
Abstract
Background:
People from ethnic minority groups and deprived socioeconomic backgrounds have worse outcomes from COVID-19.
Aim:
To examine associations between ethnicity and deprivation with timing of palliative care referral for inpatients with COVID-19.
Design:
Service evaluation of consecutive patients with COVID-19 referred to palliative care. Sociodemographic (including age, sex, Index of Multiple Deprivation, ethnicity coded as White/non-White) and clinical variables were described. The primary outcome was timing of referral to palliative care. Associations between ethnicity and socioeconomic deprivation with the primary outcome were explored using multivariable regression.
Setting/participants:
Patients with COVID-19 referred to a hospital palliative care service across two London hospitals February–May 2020.
Results:
A total of 334 patients were included. 119 (36%) were from a non-White ethnic group; most commonly Black British (77, 23%) and Asian British (26, 8%). A longer time between admission and palliative care referral was associated with male gender (IRR 1.23, 95% CI 1.14–1.34) and lower levels of socioeconomic deprivation (IRR 1.61, 95% CI 1.36–1.90) but not ethnicity (IRR = 0.96, 95% CI 0.87–1.06).
Conclusions:
This large service evaluation showed no evidence that patients from ethnic minority or more deprived socioeconomic groups had longer time to palliative care referral. Ongoing data monitoring is essential for equitable service delivery.
What is already known about the topic?
Those from ethnic minority and deprived socioeconomic groups receive suboptimal palliative and end-of-life care. A small, single-centre study from the UK suggested that patients with COVID-19 from an ethnic minority background may have delayed referral to palliative care compared to those from White ethnic groups.
What this adds
In this service evaluation of a large ethnic minority and socioeconomically deprived population, those from ethnic minority and more deprived socioeconomic groups who were diagnosed with COVID-19, did not have later referral to hospital palliative care.
Implication for practice, theory, or policy
Equity in delivery of care for patients with COVID-19 is essential, especially for those groups disproportionately affected including ethnic minority groups and those from more deprived socioeconomic groups. Ongoing monitoring of meaningful data is needed to ensure equitable delivery of services.
Background
COVID-19 has caused more than three million deaths worldwide. 1 Two important risk factors for dying from COVID-19 are being from an ethnic minority or deprived socioeconomic group. 2 Early referral to palliative care is recommended. 3 A small, single-centre study from the UK suggested that patients from an ethnic minority group diagnosed with COVID-19 may have delayed referral to palliative care. 3 This is in contrast to a US study which found ethnicity was not a predictor of time to inpatient palliative care consult. 4 No studies have examined the association between socioeconomic position and palliative care access for patients diagnosed with COVID-19. Information on how ethnic group and socioeconomic position are associated with palliative care referral for these patients and families could inform service planning and equitable care.
We aimed to examine the association between ethnicity, deprivation and timing of palliative care referral.
Methods
Design
Service evaluation using electronic patient data from one NHS trust, including two large teaching hospitals in South East London. Hospital 1 has 1100 beds and serves an inner-city ethnically diverse and socioeconomically deprived population of 700,000. Hospital 2 has 512 beds and serves a mainly White British population of 581,000. Both have emergency departments, acute medical beds and intensive care units. London experienced very high levels of COVID-19: between 02/02/20 and 09/05/20, the trust had 2490 COVID-19 patients with 480 deaths across the two hospitals.
The hospital multi-professional palliative care team is well established, working as an advisory team across the both hospitals. The team provides a visiting service 9 am–5 pm, 5 days a week, with 24/7 consultant-led telephone support. There is a limited weekend and public holiday visiting service. During the first wave of the pandemic, referrals increased from a mean of 39–75 per week; deaths from 13 to 52 per week. Multiple actions were taken by the team to manage the surge in referrals including rapid development of a full seven-day service, proactive approach for identifying patients through frequent ward rounds on general medical wards and focused teachings to healthcare professionals throughout the two hospitals.
This project was registered as a service evaluation and quality improvement audit within our institution (PC048).
Data collected and coding
We included in-patients with confirmed COVID-19 referred to the palliative care service between 02/02/20 and 09/05/20. Data were extracted by a single clinician (RC, PE, KR, NL, LM). Socioeconomic variables included ethnicity, usual place of residence and the Index of Multiple Deprivation (IMD) as a proxy for socioeconomic position. 5 Clinical variables included reason for admission (COVID-19 or other), time from admission to palliative care referral, outcome (death or discharge), Charlson Comorbidity Index, 6 clinician-assessed illness phase (stable, unstable, deteriorating and dying) characterised by care needs and appropriateness of care plan and Australian-Modified Karnofsky Performance Status. 7
Analysis
Data were analysed using STATA 15. 8 Sociodemographic and clinical variables were described using percentages for categorical variables, and medians and ranges for continuous variables. Ethnicity was coded as White (White British and White Other) or non-White (Asian/Asian British, Black/Black British, mixed, other) based on that used by Public Health England. 2 A multivariable Poisson regression model was used to examine the association between ethnicity (dichotomous variable) and socioeconomic deprivation (in quintiles) with length of time between hospital admission and palliative care referral (in days), adjusted for sociodemographic, illness and service factors (age, sex, comorbidities, reason for hospital admission and hospital site).
