
Abstract
Background:
Specialised palliative home-care supports patients with life-limiting diseases in their familiar surroundings. The number of palliative care teams and patients being cared for is increasing worldwide. To assess and improve quality, it is needed to understand, how specialised palliative home-care can be provided successfully. For this purpose we examined the views of all involved stakeholders.
Aim:
To identify the issues that patients, their relatives and involved health professionals view as important in ensuring the success of specialised palliative home-care.
Design:
We used a qualitative design based on participant observations, interviews and focus groups following the principles of a Grounded Theory approach.
Setting/participants:
All specialised palliative home-care teams (n = 22) caring for adults in Hesse, Germany, participated. We conducted participant observations (n = 5), and interviewed patients (n = 14), relatives (n = 14) and health professionals working in or collaborating with specialised palliative home-care (n = 30). We also conducted focus groups (n = 4) with health professionals including a member check.
Results:
Successful specialised palliative home-care needs to treat complex symptoms, and provide comprehensive care including organisation of care, involving relatives and addressing issues of death and dying. Sense of security for patients and relatives is key to enable care at home. Care delivery preferences include a focus on the quality of relationships, respect for individuality and the facilitation of self-determination.
Conclusions:
Consideration of the identified key issues can help to ensure successful specialised palliative home-care. Knowledge of these should also be considered when researching and assessing quality of care.
Trial registration:
German Clinical Trials Register DRKS-ID: DRKS00012421; http://www.germanctr.de.
Keywords
Specialised palliative home-care enables patients to die at home and supports patients and their relatives in this situation. It aims to promote quality of life and self-determination, but it is not clear how to achieve these aims.
Quality assessment helps address the needs of patients and their relatives and fosters patient-centred care. By evaluating the quality of care, it also reveals potential for improvement.
As specialised palliative home-care focusses on the needs of patients and their relatives, their perspective is essential in any assessment of quality of care.
Successful specialised palliative home-care needs to address the treatment of complex symptoms. It further needs to offer comprehensive care that includes organisation and coordination of care, involves relatives and addresses issues of death and dying.
To enable care and dying at home, a sense of security for patients and relatives needs to be promoted.
Preferences in how care is delivered comprise a focus on the quality of relationships, respect for individuality and the facilitation of self-determination.
The results help specialised palliative home-care teams to recognise and address needs. Improved understanding of what constitutes successful palliative home-care can ensure care is patient-centred.
Both, service providers and policymakers, should take the identified issues into account when planning and organising specialised palliative home-care.
The identified issues should be considered when researching the quality of specialised palliative home-care. They form the basis to develop a method of quality assessment that is adapted to this specific setting and considers the perspectives of those involved.
Introduction
The aim of palliative care is to enhance quality of life in patients with life-limiting diseases. 1 Specialised palliative care provides extensive support to those with complex needs who require a specially qualified team. 2 Evidence shows that most patients would prefer to die at home, and specialised palliative home-care helps patients to continue living at home.3,4 In Europe, more than 2500 teams provided specialised palliative home-care in 2019. 5 Worldwide trend shows an increasing number of palliative care teams and patients cared for, which raises the question of how successful care can be provided and assessed. 6
Quality assessment promotes patient-centred care and helps to address patient needs. 7 Furthermore, it is gaining increasing attention from those responsible for allocating resources. 8 A variety of outcome assessment tools in palliative care exist. They focus on different target groups like patients, relatives, health professionals or the healthcare system and cover different domains, that range from symptoms to spiritual needs.9,10 Some initiatives like the Australian Palliative Care Outcomes Collaboration 11 and the Outcome Assessment and Complexity Collaborative 12 focus on comprehensive approaches to evaluate palliative care. It is recommended to use validated outcome measurement tools, that include patients as well as relatives, are appropriate for the setting they are used in, and cover all relevant aspects of care. 7
In order to improve and to assess the quality of specialised palliative home-care, it is crucial to know which issues influence quality in this setting. Studies indicate that beyond symptom control, further complex issues like security and the organisation of everyday life contribute to successful palliative home-care. 13 Previous studies have examined the views of different stakeholders concerning successful care: Patients and relatives value provision of appropriate resources, reliability and partnership, as well as security and continuity. 14 For the bereaved, the consideration of their own capacity for care, the preparation, presentation and support after death, as well as professionalism combined with humanity are relevant issues.15,16 Health professionals also describe beside anticipation, commitment and flexibility that the teams’ capacity and communication promote successful care.17,18 However, no previous study with focus on specialised palliative home-care incorporated all perspectives combined. Other studies focussed on successful care for patients with specific diseases.19–21 But for a broad-based quality assessments aiming at including every case, the approach should be independent of the underlying disease.
Because patients and their relatives are in the focus of care, their perspective is decisive on which issues are relevant for successful care. Integrating the opinion of health professionals enables a comprehensive view across individual cases. Research is needed to understand what successful specialised palliative home-care means to all directly involved stakeholders, particularly to patients and their relatives, regardless of the underlying disease.
