
Abstract
Background:
Palliative care is advocated for older people with frailty and multimorbidity in the community. However, how to best deliver it is unclear.
Aim:
To develop and model an intervention of short-term specialized palliative care that is initiated timely based on complex care needs and integrated with primary care for older people with frailty and their family, detailing the intervention components, outcomes and preconditions needed for implementation, using a novel theoretical approach.
Design:
Observational study informed by the UK MRC guidance for complex interventions integrated with a Theory of Change (i.e. hypothetical causal pathway to impact) approach. We synthesized evidence from a systematic review, semi-structured interviews, group discussions and Theory of Change workshops.
Setting:
Primary care in Flanders, Belgium.
Results:
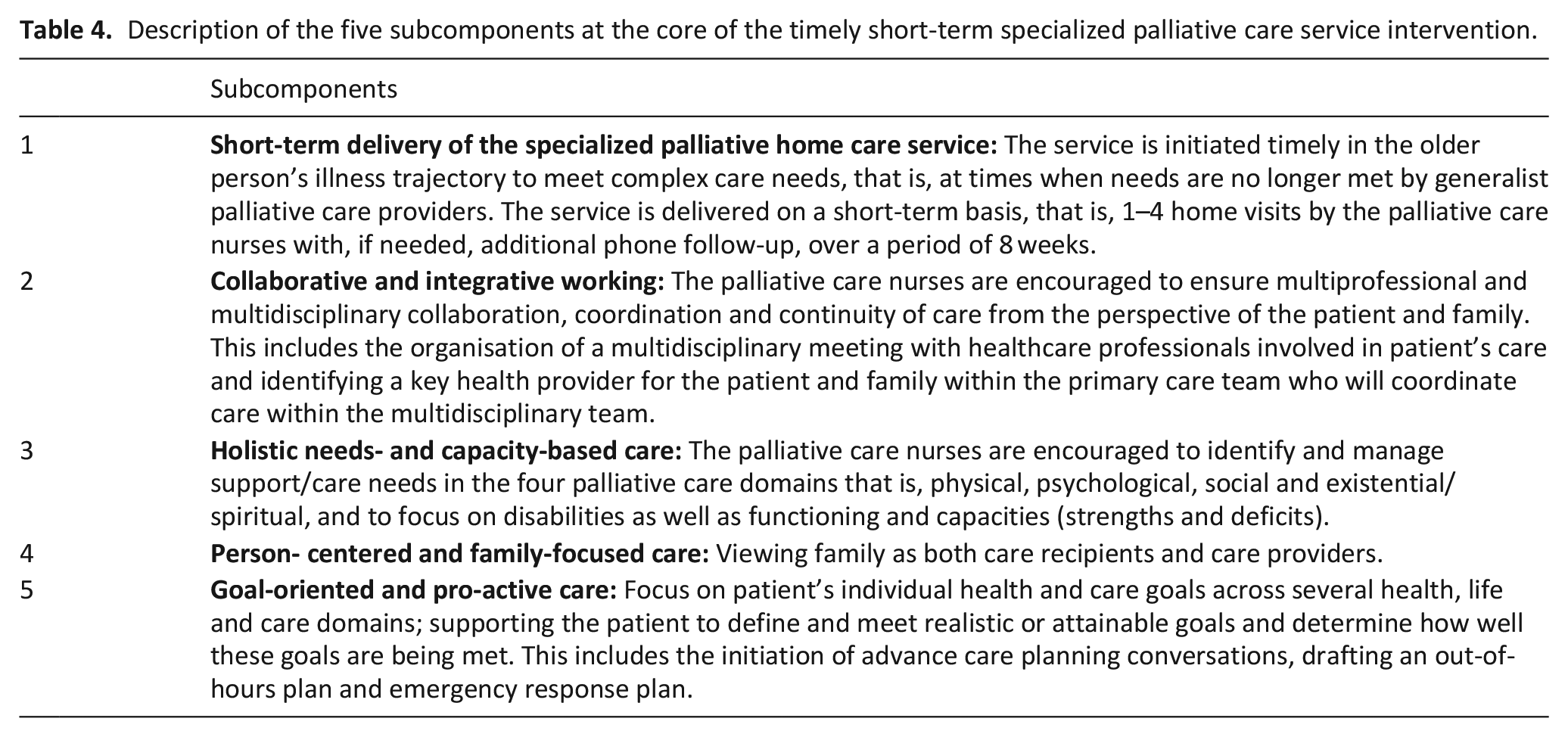
We identified patient and family carer-related long-term outcomes and preconditions to achieve them for example, service providers are willing and able to deliver the intervention. The intervention components included implementation components, for example, training for service providers, and a core component, that is, provision of timely short-term specialized palliative care by a specialized palliative home care nurse. The latter includes: short-term service delivery; collaborative and integrative working within primary care; delivery of holistic needs- and capacity-based care; person-centred and family-focussed; and goal-oriented pro-active care.
Conclusions:
The Theory of Change approach allowed us to identify multiple intervention components targeting different stakeholders to achieve the desired outcomes. It also facilitated a detailed description of the intervention which aims to increase replicability and effective comparisons with other interventions.
Timely short-term specialized palliative care service interventions have been advocated for older people with frailty and multimorbidity with complex care needs in the community.
It remains unclear what these interventions entail and how or under what circumstances such interventions can best be implemented.
We identified the different stakeholders that should be involved when aiming to improve care for older people with frailty with complex care needs in the community, and determined multiple preconditions (e.g. older people are identified in a timely manner according to prespecified criteria), and intervention components (e.g. delivery of short-term service, collaborative and integrative working, holistic needs- and capacity-based care, person-centred and family-focused and goal-oriented and pro-active care) needed to achieve the desired changes.
Alongside more traditional outcomes in palliative care research such as addressing holistic needs and symptoms, we identified sense of security in care as an outcome important to and valued by older people and family carers.
Following expert input from stakeholders, we integrated care approaches from different disciplines into the core of the intervention, such as combining palliative care with geriatric and rehabilitative care, and integration of goal-oriented pro-active care with advance care planning.