Results
For sociodemographic and clinical variables, see Table 1. Between 02/02/20 and 09/05/20, 334 patients were referred. Most were male (n = 205, 61%), with median age of 80 (21–98). Most patients were of White ethnicity (n = 215, 64%); the most common ethnic minority groups were Black/Black British 77 (23%) and Asian/Asian British 26 (7.8%). 52% of all patients were in the two most deprived quintiles. The most common phase of illness at time of referral was terminal (n = 181, 54.2%). Two hundred and six (62%) patients admitted to the hospital had a ward based or end-of-life escalation plan in place. For 73% of patients the reason for admission was COVID-19. The remaining 27% were admitted for other reasons and subsequently found to be COVID-19 positive. Patients of non-White ethnicity were more likely to be younger, male, from a more deprived socioeconomic background and more likely to have been admitted to hospital due to COVID-19. Patients from White ethnic groups were more likely to be in the two least deprived quintiles, have been admitted from a care home, and to have had a hospital admission in the previous 14 days.
Demographic and clinical characteristics of hospital inpatients with COVID-19 referred to palliative care, by ethnic group.
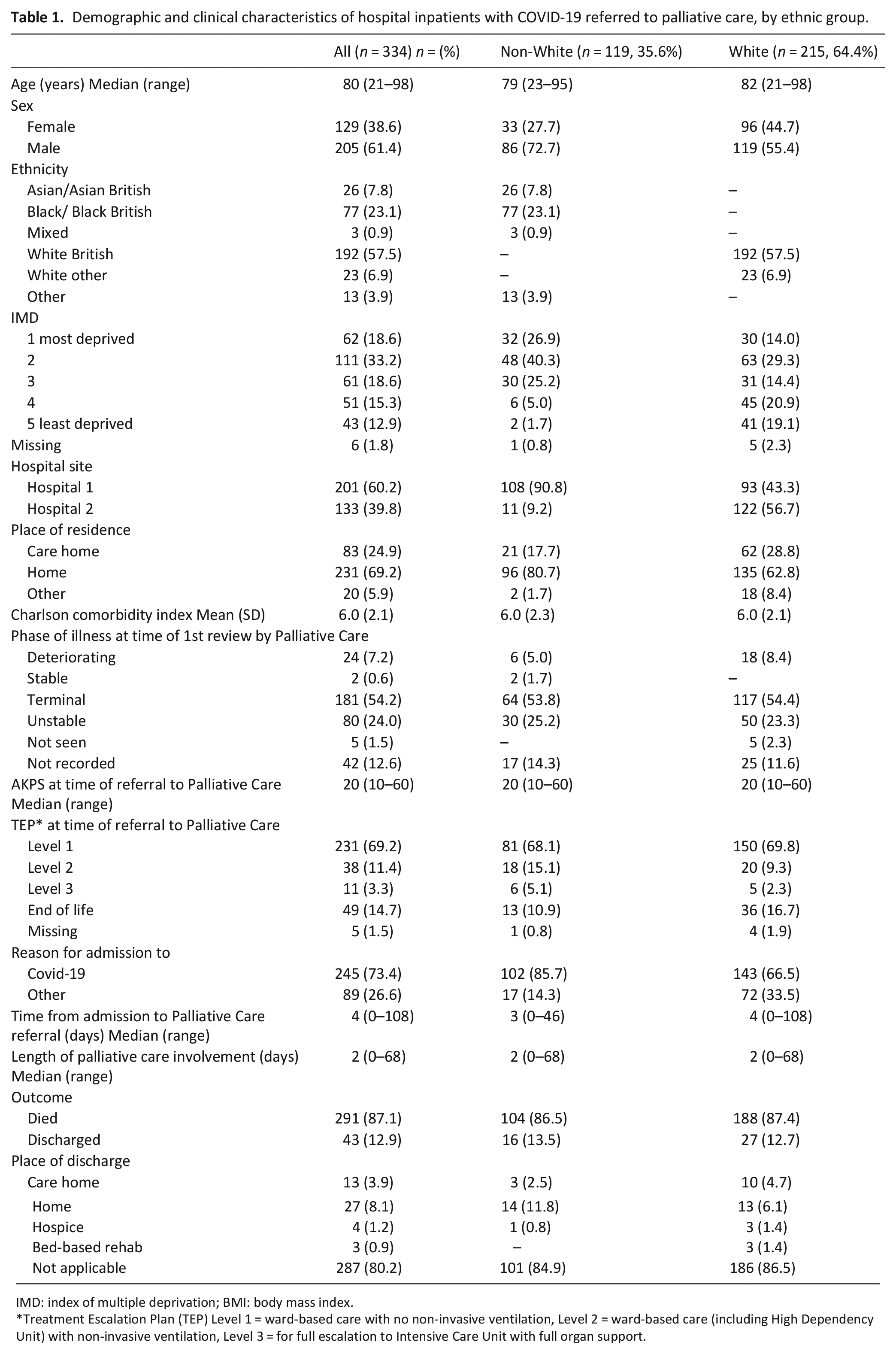
IMD: index of multiple deprivation; BMI: body mass index.
