
Abstract
Background:
Current evidence suggests that COVID-19 is having a negative impact on the delivery of end of life care in care homes around the world. There is a need to collate current evidence to provide a comprehensive overview to assess extent of the problem.
Aim:
To describe and evaluate the impact of the COVID-19 pandemic on end of life care delivery in care homes.
Design:
Systematic review and narrative synthesis of studies reporting qualitative and quantitative data.
Data sources:
The databases MEDLINE, psycINFO, SCOPUS and CINAHL were searched between December 2019 and March 2021.
Results:
Nine studies were included. For care home staff, challenges included significant increases in responsibility and exposure to death, both of which have taken an emotional toll. Results indicate that staff tended not to be offered adequate emotional support or afforded the time to grieve. For those receiving end of life care, results indicate that the end of life care that they tended to receive, especially in the form of advance planning, was disrupted by the pandemic.
Conclusion:
The effect of the pandemic has been to exacerbate existing problems in the provision of end of life care in care homes for both service providers and users, making that which was previously opaque starkly visible. Future research is needed to explore the effects of the pandemic and its management on those receiving end of life care in care homes and their significant others.
Keywords
Current evidence suggests that the COVID-19 pandemic is having a negative impact on the delivery of end of life care in care homes around the word. Thus, there is a need to collate current evidence to provide a comprehensive overview to assess extent of the problem.
The end of life care that residents and their significant others tended to receive, especially in the form of advance planning, was disrupted by the pandemic.
For members of care home staff, challenges included significant increases in responsibility and exposure to death, both of which have taken an emotional toll.
The literature also indicates that staff tended not to be offered adequate emotional support or afforded the time to grieve.
There is a need to formally recognise the dedication of the care home workforce, particularly in the form of providing adequate emotional and mental health support for those exposed to increased rates of death and dying during pandemic conditions.
Care home staff require sustained education and support to engage in advance care planning with residents.
There is a need for future research to elicit directly from people who live in care homes the effects of the pandemic and its management has had on them.
Introduction
The World Health Organisation (WHO) have reported that up to 50% of COVID-19 deaths across Europe have been in care homes. 1 Although other settings such as hospitals, hospices and the community have been impacted by increased numbers of deaths, care homes have seen the greatest increase in death rates internationally. 2 The generic term ‘care home’ will be used in this study to describe both residential and nursing homes, which both provide food and board, 24-h care cover and assistances where required with activities of daily living. Nursing homes additionally provide care by registered nurses. Both residential and nursing homes deliver end of life care. 3
An international report on the numbers of excess deaths in care homes linked to COVID-19 was published in February 2021. 2 The report shows that mortality figures in care homes linked to COVID-19 are still not available in many counties, however some countries have started to publish figures. 2 In the United States of America (USA), 139,699 excess deaths have been reported in care homes as a result of COVID-19. 2 In England, it has been highlighted that deaths in care homes have increased by 220% during the first 10 weeks of the pandemic, 4 and the latest data report 29,542 excess deaths in care homes. 5 Despite these figures only being estimations (each country measures excess death in care homes differently), 2 they still highlight the significantly increased morality rates in care homes.
One of the reasons care homes have been impacted so significantly by the pandemic is that their residents are often aged over 65 years with multiple co-morbidities. 6 For example, in the UK, care homes provide care for approximately 418,000 people which represents 4% of the population aged over 65 and 15% aged over 85. 3 Moreover, residents living in care homes tend to live in close proximity and require close contact care from nursing and care staff, 7 as well as contact from outside agencies such as general practitioners, and specialist palliative care teams. 8
Given the vulnerability of residents to COVID-19 infections, 9 a number of changes to end of life care delivery in care homes have been implemented. 10 Despite variations between counties, the most common changes to end of life care include visiting restrictions which limit who can be present at the time of a resident’s death and care home staff’s use of personal protective equipment (wearing masks, gowns and gloves).10,11
Emerging evidence suggests that these changes and challenges posed by COVID-19 have had a negative impact on the delivery of end of life care in care homes. Although the definition of end of life care can vary, generally it refers to the care given in the last 12 months of life which comforts and supports people who are dying from a progressive life-limiting condition. 12 It has been reported that the core principles that make up good quality end of life care such as care planning, maintenance of a sense of control, the opportunity to be with friends and family and having symptoms managed have all been jeopardised by the pandemic in multiple countries across the world.13,14 Recent evidence has shown that during the pandemic some residents have died alone without family and have not been given the opportunity to control their own care. 14 Problems in relation to pain management and administering palliative care drugs have also been reported. 15 Although insight into these challenges has been reported in individual studies there is a need for a comprehensive overview to assess extent of the problem. The aim of this paper is therefore to describe and evaluate the impact of the COVID-19 pandemic on end of life care delivery in care homes.
