
Abstract
Background:
Providing unawareness and pain relief are core elements of palliative sedation. In addition to clinical scales, nociception and electroencephalogram-based depth of sedation monitoring are used to assess the level of consciousness and analgesia during sedation in intensive care units and during procedures.
Aim:
To determine whether reported devices impact the outcomes of palliative sedation.
Design:
Systematic review and narrative synthesis of research published between January 2000 and December 2020.
Data sources:
Embase, Google Scholar, PubMed, CENTRAL, and the Cochrane Library. All reports describing the use of any monitoring device to assess the level of consciousness or analgesia during palliative sedation were screened for inclusion. Data concerning safety and efficacy were extracted. Patient comfort was the primary outcome of interest. Articles reporting sedation but that did not meet guidelines of the European Association for Palliative Care were excluded.
Results:
Six reports of five studies were identified. Four of these were case series and two were case reports. Together, these six reports involved a total of 67 sedated adults. Methodological quality was assessed fair to good. Medication regimens were adjusted to bispectral index monitoring values in two studies, which found poor correlation between monitoring values and observational scores. In another study, high nociception index values, representing absence of pain, were used to detect opioid overdosing. Relatives and caregivers found the procedures feasible and acceptable.
Keywords
Insufficient and ineffective sedation is not uncommon.
In daily practice, the assessment of a patient’s unawareness and comfort under palliative sedation relies on simple clinical scales, the use of which has limitations.
Nociceptive indexes and processed electroencephalogram-based depth of sedation monitoring with bispectral analysis could potentially improve the assessment of analgesia and level of unconsciousness during sedation.
There is no evidence that the use of these monitoring tools provides clinically relevant improvements for patients during sedation.
Studies suggest poor correlation between bispectral analysis values and observational clinical scores for deeply sedated patients.
Nociception monitoring could help detect opioid overdosing and insufficient analgesia.
Next of kin and caregivers reported finding the monitoring useful and without burden.
Further studies are needed to measure the impact of these monitoring tools for use in the context of palliative care.
Future studies should include a control group and outcomes that are relevant to patients under palliative sedation and should consider including patients and next of kin in the research team.
Background
Palliative sedation aims to provide relief to patients with intractable suffering that cannot be relieved in an awake state, when all other existing methods have failed. 1 Palliative sedation includes a continuum of sedation states: minimal, mild, moderate, or deep. It is very difficult to predict how an individual patient will respond to a given sedation regime, in terms of depth of sedation, as well as hemodynamic and respiratory stability. 2
Finding the balance between the risks and the intended relief of burdensome symptoms is a major challenge. The level of sedation needs to be carefully adjusted, using a step-by-step approach, to identify the lowest dose providing adequate relief of suffering.1,3 Since palliative sedation therapy aims to induce a state of decreased or absent awareness (which may be intermittent or continuous, and may vary in depth), consciousness assessment is crucial during the process. 4
Palliative sedation is applied in many circumstances in which intractable pain is not the primary reason for sedation. However, pain is present in up to 36% of patients with the various indications for palliative sedation,5–8 and patients often experience moderate to severe pain at the end of life. 9 Since these patients receive opioids in combination with palliative sedation agents, an additional challenge in the application of palliative sedation is to monitor analgesia. 8
Extensive literature provides guides and recommendations for palliative sedation and assessment. Yet the incidences of insufficient sedation and delayed or inadequate relief do not appear to be decreasing. A study published in 2005 revealed that palliative sedation failed to relieve symptoms in 17% of individuals and that nearly half of these patients experienced unwanted awakening after falling into a deeply sedated state. 10 A recent Cochrane review noted insufficient evidence regarding the efficacy of palliative sedation in terms of individual quality of life and symptom control, particularly with regard to delirium and dyspnea. 11 Furthermore, whereas Wright underscored the relevance of consciousness in experiences of death and dying 12 , a recent Dutch study reported that nurses rated the incidence of insufficient sedation in up to 40% of cases. 13
Moreover, sedation is not always successful, even when patients appear to be unconscious. 14 Despite the various criteria used to define a state of “adequate sedation,” there is a consensus that, under optimal sedation, patients should remain “unaware.” However, patients sedated in this way may still experience pain, anxiety, and helplessness—symptoms which may remain unnoticed by caregivers—in the absence of reliable objective tools for assessing sedation. 15 Notably, there is a lack of a reliable method to objectively assess the level of consciousness.16,17 Caregivers most frequently base their assessment of depth of sedation and patient comfort on clinical observational scales such as the Critical Care Pain Observational Tool (for pain), the Ramsay score, and the Richmond Agitation-Sedation Scale (RASS).18–20 The RASS aims to determine the level of sedation intermittently by evaluating the patient’s response to deliberate verbal and physical stimulation according to a range of expected responses. In addition, the upper range of the scale evaluates levels of agitation. These scores detect only unresponsiveness, which is assessed by the patient’s lack of interaction with the external environment. Unresponsiveness is a consistent depression or functional disconnection of lateral frontoparietal networks under anesthetics. 21 A challenging aspect is that behavioral unresponsiveness does not mean a patient is unconscious, thus the ability to measure consciousness in unresponsive patients requires methods that do not require report-based responses as well as observational methods for measuring brain activity. 22
Non-stimulating and non-invasive monitoring (including processed, electroencephalogram-based depth of sedation devices and nociception monitoring) could allow a more objective and frequent assessment of the levels of consciousness and analgesia during palliative sedation compared to clinical scales.23,24
Depth of sedation monitoring tools such as the Bispectral Index (BIS), Entropy, and NeuroSense, have been used to monitor anesthesia and sedation, with the aims of decreasing the incidence of intraoperative awareness and reducing both anesthetic consumption and recovery time.25–27 For this method, a disposable wet gel electrode is placed on the patient’s forehead to record electric signals from the cortex and transfer them to a digital converter. Subsequently, BIS values are calculated with an empirically derived algorithm to quantify changes in the electrophysiologic state of the brain being monitored. These values, which decrease as the depth of anesthesia increases, are expected to reflect the patient’s hypnotic level (BIS value of 100 = awake patient).
Nociception monitoring provides information about the physiological encoding and processing of nociceptive stimuli by analyzing the high-frequency component of heart rate variation in relation to respiratory frequency. During anesthesia, nociception index values reflect whether analgesia is adequate and whether analgesia allows maintenance of the nociception-antinociception balance, in which parasympathetic activity predominates over sympathetic activity. 28 This monitoring offers the promise of an objective and continuous assessment of nociception and depth of sedation.