The ELSAH-study (‘Evaluation of Specialised Outpatient Palliative Care by taking the example of Hesse’) aims to implement a set of measures that enables the evaluation of quality of care in specialised palliative home-care (work package I). The study protocol has been published elsewhere. 22 The qualitative study presented in this paper provides the basis for developing an outcome measurement approach. We undertook this qualitative research in order to comprehend what constitutes successful specialised palliative home-care in the opinion of all involved stakeholders. This article follows the consolidated criteria for reporting qualitative research (COREQ). 23
Methods
Study design
Aim of this study was to comprehend what constitutes successful specialised palliative home-care in the opinion of patients, their relatives and involved health professionals. We used a qualitative design based on the principles of Grounded Theory. We considered an inductive design appropriate in understanding the perspectives of those involved.24,25
Setting
The study took place in the state of Hesse, Germany, where all specialised palliative home-care teams are members of the Professional Association of Specialised Palliative Homecare and provide state-wide care. 26 We invited all teams providing care to adults (n = 22) to participate. In Germany, all statutory health insured persons with non-curable, progressive, life-limiting diseases are eligible to receive specialised palliative home-care when they have complex symptoms and associated care requirements that can be met in the outpatient setting. 4 The interprofessional palliative care team includes nurses, physicians and sometimes other professions like psychologists and social workers. 27 They provide outpatient care in familiar surroundings in cooperation with other health care providers, including a 24 h on-call-service. 28 Mean duration of care lasts about 20 days (median 11). 29
Sampling
All participants had to be at least 18 years old, to speak German fluently, and to provide written informed consent. To be eligible, patients had to be receiving specialised palliative home-care. Sampling was purposive and followed the principles of ‘Theoretical Sampling’. 30 When analysis revealed, that relatives have an important role in specialised palliative home care, we contrasted this information by recruiting people living alone to examine their perspective. Furthermore we enhanced inclusion of non-oncologic patients, because our sample included many patients with oncologic diseases.
Health professionals either worked in, or collaborated (hospice service coordinators, chaplains, general practitioners) with specialised palliative home-care. We sampled them by considering their profession, experience of palliative care, team location and team structure.
Recruitment
We contacted health professionals by phone or email. If they were interested in participation, we sent study information. Specialised palliative home-care team members provided patients and relatives with study information. If potential interview partners allowed us to contact them, we called them by phone, gave further information, answered questions and made an appointment. The patients themselves or specialised palliative home-care team members proposed relatives. As no prior relationship with the participants existed, we introduced ourselves and explained that we were researchers. We stopped recruiting, when no new themes emerged from data and data saturation was esteemed to be achieved.
Data collection
Data collection took place from May to November 2017. Every participant received study information written and orally, and consented in a written form. After data collection, participants in the interviews and focus groups were asked to complete a form requesting demographic information.
Interviews
We interviewed health professionals, patients and relatives in order to gain insight into the perspectives of those involved. 31 Two experienced female health researchers (HS, KK) conducted face-to-face semi-structured interviews. In case both, a patient and relative participated, the patient decided whether interviews should be conducted separately or jointly. We asked interviewees to describe their experiences and what successfulness in specialised palliative home-care means for them. We developed semi-structured interview guides for interviews with health professionals, and another one for those affected. We adapted them to suit the interviewee and combined them in jointly conducted interviews (Supplemental Material A). We used them flexibly and carefully navigated difficult issues, while providing the participants with the opportunity to present their main concerns. 32
We audio-recorded the interviews and wrote additional field notes. The interviews were transcribed verbatim following commonly used standards using f4transkript, and pseudonymised.33,34 The transcripts were not returned to the participants.
Participant observations
We (KK, HS) undertook participant observations in specialised palliative home-care teams by accompanying team members throughout the working day. We focussed on interaction between health professionals, patients and relatives to understand how specialised palliative home-care is conducted in practice.35,36 The health professionals introduced the researchers and explained the study. We paused observation, if persons were unwilling or unable to consent, or if health professionals did not estimate observation appropriate. We wrote field notes during car rides or breaks and completed them directly after the observation. The observation reports contained detailed descriptions of situations, interactions, conversations and the researchers’ views.
Focus groups, member check
We conducted focus groups with specialised palliative home-care team members to facilitate the discussion of different perspectives and experiences. Based on the results of interviews and participant observations, we developed a topic guide with focus on how successfulness is incorporated into daily work and how it could be assessed (Supplemental Material B).
We organised a final focus group in March 2018 that involved a member check to discuss whether our results were representative of the stakeholders’ perspectives. 37 For this we invited all team members that had previously participated in interviews or focus groups. We presented our methods and findings and encouraged the participants to discuss them. 38 Two or three of us (HS, KK, SB, JH) moderated each of the focus groups and afterwards reflected the discussion in written field notes. The discussions were videotaped.
Data analysis
According to the principles of Grounded Theory, we undertook data collection and analysis simultaneously. 39 Based on the findings, we reviewed and adapted the samples, as well as the interview and focus group guides (Supplemental Materials A and B) for new emerging issues. By using inductive open coding supported by MAXQDA 2018 software, each analyst (HS, KK, JH, CM) coded the first three interviews, field notes and observation reports. 40 We discussed the coding trees (Supplemental Material C) until consensus was reached. We continued separately and regularly discussed axial coding in team meetings.
In a first round, we used MAXQDA 2018 to code the videos of focus groups thematically. 40 We then discussed all sequences in the research group (HS, KK, JH, SB), and created knowledge maps in a similar way to the method used in Focus Group Illustration Maps. 41 We used this method in order to guide the focus on the participants’ core concepts. Identified key sequences were transcribed verbatim. 34
We triangulated the findings of interviews, focus groups and participant observations by complementing the findings (method triangulation). 42 Finally, we identified key issues using selective coding. As a last step, we conducted the member check focus group. We transcribed the member check verbatim to capture discussions in detail. 34 Then we reviewed our findings by discussion in the research group until consensus was reached to broaden analysis by investigator triangulation. 42
Ethical considerations
We communicated with the caring health professionals before and after contact to patients and relatives to inform about potential incidents. 22 The whole study team is experienced in care and research on vulnerable groups, has undergone training, and was offered supervision. The study was approved by the Ethics Committee of the Faculty of Medicine, Philipps University Marburg (27-04-2017; ref. 34/17).