Methods
Aims
To describe and evaluate the impact of the COVID-19 pandemic on end of life care delivery in care homes.
Design
A mixed-method design, integrating qualitative, quantitative and mixed method evidence to address the review aim, was chosen.16,17 Such an approach was deemed most appropriate because emergent reactions to change can often only be understood through the synthesis of qualitative and quantitative evidence. 16
Although a number of synthesis methods can be used to integrate the different types of evidence, this review used narrative synthesis 18 as the included studies produced findings that could be readily synthesised into one another to address the review aim. 17 The review was reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA). 19
Search strategy
Preliminary searches were conducted which provided insight into the different terminology used within articles in the field. Additionally, the authors previous experiences of conducting systematic reviews in the field8,20 was used to construct the search terms.
Four electronic databases were searched: MEDLINE; psycINFO, SCOPUS and CINAHL. The search was limited to English language papers published between December 2019 and 15th March 2021. The search strategy, and Boolean terms used are included in Table 1. The search strategy also included forward and backward citation searching of relevant papers, and policy guidelines as well as searching grey literature. Relevant papers known to the authors were also included.
Search strategy.
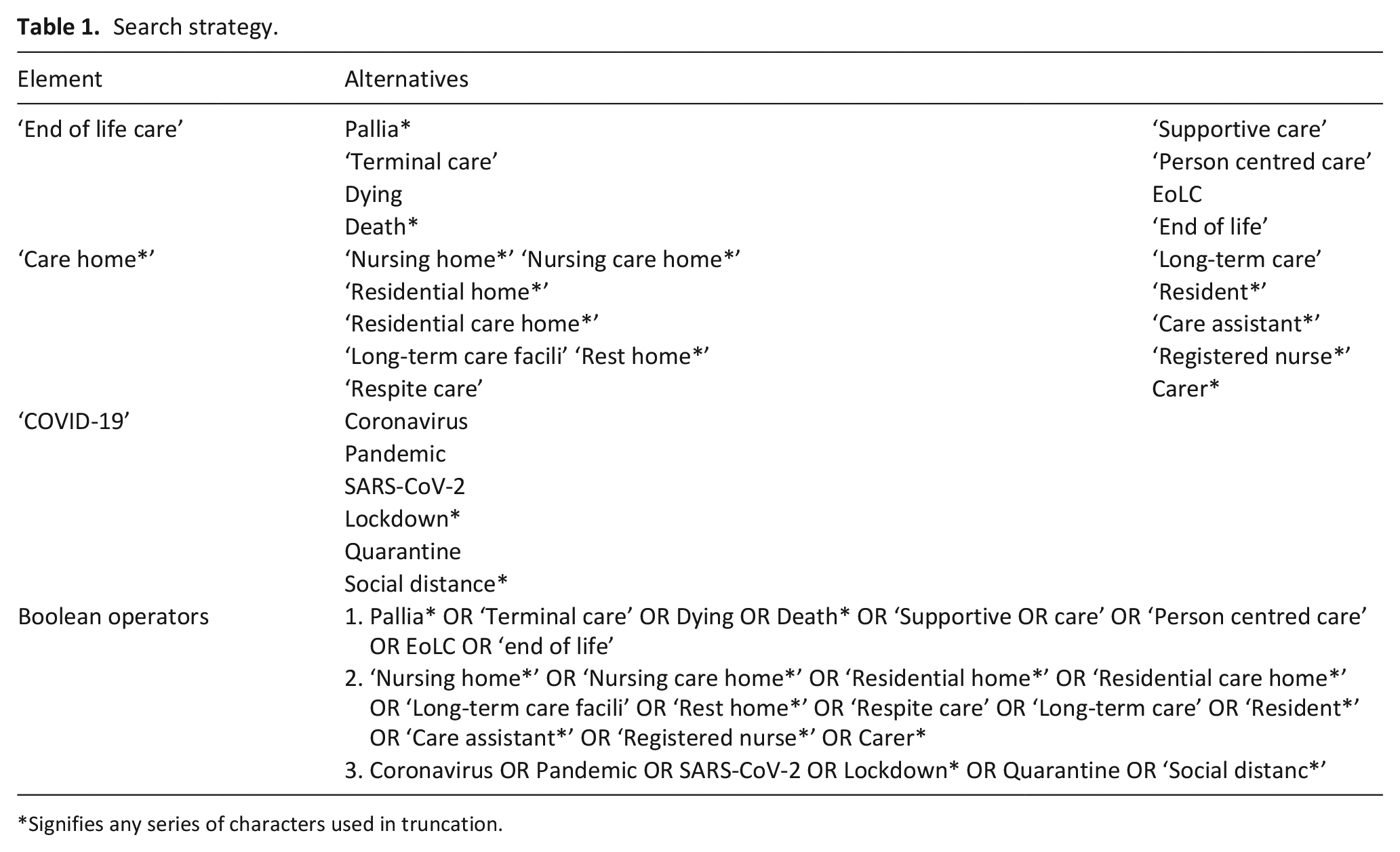
Signifies any series of characters used in truncation.
