
Abstract
Background:
To date, little is known about the characteristics of patients who are admitted to a palliative care bed for end-of-life care. Previous data suggest that there are disparities in access to palliative care services based on age, sex, diagnosis, and socioeconomic status, but it is unclear whether these differences impact access to a palliative care bed.
Aim:
To better identify patient factors associated with the likelihood/rate of admission to a palliative care bed.
Design:
A retrospective chart review of all initiated palliative care bed applications through an electronic referral program was conducted over a 24-month period.
Setting/participants:
Patients who apply and are admitted to a palliative care bed in a Canadian metropolitan city.
Results:
A total of 2743 patients made a total of 5202 bed applications to 9 hospice/palliative care units in 2015–2016. Referred and admitted cancer patients were younger, male, and more functional than compared to non-cancer patients (all p < 0.001). Referred and admitted patients without cancer were more advanced in their illness trajectory, with an anticipated prognosis <1 month and Palliative Performance Status of 10%–20% (all p < 0.001). On multivariate analysis, a diagnosis of cancer and a prognosis of <3 months were associated with increased likelihood and/or rate of admission to a bed, whereas the presence of care needs, a longer prognosis and a PPS of 30%–40% were associated with decreased rates and/or likelihood of admission.
Conclusion:
Patients without cancer have reduced access to palliative care facilities at end-of-life compared to patients with cancer; at the time of their application and admission, they are “sicker” with very low performance status and poorer prognoses. Further studies investigating disease-specific clinical variables and support requirements may provide more insights into these observed disparities.
There are clear disparities in access to palliative care services based on age, sex, diagnosis, and socioeconomic status, but it is unclear whether this disparity is due to a lack of referral or differential acceptance to these services.
Patients without cancer have reduced access to palliative care facilities at end-of-life compared to patients with cancer and despite being “sicker” with poorer performance status and worse prognosis, patients without cancer had both a lower rate and likelihood of admission to a palliative care unit/hospice (referred to as “palliative care bed” in this paper).
Despite indicating a wish to be cared for in a palliative care bed, patients without cancer are less likely to be admitted to one. Further studies investigating disease-specific clinical variables and support requirements may provide more insights into these observed disparities.
Background
Access to palliative care facilities should be based on patient need and preferences for end-of-life care. However, data from Canada, the United States and the United Kingdom suggest disparities in access to palliative care services based on age, sex, disease trajectory, and neighborhood.1–6 For example, patients with low socio-economic status are less likely to access palliative care services across all settings including home,2,7,8 inpatient hospice care, 9 and specialist palliative care. 10 Other variables associated with reduced access to palliative care services include being male,2,11 older age, 8 single,2,11 living alone, 8 or immigrant status. 10
Patients with cancer are more likely to receive palliative care services at end of life12–14; in fact, those dying with cancer are up to five times more likely to receive home palliative care services compared to those with non-malignant disease. 15 Despite similar symptom needs, patients with non-malignant disease tend to access palliative care later in the disease trajectory2,5,16,17 and tend to be less functional when referred to palliative care services. 18 The sole existing study comparing characteristics of patients with and without cancer admitted to palliative care beds 19 used data from local databases of four palliative care units. Compared to patients with cancer, those without cancer had a shorter prognosis on admission and a shorter length of stay. It is unclear from these results whether disparities in admission practices contributed to these differences, as these studies assessed only patients who were admitted, without taking into account patients who were not admitted.
Our current study compares characteristics of patients with and without cancer who apply and are admitted to palliative care beds in Toronto, Canada. The analysis of admission patterns can provide a better understanding of current gaps in ensuring equitable access to palliative care beds.
Methods
The primary objective of this study was to determine if patient related factors are associated with the increased likelihood and rate of admission to a palliative care bed.
Setting and data sources: Palliative care bed application process
Toronto has a web-based palliative care bed application system that matches patients to appropriate clinical services. At the time of this study, the program managed referrals to 210 palliative care beds in 8 palliative care units and 1 residential hospice, for a total of 9 sites. These publicly funded palliative care units are located in and around the city of Toronto (population 6 million) and are located in acute care, long-term care, complex continuing care, and stand-alone facilities. Patients are most often referred for end of life care but may also apply for palliative care beds for respite or optimizing symptom management. Only those referred for end of life were assessed in this study. Applications for all sectors are assessed by clinicians and health administrators who triage the referrals. This includes patients who are both within and outside the region (previously called a Local Health Integration Network, as defined by government boundaries), 20 applying from acute care, complex continuing care, long-term care, and the community. Each site reviews applications and makes an internal decision to reject, or accept and admit patients. Most facilities accept patients with a prognosis of less than 3 months for end of life care. Data from patients living outside the region were excluded from our analysis, as they could have also applied to palliative care beds in their own region, which would have been managed by a different application system.