Findings
Study sample
We interviewed health professionals (n = 30), patients (n = 14) and relatives (n = 14). One of the relatives was bereaved, as the palliative patient had died 3 months earlier. Two patients and two relatives withdrew before the interview because of health deterioration. The interviews with patients and relatives lasted 23–85 min (mean 44; SD 15.8) and took place at the patients’ homes, while interviews with health professionals lasted 27–98 min (mean 55; SD 18.5) and were carried out at their workplaces.
We conducted the five participant day-observations in different teams, and performed 16 home visits overall. Four of the visits were not included in the data analysis because patients were not able to provide their consent. A total of 13 participants attended the three focus groups, which lasted 77–115 min. Seven nurses and one social worker gave feedback in the 94-min member check focus group.
Characteristics of all participants are classified by method and shown in Table 1. Table 2 presents more detailed characteristics of interviewed patients and relatives, and Table 3 the characteristics of health professionals.
Characteristics of patients, relatives and health professionals (HPs), ordered by method.
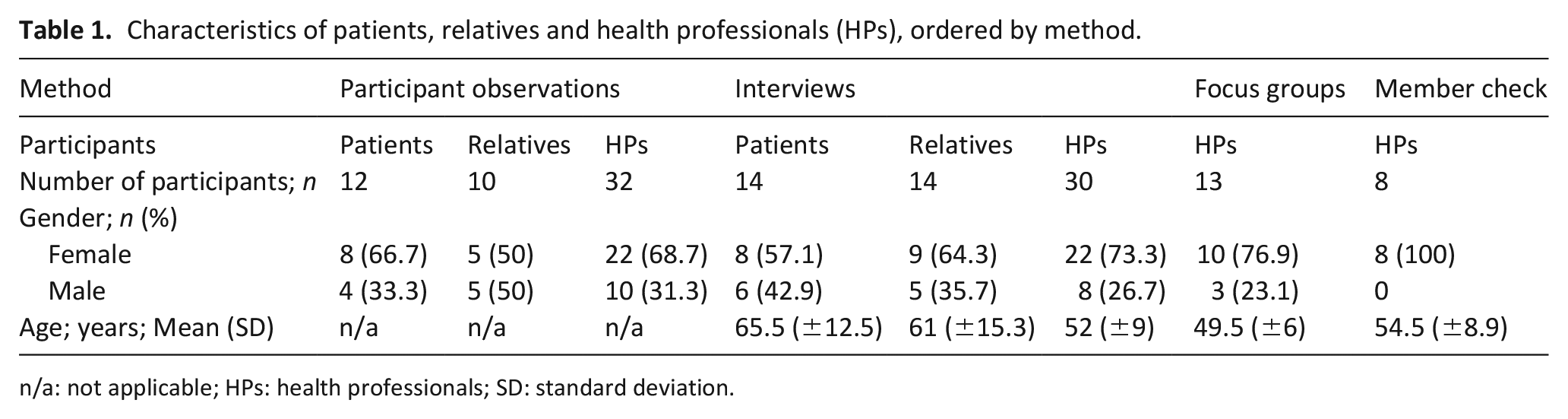
n/a: not applicable; HPs: health professionals; SD: standard deviation.
Detailed characteristics of interviewed patients and relatives.
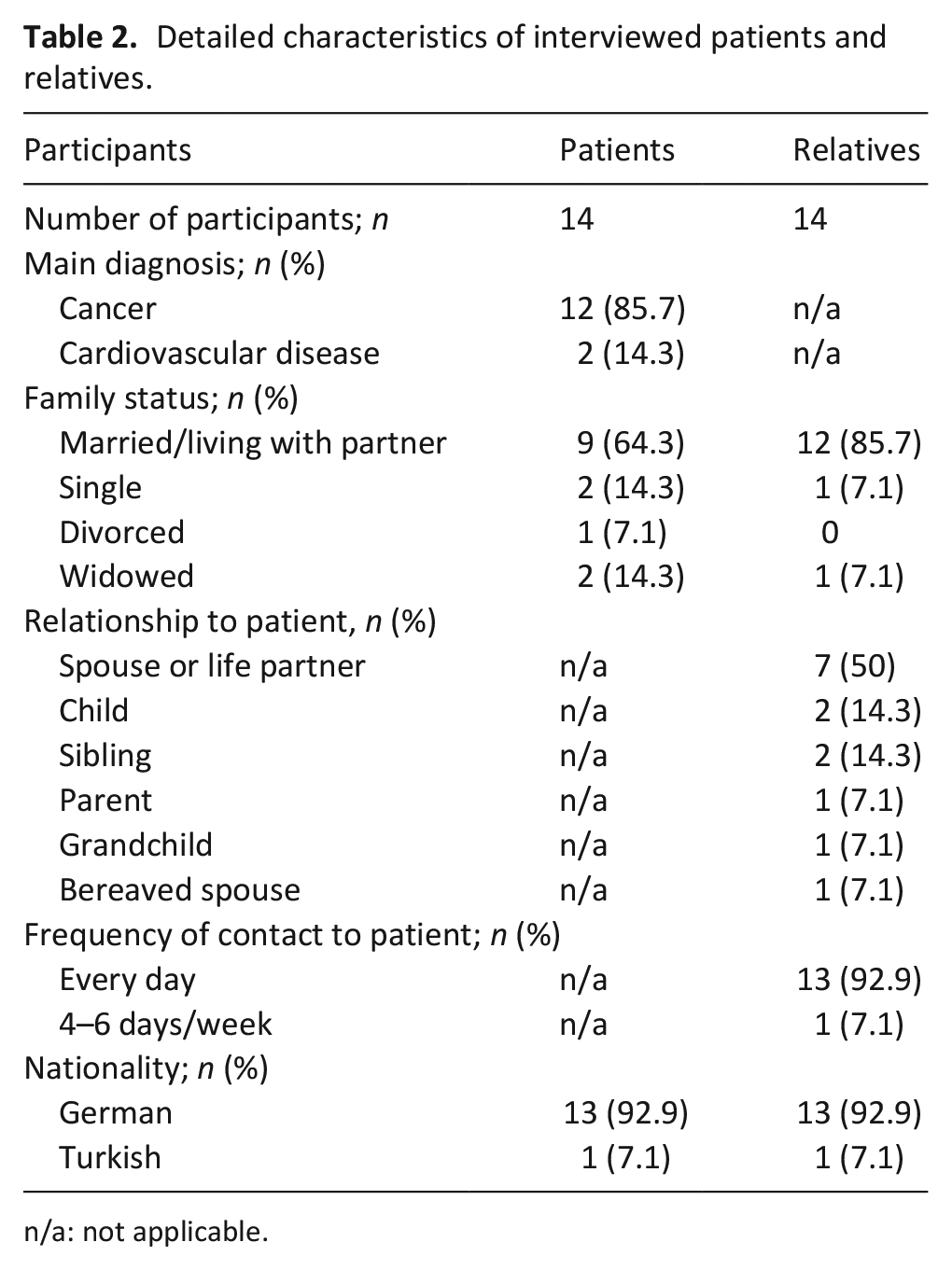
n/a: not applicable.
Detailed characteristics of health professionals (interviews, focus groups, member check).
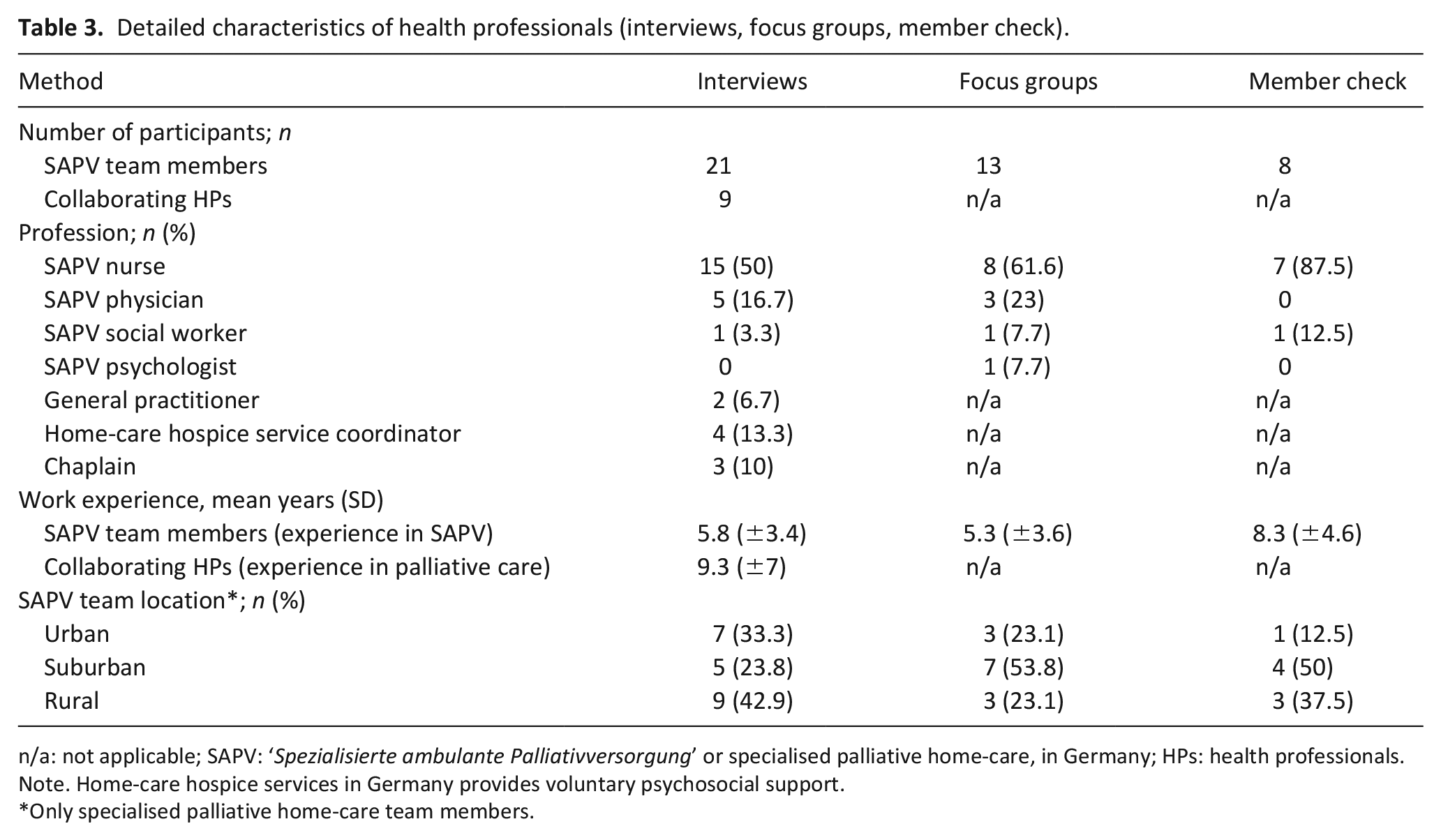
n/a: not applicable; SAPV: ‘Spezialisierte ambulante Palliativversorgung’ or specialised palliative home-care, in Germany; HPs: health professionals.