The date restriction (December 2019–March 2021) was placed on the search as the COVID-19 outbreak started in China in December 2019. 21 In order to capture all relevant international literature, no location restrictions were placed on the search.
Inclusion and exclusion criteria
Initial screening of titles and abstracts was carried out by A.S., M.B. and S.P. Articles relevant for inclusion were then subject to a full text screening by A.S., S.P. and M.B., who assessed them against the inclusion criteria detailed below.
Data extraction
Data was extracted by A.S. into Microsoft Excel which included the main features of each article including title, author(s), date, country, study methodology, main findings/results. The data extraction process was cross-checked by S.P., M.B. and J.S.
Quality assessment
Quality assessment was independently carried out by two authors A.S. and J.S., using an appraisal tool designed to assess qualitative, mixed methods and quantitative studies. 22 Following the screening questions, the quality of the studies is assessed against set criteria for each section. Any disagreements were discussed. If no agreement could be reached it would have been settled by S.P. and M.B. The quality of the studies was graded from 0% to 100% with 0%–20% being (very low), 20%–50% (low), 50%–70% (moderate) and 70%–100% (high). No studies were excluded based on quality, and all the included studies were graded moderate to high quality.
Data synthesis
We conducted a narrative synthesis of the included studies. 18 Narrative synthesis involves the juxtaposition of findings from multiple studies, as well as identifying common themes or areas across the studies. 18 It is commonly used to synthesise evidence from studies which are heterogeneous, thus, narrative synthesis does not necessarily aim to transform data beyond the findings of the studies.18,23 This is important given the heterogeneity of the study designs, methods and samples of the included studies which meant that a separate meta-analysis of outcomes was not possible. Consequently, a single narrative synthesis of both qualitative and quantitative evidence was conducted.
The synthesis was initially carried out by A.S., who first examined the extracted evidence from each study. This evidence was then collated, and relationships/common themes were explored both between and within the extracted evidence from the studies. This synthesis process was triangulated by all authors. The findings were then grouped into themes which were decided upon by mutual agreement between authors.
Results
