
Abstract
Background:
Pediatric palliative care has established benefits for children with cancer and their families. Overcoming organizational and healthcare provider barriers have been demonstrated as central for the provision of palliative care in pediatric oncology. A deeper understanding is needed of the influence of these barriers and the interactions between them, specifically in primary palliative care in hospital settings.
Aim:
To identify the organizational and healthcare provider barriers to the provision of primary pediatric palliative care.
Design:
This study utilized the grounded theory method. Semi-structured interviews were conducted and analyzed line by line, using NVivo software.
Setting/participants:
Forty-six pediatric oncologists, nurses, psychosocial team members, and other healthcare providers from six academic hospital centers participated in the research.
Results:
Organizational and healthcare provider factors were identified, each of which acted as both a barrier and facilitator to the provision of pediatric palliative care. Organizational barriers included lack of resources and management. Facilitators included external resources, resource management, and a palliative care center within the hospital. Individual barriers included attitudes toward palliative care among pediatric oncologists, pediatric oncologists’ personalities, and the emotional burden of providing palliative care. Facilitators include dedication and commitment, initiative, and sense of meaning. Provider facilitators for palliative care had a buffering effect on organizational barriers.
Conclusion:
Organizational and healthcare provider factors influence the quality and quantity of palliative care given to children and their families. This finding has implications on interventions structured to promote primary palliative care for children, especially in healthcare systems and situations where resources are limited.
• Pediatric palliative care is defined by the World Health Organization (WHO) as the total care of the child’s body, mind, and spirit, and has been recognized as a basic human right.
• Pediatric palliative care reduces children and families’ suffering and improves their quality of life.
• Specialized palliative care teams improve care, but are often absent or underutilized. Therefore, primary oncology healthcare providers are the central, and occasionally, the only providers of palliative care for children with cancer.
• This study demonstrates pediatric oncology multi-disciplinary teams’ understanding of the organizational and provider barriers and facilitators to the provision of primary palliative care for children.
• Pediatric oncology teams report lack of resources and mismanagement of existing resources as central organizational barriers to provision of primary palliative care. They acknowledge the negative influence of attitudes, personality attributes, and emotional burden on primary palliative care.
• Organizational and provider factors are interrelated. Pediatric oncological teams report that provider facilitators for palliative care, such as dedication, availability, and initiative, have a buffering effect on organizational barriers.
• Policy makers should consider both organizational and individual factors, as well as how they interact, when striving to promote better care models for primary pediatric palliative care worldwide.
• There is a need for more research to unravel the relationship between different barriers and facilitators in pediatric palliative care. Results may improve the provision of primary and specialized pediatric palliative care services.
Introduction
Pediatric palliative care is a holistic field related to the treatment of children and their families. It is defined by the World Health Organization as the total care of the child’s body, mind, and spirit 1 and has been recognized as a human right. 2 The efficacy of the field in reducing suffering is well-documented for children with oncological diseases. 3 Nevertheless, it is often underutilized, thus evoking the interest of both researchers and policy makers who have called for further research in the field.4–7 Literature reviews indicate that care-models that include both primary and specialized palliative care teams are preferable because they reduce suffering and increase management of symptoms.3,8 While aspiring to develop this two-layered model, many countries still base their services on the primary pediatric oncology team model where oncologists and nurses are responsible for both curative and palliative care. 9 Moreover, in countries that do have pediatric palliative care expertise, the demand for services often exceeds availability. 10 The heterogeneity of the field11,12 was demonstrated in a recent study of 18 countries in which 25% of the pediatric oncological medical settings did not have palliative care programs, and 7% did not have any palliative care services available for patients receiving cancer-directed therapy. Access to palliative care is more widespread in the United States and other higher income countries.13,14 This suggests a significant gap in care, as the vast majority of children under the age of 19 who are in need of palliative care live in low and middle-income countries. 14 Thus, improvement of primary palliative care accessibility is needed worldwide.
Barriers to the implementation of pediatric palliative care have included the patient and the family, as well as insurance coverage.8,15–17 For example, one study found the most frequently reported barriers to palliative care by providers were families’ preferences for life-sustaining treatment and not being ready to acknowledge situations where cure is not possible. 17 Another study found that though adolescents stated that is it important to inform their caretakers of their end of life wishes, half of the participants surveyed didn’t talk to anyone about their preferences. 16 The important role of the primary healthcare provider has also been identified in studies on barriers to pediatric palliative care implementation including the provider role, conflicting philosophies about palliative care, and emotional relationships with patient/families.15,18 Additional barriers included provider beliefs that palliative care cannot be delivered concurrently with curative cancer treatments, discomfort talking about death, 8 and perception that there is little or no benefit in incorporating palliative care at end of life. 13 More recently, in the mixed-methods study published by Cuviello et al., 19 healthcare providers acknowledged their discomfort with providing palliative care as a barrier, mentioning both difficulty with end-of-life care and conflicting goals of care.
