sheldon, Miriam Johnson, Rebecca Woodhouse, Jason W Boland, Annmarie Hosie, Peter Lawlor, Gregor Russell, Shirley Bush and Najma Siddiqi in Palliative Medicine
Supplemental Material
sj-pdf-4-pmj-10.1177_02692163211065278 – Supplemental material for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis
Supplemental material, sj-pdf-4-pmj-10.1177_02692163211065278 for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis by Imogen Featherstone, Trevor Sheldon, Miriam Johnson, Rebecca Woodhouse, Jason W Boland, Annmarie Hosie, Peter Lawlor, Gregor Russell, Shirley Bush and Najma Siddiqi in Palliative Medicine
Supplemental Material
sj-pdf-5-pmj-10.1177_02692163211065278 – Supplemental material for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis
Supplemental material, sj-pdf-5-pmj-10.1177_02692163211065278 for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis by Imogen Featherstone, Trevor Sheldon, Miriam Johnson, Rebecca Woodhouse, Jason W Boland, Annmarie Hosie, Peter Lawlor, Gregor Russell, Shirley Bush and Najma Siddiqi in Palliative Medicine
Supplemental Material
sj-pdf-6-pmj-10.1177_02692163211065278 – Supplemental material for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis
Supplemental material, sj-pdf-6-pmj-10.1177_02692163211065278 for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis by Imogen Featherstone, Trevor Sheldon, Miriam Johnson, Rebecca Woodhouse, Jason W Boland, Annmarie Hosie, Peter Lawlor, Gregor Russell, Shirley Bush and Najma Siddiqi in Palliative Medicine
Supplemental Material
sj-pdf-7-pmj-10.1177_02692163211065278 – Supplemental material for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis
Supplemental material, sj-pdf-7-pmj-10.1177_02692163211065278 for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis by Imogen Featherstone, Trevor Sheldon, Miriam Johnson, Rebecca Woodhouse, Jason W Boland, Annmarie Hosie, Peter Lawlor, Gregor Russell, Shirley Bush and Najma Siddiqi in Palliative Medicine
Supplemental Material
sj-pdf-8-pmj-10.1177_02692163211065278 – Supplemental material for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis
Supplemental material, sj-pdf-8-pmj-10.1177_02692163211065278 for Risk factors for delirium in adult patients receiving specialist palliative care: A systematic review and meta-analysis by Imogen Featherstone, Trevor Sheldon, Miriam Johnson, Rebecca Woodhouse, Jason W Boland, Annmarie Hosie, Peter Lawlor, Gregor Russell, Shirley Bush and Najma Siddiqi in Palliative Medicine
Footnotes
Acknowledgements
The authors thank Kath Wright (Information Service Manager, Centre for Reviews and Dissemination, University of York) for her essential contribution to the electronic database search. We also thank David Marshall and Mami Meader for their valuable support in translating the Spanish and Japanese papers respectively.
Authorship
IF, TS, MJ, RW, JB, AH, PL, GR, SB and NS made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data. IF, RW, JB, AH and PL screened papers for inclusion in the review. IF, GR and RW conducted risk of bias assessment. IF drafted the article and all other authors revised it critically. All authors approved the version to be published.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: PL authored a paper included in this review but he did not contribute to risk of bias assessment of the included studies. The authors declared no other potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/ or publication of this article: Imogen Featherstone is funded by a National Institute for Health Research (NIHR) Doctoral Fellowship [DRF-2017-10-063] for this research project. This paper presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Ethical approval
No ethical approval was required for this research, as it was a review of existing published articles with no new primary data collected.
ORCID iDs
Data management and sharing
All of the papers included in this review are available through their respective journals.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.