Although there are studies reporting procedure-related outcomes and monitor-guided sedation outcomes in intensive care units, these findings may not be relevant to palliative care. 29
The purpose of this review was to systematically identify and examine evidence for the use of depth-of-sedation and nociception monitoring on palliative sedation outcomes and their potential benefit for patients. The review aimed to provide recommendations for palliative sedation practice and future research in this area.
Review questions
What impact do awareness and nociception monitoring have on palliative sedation outcomes?
What are the benefits and limits of monitoring for patients, families, and caregivers?
Methods
The authors conducted a systematic review and narrative synthesis of the evidence. This research design was chosen to systematically search for, appraise, and synthetize research evidence pertaining to palliative sedation monitoring. The evidence included data from a limited number of very small studies not suitable for a meta-analysis.
The narrative synthesis of this review is reported according to SWIM (Synthesis Without Meta-analysis) reporting items check-list, an extension to PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines (Supplemental Appendix 1). 30
Qualification of researchers
The research team included both physicians specialized in palliative care medicine (NDR, SP) and a physician with training and experience in research methodology and systematic reviews (NE).
Search strategy
We searched reports available from the Cochrane Central Register of Controlled Trials (CENTRAL; 2020, Issue 7), Google Scholar (2000−2020), MEDLINE (Ovid) (2000−2020), and EMBASE (Ovid) (2000−2020). We also searched one clinical trial registry (ClinicalTRials.gov) to identify ongoing trials.
We applied no language restrictions and used search terms related to palliative care, sedation, awareness, and nociception monitoring. An initial broad search was performed with each of the four databases to identify a list of relevant search terms. The four databases were then systematically searched using a combination of free-text terms or subjects, including a palliative (#1), a sedation (#2), and a monitoring of awareness (#3) or analgesia term (#4). We used the search strategy described to obtain titles and abstracts of studies that may be relevant to this review. The last search was performed on 05th of March 2021. Table 1 provides an overview of the specific search terms used and filters applied, according to database searched. See Supplemental Appendix 2 for search strategy via MEDLINE.
Summary of search strategies and number of results.
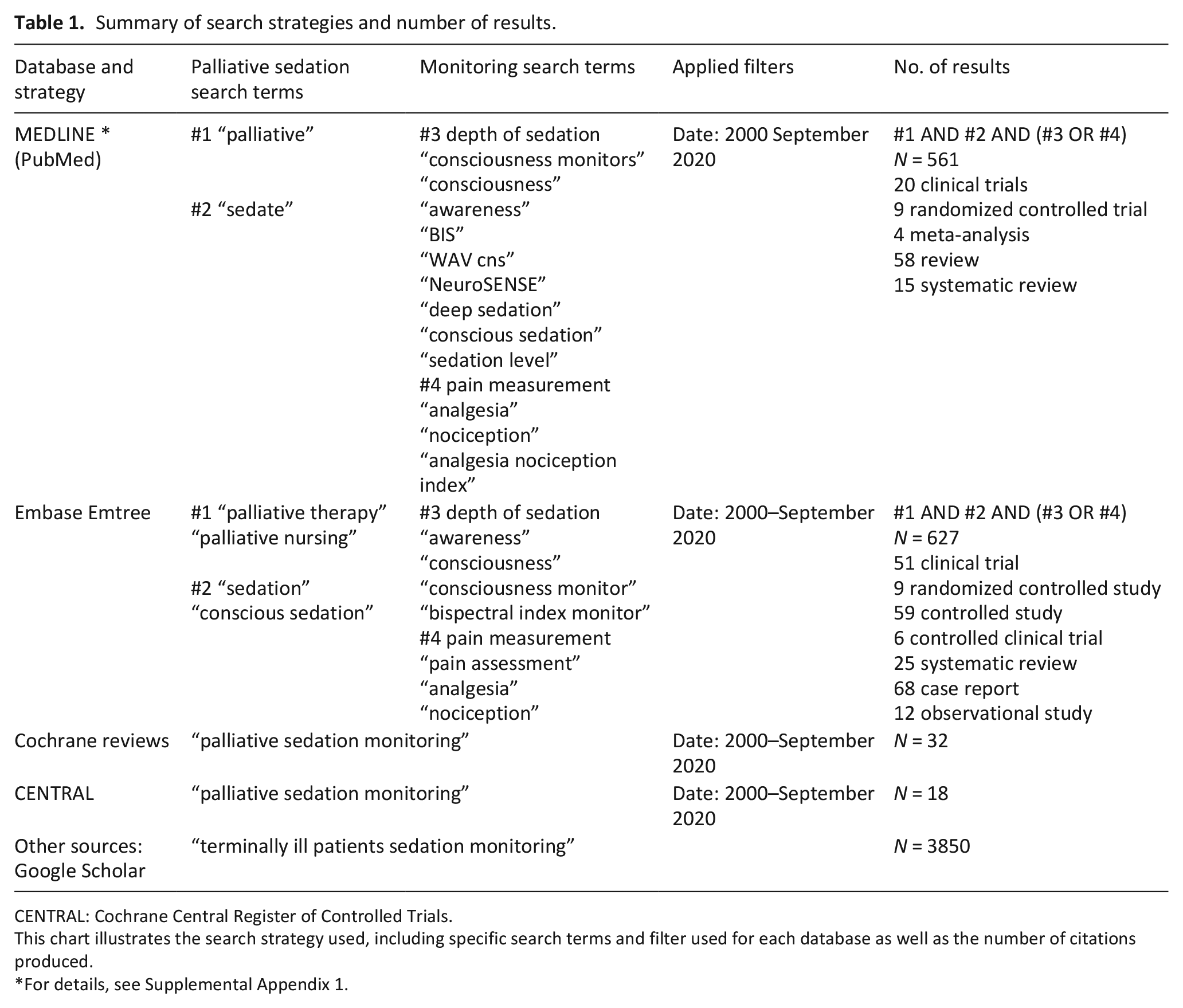
CENTRAL: Cochrane Central Register of Controlled Trials.
This chart illustrates the search strategy used, including specific search terms and filter used for each database as well as the number of citations produced.
For details, see Supplemental Appendix 1.
Eligibility and study selection
We aimed to include only Randomized Controlled Trials (RCTs) or quasi-RCTs, and non-randomized experimental designs. Insufficient reports were identified, and it was decided to extend the search to observational studies which included control groups as well as case series and case reports.