Study design and patients
We conducted a retrospective chart review of all initiated electronic applications for all nine palliative care bed sites, specifically for end of life care, during the period of January 1, 2015 to December 31, 2016. Patient demographic data included: age, sex, primary language, postal code, primary palliative diagnosis, palliative performance scale (PPS),21–23 and anticipated prognosis at the time of application. We also reviewed applicants’ special care needs, including oxygen, drains (i.e. catheters), wound care, behavioral observation, infusion pumps, central lines, hydration, therapeutic surface, and ostomy care.
Patient postal code details 24 were utilized to infer data related to neighborhood income per person equivalent (Quintile of Annual Income Per Person Equivalent (QAIPPE)), based on Statistics Canada census data from 2006. 25 This represents the neighborhood income quintile in which the patient lived, where QAIPPE 1 refers to the lowest income quintile, 5 refers to highest income quintile, and 9 refers to missing data. 25
Statistical analysis
The primary objective of this study was to identify factors associated with the likelihood and rate, respectively, of admission to a palliative care bed. The unit of the analysis was the patient; a patient could apply to an unlimited number of palliative care units.
First, we calculated simple descriptive statistics in the form of means and standard deviations for continuous variables and counts and percentages for discrete variables. We compared characteristics of patients with and without cancer who were referred and admitted, respectively, using t-tests for continuous variables and chi-square tests for categorical variables.
Next, we conducted regression analyses, using two outcomes. The first outcome was binary, denoting whether or not the patient was admitted to a palliative care bed. Bivariate and multivariate logistic regression was used to investigate factors impacting the likelihood of a patient being admitted to a palliative care bed. Over-dispersion was accounted for by using the deviance scale adjustment factor. The second outcome was rate-based and assessed the number of admissions per palliative care bed application. Poisson regression was used, modeling factors impacting the expected rate of admission. Over-dispersion was accounted for by using the deviance scale adjustment factor. We included all variables measured in the web-based system in our multivariate regression analysis.
Although both outcomes reflect patients’ admission to palliative care beds, they denote distinctly different evaluations. The binary outcome, “likelihood of admission” reflects whether a patient was admitted to a palliative care bed. This does not take into