Database searching yielded 716 unique records, 677 articles were excluded based on title and abstract screening. Full-text versions of the remaining 39 studies were screened for eligibility. Seven articles were left which met the inclusion criteria. Citation searching, and relevant papers already known to the authors identified an additional two articles. Nine articles were included in total. See Figure 1 for a flow diagram of the study selection process.
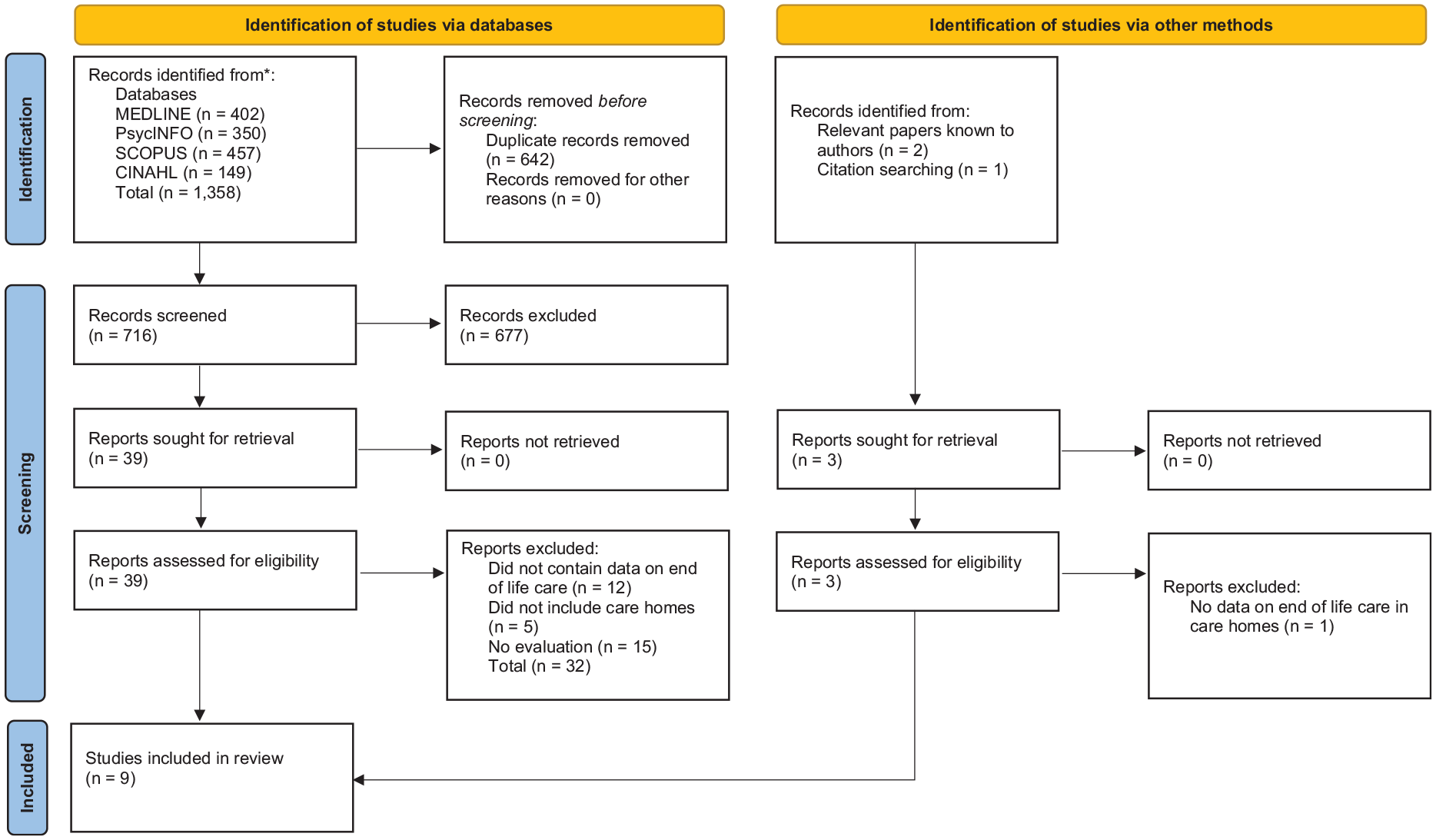
PRISMA flow diagram of the study selection process.
Overview of included studies
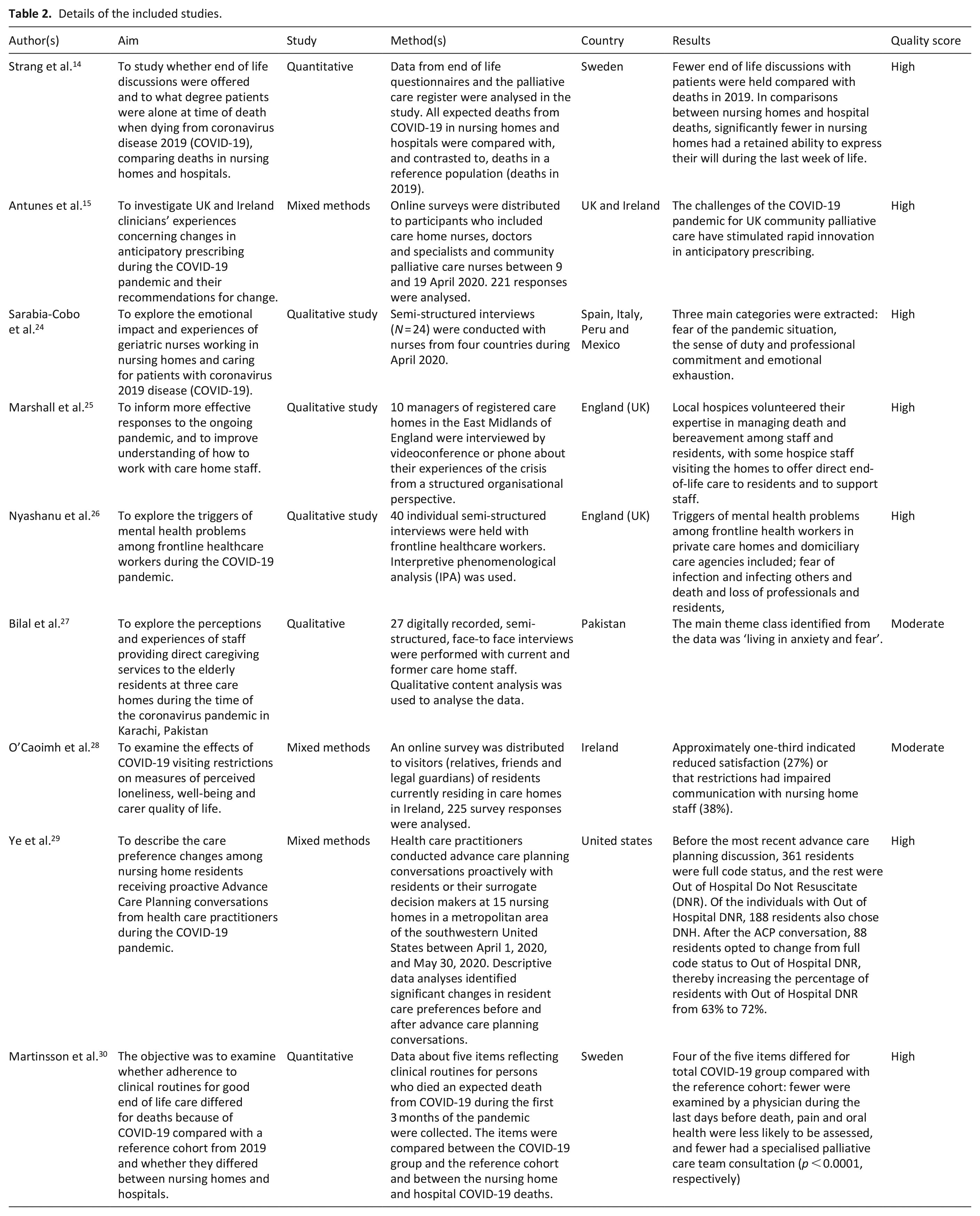
Of the included studies, four were qualitative,24–27 three used a mixed method design15,28,29 and two were quantitative.14,30 The studies included populations from nine countries, including the UK (N = 3),15,25,26 Sweden (N = 2),14,30 Ireland (N = 2),15,28 Spain (N = 1), 24 Italy (N = 1), 24 Mexico (N = 1), 24 Peru (N = 1), 24 Pakistan (N = 1) 27 and the USA (N = 1) 29 (Table 2). Participants in five studies consisted of care home staff, which included registered nurses, home managers and non-registered staff such as care assistants and domiciliary staff. Participants in one study were relatives of residents. Residents or their surrogate decision makers only participated in one study. Qualitative methods included semi-structured qualitative interviews, focus groups (via video conferencing) and online surveys. Quantitative methods included analysis of mortality statistics, palliative care registers and residents’ chart analysis. See Table 2 for a breakdown of each included study.
Details of the included studies.
Four main themes were derived: The importance of advance care planning; Increased responsibilities and expectations; Emotional trauma and fear; Professional pride and resilience. Each theme is detailed below.
The importance of advance care planning
The increased importance of care planning discussions in advance of end of life care during the COVID-19 pandemic in care homes was noted by several studies.14,28,29 Ye et al., 29 conducted a retrospective chart analysis of n = 963 residents and their surrogate decision makers from 15 nursing homes in Texas, USA between April 1, 2020 and May 30, 2020. The study found that advance care planning discussions during the COVID-19 pandemic led to increased numbers of residents changing their wishes. For example, residents choosing the ‘do not hospitalise’ option increased from less than a quarter to almost half of nursing home residents. Moreover, Ye et al. report that out-of-hospital ‘do not resuscitate’ orders increased by 9%. These findings highlight the importance of proactively engaging in advance care planning during the COVID-19 pandemic to ensure care is consistent with the wishes of residents.