Organizational barriers also have critical implications for the provision of pediatric palliative care.13,20,21 These include: fragmentation of care within complex health system settings, challenges of coordinating multidisciplinary teams, 8 and difficulty in selecting and adapting a working model that fits the medical setting and context.8,22
Pediatric palliative care in Israel: The research cited above was mostly conducted in the United States and Europe, and recognizes the significance of organizational and provider-level barriers.8,15,19,21 The current study, took place in Israel which has an advanced healthcare system with free national health insurance coverage for all citizens.23,24 Nevertheless, palliative care provision for adults, and especially for children is in the development stages, and is not widely available. In this sense, Israeli palliative care programs are an interesting case study because of the advanced level of the overall healthcare system as compared to the sparse availability of palliative care for the population. The Israeli palliative care development process may resonate with other places in the globe where palliative care for children and their families has only recently been implemented.
In a recent mapping of pediatric palliative care in the European region, the authors note that 92% of palliative care services are offered in countries that are classified as high-income. This statistic included Israel, however, both Israel and Ireland provide some pediatric palliative services by adult specialists who do not have any special training in pediatrics. 9 In the United States, palliative care specialists are available in most centers caring for children with cancer, but their integration level is diverse. 13 Switzerland also reports deficiencies in resource allocation to palliative care, as well as providers’ challenges in communication and attitudes toward end of life care. 25 In Australia and Holland, unmet palliative care needs of parents for off hour support, respite, and home support were also reported. 26
In Israel, palliative care was recognized as a medical specialty in 2013 and a nursing specialty in 2009 and mostly focused on the treatment of adults.27,28 The vast majority of pediatric palliative care is provided in hospitals by primary oncology teams. Cancer centers for children have at most one physician with formal palliative care training, 28 and only one pediatric oncology unit provides a combination of hospice care hospitalization with palliative care throughout the illness trajectory. 29 Due to the lack of information on pediatric palliative care in Israel, in another paper, our study team looked at how the field is defined by pediatric oncologists. They reported that in their view, pediatric palliative care includes symptomatic treatment and pain relief, promoting quality of life, enabling curative treatment, and promoting quality of death. 30
In this study, we sought to identify the barriers and facilitators to the provision of primary pediatric palliative care, as this is the predominant means of providing palliative care for children suffering from cancer worldwide.
Methods
Research question
This study is part of a larger project exploring pediatric palliative care in Israel. Earlier findings from the project reflected on oncologist conceptualizations of pediatric palliative care and the relationship between the physician and patient/parent.30,31 The current study looked at barriers and facilitators to the provision of primary palliative care for children with cancer.
Study design
We utilized the grounded theory method of data collection and analysis which was based on the epistemological and ontological constructivist philosophy of knowledge being a product of multiple viewpoints, theories, and concept synthesis.32,33 Hence, researchers’ professional backgrounds and personal life events were reflected upon as motivators for study initiation and monitored during the process of conducting this research for potential bias. The first author works as a health psychologist in Israel with adult oncology patients, and thus, has an acute awareness of differences in needs and availabilities with pediatric population when it comes to the provision of palliative care. The second author is a Canadian health psychologist and professor with extensive experience researching oncological palliative care for children. The third author is an American pediatric oncology social worker and is world-renowned for her work on palliative care for children. These authors’ extensive experience in the fields of palliative care for children within oncology provided the research context for this work and their international locations highlighted the similarities and differences in cultural and organizational perspectives and practices in providing palliative care to children. The fourth author is a health sociologist, with extensive experience in qualitative research focusing on healthcare organizations, policy, and personnel. The fifth author is a senior Israeli pediatric oncologist with a specific interest in pediatric palliative care who provided clinical expertise and face validity to the findings. Furthermore, to ensure research rigor, we followed Tracy’s (2010) principles of qualitative research that includes selecting a worthy topic, implementing a rich rigor, sincerity, credibility, resonance, significant contribution, ethics, and meaningful coherence throughout the process of data collection and analysis. 34
Population and setting
The sample consisted of 21 pediatric oncologists, 9 nurses, 10 mental health professionals including social workers, psychologists, and psychiatrists, 2 physicians including palliative care and radiation oncology experts, and 4 other support therapists including art therapists, bibliotherapists, and acupuncturists. Inclusion criteria included working as a clinician in one of the six pediatric oncology centers. Most interviews took place in medical academic centers that treat children with cancer. A few interviews were conducted in another location such as a coffee shop.
Sampling and recruitment
We used theoretical sampling to ensure variation and interviewed providers at various stages in their careers from all six pediatric-oncology medical centers in Israel. Recruitment took place between November 2017 and January 2019. Co-investigators at each center sent out invitations by email to potential participants. Forty-six providers working in pediatric oncology responded to the email, and thereafter, contacted by the researcher. All those who responded to the email agreed to participate in an interview after hearing more about the research goals.
Data collection
Interviews were conducted by the first author, a trained health psychologist with vast experience in psycho-oncology, who had no prior acquaintance with the study participants. The interviews were scheduled one-on-one at a place and time convenient to participants. All participants signed a written consent form prior to the interview. A semi-structured interview guide was used containing questions related to barriers and facilitators for integrating pediatric palliative care (Appendix A). Interviews lasted between 35 and 100 min and were digitally recorded, anonymized, and transcribed.
Data analysis
Data was collected and analyzed concurrently. 35 Inductive analysis was used with line-by-line coding of participants’ narratives, to allow codes, categories, and themes to emerge from the interview data. Constant comparison was used to understand the relationships between emerging codes. Coding was done by first author, and team meetings between the study PI (second author) and the co-investigators were conducted regularly during data collection and analysis to discuss preliminary findings, evaluate data, and challenge emerging conceptions. Memo writing throughout the study helped increase the level of abstraction and form theoretical categories. 32 To validate our findings, we incorporated peer debriefings and team meetings with co-investigators, national and international experts in the fields of pediatric oncology. Once we reached data saturation and no new codes emerged, data collection ceased. NVivo software was used to manage the coding process and to organize and store the data.