account the practice of sending multiple palliative care bed applications for one patient to improve the chance of admission to any palliative care bed. Thus, the rate-based outcome indicates a “rate of admission” controlling for the number of applications.
Ethics approval
This study was approved by Research Ethics Board at the University Health Network, Toronto, Ontario.
Results
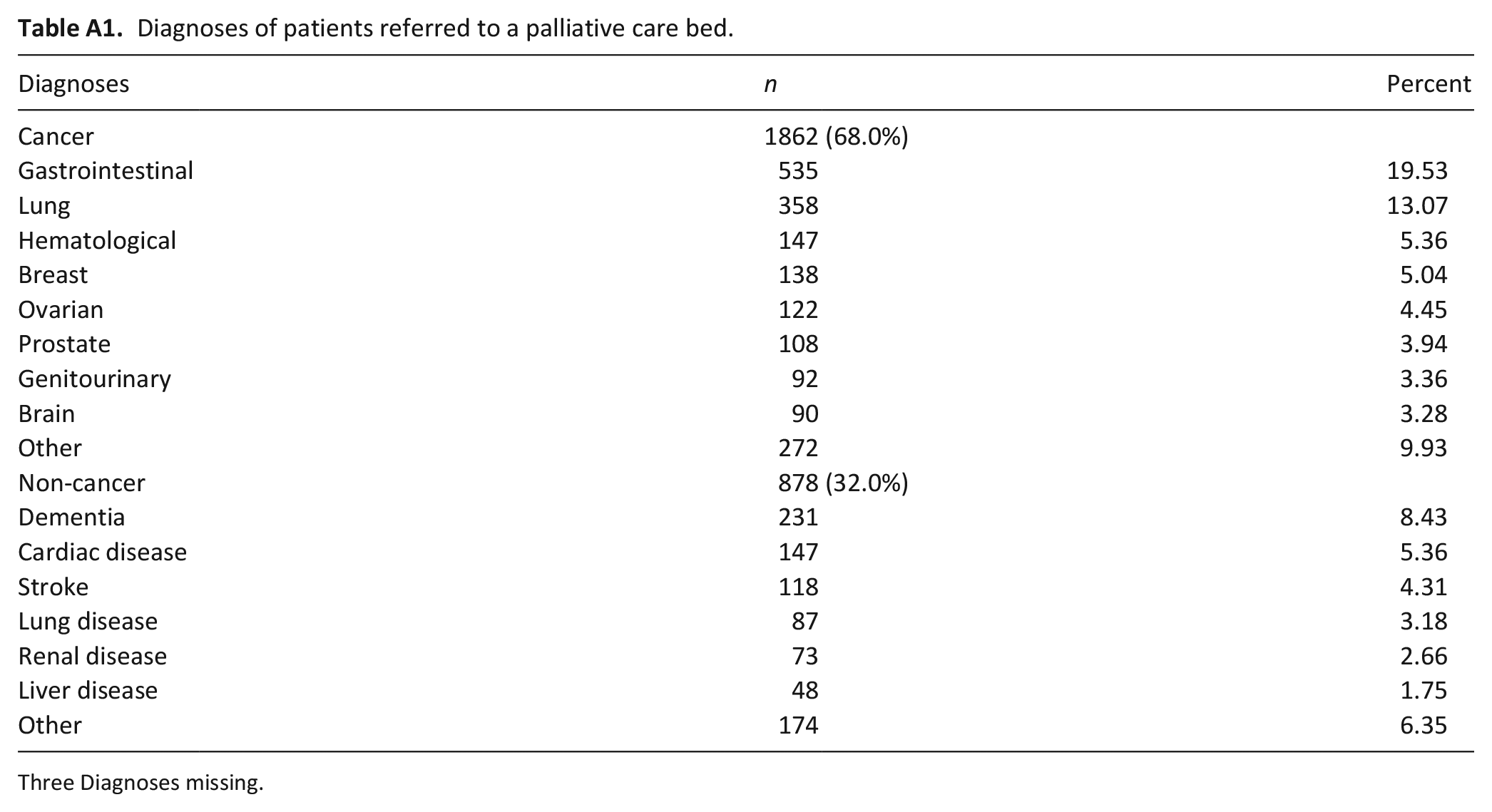
A total of 2743 unique patients placed 5202 applications for palliative care beds for a mean of 1.896 (SD 1.315) applications per patient through the application program during the study time frame. Patients had a mean age of 78.9 years; approximately half were female (51%) and most spoke English as a first language (80%) (Table 1). Most had PPS scores of 30%–40% (62%) and had a prognosis of <3 months (57%). For neighborhood income, 49% of applications were from the two lowest quintiles and 36% from those with the highest income. The most common non-malignant diagnoses of referred patients (see Appendix Table A1) included dementia (8.4%), cardiac (5.4%), and stroke (4.3%) whereas the most common cancer diagnoses included gastrointestinal (19.5%), lung (13.1%), and hematological (5.4%) malignancies.
Comparison of characteristics between cancer and non-cancer patients referred and admitted to a palliative care bed.
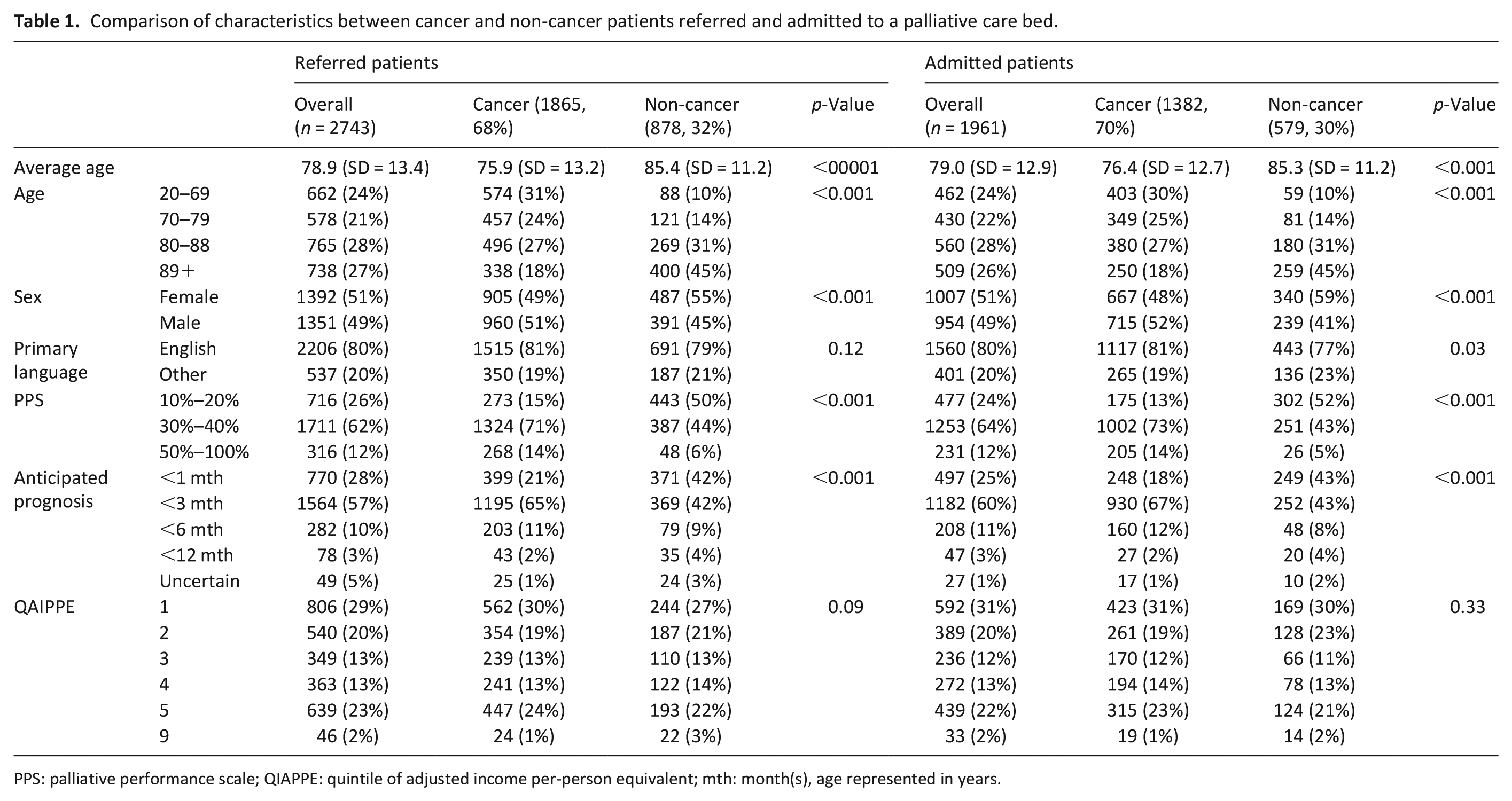