All included studies reported at least one quantitative or qualitative outcome related to either pain or the quality of sedation.
Three authors (NDR, GM, and SP) performed the literature search and screened titles and abstracts of identified studies that were potentially relevant to this review. Appropriateness for inclusion of the studies was assessed by author independently. In case of disagreement, a consensus was reached through discussion.
Table 2 details inclusion and exclusion criteria.
Eligibility criteria.
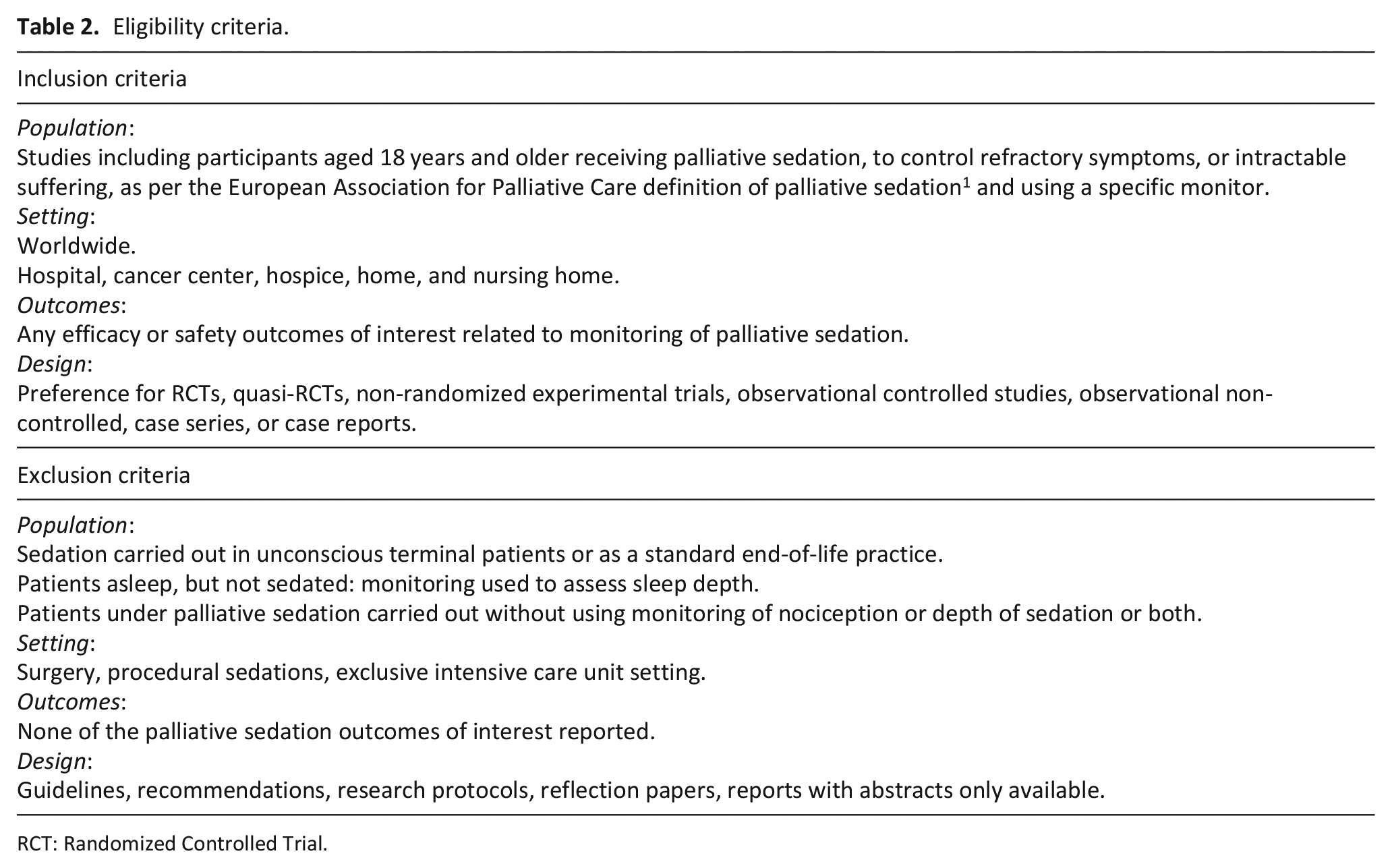
RCT: Randomized Controlled Trial.
Data extraction and data items
Two authors (NDR, GM) independently carried out data extraction using standard data extraction forms. A third author (SP) acted as an arbiter in the event of disagreement.
The following study data were extracted: name of the first author, year of publication, country in which the study was performed, study design, population type, sample size, setting, aim of the study, description of the intervention/control administrated, sedatives used, type of monitoring tool and duration of use, monitoring values targeted and reported, and sedation or pain outcomes.
Outcomes
Primary outcome:
- Degree of patient comfort under sedation, measured by any scale (e.g. Patient’s Comfort Score)
Secondary outcomes:
- Depth of sedation (reflecting level of unconsciousness, any scale)
- Time to reach the desired level of sedation
- Successfulness of symptoms relief
- Successfulness of sedation reversibility (when arousability was desired)
- Presence or absence of instability of vital signs (e.g. tachycardia/bradycardia, hypotension, and low oxygen saturation)
- Presence or absence of agitation or RASS score greater than 0 31 or any of the following behaviors: purposeless movements, grimacing, groaning, shouting, and touching an area 32
- Acceptance of monitoring devices by family and health care professionals.13,32
Quality grading
Existing quality assessment tools were used to grade the quality of the included studies, according to the study design: using the Cochrane Bias assessment tool for RCTs or, for observational studies, the National Institute of Health (NIH)—Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies for observational studies. 33 The quality assessment was independently undertaken by two authors (NDR, NE).
Data analysis and synthesis
A quantitative analysis of the impact of the sedation monitoring tools on major outcomes using meta-analyses methods was planned to be performed if more than three trials or 100 patients reported on the same outcome across different studies.
As too few trials were identified, we performed a narrative synthesis of the extracted data. Studies were tabulated and grouped by features, setting and population, and main outcomes.
The evidence was synthetized to provide a meaningful narrative, relevant to the research question.
Results
Figure 1 details the selection process. We identified 5091 citations. Two authors (NDR, GM) independently screened the titles and abstracts and excluded studies that did not meet our inclusion criteria. We initially kept all studies and reviews that may have included relevant data or references and searched their reference lists, as well as the reference lists of all included papers for additional relevant studies.