The Theory of Change of the intervention provided insight into the hypothetical causal pathway to achieve long-term outcomes and impact. This in-depth knowledge is needed to better understand how the intervention is likely to work in practice and how to evaluate implementation when delivered.
This Theory of Change approach could serve as an example for researchers of how to build a programme theory of their intervention.
Detailed reporting of the intervention will enable researchers and clinicians to replicate the intervention and to compare our intervention with others more effectively.
Introduction
As people live longer, many experience long periods of multimorbidity or frailty.1,2 Different conceptualisations are used to describe frailty; some primarily focus on the physical/medical domain of frailty, particularly in the field of geriatrics, others tend to be broader and also include other domains such as the psychological and social, particularly in the social sciences.3,4 In this study, we focused on the medical syndrome of frailty and described frailty as an age-related clinical condition, typically with deterioration in the physiological capacity of several organ systems, that causes an increased susceptibility to stressors.3,5 Older people with frailty often experience a prolonged period of gradual decline that is punctuated by stressor events (e.g. acute illness) resulting in fluctuating palliative care needs in the last years of life.1,3,6 Palliative care is indicated for addressing these needs. It encompasses generalist palliative care (i.e. provided by health professionals with a good basic knowledge of palliative care) and specialized palliative care services (i.e. provided by a multidisciplinary service or a clinician specifically trained in palliative care for patients with complex problems, and by family carers). 7 Timely integration of these services has been suggested to meet complex palliative care needs. This means initiation of specialized palliative care at times when needs cannot be addressed by generalist palliative care providers alone.8,9 Although there is no standard definition of complex needs in palliative care, it is recognized that they can affect different domains, that is, physical, psychological, social or spiritual/existential. 10 Despite the fact that the need for timely integration of services has been recognized, research shows that these services are often initiated only shortly before death (e.g. the median number of days ranged from 15 in Belgium to 30 in Italy in a four-country comparison). 11 This is particularly the case for older people with frailty, who typically have an unpredictable disease trajectory that makes prognostication difficult. 12 Integration of specialized palliative care services is particularly relevant in primary care, as the majority of older people prefer to remain in their usual residence (e.g. home). 13
A model of short-term integrated palliative and supportive care for older people with frailty in community settings in England has recently been developed aiming to provide timely short-term specialized palliative care services. 14 The intervention intends to deliver specialized palliative care during episodes of decline and complex symptom presentation and aims to facilitate integrated working between the specialized palliative care teams and existing community care providers (e.g. GPs and community nurses), involved in patient’s care. 14 It foresees short-term delivery of the palliative care services, through one to three visits over a period of 3 months. 14 While it has been argued that such a model has potential benefit for older people and family carers, it remains unclear what this intervention entails, and how or under what circumstances it can best be implemented.
A major reason for this lack of clarity is the difficulty of describing a complex intervention in full detail. Most interventions in palliative care are complex interventions. They consist of several interacting components situated at different levels and interacting with contextual barriers and facilitators. 15 The established guidance on complex interventions of the UK Medical Research Council (MRC) states that theoretical underpinning is needed when developing and evaluating complex interventions, to be able to understand the role of different components, their link to the desired outcomes and the hypothesized causal pathway of their effects.15,16 In the absence of specific guidance concerning choice of theoretical models, we used the Aspen Institute’s Theory of Change approach 17 which has rarely been used in the field of palliative care research. 18 Following the accepted definition of the Aspen Institute, a Theory of Change is defined as ‘a theory of how and why an initiative works which can be empirically tested by measuring indicators for every expected step on the hypothesized causal pathway to impact’.17,19 Such a programme theory is developed specifically for a given intervention based on current evidence and in collaboration with stakeholders using backwards-mapping processes. 17 The process starts with defining the impact and long-term outcomes (i.e. the outcomes that the intervention is able to change on its own) of the intervention and works backwards to determine the preconditions or intermediate outcomes to achieve the long-term outcomes. It then identifies intervention components needed to achieve the outcomes, the rationale behind them, and assumptions that must exist for them to be achieved. The specific objective of this work is to describe the hypothesized causal pathway or Theory of Change of a timely short-term specialized palliative care service intervention for older people with frailty with complex needs and their family carers in primary care.
Methods
Study design and setting
We applied an observational study design combining multiple qualitative data methods in a serial way informed by the UK MRC guidance to develop complex interventions 15 integrated with a Theory of Change approach. 17 We developed a Theory of Change of a timely short-term specialized palliative care service intervention (henceforth named the Frailty+ intervention) by synthesizing evidence from a systematic review on specialized palliative care services for older people in primary care, 20 findings from qualitative interviews and group discussions with patients and family carers, and Theory of Change participatory workshops with professional stakeholders. The different methods used and the synthesis process for developing and modelling the Theory of Change are described in Figure 1. The Theory of Change is visualized in a map and uses specific terminology described in Table 1. The intervention was developed over a 2-year period (Sept 2017 – Sept 2019). The qualitative interviews, group discussions and Theory of Change workshops were conducted in Flanders, the Dutch-speaking region of Belgium.