PPS: palliative performance scale; QIAPPE: quintile of adjusted income per-person equivalent; mth: month(s), age represented in years.
Although characteristics of referred patients were similar to those for admitted patients, there were differences between patients with and without cancer (Table 1). Referred and admitted patients with cancer were more likely to be younger (p < 0.001), male (p < 0.001), and to have higher PPS scores (p < 0.001) compared to patients without cancer. The distribution of anticipated prognosis also varied: non-cancer patients were more likely to have a prognosis of <1 month, whereas patients with cancer were more likely to have a prognosis of <3 months.
Table 2 compares the care needs that were documented for patients with and without cancer who were referred and admitted to a palliative care bed. Of the patients admitted, those with cancer had significantly more care requirements for drains, infusion pumps, central lines, and ostomies compared to non-cancer patients. In contrast, non-cancer patients who were admitted had significantly greater requirements listed for oxygen and wound care.
Comparison of care needs for patients with and without cancer who were admitted to a palliative care bed.
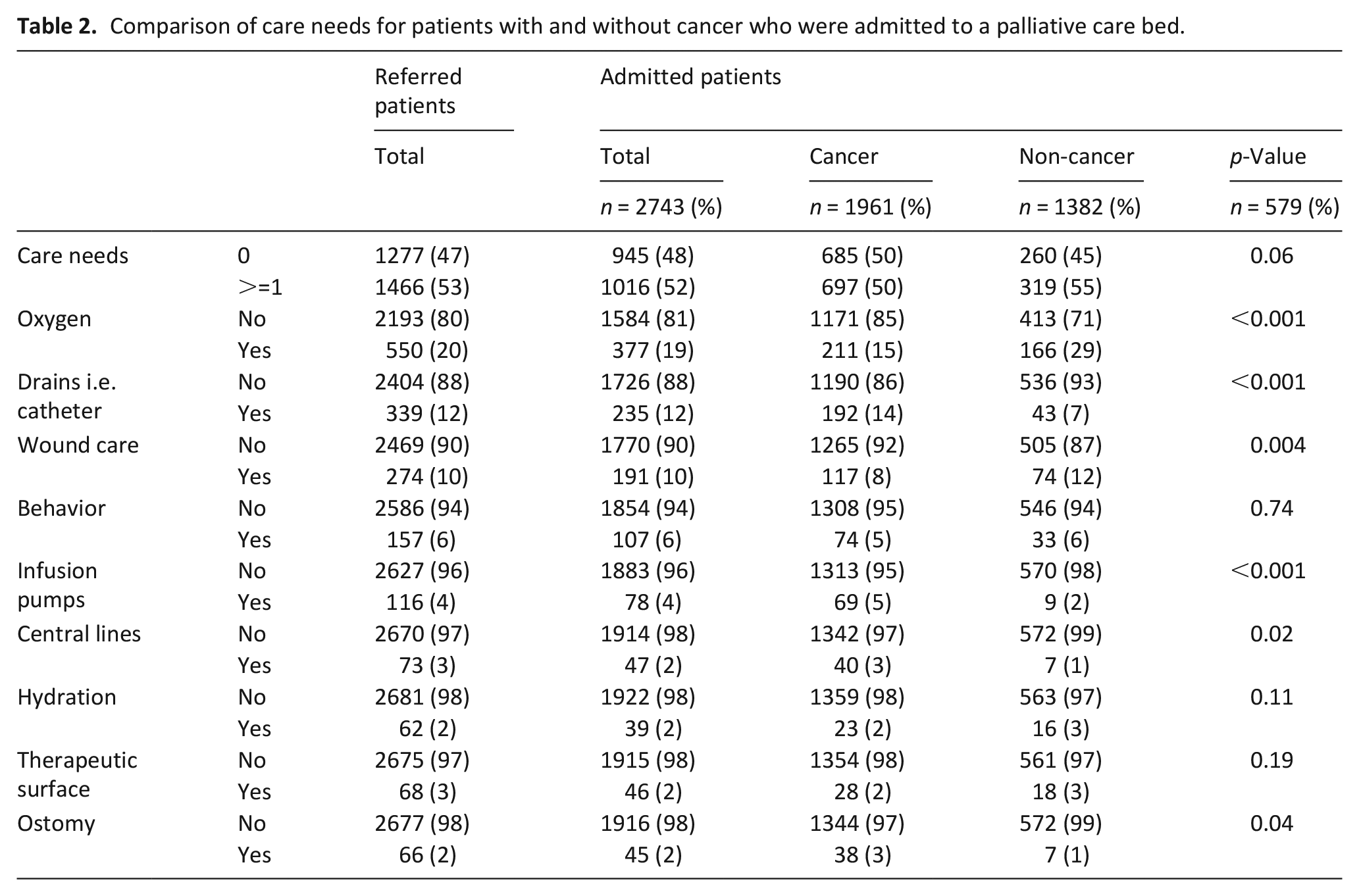