Ethical issues
Research ethics board committees approvals were obtained from the of the participating centers (No. 1532-1, Date 28.07.2017; No. 4424-17, Date 3.10.2017). Participants were offered access to psychological help if they experienced distress after the interview, however, no participants requested such a debriefing.
Findings
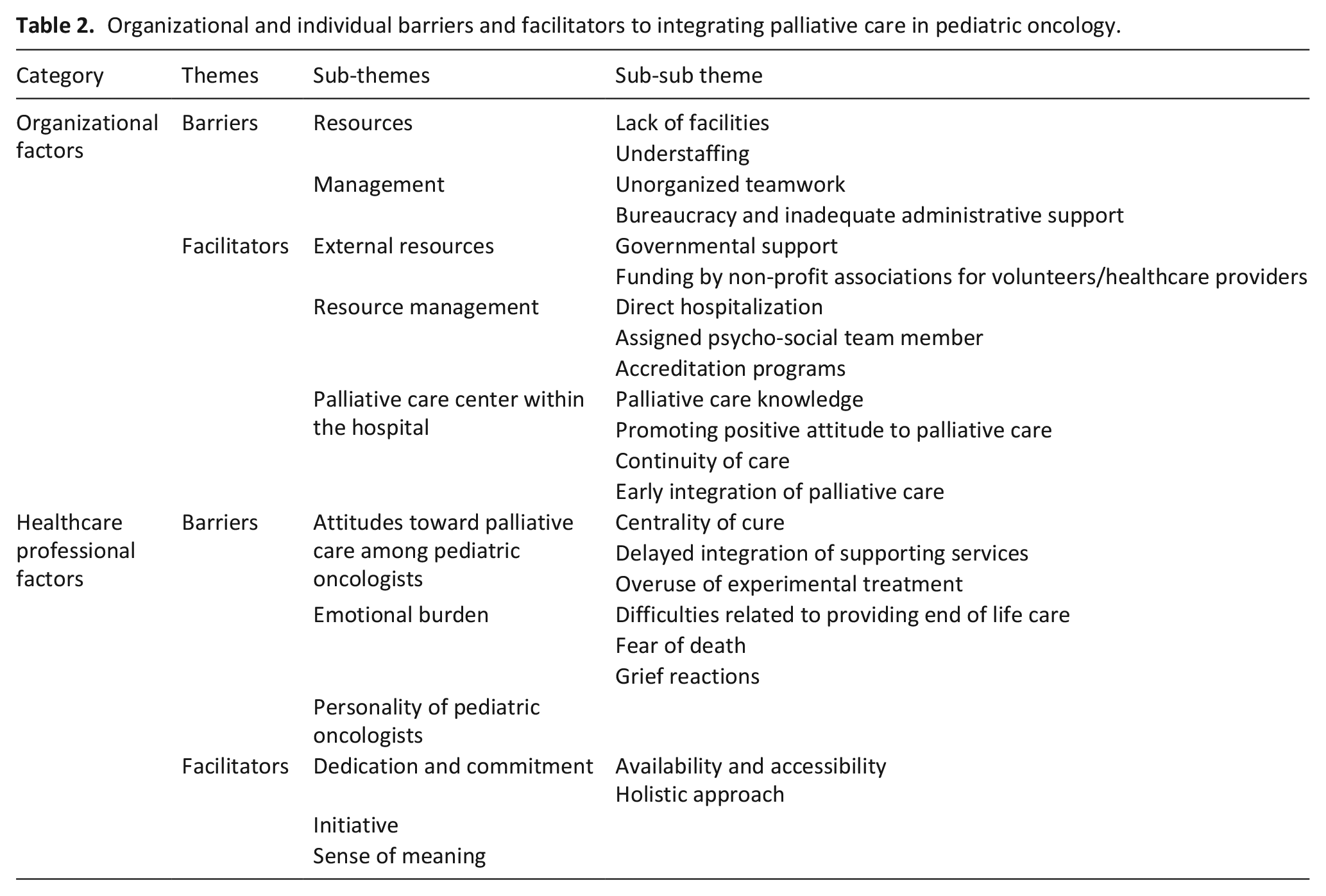
Forty-six providers working in pediatric oncology were interviewed (See Table 1 for demographics). Our analysis revealed two major themes that were described as both barriers and facilitators to integrating pediatric palliative care. The first involved organizational factors and the second pertained to healthcare provider factors (Table 2). Participants referred to the interactions between organizational and provider factors in several ways as is illustrated in our conceptual model (Figure 1). Facilitators could compensate for barriers or the reverse, barriers could place increasing burden on the facilitators. For example, organizational barriers were noted as augmenting provider barriers so that lack of resources for the provision of palliative care, increased the emotional burden on the healthcare provider. In the section below we present our findings with supporting quotations.
Participant demographics.