Treatment Escalation Plan (TEP) Level 1 = ward-based care with no non-invasive ventilation, Level 2 = ward-based care (including High Dependency Unit) with non-invasive ventilation, Level 3 = for full escalation to Intensive Care Unit with full organ support.
Ninety-nine (83%) patients in the non-White group versus 170 (79%) patients in the White group had a ward-based treatment escalation plan (non-invasive ventilation but not for escalation to Intensive Care Unit) at the time of referral to palliative care. In total, 291 (87.1%) patients died (non-White ethnicity: 104 (86%) vs White ethnic group: 188 (87%)).
Time from admission to palliative care referral
For association between ethnicity and socioeconomic deprivation and length of time between hospital admission and palliative care referral, see Table 2. Time from admission to palliative care referral was a median of 4 days (0–108). A longer time between admission and palliative care referral was positively associated with male gender (IRR 1.23, 95% CI 1.14–1.34) and lower levels of deprivation (IRR = 1.61, 95% CI 1.36–1.90 for quintile 5 compared with quintile 1). Non-White ethnicity was not associated with a difference in time to palliative care referral (IRR = 0.96, 95% CI 0.87–1.06). A non-COVID-19 admission was associated with a longer time to palliative care referral (IRR = 4.00, 95% CI 3.69–4.33).
Poisson regression model examining the association between ethnicity and socioeconomic deprivation with length of time between hospital admission and palliative care referral adjusted for service, illness and sociodemographic factors.
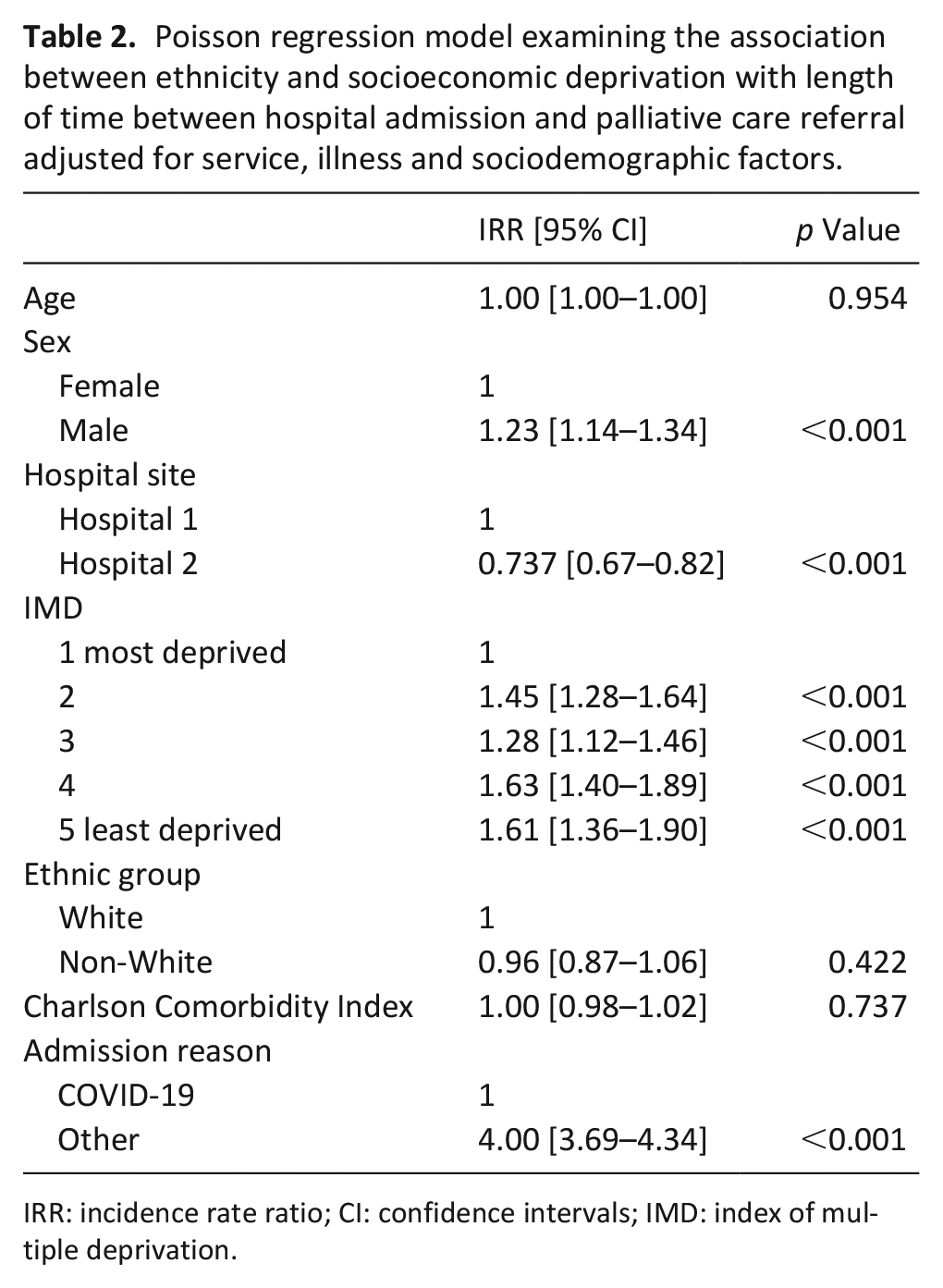
IRR: incidence rate ratio; CI: confidence intervals; IMD: index of multiple deprivation.
Discussion
In this large service evaluation, we found that a longer time between hospital admission and palliative care referral for people with COVID-19 was positively associated with male gender and lower levels of deprivation but was not associated with being from an ethnic minority group.
Main findings
Inequalities in palliative care delivery for those from ethnic minority groups are well described. 9 In this study, we used time from admission to palliative care referral as a quality indicator to examine differences between groups, based on a previous study. 3 In contrast to the previous study, we did not find that patients from ethnic minority groups had a longer time from admission to palliative care referral. This may be due to differences in patient population, hospital structure and palliative care service model. Alternative quality indicators, in particular patient-reported outcomes, should be investigated.