Table 3 reports bivariate factors associated with the likelihood of an admission to a palliative care bed. Patients with a cancer diagnosis were more likely to be admitted compared to those with a non-cancer diagnosis (OR 1.48, 95% CI 1.24–1.76, p < 0.001). Patients with better prognosis (PPS scores of 30%–40% or 50%–100% compared to 10%–20%), an anticipated prognosis of less than 3 or 6 months, and no special care needs were more likely to be admitted. Patients from mid or upper income quintile neighborhoods (QIAPPE 3 and 5) were less likely to be admitted than those from the lowest income neighborhoods. There were no observed statistically significant associations between specific special care needs and the likelihood admission.
Unadjusted probability and 95% confidence interval of likelihood of admission to a palliative care bed. Odds ratios, 95% confidence intervals, and p-values from bivariate logistic regression modeling of factors impact the odds/likelihood of an admission.
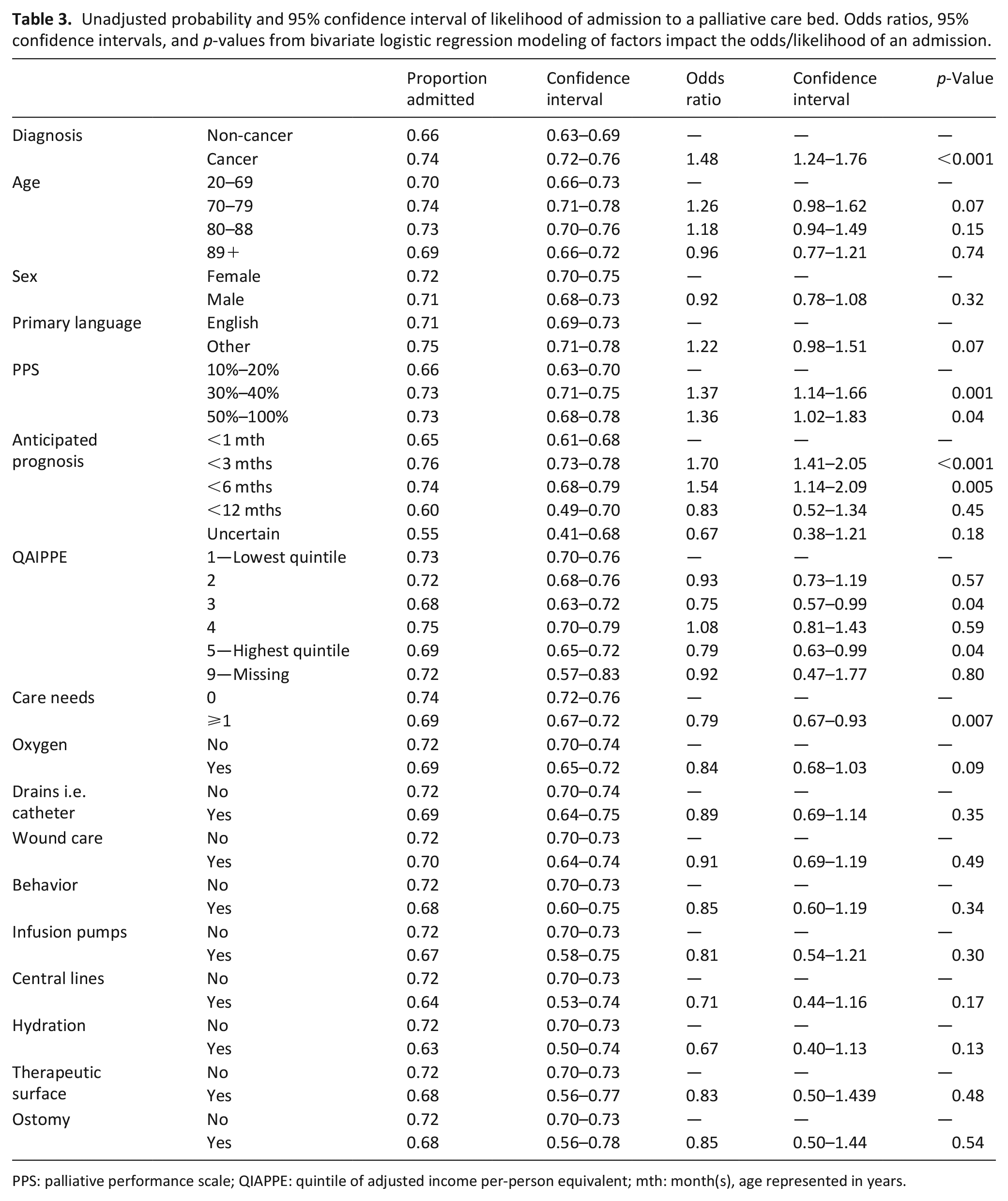
PPS: palliative performance scale; QIAPPE: quintile of adjusted income per-person equivalent; mth: month(s), age represented in years.
Table 4 presents bivariate associations on factors influencing the rate of admission to a palliative care bed (per application sent). Patients with a cancer diagnosis had an increased rate of admission compared to those without cancer (RR 1.14, 95% CI 1.05–1.24, p = 0.001). Those with a longer expected prognosis (<12 months, p = 0.005) and those identified to have one or more special care need (p = 0.002) had a lower rate of admission. Those who indicated a behavioral special need (i.e. requiring a bedside sitter, risk of wandering, etc.), and a need for a therapeutic surface (i.e. mattress or special bed requirement) had lower admission rates.
Unadjusted rates and 95% confidence intervals of the rate of admission to a palliative care bed. Rate ratios, 95% confidence intervals, and p-values from bivariate Poisson regression modeling of factors impact the rate of an admission per application sent.
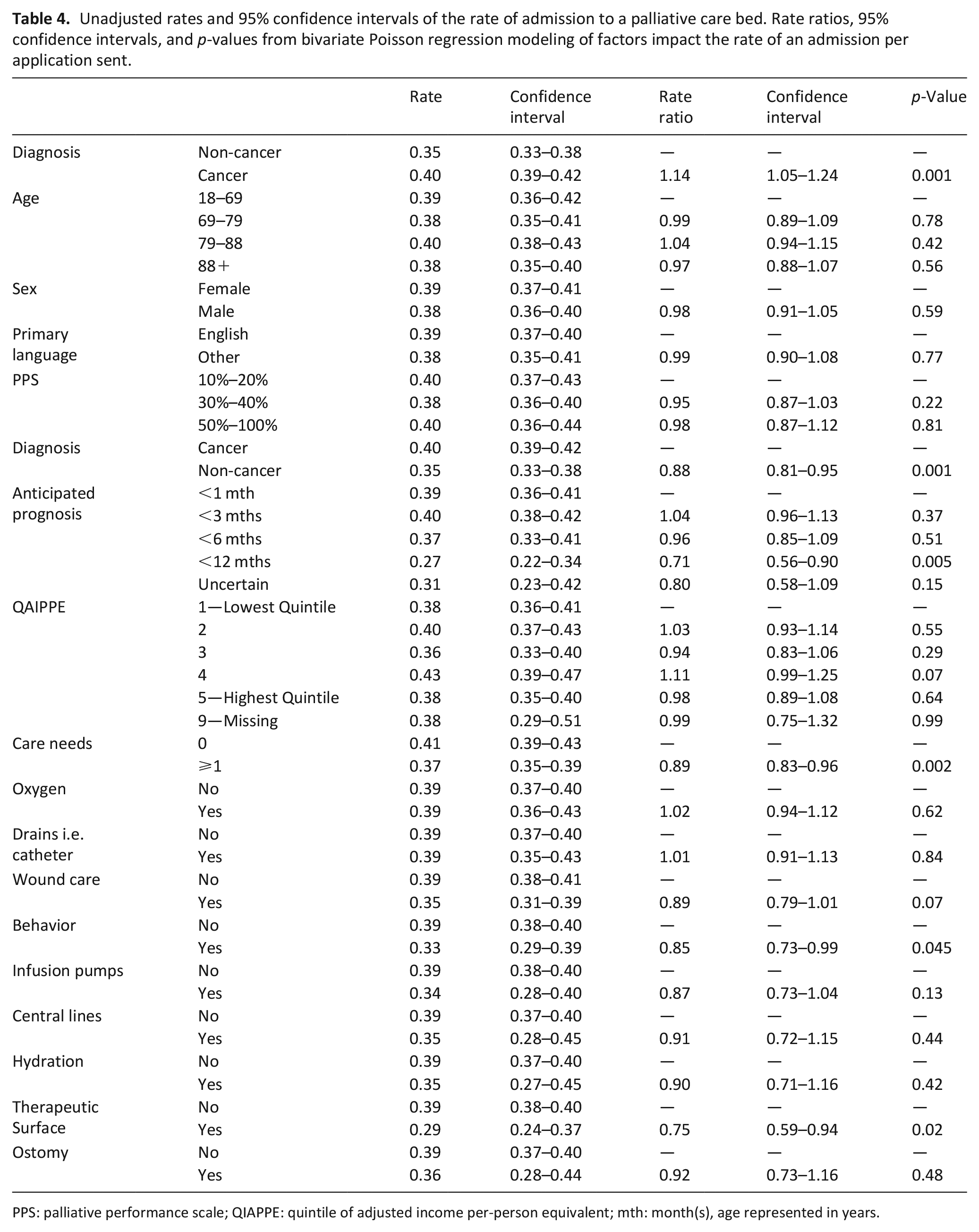
PPS: palliative performance scale; QIAPPE: quintile of adjusted income per-person equivalent; mth: month(s), age represented in years.
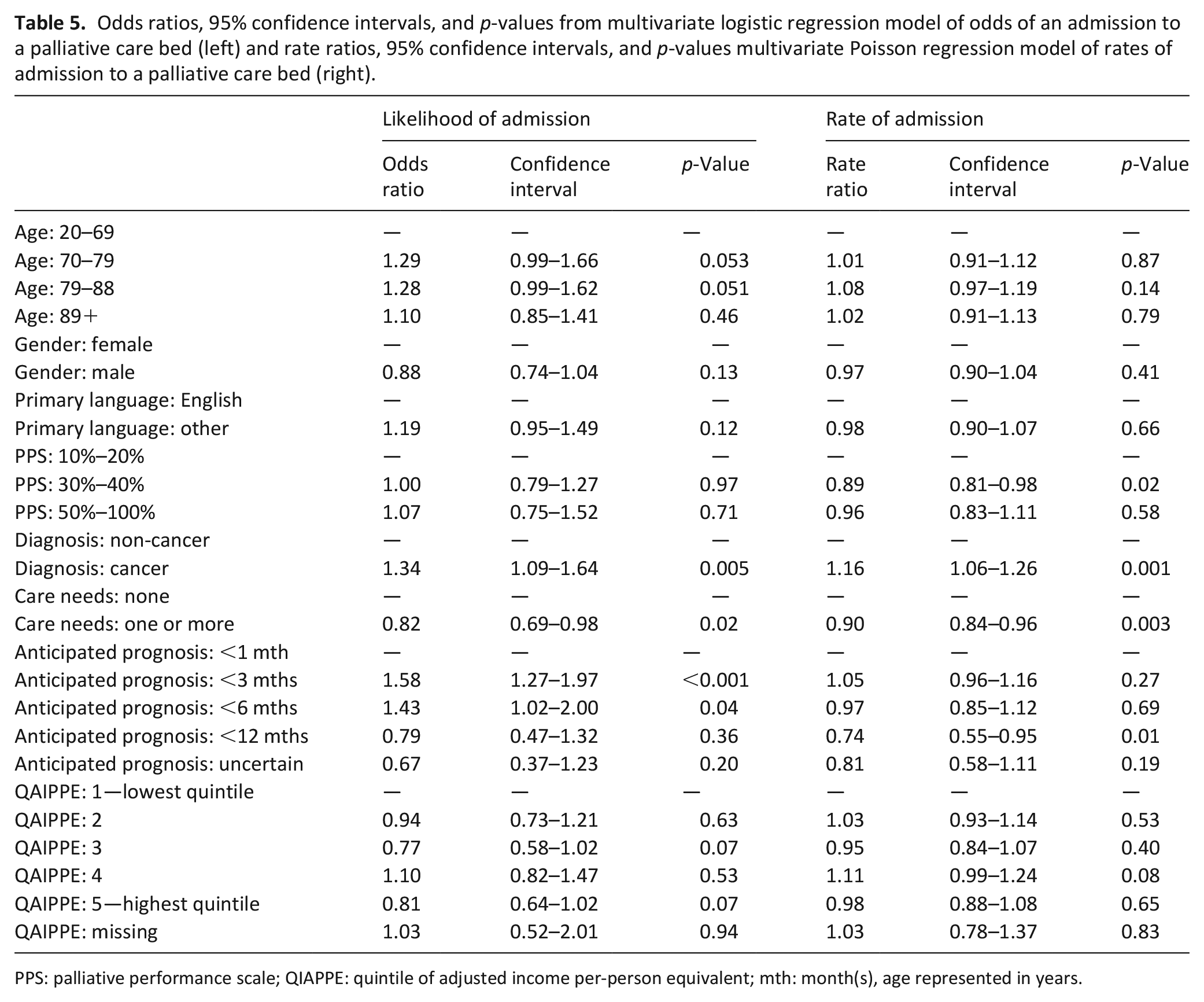
Table 5 presents the results of the multivariate logistic regression and multivariate Poisson regression analyses. On multivariate logistic regression analysis, patients with a cancer diagnosis had increased odds of admission compared to those without a cancer diagnosis (OR 1.34, 95% CI 1.09–1.64, p = 0.005). Older patients (aged 70–88) had higher odds of admission compared to younger patients (aged 69 or younger). Those with no special care needs and a short (<3 months) or mid-term (<6 months) prognosis had increased odds of admission to a palliative care bed.