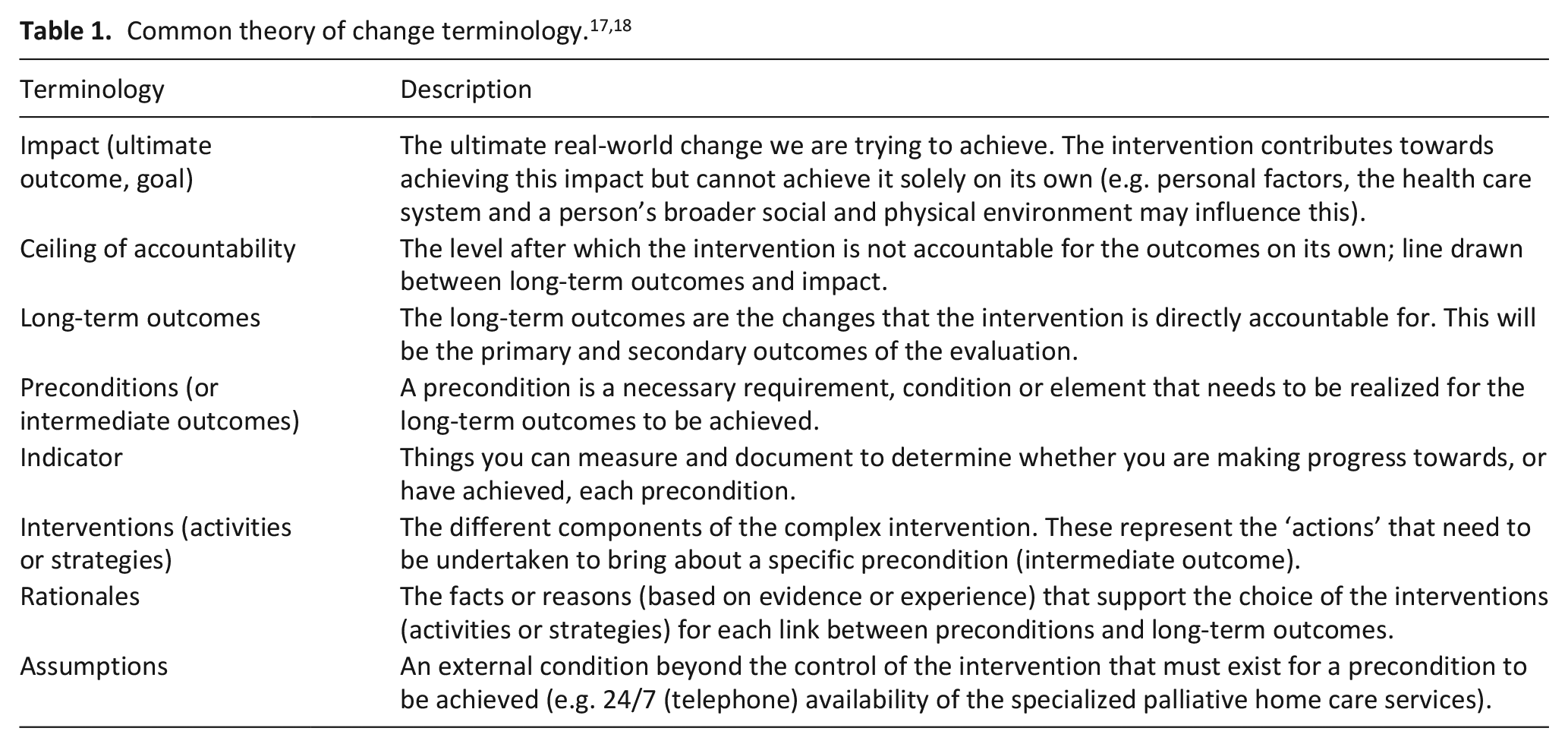
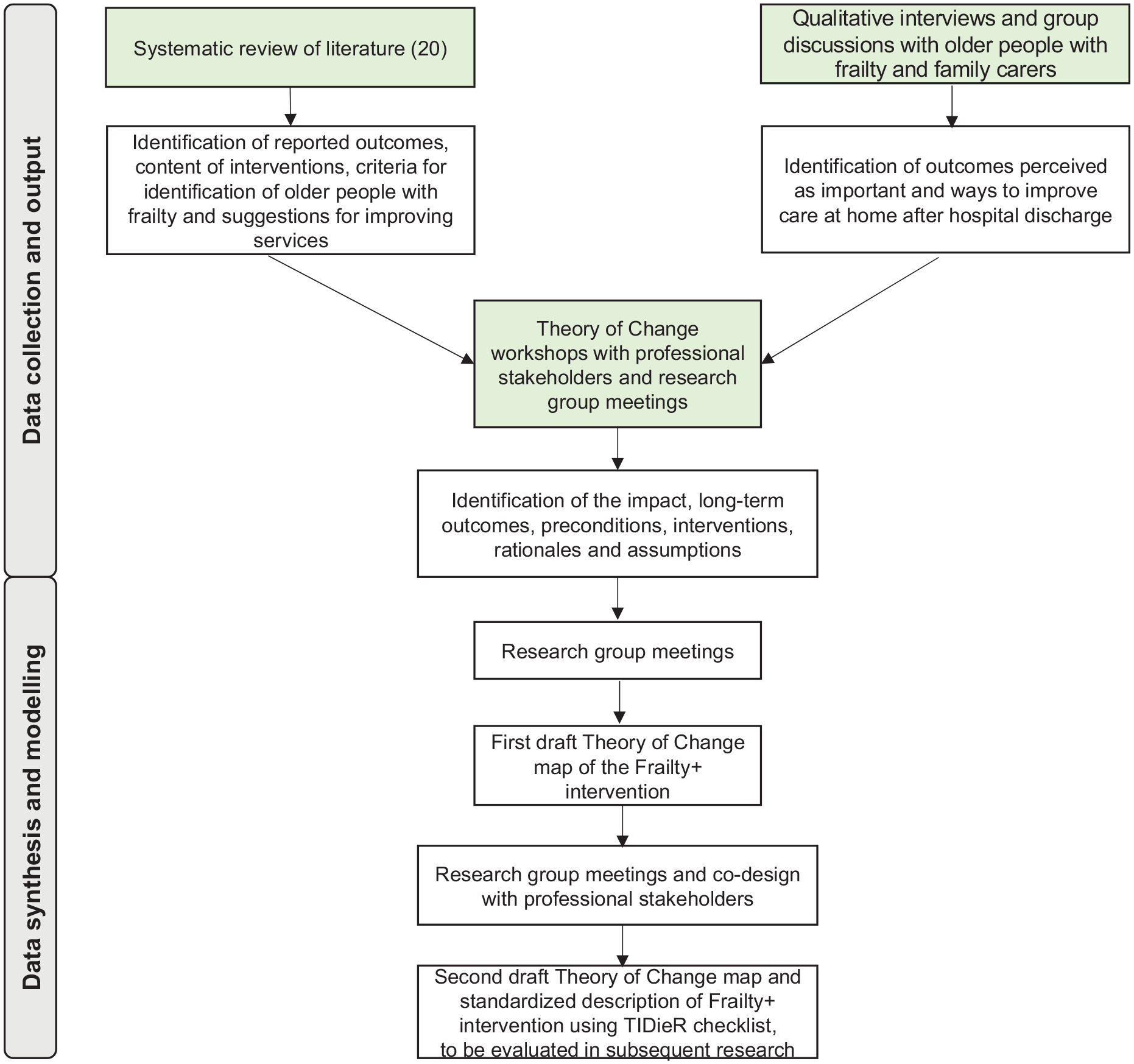
Diagram of information sources and synthesis process for developing the Theory of Change of the Frailty + intervention.