We found that those from less deprived socioeconomic groups were more likely to have a longer time between hospital admission and palliative care referral. This is in contrast to what has been reported previously reported. 10 It may be that patients from more deprived socio-economic groups have more complex needs (e.g. high levels of co-morbidity) and are referred earlier to palliative care. However, in our model we found no association between comorbidities and time to referral. It may also be that patients from more deprived socioeconomic groups present later, with more advanced illness, prompting earlier referral to palliative care following admission. The palliative care team’s proactive approach for identifying patients through frequent ward rounds on general medical wards and focused teachings to healthcare professionals may have influenced referral practices. Despite this proactive approach, almost half of patients were already in the Terminal phase at the point of review by the team. Being admitted with conditions other than COVID-19 was associated with a longer time to palliative care referral. It is likely that these people were infected with COVID-19 as hospital in-patients.
Strengths and limitations
To our knowledge this is the largest palliative care service evaluation of an ethnic minority population to date, and the first to examine association between socioeconomic position and outcomes. Data were from one NHS Trust, which may limit generalisability. However, we provide methods for use in other settings to examine potential inequity of delivery of services. We grouped our sample as ‘White’ and ‘non-White’. We acknowledge that these groups are not homogenous entities. We used deprivation scores based on postcode rather than individual-level indicators of deprivation, for example, level of education or occupation. We did not examine the intersectional effects of ethnicity and socioeconomic status. We used time from admission to palliative care referral as a proxy for quality, there may be other appropriate measures.
Conclusion
Disparities in care among ethnic minority populations and those from deprived socio-economic groups are widely prevalent in the UK health-care system. Understanding the effects of ethnicity and socioeconomic status on palliative care outcomes for patients with COVID-19 is essential, but relatively unexplored. In this large dual-centre service evaluation of people with COVID-19, there was no evidence that patients from ethnic minority or more deprived socioeconomic groups had longer time to palliative care referral. Ongoing data collection and monitoring, including data on ethnicity, socioeconomic position and patient-reported outcomes, are essential to identify discrepancies and support equitable service delivery during the pandemic and beyond.
Footnotes
Authors’ contributions
SB, PE, RC, NL, EY and KES made a substantial contribution to the concept of the work; RC, PE, KR, NL and LM reviewed medical notes and inputted data; EY and KES analysed the data; SB, PE, RC, NL, EY and KES interpreted the data; SB drafted the manuscript and all authors revised it critically for important intellectual content; all authors approved the final version for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KES is funded by an NIHR Clinician Scientist Fellowship (CS-2015-15-005), and is the Laing Galazka Chair in palliative care at King’s College London, funded by an endowment from Cicely Saunders International and the Kirby Laing Foundation.