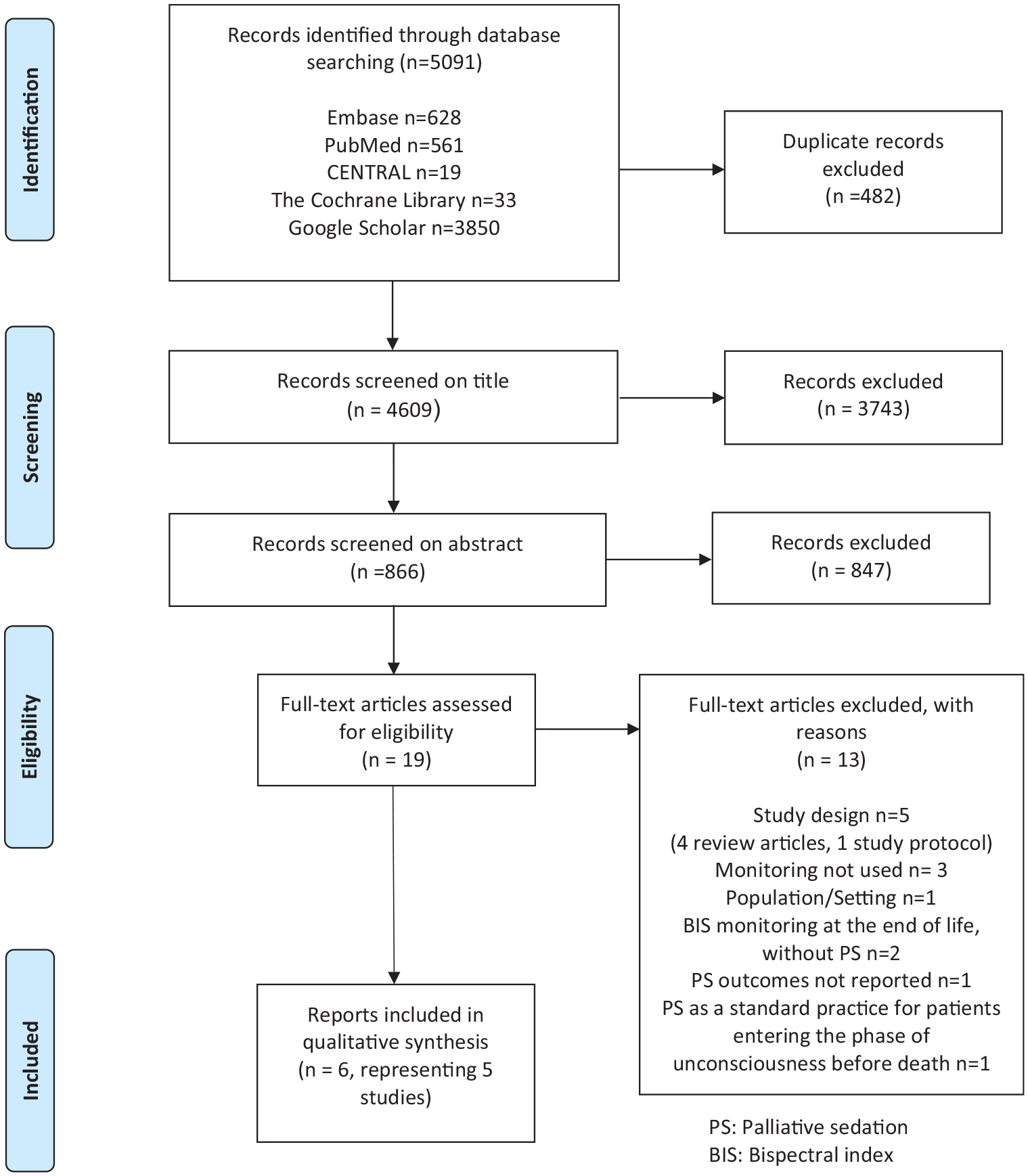
Flow Chart selection process (based on PRISMA Flow Diagram, adapted from: Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6(7): e1000097).
After title and abstract screening, we reviewed 19 full-text articles; 13 were excluded (as reported in Supplemental Appendix 3), and six reports representing five studies were included. We found no unpublished studies from the clinical trials register searched.
Study characteristics
We found no RCT or observational studies with control groups. Six reports published between 2016 and 2020 satisfied our selection criteria. Four of these were observational, prospective, consecutive multi-case series, and two were case reports of individual cases. The studies are summarized in Table 3.
Description of included reports.
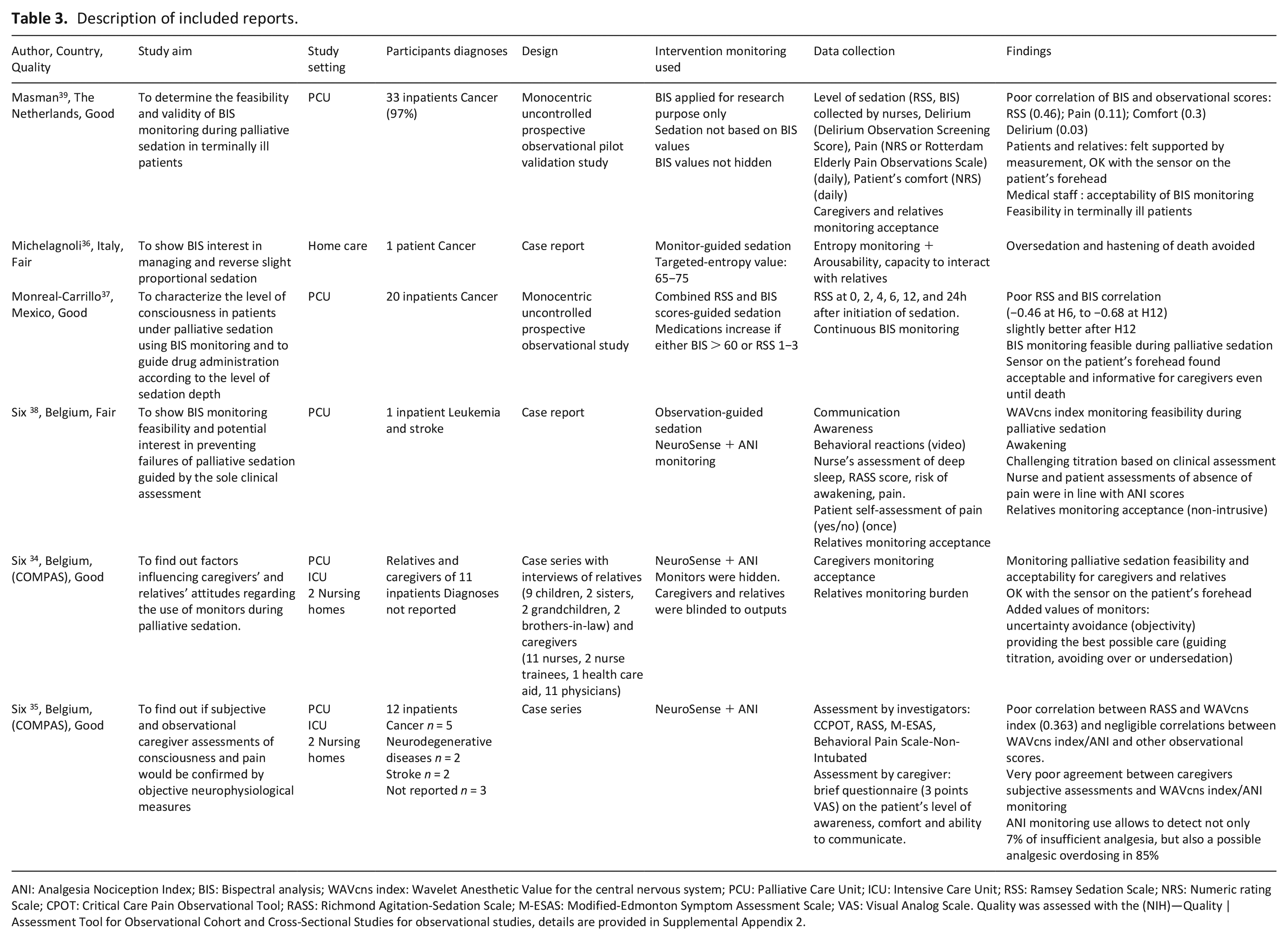
ANI: Analgesia Nociception Index; BIS: Bispectral analysis; WAVcns index: Wavelet Anesthetic Value for the central nervous system; PCU: Palliative Care Unit; ICU: Intensive Care Unit; RSS: Ramsey Sedation Scale; NRS: Numeric rating Scale; CPOT: Critical Care Pain Observational Tool; RASS: Richmond Agitation-Sedation Scale; M-ESAS: Modified-Edmonton Symptom Assessment Scale; VAS: Visual Analog Scale. Quality was assessed with the (NIH)—Quality |Assessment Tool for Observational Cohort and Cross-Sectional Studies for observational studies, details are provided in Supplemental Appendix 2.
Five reports originated from Europe (three reports from Belgium, and one each from The Netherlands and Italy) and one originated from Mexico. The three reports originating from Belgium were authored by the same research team (Six et al.) and two of these reported on the same 12 patients, their relatives and healthcare providers (representing two parts of the “Compas study” 24 ). Studies were mainly conducted in a single setting, except for the two reports of Six et al., which involved two nursing homes.34,35 Studies were mainly carried out in palliative care wards. One was conducted at the patient’s home. 36 One study included a patient from a cancer center. 37
The six reports included data from 92 patients—67 of whom received palliative sedation—and information from 11 relatives and healthcare givers. The study sizes ranged from 1 to 33 patients, who received palliative sedation 38 Characteristics of the participants were inconsistently reported. Among the studies in which some patient characteristics were reported, most patients had a diagnosis of cancer. Four studies enrolled elderly patients: one report described a woman in her 80s 39 and, in the other reports the median age of the patients ranged from 75 to 76 years.34,35,38 In contrast, the two remaining studies described much younger patients: one report described young mother 36 , and another reported on patients with a median age of 41 years. 37