For reporting, we followed the Consolidated criteria for Reporting Qualitative research checklist, 21 the guidance for the reporting of intervention development 22 and the Template for Intervention Description and Replication (TIDieR) checklist. 23
Population and sampling
Qualitative interviews and group discussions
We conducted individual semi-structured face-to-face interviews with older people and face-to-face group discussions involving older people and family carers. For the qualitative interviews, we purposefully selected a heterogeneous sample of older people using the following inclusion criteria: (1) had a functional impairment AND (2) had been hospitalized at least once in the past 2 years (for any reason). The same criteria were used to select a sample of older people for the group discussions. We used the following exclusion criteria: (1) person not living at home OR (2) person with impaired cognition that prevented participation. We also included family members in the group discussions and included those to whom the following applied: (1) a family carer of a person with a functional impairment AND (2) a family carer of a person who had been hospitalized at least once in the past 2 years (for any reason).
Theory of change workshops with professionals
We held Theory of Change workshops with professional stakeholders (e.g. researchers, policymakers and healthcare professionals). They were purposively sampled using the following criteria: (1) providing formal care (i.e. paid care services) to older people in any setting OR working in healthcare management, policy organizations or research that concerns care for older people, AND (2) having experience in palliative care through their professional work. Stakeholders could attend one or several workshops, because each of the workshops aimed for discussion and consensus on different elements of the Theory of Change map and constituted an iterative refinement of previous draft of the map, following relevant guidance.17,19
Recruitment
Qualitative interviews and group discussions
Participants of the group discussions were recruited from a public welfare centre and among day-care clients in a nursing home in Flanders. The coordinator of the centre approached eligible participants and asked whether they would be interested in participating. The first participants meeting the inclusion criteria who agreed were included. For the interviews, we recruited participants from a University Hospital (Ghent University Hospital) in Flanders. They were first approached by their treating physician (NVDN) and, if they agreed, visited by a researcher during their hospital admission. The interviews were part of the multiple methods we combined to develop the theoretical model of the intervention. Our aim was not to reach data saturation but to ensure that the input of older people was included in the development process. We have therefore included a smaller sample than would likely be required to reach saturation.
Theory of change workshops with professionals
The research team identified stakeholders who met the inclusion criteria through the personal network of the research and clinical team supervising the study. The stakeholders were approached by the researcher (KdN) via email or phone regarding their participation in the workshop.
Data collection
Qualitative interviews and group discussions
All interviews were conducted face-to-face by the researcher (KdN) and the group discussions were conducted face-to-face by three researchers (KdN, LP and YP). We used case vignettes to prompt participants to explore which outcomes of care are important to them and how to improve care at home after hospital discharge. The use of vignettes provides a way of exploring possible sensitive topics without obliging participants to share personal experiences. 24 Participants were invited to reflect on the case vignettes and the possible role of a specialized palliative home care service in the situation described in the vignettes. All interviews and group discussions were audio-recorded.
Theory of change workshops with professionals
The Theory of Change workshops were conducted face-to-face and facilitated by the researchers (KdN, LP, LVdB), in which we determined the elements of the Theory of Change map. 17 The workshop guide was developed based on the findings of the interviews and group discussions. We started with an introduction of the researchers, the project and the method. The workshops followed a structured format (see Supplemental Table 1). The procedure we used to create a Theory of Change map is called ‘backwards outcome mapping’. This means that participants first identified the desired impact and long-term outcomes of the timely short-term specialized palliative care service intervention. Subsequently, they ‘worked backwards’ through identifying preconditions or intermediate outcomes that are needed to achieve the long-term outcomes. 25 We used the findings of the systematic review and qualitative research to guide the discussion. We asked questions concerning the identified themes, used the themes to inform and stimulate the discussion and as prompts to resolve discrepancies, while allowing for new themes to emerge. After each workshop, the researcher (KdN) created a draft Theory of Change map and discussed this during meetings with the research team (consisting of social science researchers, a general practitioner and a hospital geriatrician, all with experience in palliative care). The map was then presented in the next workshop. After the workshops, the research team discussed and reviewed the formulation and content of the different parts of the Theory of Change map. All workshops were audio-recorded.
Data analysis and integration
The researcher (KdN) analysed the qualitative interviews and group discussions in MS Excel using directed content analysis 26 and discussed this with the research team. The analysis followed a partly deductive and partly inductive coding approach. The interview transcripts were deductively coded in accordance with the pre-determined coding scheme that was based on the two key areas explored across the interviews and discussions, namely the outcomes important to patients and family carers and how to improve care at home after hospital discharge. Additional codes were developed during analysis for relevant data that could not be coded according to the pre-determined coding scheme. The codes were then inductively categorized into overarching subthemes and themes.
Regarding the Theory of Change workshops, the researcher conducted directed content analysis in MS Excel 26 and discussed this with the team. The pre-determined coding scheme was based on elements of the Theory of Change checklist, that is, impact, long-term outcomes, preconditions, interventions. 27 In the workshops, participants generated many ideas and then they jointly developed the Theory of Change map until consensus was reached. These points on which consensus was reached were noted and summarized in written form by the researcher (KdN). We deductively coded this data in accordance to the pre-determined coding scheme, followed by the process of inductively categorizing the codes into overarching themes and subthemes. These themes and subthemes were included in the map and this resulted in a first draft Theory of Change map. Subsequently, the map was checked against relevant literature and rationales by the research team and co-designed with professional stakeholders. This resulted in a second draft Theory of Change map and an accompanied standardized description of the intervention using TIDieR checklist. 23
Ethics
Ethics approval for this study was given by the Commission of Medical Ethics of the University Hospital Brussels (B.U.N. 143201732678). Older people and family carers gave written informed consent prior to recording and the professional stakeholders who participated in the Theory of Change workshops gave verbal consent. All obtained data were pseudonymised.