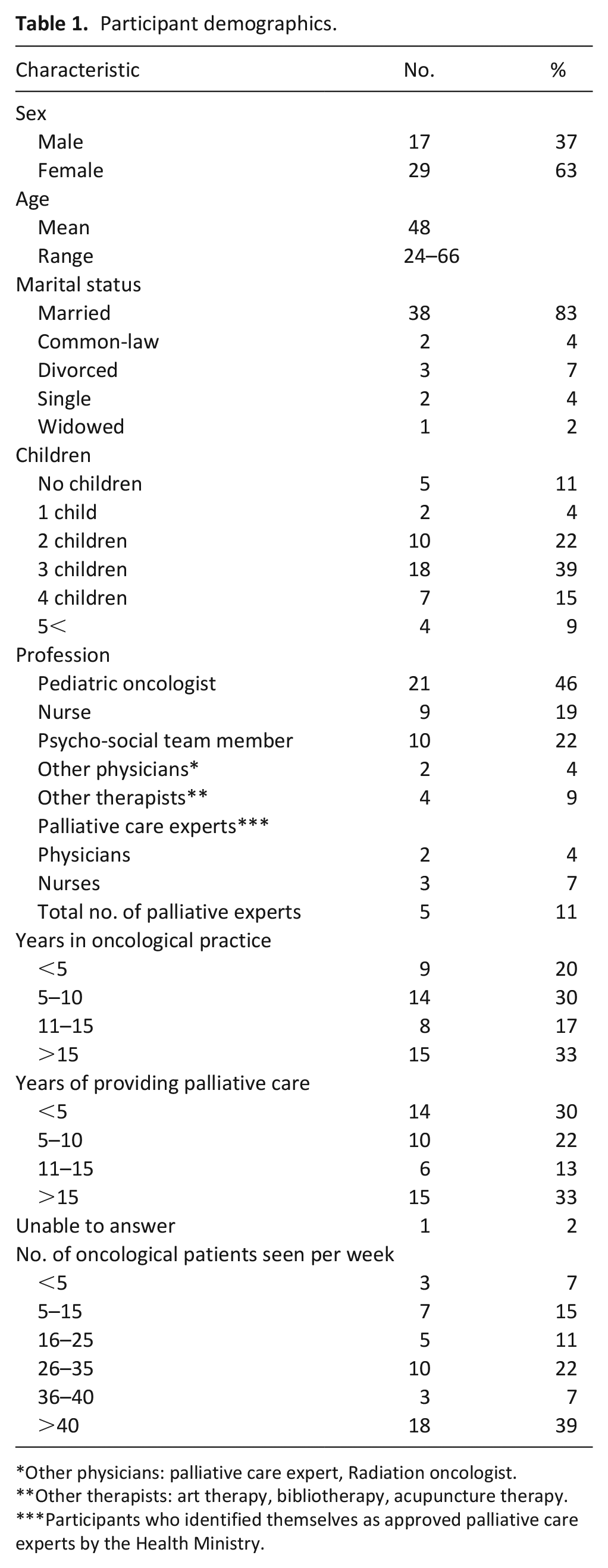
Other physicians: palliative care expert, Radiation oncologist.
Other therapists: art therapy, bibliotherapy, acupuncture therapy.
Participants who identified themselves as approved palliative care experts by the Health Ministry.
Organizational and individual barriers and facilitators to integrating palliative care in pediatric oncology.
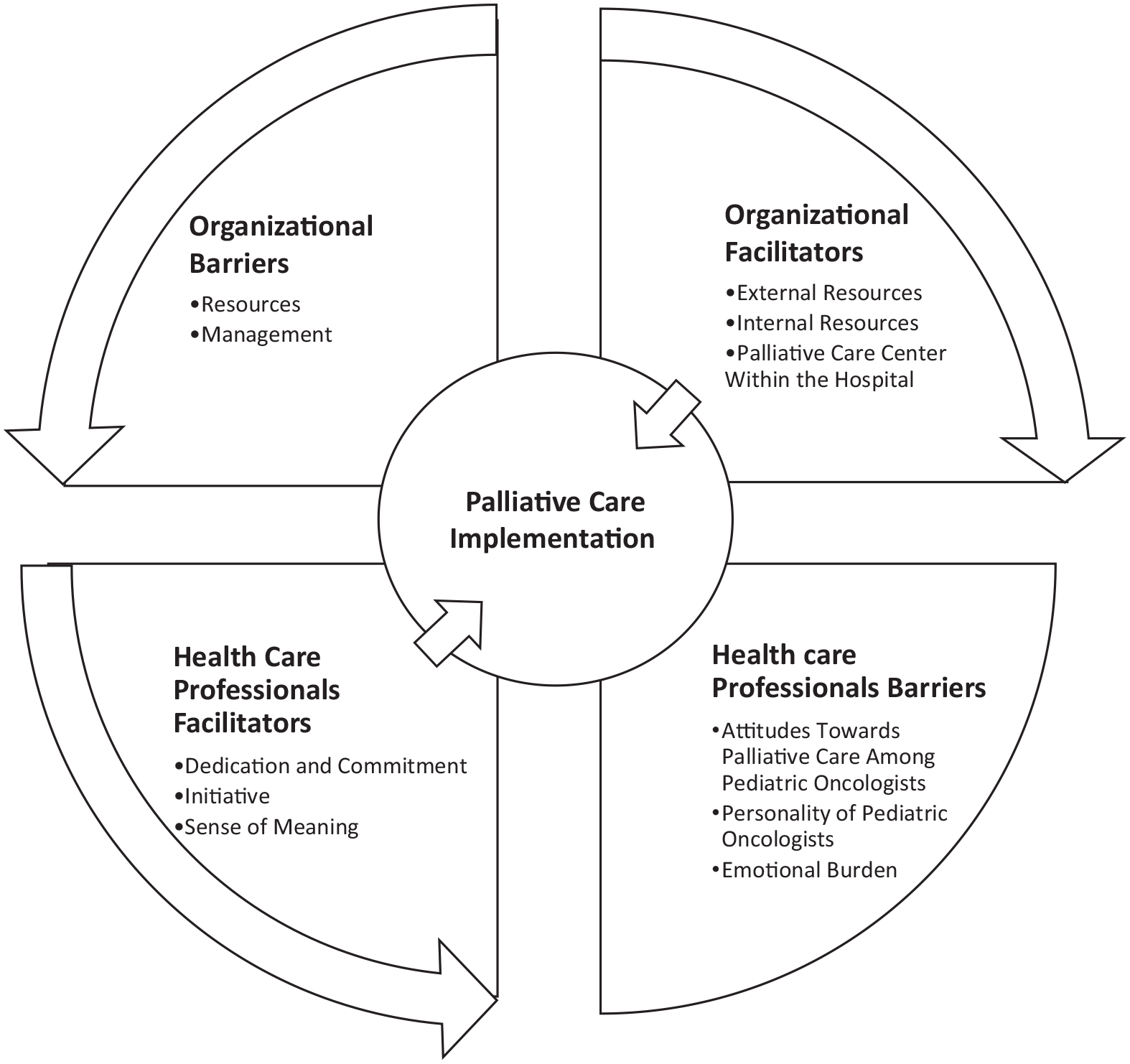
Organizational and individual factors effecting palliative care implementation and their interrelations.
Organizational factors influencing the integration of palliative care
Healthcare providers described organizational factors that impact their ability to provide appropriate palliative care. Barriers were related to resources and management, whereas facilitators were related to external resources for palliative care, management of palliative care resources, and having a palliative care center within the hospital.
Organizational barriers
Resources
Resources deficiencies were central, described frequently by participants as a barrier to the provision of palliative care.
Lack of facilities included treatment rooms, private rooms for end of life care, and beds and chairs for the child and the caregiver. A nurse described the severity of these shortages and the distress they caused: “I don’t have enough chairs for people to sit on. It’s that bad. Children! Not to mention that the mother should also have a chair to sit on. . . People sit like sardines. I feel so bad about it” (17NU).
Understaffing
Providers reported that being understaffed resulted in work overload and high turnover rates. One nurse reported, “There is an overflow, an overflow of needed treatments and you need to do them all” (18NU). Another nurse referred to the turnover rates as “something I can’t even begin to describe. It is enormous” (1NU).
This shortage challenged time allocated to palliative care in a more pronounced manner than cure-oriented treatments, as one pediatrician explained: We have many, many, patients here. Many, and not a lot of personnel. Everything depends on the workload. . .I’m sure that given time, everyone would like to sit in their rooms, have time to talk about other things, get to know the patient. (9PO)
Management
Unorganized teamwork
The organizational challenge of managing multi-disciplinary teams providing primary palliative care was noted.