Despite the increased importance of advance care planning, data analysis in this review suggests that advance care planning was significantly hindered by the COVID-19 pandemic in care homes. Specifically, several studies suggest decreased advance care planning and end of life discussions with residents and relatives.14,28,29 Strang et al. 14 analysed the national Swedish Register of Palliative Care to compare deaths in care homes during COVID-19 to pre-pandemic deaths, n = 908 expected COVID-19 deaths in care homes were analysed. Although results do not suggest changes in advance care planning discussions occurred for all residents during the pandemic, the study did find that fewer care planning discussions were taking place compared to pre-pandemic data, with 35% fewer residents being able to retain the ability to express their wishes during the last weeks of life. Furthermore, analysis identified that the unpredictable and unplanned decline of residents with COVID-19 coupled with fewer care planning conversations led to more unnecessary admissions to hospital at the end of life.14,29 This situation may have contributed to the increase in residents dying without their relatives and friends around them.14,28
The reasons behind the decreased occurrence of advance are planning and end of life discussions varied between studies. One study suggested that less care planning discussions occurred with relatives because of the social distancing measures preventing them from physically visiting care homes. 14 Other studies suggest that it may be because of decreased clinical routines and visits from external service staff such as General Practitioners and specialist palliative care teams.25,30 Lastly, particularly towards the beginning of the pandemic, care home staff’s fear of being infected or infecting residents with COVID-19 may have prevented regular care planning discussions.26,27
Reductions in advance care planning discussions seem to have most significantly impacted residents living with dementia, who are often reliant on relatives and surrogate decision makers.5,14 Strang et al. 14 found that because of social distancing measures in place, care planning with relatives and surrogate decision makers significantly reduced, meaning residents living with dementia were left without an appropriate care plan in place before their death. Furthermore, Ye et al. 29 found it was older resident groups often with cognitive impairment who were most likely to choose not be resuscitated or hospitalised in their care plan.