Results
Participants characteristics
We held two group discussions with older people (n = 11, mean age 78.3 years, female n = 8), one with family carers (n = 8, mean age 71.9 years, female n = 5) and individual semi-structured interviews with older people (n = 3, mean age 82.0 years, female n = 1). We conducted four half-day Theory of Change workshops with professional stakeholders (see Table 2, stakeholder characteristics).
Characteristics of stakeholders involved in the workshops.

Theory of change of the intervention
We present the impact and ceiling of accountability, long-term outcomes, preconditions, interventions, rationales and assumptions, as suggested by the checklist for reporting Theory of Change. 27 As limited data are available to determine standards or cut-offs for achieving a precondition, we have not yet developed the indicators. In the next stage, we will test the feasibility of the intervention and will use the data gained from that work to suggest indicators for measuring whether preconditions have been achieved. The Theory of Change map is presented Figure 2.
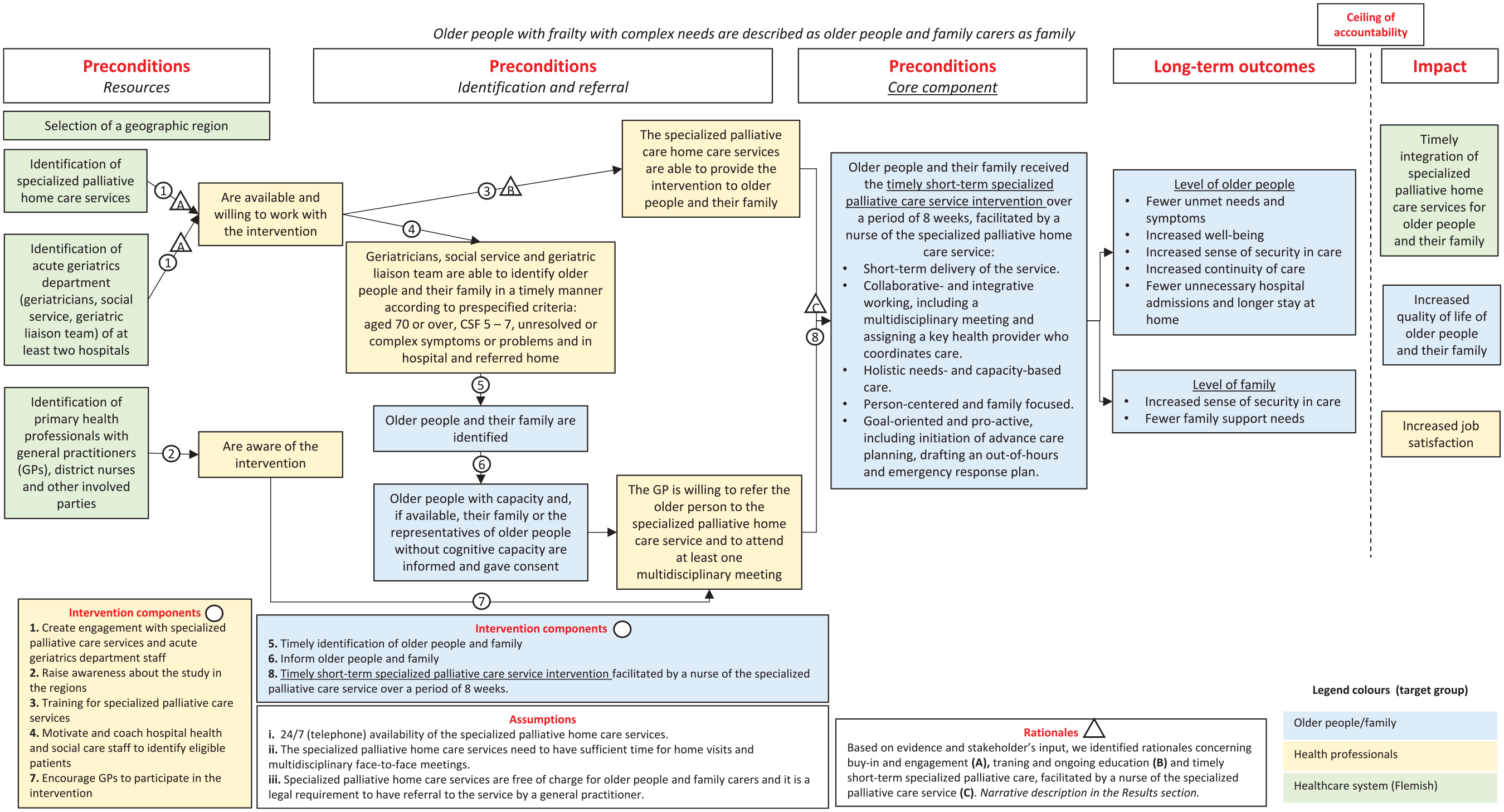
Theory of Change map of the Frailty + intervention: Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care.
Impact and ceiling of accountability
Based on the qualitative research, we identified the real-world impact of the timely short-term specialized palliative care service intervention. This was defined as ‘timely integration of specialized palliative home care services for older people with frailty with complex needs and their family carers’, ‘increased quality of life of older people with frailty with complex needs and their family carers’ and ‘increased job satisfaction among health professionals’. In the Theory of Change map, a line is drawn between the long-term outcomes and the impact, showing that the intervention, although it can contribute, is not directly and solely responsible for achieving the impact.
Long-term outcomes
We identified long-term outcomes of the timely short term specialized palliative care intervention, relating to older people with frailty and their family carer. Based on the qualitative interviews, we identified the outcome ‘increased sense of security in care’, explained as patients having the feeling that they can rely on their care providers. Through the Theory of Change workshops and the systematic review, 20 we identified ‘increased well-being’, ‘fewer unmet needs and symptoms’, ‘increased continuity of care’, ‘fewer unnecessary hospital admissions’ and ‘longer stay at home’ as important patient-related outcomes. The family carer-related long-term outcomes include: ‘increased sense of security in care’, valued as important outcomes in the group discussions by family carers and ‘fewer family carer support needs’, identified through the systematic review 20 and the Theory of Change workshops.