There are no multi-disciplinary meetings to discuss the child [with palliative needs]. It is very unorganized. No updates. Sometimes someone will say something in the morning. . . Here, it is more about putting out fires. . . children come in with relapses, and new children are continuously added. Nobody has the time to stop and conceptualize what has happened so far. (32BIBLIOTHERAPIST)
The lack of organized multi-disciplinary work was also illustrated in providers’ descriptions of the referral procedures for primary palliative services, impacting both treatment frequency and standardization. A social worker reported: Yeah, it will sound absurd, but it works very. . . through all kinds of informal channels. Ideally, the medical team would let us know that a new patient is about to get a diagnosis. This rarely happens. In practice - it will sound ridiculous, but we kind of hunt them down. (2SW)
At end of life, the lack of an organized multi-disciplinary team dedicated to palliation was to add unnecessary strains on the care providers. As one pediatric oncologist remarked: “There’s no team that I tell: ‘we have a patient at end of life, so please come and help me’. No. I need to construct a puzzle to help the patient" (43PO).
Bureaucracy and inadequate administrative support was another aspect of ill-management that caused depletion of resources that would otherwise be allocated for palliative care. On this, one acupuncturist remarked: I manage my own appointments. I guess that if there was something more organized it would be better. I have 8 hours a week to treat all the children I can find. . . It affects the quality and quantity of the work. The same goes for social workers and psychologists. (11ACUP)
Organizational facilitators
External resources for palliative care
This included government support for home hospice care, and non-profit associations that fund healthcare provider and volunteer positions. These volunteers are part of the clinical routine and “are considered semi-professionals as if they are part of the palliative care team” (40PO). External resources were described as providing children continuity of care outside the hospital, increasing the number of available healthcare providers, and adding to the care of non-professional staff.