Increased responsibilities and expectations
A common theme running through the studies regardless of country was the increased responsibilities and expectations of care home staff delivering end of life care during the pandemic.15,24–26,30 Care home staff were found to be taking on care responsibilities usually delivered by trained clinicians within primary care, 25 and specialist palliative care teams. 30 For example, it was found some managers in the UK were asked to verify residents’ deaths without appropriate training or support. Furthermore, in the UK during the first lockdown some managers were making decisions as to whether to admit residents with COVID-19 to the care home. 25 Moreover, more untrained care home staff were relied on to administer drugs during residents end of life care. 15
It was evident that many of these increased responsibilities and expectations were due to poor communication, demand and access restrictions impacting on external services usually involved in supporting residents’ end of life care in care homes.24,25,30 For example, Martinsson et al. 30 found that as a result of the restrictions in Sweden, fewer residents were examined by a physician during the last days of their life, and pain management as well as oral health were assessed less frequently, and consultations with specialist palliative care teams reduced. Similarly, a study which collected data from four countries in Europe and Latin America also highlighted instances where care home staff expressed feelings of abandonment by external services and government organisations. 24 In the UK, a lack of prioritisation of care home services by the government was noted which led to changing rules and regulations not being effectively communicated to care home staff. 25 Similar findings emerged from a study in Pakistan where changes to end of life practice, such as amendments to social distancing were not effectively communicated to care home staff. 27
One study indicated that these increased responsibilities and expectations led to some staff becoming more tenacious and creative in their roles, especially to facilitate ‘good’ deaths. 25 For example, some care home staff were able to build and develop stronger links with their local community services and hospices. Local hospice staff would visit the homes to offer increased end of life care support to not only residents but staff as well. 25 Despite this, several studies indicate that the extra responsibilities placed on care home staff were not sustainable as they put extra pressure on staff during an already demanding time, particularly home managers.15,25,27 Specifically, some care home staff even blamed themselves for allowing patients to be admitted to the care home from hospital with COVID-19, others felt guilty if residents died soon after pain medication was administered.15,25,26
Emotional trauma and fear
All the studies included in this review made at least some reference to the increased mortality rates in care homes, and in particular the emotional impact it was having on residents, relatives and care home staff.
Although only one study included visitors (relatives and friends of residents who were receiving end of life care during the pandemic), it evidenced some of the negative consequences of increased mortality in care homes. 28 O’Caoimh et al. 28 distributed an online survey to visitors (relatives, friends and legal guardians) of residents currently residing in care homes in Ireland; 225 survey responses were analysed. Results highlighted the emotional burden experienced by some visitors and residents as a result of the pandemic. It was reported that attempts to shield residents and relatives from excess mortality through social distancing restrictions led to increases in loneliness and isolation, and relatives felt that this negatively impacted on end of life care.
The emotional impact on care home staff received more attention in the studies.24–27
The increased exposure to death and dying was found to have a significant impact on care home staff’s mental wellbeing. The most prevalent emotions care home staff expressed within these studies included; fear, depression, stress, anxiety, hopelessness and grief.24,26,27 Bial et al. 27 conducted 27 digitally recorded, semi-structured, face-to face interviews with current and former care home staff in Pakistan. The study found that when residents become sick and died from COVID-19, staff become worried themselves that they would also catch it, and potentially infect residents or even become seriously ill or die themselves. Similarly, Sarabia-cobo et al. 24 highlighted the stress and fear of potentially infecting vulnerable residents further heightened stress and anxiety within the workforce.
As well as infecting residents in the care home, staff feared bringing the COVID-19 home to their own families.24,26,27 Nyashanu et al. 26 conducted 40 semi-structured interviews with frontline care home staff. The study found that care home staff who had lost someone close or a colleague to COVID-19 were even more fearful of not only being infected themselves but passing that infection on to other colleagues and residents. This fear was particularly evident amongst care home staff who lived with vulnerable family members. Additionally, Sarabia-Cobo et al. 24 and Bilal et al. 27 both found that nurses and frontline care staff in care homes feared getting infected and were being worried for their own life, as well as being worried about their families and did not want to bring the virus home with them. Analysis suggests that this fear inhibited their ability to provide effective end of life care and may have played a part in the reductions of advance care plans discussed in theme one.