Preconditions
Based on the qualitative research, we identified several preconditions that need to be fulfilled for the long-term outcomes to be achieved. These preconditions are presented in different colours in Figure 2, according to the level to which they are most applicable (i.e. the level of older people, family carers, health professionals or the healthcare system).
At the start of the intervention, the following stakeholders within a geographic region should be identified: specialized palliative home care services, acute geriatrics department (i.e. geriatricians, social service, geriatric liaison team) and primary health professionals including but not limited to general practitioners and district nurses. The specialized palliative home care services and the acute geriatrics staff should be available and willing to work with the intervention, and primary health professionals in the region should be aware of the intervention. To identify and refer older people with frailty and family carers to the specialized palliative home care service, a first precondition which should be fulfilled is: geriatricians, social service and geriatric liaison team are able to identify older people with frailty and their family carers in a timely manner according to prespecified criteria (see Supplemental Table 2 for more details inclusion criteria):
aged 70 years or over,
Clinical Frailty Score 5–7, 28
one or more unresolved or complex symptoms or problems in one of the four palliative care domains, these can include situations such as, but not limited to complex end-of-life issues such as being ‘tired of living’, highly conflicted decision-making, consideration of palliative sedation, requests for assisted dying or euthanasia or other end-of-life decisions; difficulties with advance care planning; patient characteristics or complexity due to cumulation of multiple problems; pre-existing complexity, for example long-standing difficulties with finances/housing or mental health needs; difficult interactions between the patient, family and healthcare professionals (e.g. dissonance or conflicts, older patients who refuse care),9,29 and
are in a hospital and referred to return to their home.
Other preconditions were: older people and their family carers are identified, informed about the intervention and asked for consent (representatives give consent for older people without cognitive capacity to do so); the specialized palliative home care services are able to provide the intervention; and the general practitioner is willing to refer to the service (as this is a legal requirement in Belgium). Patients and family carers should then receive the intervention facilitated by a nurse of the specialized palliative home care service to achieve the long-term outcomes.
Intervention components
Based on stakeholders’ input and the systematic review, 20 the intervention components that are required to achieve each of the preconditions were identified. We distinguished implementation components and a core component with subcomponents. Following TIDieR, Table 3 summarizes for each of the components the materials and procedures; providers; the ‘how’, ‘where’, ‘when’ and ‘how much’ of delivery for each component, whether the component can be tailored, and the planned fidelity (i.e. strategies that will be used to maintain or improve intervention adherence).
Summary description of the Frailty + intervention based on the TIDieR checklist. 23
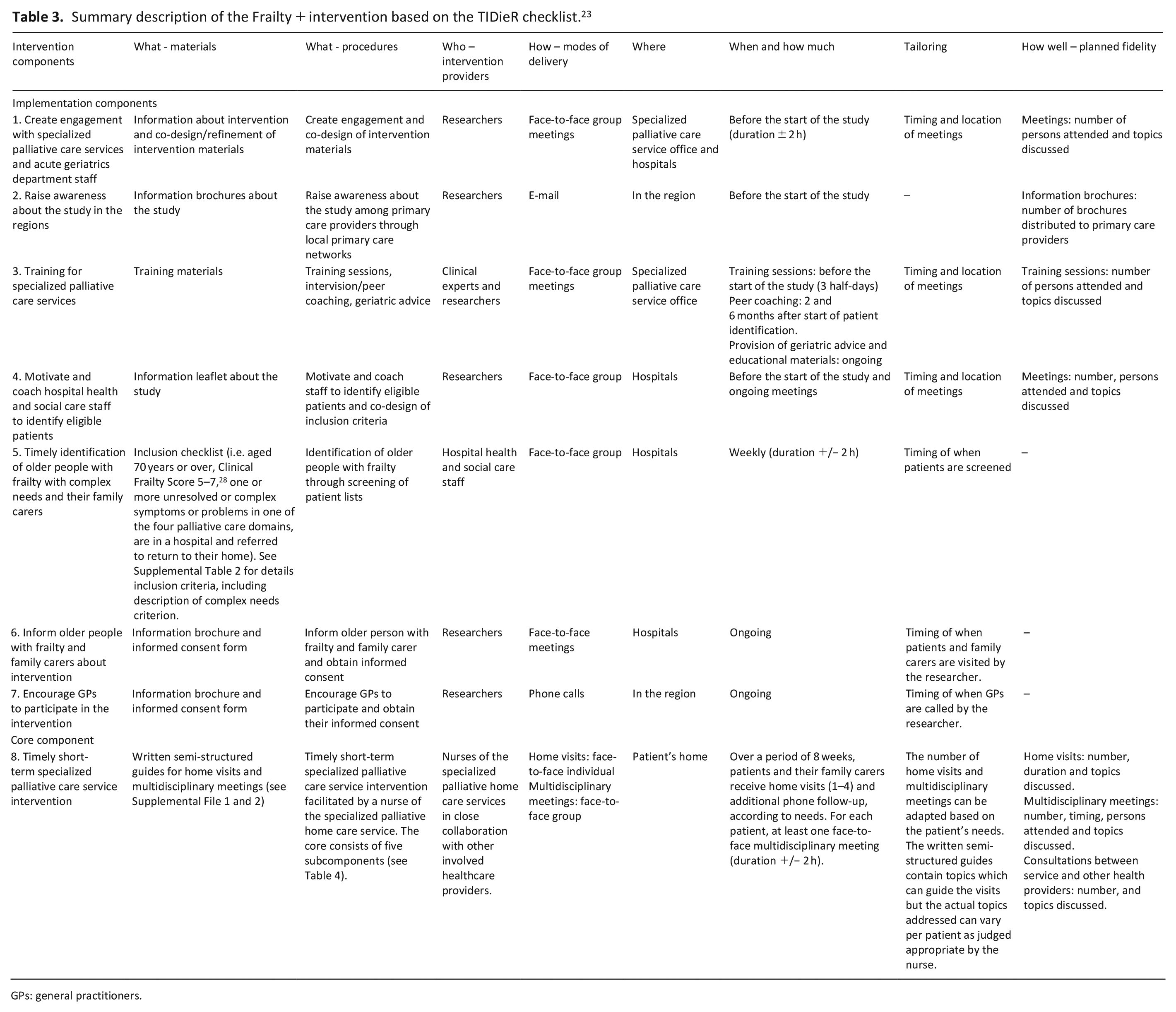
GPs: general practitioners.