Management of resources
Direct hospitalization
Internal hospital facilitators of palliative care included the hospitalization of children directly in an oncology ward without spending unnecessary, and sometimes potentially life-threatening time in the Emergency Department. This was especially important at end of life, allowing for both continuity of care by known personnel, and dynamic decision making regarding the place of death. A palliative care nurse noted: They can stay home most of the time and feel safe, to an extent, and near the end decide that they want to come here. . .Go back and forth, and at the end die here. Ultimately, they trust the familiar staff here. (39NU)
Assigned psycho-social team member
A second internal resource mentioned was related to psycho-social services and how “a newly diagnosed patient is automatically assigned to a social worker” (12PO). Social workers were responsible for case management of in-hospital supportive services and aid with family financial insecurity. This process enabled early integration of a palliative holistic approach and family care.
Accreditation programs
A third resource included hospital enrollment for international healthcare accreditation programs such as the Joint Commission International, an organization that assesses and promotes quality of healthcare based on international standards. Accreditation programs were noted to help organizations implement international standards for palliative care.
Palliative care center within the hospital
One hospital reported having a specialized palliative care center for pediatric oncology inpatients, with continuity of care by teams from the main oncology department. Other advantages of this service included the distribution of high-level palliative care knowledge, promoting positive attitude to palliative care, and early integration. When describing how palliative care is integrated and continuity of care is ensured, a nurse explained: The child can be in the hospital for his first treatment but diagnosed with Ewing sarcoma that metastasized to the lungs. We will do our best to bring him here because the chances that we will meet later are very high. (1NU)
Healthcare professional factors influencing the integration of palliative care
Healthcare provider barriers to integrating palliative care included attitudes toward palliative care among pediatric oncologists, the emotional burden of providing pediatric palliative care, and the personality of pediatric oncologists. Provider facilitators for integrating palliative care included dedication and commitment, taking initiative, and sense of meaning.
Healthcare professional barriers
Attitudes toward palliative care among pediatric oncologists
Centrality of cure
Pediatric oncologists’ focus is on curing the child. As such, some considered palliation to be peripheral to their work. The following two quotes by different pediatric oncologists demonstrate how deeply this attitude is entrenched. One remarked, Even if we do the best we can, we are still as a team, “a heal me team”. This is our training. This is what we do daily. Palliative care here, in my opinion, will always be a somewhat lower priority. (34PO)
Another similarly noted, “Pediatric oncology for me is 82.5% cure. When I chose pediatric oncology, it was not related to palliative care. Not at all and it still isn’t” (37PO).
Delayed integration of supporting services
The centrality of cure was mentioned as delaying integration of available primary palliative care supporting services, as they benefit from pediatric oncologists’ referral. On this, one social worker noted: “I think that they are very aware of the importance of palliative care and emotional treatment for children and their families. But they don't always think of it. . . they don’t always refer their patients” (3SW).
Overuse of experimental treatment
Continuation of cure-oriented treatment at end of life was communicated as a widespread practice. As one pediatric oncologist recalled, “Someone once told me a joke. What is a hematologist? Someone who runs into a funeral saying, ‘Just a minute I have another line of treatment to offer’” (38PO). A senior nurse reflecting on her experience added that “it is very easy to offer treatment and very hard not to. . . I hardly remember cases when parents are told their child is going to die” (20NU).
Though participants stated that it was easier to offer treatment, some spoke about the emotional distress this entails: “You understand that you are not helping. That it can cause additional suffering. But not to give it. . . I mean it is not acceptable to hold back those treatments. It is the new standard” (36PO).
Emotional burden of providing pediatric palliative care
Emotional factors were mentioned as a significant barrier that can delay or prevent the integration of a palliative approach.
Difficulties related to working with children at the end of life and healthcare providers’ fear of death emerged, as noted in the following quote by a pediatric oncologist: Pediatricians in general are afraid, distant, anxious. As a result, they don’t offer the service, don’t offer palliative care. They don’t know that there is something that can be done. Especially with a dying child, a very sick child, many emotional layers of the caregiver are blocked . . . Also, in the haemato-oncological community, some don’t know enough. They don’t want to know, they’re afraid to say the horrible and terrifying word “death”. It is horrible for them. (23PO)
The tendency to withdraw when encountering end of life situations was described as well.
It doesn’t suit everyone to work with children at the very end [of life]. Especially when the child barely gets up or is anesthetized and ventilated, or in the ICU. It really depends. The majority don’t. . . don’t. . . don’t like to go there. It is not comfortable for them. (32BIBLIOTHERAPIST)
Grief reactions reflect another aspect of the emotional burden of palliative care provision. As one pediatric oncologist recounted: When my children were small, I used to go to parties at their kindergarten. And there wasn’t a single thing that didn’t remind me, a picture, even the songs, “good morning to. . .” immediately pictures run through my head of a child taking his last breaths, where the mother played him these songs. And I’m sitting in the kindergarten and listening. It is physically, physically just awful. (6PO)
Personality of pediatric oncologists
Participants spoke of personality attributes such as optimism as related to continuity of cure-oriented treatment at end of life, which functioned as a barrier to the implementation of palliative care treatments and decision making. Being empathic and compassionate were spoken of a personality attributes that promoted palliative centered treatment and development of pediatric palliative care. They also noted that implementation of palliative care depends on provider factors such as upbringing, personal values, and personal outlook of end of life.