Note. Home-care hospice services in Germany provides voluntary psychosocial support.
Only specialised palliative home-care team members.
Key issues contributing to successful palliative home-care
We identified six key issues contributing to successful specialised palliative home-care: The main issues were (1) treatment of complex symptoms, (2) comprehensive care and (3) a sense of security. Related issues describing care delivery preferences were: (4) a focus on the quality of relationships, (5) respect for individuality and (6) facilitation of self-determination. Figure 1 presents a model showing how specialised palliative home-care can successfully achieve its aims in this setting. We illustrate our findings with pseudonymised quotations, which we have translated into English.
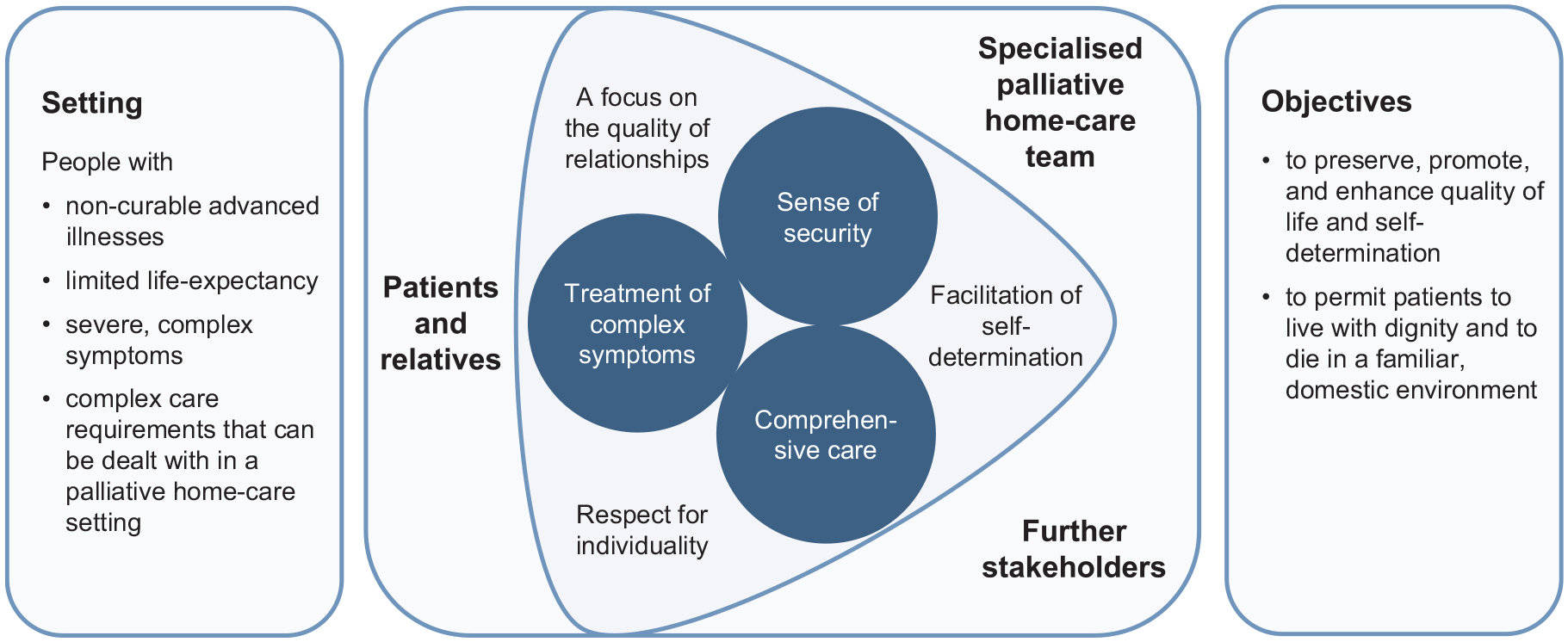
ELSAH model of successful specialised palliative home-care.
Treatment of complex symptoms
Health professionals characterised the treatment of complex symptoms as a key issue. Patients and relatives shared their view:
Well, the most important thing to me is not to be in pain. I’m not afraid of dying but I’m afraid of being in pain or whatever, in my dying days. That’s what I’m really terrified of. (1102P, patient, male, interview)
Study participants throughout the sample described the treatment of complex symptoms as a broad issue made up of physical, mental and emotional aspects.
So, what they give is also emotional support. [. . .] It’s easy to talk about your fears, too. That’s how they really support you. I mean, for me now is the time; it’s not like I can say: “I’ll be cured tomorrow.” It’s more like I’m heading straight towards death. (1312P, patient, female, interview)
Professionals specified that ‘treatment’ means providing the greatest possible relief in accordance with the patients’ will. It establishes trust between the patients, their relatives and the specialised palliative home-care team. It also provides room to take care of other issues that are relevant for patients and their relatives. Observations showed that physical symptoms are often addressed first, then team members initiated an emphatically relaxed conversation, to address other issues.