Description of the five subcomponents at the core of the timely short-term specialized palliative care service intervention.
Rationales
Based on existing evidence and stakeholder’s input, we have identified several rationales that support the choice of the different intervention components. The rationales are marked in the Theory of Change map (see Figure 2) and elaborated here.
As implementation science studies have shown, buy-in and engagement of stakeholders (A) is needed to effect change and to create an environment conducive to the successful implementation of the intervention.30–32 In addition, training and on-going education of the stakeholders (B) on how to use and integrate the intervention into practice is key for optimal implementation. 33 The intervention materials that were co-designed with the specialized palliative care services (i.e. the written semi-structured guides for home visits and multidisciplinary meetings) and the hospital health and social care staff (i.e. inclusion criteria), were produced with an understanding of the local context and meeting the needs of the stakeholders. 34
Rationales supporting the core component (C) include research indicating that timely initiation and short-term delivery of specialized palliative care services is feasible and beneficial for patients with multiple sclerosis and has been proposed for older people with frailty and multimorbidity.14,34–36 The professional stakeholders stressed the importance of collaborative and integrative working in primary care and particularly the need for organizing multidisciplinary team meetings, to ensure that there is a mutual understanding of patient’s needs, goals and wishes, to allow continuity and coordination of care, identify a key care coordinator, and deliberate an out-of-hours and emergency response plan with the patient and family. This expert advice also corroborates with the multidisciplinary collaborative care model.37–39 Recent work studying different service delivery models for older people highlighted the need for an integrated approach in this population combining palliative care (which mainly focuses on patients’ needs, symptoms and concerns) with rehabilitation/geriatric care (focusing on maintaining and optimizing patient functioning and capacities).40,41
The professional stakeholders indicated that older people with frailty with complex needs often require support from family carers. This is also highlighted as a central part of a palliative care approach. 42 This intervention therefore follows a care approach that includes family carers as both care recipients and care providers. 43 The professional stakeholders mentioned goal-oriented care as well as advance care planning as important features; both part of a pro-active care approach which has been advocated as important in the care approach for older people. 44 Hence, as part of the core component, we included the need to have conversations about people’s life, health, and care goals, including but not limited to medical care or end-of-life care.45,46
Assumptions
Based on the findings of the systematic review 20 and the qualitative research with patients, family carers and professional stakeholders, we identified that the following conditions must be in place to achieve the identified preconditions: (i) 24/7 (telephone) availability of the specialized palliative home care services, (ii) specialized palliative home care services need to have sufficient time for home visits and a multidisciplinary meeting and (iii) specialized palliative home care services are free of charge for patients and family carers.
Discussion
Using a participatory Theory of Change approach, we created a hypothetical causal pathway of a timely short-term specialized palliative care service intervention for older people with frailty with complex needs and their family carers in primary care. This is presented in a Theory of Change map that specifies through which changes and under which circumstances the intervention’s long-term outcomes can be achieved. We identified long-term outcomes of the intervention related to the person with frailty (e.g. fewer unmet needs and symptoms), and the family carer (e.g. increased sense of security in care). We identified preconditions on different levels that need to be fulfilled to achieve the long-term outcomes. We have operationalized and systematically described the intervention components, consisting of a core component and implementation components, according to the TIDieR checklist.
The Theory of Change of the intervention provided detailed and comprehensive understanding and transparency of the presumed hypothetical pathway of the implementation and organization of the intervention. This detailed information is deemed crucial to understand how the intervention might work in clinical practice, and to facilitate replication and comparison with other studies.15,16,23,47 By using this elaborate and participatory approach, we were able to identify all stakeholders that should be involved when aiming to improve care for older people with frailty with complex needs and their family carer in primary care, and determine the multiple intervention components targeting them to achieve the desired change.
We identified several long-term outcomes of the intervention, of which some were expected based on previous research such as fewer unmet needs and symptoms,48,49 but others were less frequently reported in research such as increased sense of security in care. The patients, family carers and professionals all identified this subjective feeling concerning the provided care as a very relevant outcome in this population. One meta-ethnographic study on the effects of home palliative care 50 also highlighted ‘the safety of care at home’ but the concept has not been widely studied so far. Trials evaluating effectiveness of palliative care interventions or current outcome measures for a palliative care population (e.g. iPOS) have not yet focused on this as a possible outcome.
Through the participatory Theory of Change workshops with professional stakeholders, we revealed intervention components that were not made explicit in many other previously developed palliative care interventions including those for older people with frailty in primary care, 20 such as steps to ensure buy-in and engagement with the professionals involved. In addition, we integrated care approaches from different disciplines as the core of the intervention, such as combining palliative care with geriatric and rehabilitative care, and the integration of goal-oriented pro-active care with advance care planning.40,41 There was consensus among stakeholders that the focus of care should move beyond the purely medical domain to include broader health, life and care domains focusing on the things that matters most to the patient and his/her family, and that realistic or attainable goals should be discussed to guide care.45,46
The developed intervention has a short-term nature and outcomes are measured directly after the intervention period, that is, 8 weeks post-baseline. These data will not allow us to determine the sustainability of any positive intervention effects. Earlier studies of short-term palliative care for people with MS 51 and for older people with chronic noncancer conditions 52 both with a service delivery for a period of 12 weeks, showed that the effects appear to wane over time. The developed intervention might have the potential to sustain its effects through its integrative and collaborative care approach, including the organization of multidisciplinary meetings on palliative care with all involved health and social care providers in which ways for future communication and collaboration were established and a key health provider was assigned who coordinates care within the multidisciplinary team. This could enhance coordination and continuity of care after the intervention period and facilitate re-referral of the older person to the specialized palliative service in case of complex care needs. Further research is required to determine whether this can maintain positive intervention effects over time and how exactly.