This, diversity in palliative care between physicians emerged repeatedly in the participants’ interviews. On this, one oncologist said: Everyone is different in the way they understand it [palliative care], and how they present what they do. I’m not sure, it is very difficult, this thing. Because it depends on your personality, you can’t help it. How much you can take, how emotional you are, how much compassion you have, how much empathy you have at the moment, how connected you are to the situation and the child. Do you want to be there or not. (9PO)
Healthcare professional facilitators
Dedication and commitment
Availability and accessibility
Being available and accessible to parents and children was described as promoting the quality of palliative care. Use of a personal cell phone and an open-door policy are some of the many examples that were given to illustrate this availability that extended 24 hours a day, 7 days a week. Facilitation of palliative care by offering personal time was reported to begin at the child’s diagnosis and increased if the child’s disease progressed and cure was no longer an option.
When you get to this stage [end of life], I think every member of the staff, regardless of the patient load and how many patients are waiting; they are touched on a different level emotionally. I see my attitude towards patients that are near the end of life. How they occupy my thoughts, how much time I dedicate to them, how flexible my hours become. (13PSY)
Holistic approach
Dedication and commitment promoted a style of care that went beyond the call of duty, which facilitated a holistic, family-centered approach. On this, one pediatric oncologist remarked: “I’m a physician but I’m also a friend and a brother and a father. I’m everything. And I think that though that comes with a price, it can’t be done differently” (36PO).
This was also reflected in an account by an oncologist who visited the home of a mourning family during the traditional Jewish mourning period: Suddenly he [the father] said to a friend near him, “You know what this physician offered me? One Thursday I told her that I was staying in the hospital without leaving, so she said to me ‘I’m on the way to the supermarket. Do you need anything?’ I didn’t even remember that I said something like that. The father said, ‘That is what I needed at the time’”. (15PO)
This theme reflected healthcare providers’ understanding that being there for the children and their families both emotionally and practically is an essential part of how they practice palliative care.
Initiative
Providers enhance palliative care implementation by initiating institutional changes and maintaining a pro-active approach to palliative patient care. Senior oncologists spoke of demanding and advocating for a multi-disciplinary staff when building their units to support the provision of palliative care. Psycho-social teams members proactively reached out to children and families to improve their quality of life. Other healthcare providers reported dealing with bureaucracy and regulations to incorporate innovative medication that could improve symptom management. On this, one oncologist explained: Initiative is when you establish procedures. Initiative is also when you overcome shortage and utilize things that you have. Indeed, it is often said that the system is poor, lacking resources. But I think that you can procure them. Most situations have a solution, you need to draw it in favor of the palliative patient. (34PO)
Sense of meaning
While some avoided emotionally difficult situations, others found meaning in palliative and end of life care. “I need to be capable of really listening to the hardest things. And if I can’t, it will not be the place for me.. . .I see it as a calling to be there for these people in these places” (10SW).
Sense of meaning was described as being related to personal history, which included experiences with death and the individual’s worldview. On this, one nurse noted, “Suffering is a lot worse than death itself. After you die you are in a world that is much better. I don’t know if it’s really better, with heaven or without. But preventing pain, it is my essence” (NU29).
Interrelationship between the findings
In Figure 1, we outline the ways in which our findings on barriers and facilitators interact to affect one another in a symbiotic relationship. For example, the findings illustrate that organizational barriers such as lack of resources were counter-balanced and compensated for by facilitators such as individual providers’ dedication, commitment, and initiative in providing palliative care. Similarly, lack of effective management and lack of standardized pediatric palliative care caused more barriers so that individual pediatric healthcare provider attitudes toward palliative care influenced whether it was provided or not. On the other hand, this lack of standardization also allowed for individual clinician factors such as personality traits to influence pediatric palliative care provision in some centers. Emotional burden was noted to be connected to lack of resources as providers felt they could not provide an adequate level of care and sense of meaning as a way to better endure the emotional burdens caused by treating children with life threatening diseases. Finally, a palliative care center, which was named as an organizational facilitator, promoted providers’ positive attitudes toward palliative care, and therefore, influenced individual barriers.
Discussion
Our results highlight the importance of organizational and individual factors that functioned as both facilitators and barriers to the integration of pediatric palliative care within a context of an accessible, well-run public healthcare system. Our findings highlight that allocating organizational resources dedicated to primary palliative care and managing the existing ones effectively is critical to providing pediatric palliative care for children. On the individual level, significant barriers to the integration of pediatric palliative care included pediatric oncologists’ attitudes toward palliative care, the impact of personality, and the emotional burdens of healthcare providers. Organizational facilitators included resource management, utilization of resources external to the organization, and a palliative care center within the organization. Individual facilitators included healthcare providers’ dedication and commitment, initiative, and sense of meaning.
What this study adds
Our study adds critical new information about the potential barriers and facilitators to integration of pediatric palliative care in both the local and international context. Locally, in the Israeli context, to the best of our knowledge, this is the first study done within the Israeli healthcare system to explore organizational and provider barriers and facilitators to the provision of primary pediatric palliative care. There is inconsistent integration of palliative care for children in Israel, which has been described as lacking a comprehensive approach and suffering from a shortage of human, material, and other resources.28,36,37 Our study adds to the existing knowledge by identifying the influential organizational and individual factors and the relationships between them. The buffering effect of the individual facilitators on the organizational factors provides a potential explanation for the gap between the high level of care and the low level of organizational resources. Added resources dedicated to primary and specialized palliative care teams may help overcome this gap.