Moreover, care home staff’s perception that they were not able to provide the same level and quality of end of life care they otherwise would have seemed to add to these negative emotions.14,24,26 Feelings of hopelessness and being overwhelmed were expressed by care home staff who due to social distancing and infection control, could do less to comfort and support residents receiving end of life care. 24
The pandemic starkly demonstrated the degree to which the close involvement of relatives is key to effective care. The deleterious consequences of their absence as a result of infection control restrictions was illustrated by a Swedish study which found that only 13% of nursing home residents dying from COVID-19 had a relative present at the time of death. This put further responsibility on staff members to be there at the end of life, however while staff members were present at the time of death in 52% of cases, 39% of residents dying from COVID-19 died alone. The authors noted the negative social and existential consequences for patients and their families that can result from a solitary death. 14 Similar, findings were also evident within UK care homes to the extent where home mangers reported closer relationships with residents because of this approach to end of life care. 25 Nonetheless, this situation was found to be deeply upsetting for residents and relatives. In Ireland, O’Caoimh et al. 28 reported that 38% of relatives indicated that visiting restrictions had a significant negative affect on relationships with care home staff, and 27% reported decreased stratification with the care. Almost half (49%) reported that their resident was not coping well displayed a negative change in mood during the pandemic.
We found no studies that sought to ask care home residents directly about the emotional impact that being in a care home during a deadly pandemic had upon them.
Professional pride and resilience
Despite the significant emotional challenges for care home staff, a consistent theme of resilience and a sense of duty in the face of the pandemic must be acknowledged. Regardless of country, care home staff’s sense of duty and collective peer support was evident.24–27 It was apparent that this resilience and collective support was essential in helping care home staff deal with their increased exposure to death and dying, working in the home was compared to a ‘warzone’, 27 with staff needing to quickly adapt and cope with the situation for the sake of the residents. 25
Sarabia-Cobo et al. 24 and Marshall et al. 25 found that all care home staff expressed pride for being part of the caring profession during such a difficult and demanding time. Furthermore, Bilal et al. 27 describes how a spiritual sense of duty and love for the job kept some care home staff motivated and sustained. A similar sense of duty within the care home workforce was also noted by Nyashanu et al. 26 who acknowledge the internal difficulty that some care home staff had between their duty of care and their own safety/wellbeing.
In addition, there was evidence of care home staff supporting each other, for example, crying together.24,27 Again, it was evident that this form of peer support was essential to supporting fellow colleagues through the pandemic, especially in a context where resources are low, and restrictions are high.24,25 However, despite evidence of short-term resilience, analysis identified some potentially longer-term problems which may result.24–27 Specifically, some staff expressed they do not know how they will cope with the processing of the memories long-term.24,26
A commonly expressed narrative within the studies was that despite experiencing death and dying on a daily basis, care home staff did not have the time to process, grieve or mourn. 26 Home managers spoke about how some relatives could not attend residents’ funerals, but also implied care home staff were also not able to attend, which was not conducive to their grieving process. 25 Thus, these studies indicate that care home staff were not effectively able to share and deal with their emotions, and instead bottled them up as a coping strategy.24,26,27 As a consequence, these findings suggest there may be significant mental health crisis in care home workforce following the COVID-19 pandemic.
Discussion
This review has provided the first comprehensive overview of the impact of the COVID-19 pandemic on end of life care delivery in care homes. From analysis of the literature, four themes were identified: the importance of advance care planning; increased responsibilities and expectations; emotional trauma and fear; and professional pride and resilience. The results presented in this review highlight the significant challenges as well as the opportunities which have emerged during the pandemic. Thus, the review provides a valuable collation of current evidence to inform immediate and future policy, practice and research.
Results presented in this review suggest that advance care planning with residents and relatives reduced during the COVID-19 pandemic.14,28,29 However, challenges with advance care planning are not new. Research has long highlighted that engagement in advance care planning has not been consistent across the care home sector.8,32 Nor is the problem confined to care homes, having also been identified in the acute care sector. 33 The effect of the pandemic has been to exacerbate an already existing problem in the end of life care of people who reside in care homes.
The problem is significant because it has been established that advance care planning can improve care quality, reduce unnecessary admissions to hospital at the end of life, and lower stress and anxiety for all involved. 31 It is known that sustained education and emotional support are important facilitators of effective care planning discussions between care home staff, residents and relatives, and that these are not always effectively implemented in the care home sector. All too frequently, the lack of sustained education of staff is the result of lack of financial resource.20,32
It is difficult to judge the extent to which more robust education and support would have improved the volume and quality of advance care conversations in isolating pandemic conditions. However, it is reasonable to assume that a more knowledgeable and emotionally confident workforce would have been in a better position to develop novel approaches that mitigated the effects of physical isolation upon the ability to have meaningful conversations. But it is not just the gaps in support that have been exposed by the pandemic. Ye et al.’s 29 demonstration of the dynamic responsiveness of residents and their surrogates to the changing circumstances generated by the pandemic is powerful evidence in support of seeing advance care conversations as part of a continuous process rather than as one-off events. 34
Results presented in this review suggest that care home staff’s increased exposure to death and dying as a result of the COVID-19 pandemic has heightened many of the existing emotional challenges associated with delivering end of life care. Knowledge of previous epidemics has evidenced that they can cause significant psychological damage to people, with symptoms often manifesting as feelings of helplessness, anxiety and depression. 35 These symptoms are similar to the ones reported by care home staff in this review. However, our results indicate that because of the COVID-19 restrictions, care home staff were not able to share and deal with these emotions, and instead bottled them up as a coping strategy. This suggests there may be significant mental health crisis in care home workforce in the coming years. Although more emotional support for care home staff delivering end of life care has been called for in previous research, 32 analysis within this review suggests an urgent need for mechanisms to be put in place to support care home staff’s long-term mental health and wellbeing.