Symptoms that constituted the indications for palliative sedation were clearly reported as refractory in one study in which delirium (75%), pain (65%), and dyspnea (30%) were the most frequent indications reported. 37 All studies reported on continuous palliative sedation, with one exception of intended proportional intermittent sedation. 36 Midazolam was administrated as the sole sedative in one study, 38 and in addition to haloperidol36,39 or propofol. 37 Six et al. did not report the sedatives used.34,35
According to the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies, studies were graded fair to good (for details see Supplemental Appendix 4). 33
Interventions and studies purposes
Interventions are described in Tables 3 and 4.
Sedation indications, characteristics and outcomes according to the monitoring used.
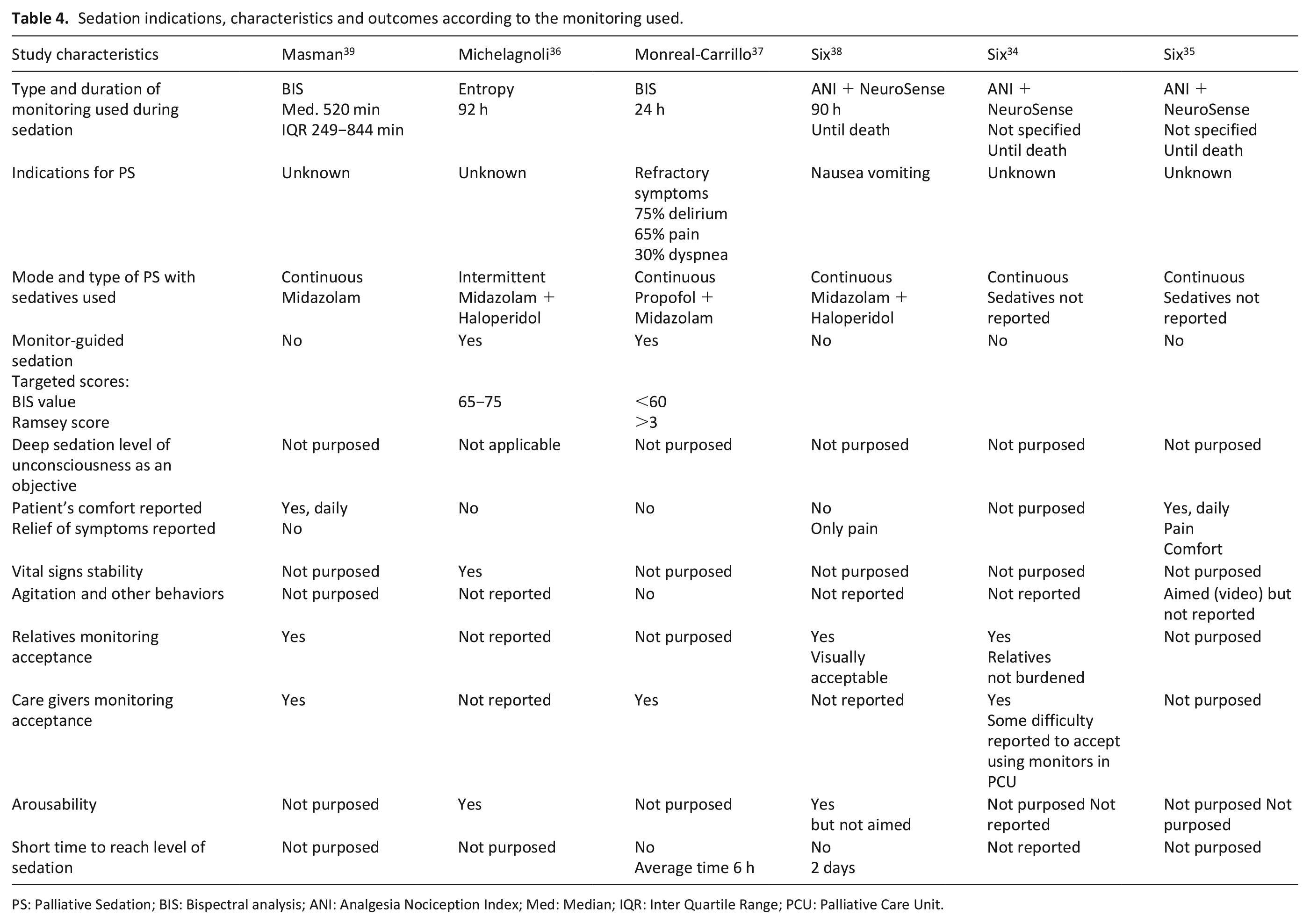
PS: Palliative Sedation; BIS: Bispectral analysis; ANI: Analgesia Nociception Index; Med: Median; IQR: Inter Quartile Range; PCU: Palliative Care Unit.
All the selected studies monitored the depth of sedation. The monitoring duration ranged from 4 to 92 h. Three different monitors were used: BIS, Entropy, and NeuroSense. These monitors were used for the following purposes: to validate BIS monitoring during palliative sedation (one study 38 ), to show its feasibility and acceptability in palliative care setting (two studies34,38), to show its appropriateness in managing slight proportional sedation when reversibility was desired (one study 36 ), to guide drug administration based on the level of sedation depth (two studies36,37), and to show its potential use in detecting under or overdosages of sedatives and/or opioids during palliative sedation guided by the sole clinical assessment (two studies35,39). In the three selected reports by the same author, nociception monitoring (ANI) was used in addition to depth of sedation monitoring, and these were continued until patient death.34,35,39 BIS values were used to adjust the rate of medication administration in two studies.36,37
Synthesis of outcomes
The ability to conduct meta-analyses was precluded by the scarcity and the design of the studies lacking control groups; we therefore report outcomes narratively.
Table 4 provides details regarding sedation safety and efficacy outcomes, according to the monitoring method used.
Efficacy outcomes
Primary outcome
Patient’s comfort
Patient comfort was evaluated and reported using a numeric rating scale in only one study, in which palliative sedation was not monitor-guided. 38 In this study, one-third of the patients were reported to be uncomfortable. None of the other studies reported patient comfort.
Secondary outcomes
Unawareness assessment/depth of sedation
Two studies (Monreal-Carrillo et al. and Masman et al.) compared unawareness assessments via Ramsey Sedation Scale or BIS monitoring and showed a large variability in BIS values for patients that were clinically deeply sedated.37,39