Our results indicate that some providers compensate for organizational shortages by going beyond the call of duty, both by taking a holistic approach to care and being very available to their patients and families. This tendency increased when the child’s disease progressed and reflected the palliative care model curve of the illness trajectory. 38 There is no reimbursement for this kind of availability, such as representatives of the hospital team visiting a deceased child’s home to pay condolences. 36 This lack of financial structure and reimbursement, together with management barriers contributed to ad-hoc palliative care provision and made way for individual and personality differences to be more pronounced in influencing the inclination to provide palliative care.
The importance of both dedication and availability as facilitators for palliative care is supported by other research on this topic looking at the parents’ perspective, marking them as valued interpersonal behaviors.26,39 Backer et al. 40 stated that clinicians’ dedication can be effectively translated into clinical practice, allowing to better address specific palliative and end-of-life care needs. Our results suggest that these exist in the context of the Israeli healthcare system as well.
Internationally, our analysis reflects other studies in which insufficient resource allocation was found to be a fundamental barrier to primary palliative care.8,41,42 A recent Swiss study noted lack of financial resources, understaffing, and infrastructure as barriers to primary palliative care. 25 Insufficient resources also have a significant indirect influence, as it is strongly related to other barriers such as the healthcare provider’s time.25,41,42 We found that external resources such as volunteers were used to compensate for a lack of organizational resources. This phenomenon has also been found in Germany and Austria. 9
Interestingly, and perhaps of most relevance to an international audience, the healthcare context in which pediatric palliative care is being developed in Israel, resembles other healthcare systems in European countries, including Switzerland, Sweden, and Slovenia. In these nations, the availability of palliative care specialists vary and most do not have specialized pediatric palliative care programs or standards for training. 9 As noted in the introduction, Israel has a highly developed healthcare system and has stated that all citizens are eligible for palliative care services. 43 Despite the emphasis on public health, equitable access to healthcare, advanced medicine, and a focus on scientific research and breakthroughs, pediatric palliative care remains remarkably underdeveloped in Israel and around the globe. Indeed, most pediatric palliative care is provided by the primary oncology team with little specialized training in pediatric palliative care. Our findings suggest that one answer to this paradox may be that both barriers and facilitators are linked to factors beyond resources that have to do with emotional and personnel factors such as the emotional distress of providing pediatric palliative care, or negative or positive attitudes of the healthcare providers toward the provision of this care.
Likewise, other high income countries with well-resourced healthcare systems in Europe and North America including Canada, Sweden, and Switzerland, struggle with the implementation of pediatric palliative care. These challenges may have more to do with policy and allocation of resources than a lack of resources.9,25,44 As such, our findings on the barriers and facilitators to integration of pediatric palliative care are especially instructive and reflective of other high-income nations with advanced healthcare systems that are also struggling to set up these programs in their centers.
Strengths and limitations
This is the first study to address facilitators and barriers to integration of palliative care for children in Israel. Strengths of the study include variation in sampling in the participants’ professions and the multiple centers in which they work, allowing for different perspectives to be addressed and analyzed. Utilizing a qualitative approach to inquiry enabled integration of the richness of the interview data with methodological thoroughness. The research team’s adherence to the same principles of variation facilitated in-depth analysis.
One limitation of this study is the generalizability of findings, as it was conducted in a single country where specialized palliative care is mostly unavailable. However, our findings are relevant for the vast majority of countries that are in the process of palliative care development for children. Finally, while the focus of this study was to understand barriers and facilitators to the implementation of pediatric palliative care for children from the healthcare provider perspective, further research might include patients and their families to further understand what role they play in this context.
Implications
Our findings have practical implications for the improvement of organizational and healthcare provider factors that are critical to ensuring good pediatric palliative care. Organizations should consider allocating more resources such as treatment rooms, beds, and chairs for children and parents. 25 More positions for both primary and specialized palliative care personnel are urgently needed to reduce staff overload and turnover and to improve access to palliative care expertise.13,25 Designated palliative care team meetings can increase awareness of its benefits and synchronize teamwork.15,25,45 Other issues include reducing bureaucracy load and increasing administrative support.
Pediatric oncologists’ attitudes toward palliative care, combined with their inclination to make palliative care decisions based on their personality as opposed to field-related knowledge, must also be considered. Teaching palliative care to all healthcare providers will increase awareness, comfort level, and skills, and is therefore critically important.8,15,19 Finally, due to the emotional burden of providing palliative care to children, the risk of burnout is high.46–48 More research is needed to clarify whether increased provider dedication that compensates for lack of organizational recourses, might increase emotional burden. Policy makers aspiring to improve pediatric palliative care in oncology must take into account individual and organizational factors to ensure that they will not counteract one another but augment each other.
Footnotes
Appendix A: Semi-structured interview scheme
Author contributions
All authors contributed significantly to the paper and approved the final manuscript as submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Israel Science Foundation (ISF). Grant awarded to Leeat Granek (PI) (grant number 179/17).
Research ethics and patient consent
Approval to conduct the study was granted by the Ethics Committee of Ben-Gurion University (Date 28 July 2017/No. 1532-1) and The Chaim Sheba Medical Center (Date 3 October 2017/No. 4424-17). This study was performed in line with the principles of the Declaration of Helsinki. Participants received information about the study and provided written consent.
Data management and sharing
Not applicable. The data collected in this research are full interviews with healthcare providers. As such, data cannot be shared as it would violate participant confidentiality.