Additionally, this review found that many of the negative emotions experienced by care home staff were heightened by the increased responsibilities and expectations placed on then during the pandemic. For example, some care home staff were verifying residents’ deaths, admitting residents infected with COVID-19 to care homes, and administering palliative care drugs.15,25 However, increasing workloads and responsibilities within the care home workforce have long been a feature of a resource constrained sector to manage chronic workforce shortages. 7 Literature has highlighted that the increasing expectations placed on care home staff are unsustainable and unreasonable given the lack of funding, training and low pay typically seen within the sector.7,36 However, perhaps one of the most significant findings within this review is that despite all the challenges faced, care home staff showed consistent pride and duty of care, often putting the care of their residents before their own needs, as well as the needs of their own families. It might be hoped that evidence concerning increased burden and emotional stress on staff, along with their altruistic responses to the huge demands put upon them, would provide the catalyst for a revaluation of the contribution that this workforce makes to health and wellbeing, and of the support that it needs to best make that contribution. However, there are indications that this evidence is competing with a contrasting, negative narrative that seeks to lay the blame on the staff of care homes for the tragedies that COVID-19 wreaked upon so many residents.37,38
While the perspectives of residents were measured indirectly through their responses to advance planning conversations, 23 the fact that we found no studies specifically designed to elicit directly from people who live in care homes what the effects of the pandemic and its management had on them is a startling finding. Moreover, only one study included the views of relatives. 28 Once again, one of the consequences of COVID-19 has been to bring into focus an issue that has been concerning the research community for the last decade, namely the dearth of studies exploring the voices of those for whose benefit research into end of life care in care homes is carried out, namely people who face the prospect of dying or seeing their loved one die in those loci.39,40
Limitations
It is recognised that this review included studies which included data from a range of different care home types, including nursing homes and residential homes of different sizes and from different countries which may reduce the generalisability of the review. It is also recognised that the governmental and sectoral responses to the COVID-19 pandemic differ between the countries included in this review. Restricting the search to English language may have led some potentially relevant articles have been excluded.
Conclusion
This review of current evidence about the impact of the COVID-19 pandemic on end of life care delivery in care homes reflects the huge challenges that the people living and working in those institutions have faced. For members of staff, these challenges included significant increases in responsibility and exposure to death, both of which have taken an emotional toll. Unfortunately, the literature also indicates that staff tended not to be offered adequate emotional support or afforded the time to grieve. An important deficit is the lack of research data on the effect of the pandemic has had on care home residents. What the literature does tell us is that the end of life care that they tended to receive, especially in the form of advance planning, was disrupted by the pandemic.
The lessons that can be learned from these findings do not solely relate to pandemic conditions. Almost all the findings reviewed in this study could also be applied to end of life care in care homes during ‘normal’ times. The need to make advance care planning more consistent; the need to engage in sustained education and training of staff; the need to ensure that staff are properly prepared to take on the responsibilities that are expected of them; the need to provide them with support to deal with death and dying; the need to formally recognise the dedication of this workforce; and to need to take more seriously the feelings and perspectives of those receiving end of life care and their close others, are all going to remain after the threat of COVID-19 has receded. The extreme challenges generated by the pandemic have exposed these issues, making that which was previously opaque, starkly visible. We wish to contend that if this scrap of silver lining from the dark cloud of the pandemic is not acknowledged and acted upon, then the tragedy of COVID-19’s devastation of care homes will be compounded.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211029806 – Supplemental material for Impact of the COVID-19 pandemic on end of life care delivery in care homes: A mixed method systematic review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211029806 for Impact of the COVID-19 pandemic on end of life care delivery in care homes: A mixed method systematic review by Adam Spacey, Sam Porter, Michele Board and Janet Scammell in Palliative Medicine
Footnotes
Author contributions
A.S. was responsible for the planning, design, conduct and reporting of the work. A.S., S.P. and M.B. performed the study selection and data extraction. A.S., S.P., M.B. and J.S. were involved in the study appraisal process. All authors were involved in the data analysis and synthesis process. All authors contributed and agreed to the final manuscript.
Data management and sharing
All relevant data are within the manuscript. Any other data are available upon request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.