Comprehensive care
Participants also attached great importance to comprehensive care. This consists of the organisation of care, satisfaction of the patients’ social and spiritual needs and consideration for the needs of relatives.
Organisation and coordination of care, revealed in narratives and observations, included networking with collaborating health professionals, involving further care providers (e.g. home-care services, home-care hospice services, chaplains) and the provision of medication and medical supplies.
Patients and relatives expressed relief at not having to deal with such concerns, and health professionals regarded it as their responsibility:
Basically to be with them on their journey. To make plans. To provide care. To accompany them. To coordinate. To help them with organisational things. [. . .] That is very, very important. Ultimately, the symptoms. [. . .] Everything else, that’s what really helps! [. . .] That is . . . that is what you really notice (sighs) a feeling of relief; that it takes a load off the mind [of the patient] to say: ‘I do not have to worry about that’. (1706E, SAPV physician, male, focus group)
In addition to talking about dying and death in the near future, some patients and relatives raised spiritual topics and patients’ worldviews. Health professionals addressed these topics sensitively during observed home visits, and adapted the conversation to the reactions of patients and relatives. They considered such issues as a relevant issue to handle the palliative situation:
It’s more about, also finding out what gives him strength; what gives him hope. What his view of nature is, of the world outside. . ., to try to find out a bit about what gives him a feeling of courage, what is perhaps able to strengthen him, despite knowing that life is drawing to an end. (1507E, SAPV nurse, female, interview)
During the home visits observed, the well-being, concerns and needs of the relatives were always included, either by asking them directly or by wrapping it up in conversations. Almost all participants emphasised that care for relatives is an essential element of successful palliative home-care. On the one hand, relatives make it possible for patients to die at home, on the other hand, they are personally affected. Some of them described their fear of the actual process of dying and the time afterwards. Accordingly, specialised palliative home-care team members said that part of their work was to provide stability in such a situation.
Quite often there are situations - with some patients - when we go there and spend more time with the relatives than the patient, because they need more attention. But that can help you to manage the whole situation better. (1512E, SAPV nurse, female, interview)
Sense of security
Most participants described a sense of security as a key issue in successful specialised palliative home-care. It provides the basis for care in the familiar surroundings and can be strengthened by five aspects:
Firstly, the teams’ round-the-clock availability, in person and on the phone, was considered important to patients and especially to relatives. While home visits, health professionals strongly encouraged patients to call if needed, to reduce anxiety. Those affected appreciated the fast and uncomplicated response in case of need, and regular contact even in stable periods.
And so I was always lying awake at night thinking: ‘If something happens now, what are you going to do?’ And now I know: ‘Okay, if something happens, you can call palliative care!’ And that's a relief to me. Now I can sleep again! (1306A, spouse, female, interview)
Secondly, health professionals characterised anticipation of needs and precautionary actions as providing a sense of security. This involves consideration of how diseases and symptoms are likely to progress, possible emergencies, overburdened relatives, alternative care locations, explaining the care network and recommending medical supplies. Patients and relatives particularly appreciated consideration of organisational issues.
Several patients and relatives said that being empowered to act in emergencies and deal with everyday matters created a sense of security. Health professionals illustrated how empowerment makes dying at home possible.
Fourthly, observations showed that the health professionals become acquainted with all cases in team meetings. Patients and relatives described relief at knowing the team members, and knowing that they were aware of their needs and desires.
And I have people around [. . .] that know me, my situation, my living situation; that are able to judge what’s going on, and to involve me: What is now the right thing to do? You know? (1316P, patient, female, interview)
Expertise in medical topics as well as in interacting with terminally ill persons and their relatives is the fifth aspects of providing a sense of security.
A focus on the quality of relationships
Participants in all groups mentioned the importance of focussing on the ‘quality of relationships’:
On the subject of QUALITY: One crucial quality of our work that distinguishes it from other work is that we enter into relationships, into personal relationships. [. . .] Despite the professionalism, nevertheless. [. . .] That means I am here as a person, me and you, not just in the role [of a professional; author’s note]. In my opinion, successful palliative care hinges on the quality of relationships. It doesn’t have to be a relationship to all ten team members or whatever, but there have to be moments when personal relationships to certain individuals exist, under the professional umbrella. (1705E, SAPV physician, female, focus group)
Patients and relatives appreciated the attitude of the specialised palliative home-care teams. They said they felt they were treated with respect and dignity, and taken seriously.