In the study by Monreal-Carrillo et al., BIS values ranged from 35 to 85, even when Ramsey scores were between 4 and 6. The correlation between BIS values and Ramsey scores increased during the first 12 h of sedation. Nevertheless, most of the patients needed dose escalation during the first 24 h. 37
Six et al. found a poor correlation between Wavelet Anesthetic Value for the central nervous system index monitoring and RASS. 35
Time to reach the required level of sedation
Two studies reported the time taken to reach the required level of sedation. Non-monitor-guided palliative sedation induction was challenging and lasted 2 days in one study. 39 In a monitor-guided study, however, the average duration of titration was 6 h and one-third of the patients were still not sedated after 24 h. 37
Achievement of symptom relief
Two studies reported information about symptom control. In the first study, the absence of pain was assessed at only one time point using a verbal scale 39 and, in the second study, a negligible agreement between caregivers’ subjective assessments and objective neurophysiological measures of pain was highlighted. 35 Subjective caregiver assessment was found to have a positive predictive value for pain of 0% compared with ANI monitoring. 35
Arousability
A case study reporting monitor-guided proportional sedation aimed at reversibility of sedation and reported their efforts were successful. This study was the only study to highlight an interest in relying on depth of sedation while monitoring at home to be able to keep the patient arousable enough to communicate with family members. 36
Safety outcomes
Vital signs
Only one study reporting vital sign stability noted success. The study reported monitor-guided proportional sedation. 36
Agitation and unwanted behavior
Agitation and unwanted behavior were not described in the monitor-guided sedation reports.36,37
Although, video and audio recording were recorded to detect restlessness and movements in one study, the behaviors were not reported. 35
Monitoring acceptability and limits among family and caregivers
In five studies, caregivers and family members were asked to express their opinion on the monitoring method.34,36–39 Three studies reported narratively that respondents deemed the monitoring and the sensor on the patient’s forehead were “feasible and acceptable.”37–39 The familial relationship of these respondents to the patients was not specified in these studies.
Six et al. conducted semi-structured interviews with caregivers (n = 20; 8 physicians, 9 nurses, 2 nurse trainees, and 1 healthcare aide) and family members (n = 15; 9 children; 2 grandchildren; 2 sisters; and 2 brothers-in-law) after the death of patients. 34 Participants were asked to share their thoughts about the acceptability and the added value of the monitors.