Although growing attention is paid to involvement of specialized palliative care services based on needs rather than prognosis,41,42 consensus on complex needs-based criteria for referring older people with frailty to these services is lacking. Following stakeholder’s input and the systematic review, 20 we identified criteria for timely identification of older people with frailty to specialized palliative care services in primary care. These criteria were focused on patient characteristics, for example, frailty, and, to an important part, on complex needs. We identified that the necessity of involvement of specialized palliative care services can be based on complex needs in one of the four palliative care domains.
A Theory of Change map developed in one country is likely to be at least partly context-specific. All complex interventions, such as this one, are context-specific. The strength of Theory of Change is to specify the preconditions leading to outcomes so interventions can be more readily adapted. Making all steps in the pathway to change visible, will enable a scientific readership in other countries to evaluate the extent to which the identified preconditions, assumptions or rationales are applicable in their own health care system, and to consider which elements are transferable and which need further adaptation. Nevertheless, we argue that several parts of the developed map are transferable to other countries, particular to high-income countries, where primary care is the main place of care for older people with frailty, and palliative care services are available in primary care but often accessed late. For example the core intervention component, which includes integrated working, holistic, person-centred and goal-oriented care, which are identified as important palliative care approaches in primary care in many countries. 53 Elements that might not be generalizable are those that are most specific to a health care system such as fully reimbursed 24/7 access to specialist palliative home care.
It is notable that the components included in this intervention might not be unique to meet the specific needs of older people with frailty in the community. The model might therefore also be a model of care that is transferable to people with other serious illnesses, although this requires further research. Nevertheless, some parts of the intervention components highlighted by the stakeholders do seem to be more related to a geriatric care approach than to a palliative care approach (e.g. focus on capacity-based care). 41
This study has some limitations. Although the findings of the interviews and group discussions with patients and family carers were discussed in the Theory of Change workshops, patients and family carers were not involved in constructing the Theory of Change map. In addition, although this approach helps to elucidate the components of a complex intervention, the resulting model remains a rather linear causal model and thus might be a simplification of a complex reality. While the Theory of Change approach (and other theoretical approaches to intervention development) receive increasing scientific attention, 27 it has until now not been proven that interventions that were guided by this approach lead to more effective interventions. It therefore remains to be studied in subsequent research whether this comprehensive development approach can increase intervention effectiveness and guide outcome and process evaluation. In this project, we will first assess the feasibility, acceptability and preliminary effectiveness of the intervention in a pilot randomized controlled trial and conduct an in-depth mixed-methods process evaluation (Trial registration number: ISRCTN39282347). 54 The Theory of Change map will be adapted according to these findings. If the intervention is determined feasible and acceptable, our research might be followed by a full-scale RCT.
Conclusion
We developed and modelled a timely short-term specialized palliative care service intervention for older people with frailty with complex needs and their family carer, using a Theory of Change approach outlining how and in what circumstances it will lead to specific outcomes. The comprehensive and systematic description of the intervention components, outcomes and preconditions aims to increase replicability and comparability with other interventions.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211040187 – Supplemental material for Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care: Development and modelling of the frailty+ intervention using theory of change
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211040187 for Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care: Development and modelling of the frailty+ intervention using theory of change by Kim de Nooijer, Lara Pivodic, Nele Van Den Noortgate, Peter Pype, Catherine Evans and Lieve Van den Block in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163211040187 – Supplemental material for Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care: Development and modelling of the frailty+ intervention using theory of change
Supplemental material, sj-pdf-2-pmj-10.1177_02692163211040187 for Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care: Development and modelling of the frailty+ intervention using theory of change by Kim de Nooijer, Lara Pivodic, Nele Van Den Noortgate, Peter Pype, Catherine Evans and Lieve Van den Block in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163211040187 – Supplemental material for Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care: Development and modelling of the frailty+ intervention using theory of change
Supplemental material, sj-pdf-3-pmj-10.1177_02692163211040187 for Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care: Development and modelling of the frailty+ intervention using theory of change by Kim de Nooijer, Lara Pivodic, Nele Van Den Noortgate, Peter Pype, Catherine Evans and Lieve Van den Block in Palliative Medicine
Supplemental Material
sj-pdf-4-pmj-10.1177_02692163211040187 – Supplemental material for Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care: Development and modelling of the frailty+ intervention using theory of change
Supplemental material, sj-pdf-4-pmj-10.1177_02692163211040187 for Timely short-term specialized palliative care service intervention for older people with frailty and their family carers in primary care: Development and modelling of the frailty+ intervention using theory of change by Kim de Nooijer, Lara Pivodic, Nele Van Den Noortgate, Peter Pype, Catherine Evans and Lieve Van den Block in Palliative Medicine
Footnotes
Acknowledgements
We would like to thank all stakeholders who participated in the qualitative interviews, group discussions and the Theory of Change workshops. The authors would like to thank Jane Ruthven for linguistic help.
Author contributions
All authors have contributed to the following categories for authorship. Study conception and design: de Nooijer, Pivodic, Van Den Noortgate, Pype, Evans, Van den Block. Acquisition of data: de Nooijer, Pivodic, Van den Block. Analysis and interpretation of data: de Nooijer, Pivodic, Van Den Noortgate, Pype, Evans, Van den Block. Drafting the manuscript: de Nooijer. Critical revision: de Nooijer, Pivodic, Van Den Noortgate, Pype, Evans, Van den Block. All authors have approved the final manuscript and agree to be accountable for all aspects of the work. Questions related to the accuracy or integrity of any part of the work will be appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Foundation-Flanders [G.0303.16N]. LP was a Postdoctoral Fellow of the Research Foundation-Flanders (2017-2020). CE is funded by a Health Education England/National Institute of Health Research Senior Clinical Lectureship (ICA-SCL-2015-01-001).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.