I don’t just suffer pain - my prolonged disease caused a load of other illnesses to develop. Not to mention what it has done to my soul. That’s where we also need support, companionship or just somebody beside you that takes you seriously. And who feels for you. [. . .] And that’s what I noticed, [long pause] that these eight weeks [in specialised palliative home-care; author’s note] (-) it was an incredible relief to enjoy feeling and discovering that I am alive again. (1101P, patient, female, interview)
While observed home visits, the specialised palliative home-care team members showed empathy and adapted their behaviour to the patients’ mood. The professionals reasoned that this enables them to identify what matters to patients and their relatives:
You need to establish a kind of trusting relationship with the patient in order to find out about particular problems that are not visible at first sight. In some way or other, in some conversation or other - that’s how you get there, through detours. And so you have to develop a certain sensitivity. (1502E, SAPV nurse, female, interview)
Respect for individuality
Health professionals mentioned respect for individuality as another key issue. The individual wishes are constantly enquired, as the needs and desires of individuals vary:
That they really find their own way. That is success. And in case of SAPV, there is often one banal objective: ‘To make it possible to die at home.’ It’s written everywhere, but sometimes it’s not the right place, right? [. . .] We had a woman with little children, who said: ‘They can see a lot, but they don’t need to see everything. I want to come to your palliative care unit and die there!’ So, this ‘successful for whom’ is one thing, but the other thing is: What does it mean to facilitate the individual way and to take relatives’ needs into account? I think that’s the real challenge! (1705E, SAPV physician, female, focus group)
When asked to describe what quality of life currently means to patients and relatives, a variety of answers are provided: for example, relief from symptoms, to be at home, mobility, independence, a normal everyday life or participation in a social life. That supports the professionals’ view of individual needs and aims. Patients and relatives that talked about the individuality of care welcomed it:
No rigid pattern was offered to me, but a willingness to consider my susceptibilities. And that really is a great help. (1316P, patient, female, interview)
–and to create the conditions where support is possible. (1317A, life partner, male)
Yes! Yes! (1316P)
To makes things possible. And not to offer standard solutions. That is an important difference. (1317A)
Facilitation of self-determination
All participants said that acting in accordance with the will of patients and relatives is necessary for success. This became apparent in participant observations, when health professionals informed in detail about possible treatment, made a recommendation, but also followed the patient’s will when the patient disagreed with their recommendation. Some patients wished to make decisions themselves, while others appreciated sharing decision-making with the health professionals.
It’s not that I was forced to undergo some therapy or other, but rather that a piece of advice is given and discussed by different people. And later on, they have a look to see whether I react positively to the idea [. . .]. We talk about that and then discuss the degree to which it’s good or whether something else would be better, you see? (1312P, patient, female, interview)
Health professionals further described it as their duty to enable patients and their relatives to give informed consent. Fittingly, patients and relatives appreciated it when members of the specialised palliative home-care team provided comprehensible and satisfactory information:
Because of cancer? No idea! I can talk to people about flu, a cold, or something like that, everybody can. But not about this! These are things you hear about, but that don’t affect you! In the personal sphere, nobody! And then the palliative care team came. How they talked to us, explained things to us, the developments. REALLY! Like in ‘Loewenzahn’, the children’s television show . . . in a way a child could understand! Even in the true sense, they were responsive to a child! My nephew. Six years old. They really think of everything! (1404A, sibling, male, interview)
Discussion
Main findings
We identified six key issues that contribute towards successful specialised palliative home-care from the perspective of patients, relatives and the involved health professionals. Participants revealed that treatment of complex symptoms, comprehensive care and a sense of security were key issues, and they wanted specialised palliative home-care to be delivered with a focus on the quality of relationships, respect for individuality and the facilitation of self-determination. Consideration of these key issues enables the objectives of specialised palliative home-care to be achieved: promotion of quality of life and self-determination at the end of life. 4
It is obvious that these key issues are highly interrelated: for example, the quality of relationships, respect for individuality and patient-centred care are preconditions for the provision of appropriate treatment for complex symptoms and comprehensive care. Simultaneously, the effective treatment of complex symptoms and comprehensive care necessitate respect for individuality and the facilitation of patient-centred care, which, in turn, improves the quality of relationships. A sense of security is created when all issues are taken into consideration. Appropriately, a meta-ethnography concluded that a sense of security is key to meeting the needs of those affected because feeling secure provides people with the space to use their remaining time for things that matter to them. 43 The relevance of sense of security is induced by the home-care setting. Although a 24-h on-call service is provided, team members cannot always be on site immediately, especially in rural areas. Additionally, other studies also showed that factors unrelated to care, such as financial worries, also influence sense of security. 44 Here, the diversity of needs to gain a sense of security becomes clear, so that the response must be adapted to the individual situation. The importance of particular key issues can differ between cases, so that for successful care all issues should be considered, but it could turn out that there is no need for action.
As palliative care is complex, 45 good care requires more than the consideration of physical, psychological, social and spiritual wellbeing. 46 We found that by providing comprehensive care, specialised palliative home-care can stabilise a situation involving complex and individual needs. Prior studies confirm the importance supporting relatives because this enables ‘the home’ to continue functioning and prepares relatives for continuing their lives.47,48 This supports the view that the health care system could also benefit from comprehensive care as it would lead to a reduction in follow-up costs.
To strengthen individualised and comprehensive care it can be useful to increase inclusion of other professions like psychologist or social workers in the specialised palliative home-care teams. 49 Other studies have shown that also leadership, education, teamwork and communication influence team capacity and therefore affect ability to provide successful care. 50 A mutual team approach, in which every team member knows the patients’ and relatives’ situations and needs, was also mentioned in an earlier study. 47 Networking with other health care providers can facilitate successful palliative care, but in practice implementation it is difficult due to informal collaborations and different perspectives. 51
Our study revealed that personal relationships play an important role in the provision of successful specialised palliative home-care. In a Swedish study, patients and relatives describe it as a precondition for self-determination. 14 Also, interaction and communication are described as necessary to the organisation of everyday life and therefore for promoting quality of life. 52 Because trust needs time to grow, specialised palliative home-care needs enough time to address the needs of patients and relatives, and should heed early integration. 53 This constitutes, why specialised palliative home-care can only be standardised to a certain degree, but rather needs flexible approaches. 17
Strengths and limitations
Recruiting patients and relatives via the specialised palliative home-care teams may have resulted in more positive feedback, because they rely on the team for continued care. To counteract this, interviews with patients and relatives were conducted without presence of team members and the study team emphasised their obligation of secrecy.