Family members reported acceptability, utility, and an opportunity to improve care, but no burden. It was noted that a respondent was surprised to see a sensor on the patient’s forehead, as she had not previously been informed of the procedure. Some relatives felt that the use of monitoring was helpful to carry out the wish of their loved one (who had expressed the fear of experiencing a painful death), to avoid uncertainty, as well as to ease their own concerns. 34
Moreover, caregivers expressed more confidence with objective continuous measures and viewed these monitoring methods as a substantial improvement, even in cases where the administration of sedatives or opioids was not monitor-guided. Another potential interest in the use of these monitors was that very low brain activity observed before death, could provide some information for predicting when end of life would occur. 34
However, compared to caregivers who expressed no difficulty and even some interest in using continuous sedation monitoring when working in, for example, intensive care units, or in a challenging setting such as home care, some caregivers expressed that they would have difficulty in accepting it in palliative care units. 34 They also expressed concerns that monitoring tools and sensors could be a source of distress for a patient’s relatives. Nevertheless, these caregivers reported a sense of reassurance as a result of using continuous sedation monitoring. 34
BIS monitoring allowed caregivers to avoid oversedation in a home care case report. 36 In Six et al. studies, concerns about avoiding oversedation were not expressed by caregivers and relatives.34,35
Discussion
Main findings
Most of the methods used to assess awareness and comfort under palliative sedation are based on subjective scales and judgments. Anesthesia and sedation are now guided in various contexts by monitoring the reduction of consciousness and nociception. We performed a systematic review to explore the utility of these tools during palliative sedation.
Although our systematic search identified an emerging body of literature related to this topic, it returned only six reports of five uncontrolled studies. These studies involved fewer than 100 patients that received palliative sedation. Moreover, most of the studies were conducted in two European countries: the Netherlands and Belgium. The reports primarily reflected the experiences of caregivers and families—experiences that were relatively positive—and readiness for palliative sedation monitoring.
Monitoring of the depth of sedation was used in the five studies. In contrast, nociception monitoring was only reported in the Six et al. reports, which include one case report and a sample of 12 consecutive patients, thereby preventing any conclusions from being drawn.
This review suggests that, based on two reports only, non-invasive depth of sedation monitoring correlates poorly with commonly used tools, such as the RASS. Previously, Barbato et al. contributed greatly to determining this correlation in relation to unconscious palliative care patients.40–42
More recently, Barbato et al. demonstrated that, with dying unresponsive patients not receiving palliative sedation, comfort, RASS, and BIS scores significantly decrease after administration of breakthrough medication. 43 Beng et al. confirmed that there was an association between BIS values and suffering. 44 Beng et al. conducted a randomized controlled study to demonstrate that a 20-min session of mindful breathing could help alleviate suffering during palliative care. They found a statistically significant effect for the intervention on both BIS values, and suffering score. 44
Nevertheless, two studies showed high variability among BIS values in deeply sedated patients. These results are in agreement with those of Barbato et al., who found a large discrepancy between the lowest RASS scores (−5 = unresponsive), Patient’s Comfort Score (0 = complete comfort) and BIS values in unresponsive patients. 43 Potential monitor-guided sedation benefits were reported in a single study, which included only 20 patients, and one case report, using BIS and entropy methods, respectively. These studies formally reported patient’ comfort under palliative sedation, or the absence of pain. However, these reports were based on very few assessments. 37
We failed to find clear evidence that monitoring could help shorten the time to reach the required level of sedation, which was defined as shorter than 2 or 4 h.13,31,45 Indeed, a single study using monitor-guided sedation reported an average titration duration of 6 h, together with one third of the patients still not sedated after 24 h. 37
However, the findings concerning feasibility, acceptance by family members and possible sedation reversibility—together with vital sign stability and the absence of reported unwanted behavior—suggest an opportunity for improving palliative sedation outcomes.
Strengths and limitations
Our strategy was to ensure the inclusion of all relevant publications by two independent reviewers. This review employed a comprehensive search strategy, that was performed with only five electronic databases of potentially many more. The searches were not limited by language or geographical limitations, and the searched period spanned the last 20 years. Grey literature was searched using Google Scholar.
It is possible that we missed some studies, despite screening more than 5000 citations as well as references cited in reviews. We anticipated finding very few studies that fit our criteria. Thus, we chose to analyze all the studies identified, regardless of their quality, since they could contain important information relevant for designing future studies. There are several reasons why these studies are methodologically weak.
Firstly, it must be acknowledged that the complex biological basis, and therefore the assessment of consciousness, is one of the greatest challenges of neuroscience. 46 The current observational tools, based on patient’ responsiveness, are unreliable. Instead, depth-of-anesthesia monitors have been developed based on the assumption (1) that responsiveness and connected consciousness are not dissociable and (2) that a key construct—“levels of consciousness”—exists. However, it is far from clear what precisely a measurable “level of consciousness” is. The multidimensional analysis of global states of consciousness is now better explored with functional neuroimaging and electroencephalography, which are currently mostly limited to the research with comatose patients.47,48
Secondly, while ethical challenges were scarcely mentioned by the authors of the selected studies, there are some obvious ethical and practical limits to carrying out this kind of research in the end-of-life context. Patient’ recruitment is limited by the difficulty to obtain, either in advance or in emergency, patient’ (or proxy’) consent for palliative sedation research. 49 Importantly, the main ethical conflict lies in balancing expectations of a peaceful death, the patient’ privacy and dignity, fears of a painful death by families, and caregivers’ opportunity to enhance quality, security, and confidence in palliative sedation.
Other important concerns include the following: the risk of undermining the caregivers’ sense of being fiduciaries for patients, the limited interest of real-time monitoring when patients and families need peace and caregivers are unwilling to enter the patient’s room to repeatedly adapt sedation, cost-effectiveness, future requests by families to use those devices for palliative sedation and prognosis.
We chose to include studies in which the palliative sedation described met the European Association for Palliative Care’s definition. Thus, we excluded studies where sedation was carried out on patients that were dying and unresponsive. 50 Some studies were excluded because sedation was deemed a standard practice for patients entering the phase of unconsciousness before death, in which refractory symptoms were absent. 42 Moreover, most of the studies failed to report clear indications for sedation.
It should be noted that the biological, psychosocial, and physical data of most participants were not reported. Studies also lacked information about the drugs administered before sedation, which should raise concerns about the risks of delayed or failed sedation. 51
Beyond this, the studies were mainly conducted in Europe. The extent to which these monitoring methods are available in other countries should be considered. The applicability of our results may vary, as palliative sedation concepts, aims, indications, and expected outcomes vary depending on the country.
What this study adds?
Monitoring technologies developed for anesthesia 52 offer possibilities for future palliative sedation research. However, no current technology appears to offer a sufficiently broad applicability, and no firm evidence was found for clinically relevant influence of such devices on patient outcomes.
We found recent evidence that monitoring the depth of sedation is feasible in terminally ill patients under midazolam in various settings of care.35,36
Nevertheless, the range of normal BIS values for comfortable and adequately sedated patients seems to be highly variable. 38 This wide range seems to hamper its use in daily clinical practice, especially for individual titration of palliative sedation. Finally, none of the studies analyzed here have considered the fact that basal BIS values may be lower with age 53 , as well as in common palliative situations, such as delirium, 54 dementia, 55 hepatic encephalopathy, 56 hypothermia, 57 stroke, 58 and administration of anti-convulsing agents. 59
We found that palliative sedation nociception monitoring reports remain scarce, suggesting that barriers limit its use in palliative medicine. Barriers could be related to cost, limited device usefulness, and lack of validation studies among terminally ill sedated populations. Above all, there is the fact that monitoring nociception, though suitable for adapting anesthesia to nociceptive surgical stimuli, does not equate to, or allow, pain monitoring. Whereas monitoring the degree of hypnosis is achieved through the direct evaluation of the electroencephalogram signals, the nociception−antinociception balance is monitored by indirectly evaluating certain variables. From a clinical point of view, low ANI (representing high stress levels) may indicate insufficient analgesia, while high ANI (representing low stress levels) reflects the absence of pain in sedated patients, which is relevant to ensure a patient is comfortable under palliative sedation.
During anesthesia, analgesics have usually been titrated by established clinical surrogates of nociception. These surrogates combine clinical signs of stress-induced sympathetic system activation, such as an increase in heart rate, mean arterial pressure, sweating, lacrimation, and movement. In the recent past, sophisticated physiological data analysis techniques that relied on heart rate variability (such as ANI) or pupillary dilatation were developed to monitor nociception during general anesthesia. 60 Compared to simple heart rate and mean arterial pressure, the ANI and pupillary dilatation analyses were proven superior for detecting painful surgical stimulations. However, they have a limited predictive value. 60 Yet, more recent studies suggest that the variation coefficient of pupillary diameter could be useful for monitoring pain during the postoperative period, whereas the pain assessment ability with ANI is poor. 61 Although some nociception monitors, such as the surgical plethysmographic index, show promising results, no definitive conclusions can be drawn regarding the effect of nociception monitoring on intraoperative opioid consumption or other anesthesia-related outcome. 62
Finally, compared to the huge volume of literature related to palliative sedation, it is striking that a single case report suggested that monitoring palliative sedation in real-time could lead to lower recovery delays during temporary or intermittent sedation. 36 In addition, a single study reported that monitoring palliative sedation in real-time could be used to avoid opioid and sedatives overdosage thus, enhancing safety and quality of care. 35
Recommendations for future research
Our search did not identify randomized or quasi-randomized trials, and the only reports available were small uncontrolled studies. Therefore, well-designed, larger controlled observational or randomized studies are needed. This review demonstrates the lack of suitable and shared outcomes for palliative sedation in the literature, as previously reported by Schildmann et al. 63 It is recommended that a common outcome set is used in practice, as well as in studies on palliative sedation. Moreover, as reported in a recent review, it is imperative that further studies on palliative sedation report patient comfort and relief of refractory symptoms. Reports should also devote greater attention to the improvement of patient-centered results. 15
Validation studies of nociception monitoring of non-sedated terminally ill patients are lacking. Our review found no study that discussed the inapplicability of nociception-index monitoring due to low heart variability and autonomic dysfunction that are often present in some advanced cancers and in chronic heart failure.64,65 The ANI cofounders include non-sinus cardiac rhythms, apnea, beta blockers, the presence of a pacemaker, autonomous nervous system disorders or perturbations, and even surrounding noise—all of which limit ANI’s reliability and use. 24 Many of these conditions may prevent ANI usage in the end-of-life context.
Large studies are also needed to validate monitoring depth of sedation monitoring in terminally ill patients receiving midazolam in addition to various opioids and neuroleptics, such as haloperidol.
The efficacy of BIS-guided infusion of propofol, dexmedetomidine, and midazolam for sedation has been tested and validated in diverse contexts.66,67 Conversely, BIS inapplicability is known for patients sedated with ketamine, and BIS has been shown to be problematic with low-dose combinations of propofol and midazolam or fentanyl and midazolam.68–70
Conclusion
There is growing concern that the observation-based methods currently used may not be sufficiently effective to optimize outcomes in sedated patients. Given the potential benefits identified in the studies reviewed, the findings indicate that monitoring sedation has the potential for assessing the depth of sedation and the absence of pain. There is, however, no conclusive evidence that depth of sedation and nociception monitoring can improve palliative sedation outcomes and no evidenced-based reasons for palliative care caregivers to change their current practice. These findings support the need for continued—but higher quality—research in this area.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211022943 – Supplemental material for Monitoring nociception and awareness during palliative sedation: A systematic review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211022943 for Monitoring nociception and awareness during palliative sedation: A systematic review by Nathalie Dieudonné Rahm, Ghizlaine Morawska, Sophie Pautex and Nadia Elia in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163211022943 – Supplemental material for Monitoring nociception and awareness during palliative sedation: A systematic review
Supplemental material, sj-pdf-2-pmj-10.1177_02692163211022943 for Monitoring nociception and awareness during palliative sedation: A systematic review by Nathalie Dieudonné Rahm, Ghizlaine Morawska, Sophie Pautex and Nadia Elia in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163211022943 – Supplemental material for Monitoring nociception and awareness during palliative sedation: A systematic review
Supplemental material, sj-pdf-3-pmj-10.1177_02692163211022943 for Monitoring nociception and awareness during palliative sedation: A systematic review by Nathalie Dieudonné Rahm, Ghizlaine Morawska, Sophie Pautex and Nadia Elia in Palliative Medicine
Supplemental Material
sj-pdf-4-pmj-10.1177_02692163211022943 – Supplemental material for Monitoring nociception and awareness during palliative sedation: A systematic review
Supplemental material, sj-pdf-4-pmj-10.1177_02692163211022943 for Monitoring nociception and awareness during palliative sedation: A systematic review by Nathalie Dieudonné Rahm, Ghizlaine Morawska, Sophie Pautex and Nadia Elia in Palliative Medicine
Footnotes
Author contributions
NDR and GM contributed equally. NDR and NE were involved in the development of the study question. NDR and GM performed the literature search, study selection, and data extraction. NDR, GN, and NE contributed to the, data analysis, and wrote the manuscript. All authors have reviewed and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
This review did not directly involve human participants and required no approval from an ethics committee or institutional review board.
Data management and sharing
There is no further information available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.