We did not explore elements of non-successful specialised palliative home-care, because recruitment via the caring teams was not suitable for this purpose. However, our rich findings imply that the opposite of the described findings implicate non-successful care. Another study confirmed that neglecting patients’ needs and attaching little importance to the quality of relationships inhibit the success of palliative home-care. 14
The setting of specialised palliative home-care in Hesse could have overestimated our findings, because as members of the Professional Association of Specialised Palliative Homecare of Hesse all teams engage in common quality assurance procedures. 54 It can be assumed that particularly interested health professionals have agreed to participate, but by sampling them by diverse experience of palliative care, team location and team structure, we included a variety of health professionals from different teams.
We involved only one bereaved person, because specialised palliative home-care formally ends with decease of the patient, so that the teams do not accompany mourning of bereaved. To reduce recall bias, which can change the memory of the bereaved over time, we decided to involve mainly persons during care. 55 Although relatives in the 55–69 years age group most frequently care for family members, more younger and older participants as well as more unmarried participants could have been involved. 56 We included mostly persons with cancer diagnoses, which corresponds to the majority of palliative patients in Germany and Europe being cancer patients.2,57 Our predominantly female sample fits to the mainly female healthcare workforce and to the predominantly female informal caregivers.56,58
Although, we conducted participant observations for just 5 days, we included many participants from different groups in various situations. We strengthened our research by integrating different groups in our study, triangulating our methods of data collection and conducting a member check. 42 Data collection and analysis in our interdisciplinary team facilitated the interpretation of results. 36
Implications
To the best of our knowledge, our study is the first to develop a comprehensive framework that has been adapted to the specific setting of specialised palliative home-care based on the views of all directly involved stakeholders, and especially patients and relatives. Similarities to other studies suggest our results are transferable to other regions where specialised palliative home-care for adults is provided. Because care conditions, and the role of relatives in paediatric specialised palliative home-care differ, transferability to paediatric specialised palliative home-care is limited, and needs further research. 59
Taking the key issues into practical consideration can help meet the needs of patients and their relatives. In our study, all participants mentioned the same issues, indicating that health professionals endeavour to provide patient-centred care. Their efforts could be supported by using tools for quality measurement regularly. Moreover, improvements in team performance could be facilitated by evaluating their work with a focus on quality of care. 17 Further research is needed on how different professions and actors in care influence successful palliative home-care and how collaboration networks can be promoted.
Both, service providers and policymakers, should therefore take into account the identified issues when planning and organising specialised palliative home-care. For the evaluation of quality, an assessment system is needed that considers the key issues from the perspectives of those involved, and especially of patients and their relatives. Further research is needed on how best to translate the issues into practice.
Conclusion
Patients, relatives, members of specialised palliative home-care teams and collaborating health professionals described six issues that are important to the success of specialised palliative home-care: The treatment of complex symptoms, comprehensive care and a sense of security, as well as a focus on the quality of relationships, respect for individuality and the facilitation of self-determination. Policymakers and service providers should consider these issues when planning, delivering and evaluating specialised palliative home-care.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163211026516 – Supplemental material for How can we ensure the success of specialised palliative home-care? A qualitative study (ELSAH) identifying key issues from the perspective of patients, relatives and health professionals
Supplemental material, sj-docx-1-pmj-10.1177_02692163211026516 for How can we ensure the success of specialised palliative home-care? A qualitative study (ELSAH) identifying key issues from the perspective of patients, relatives and health professionals by Hannah Seipp, Jörg Haasenritter, Michaela Hach, Dorothée Becker, Lisa-R Ulrich, Dania Schütze, Jennifer Engler, Cathrin Michel, Stefan Bösner and Katrin Kuss in Palliative Medicine
Footnotes
Acknowledgements
We would like to express our gratitude to the patients and relatives that were willing to talk to us about their experiences in a difficult phase of life. We also thank all members of the specialised palliative home-care teams in Hesse for their participation and engagement. We would further like to thank Jasmin Buller for transcribing the data, Phillip Elliott for the linguistic revision and Sebastian Tischler from the Regional Management of northern Hesse for his administrative support.
Author contribution
MH, SB, LRU and JH devised this project and secured project funding. HS, KK, JH and SB collected, analysed and interpreted the data and wrote this draft of the paper. MH and DB supported the recruitment of participants and prepared the study team for and supervised them in dealing with terminally ill patients and their relatives. CM, JE, DS, MH and DB assisted in the analysis and interpretation of data. All authors revised the paper and approved the final version. Authorship follows ICMJE recommendations.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MH and DB manage the Professional Association of Specialised Palliative Homecare in Hesse. SB, JH, KK, HS, LRU, DS, JE were employed as researchers at the universities of Marburg and Frankfurt. All authors declare that there were no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Innovation fund (‘Innovationsfonds’) of the Federal Joint Committee of Germany (grant number: 01VSF16006).
Research ethics and patient consent
The study was conducted according to the Declaration of Helsinki. It was approved by the Ethics Committee of the Faculty of Medicine, Philipps University Marburg, Germany on 27th April 2017 (ref. 34/17). It is registered in the German Clinical Trials Register (![]() , DRKS00012421), which is the primary WHO-acknowledged trial register in Germany. All participants gave their written informed consent before inclusion in the study. Consent form and other relevant information will be provided to participants on request.
, DRKS00012421), which is the primary WHO-acknowledged trial register in Germany. All participants gave their written informed consent before inclusion in the study. Consent form and other relevant information will be provided to participants on request.
Data management and sharing
To protect the participants’ privacy, no original data can be released, but online supplemental material on data collection and analysis is provided.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.