Odds ratios, 95% confidence intervals, and p-values from multivariate logistic regression model of odds of an admission to a palliative care bed (left) and rate ratios, 95% confidence intervals, and p-values multivariate Poisson regression model of rates of admission to a palliative care bed (right).
PPS: palliative performance scale; QIAPPE: quintile of adjusted income per-person equivalent; mth: month(s), age represented in years.
Similarly, the multivariate Poisson regression analysis showed that patients with cancer had an increased rate of admission to a palliative care bed compared to those without cancer (RR 1.16, 95% CI 1.06–1.26, p = 0.001). Patients with no special care needs had an increased rate of admission compared to those with one or more special care need. Patients applying with a longer anticipated prognosis (<12 months) had a lower rate of admission, as did those patients with a PPS of 30%–40% in comparison to PPS 10%–20%.
Discussion
In reviewing application data to palliative care beds over a 2-year period, patients with cancer were younger, male, and more functional at the time of application compared to patients without cancer. Those without cancer were more advanced in their illness trajectory, with an anticipated prognosis of <1 month and applied with a lower PPS of 10%–20%. Despite these differences, patients with cancer were far more likely to be admitted to a palliative care bed than those without cancer. Palliative care has traditionally been linked to patients with cancer, perhaps because of the more predictable functional decline when no further cancer-directed therapies can be offered. In comparison, patients with non-cancer diagnoses tend to have a progressive yet unpredictable functional decline, with acute exacerbations and recoveries followed by eventual deterioration.26,27 Thus when patients with a non-malignant disease, such as COPD, heart failure, or dementia apply to a palliative care bed, they may be deemed “end-stage” only when death is imminent with multiple domains exhibiting loss of function.3,28,29
This discrepancy between access to palliative care beds between patients with and without cancer demonstrates the importance of reevaluating the timing and involvement of palliative care in chronic non-malignant illnesses. This inequity is particularly relevant as early palliative care has been shown to improve quality of life and decrease symptom burden.30,31 Patients suffering from chronic life-limiting disease often experience similar symptoms to those with advanced cancer—for example, COPD patients experience fatigue, dyspnea, insomnia, and low mood, similar to lung cancer patients32–34—but are often not referred to palliative care. This trend is consistent in other chronic life-limiting illnesses, such as heart failure, end-stage renal disease, and dementia.27,29,35 There is a growing sentiment that inequities exist between patients with malignant and non-malignant disease in accessing palliative care resources and support throughout their disease trajectory. For instance, a recent study found that 42.1% and 46.8% of Canadian cardiologists (n = 551) believed that specialized palliative care services prioritize and are designed to meet the needs of patients with cancer, respectively. 36 This paper highlights this disparity for patients approaching end of life.
Previous local data suggest that middle-aged patients living in urban and higher income neighborhoods have a higher odds of receiving palliative care. 3 Similarly, those living in poorer neighborhoods are least likely to receive home visits from a physician. 5 In our study, older patients and those from lower quintile neighborhoods had higher odds of admission to palliative care beds. This may be related to poorer social support, healthcare service integration, or multiple complex comorbidities. For example, lack of caregiver support or available home services may necessitate an admission to palliative care bed for ongoing care when the patient’s status deteriorates. Further investigation into the reason of referral and associated symptom burden or functional status of patients referred or admitted to palliative care beds may provide insights to how our system can improve access to and utilization of palliative care.
Declining functional status and expected survival of less than 3 or 6 months at the time of application were positively associated with a palliative care bed admission, while patients with longer expected survival had lower admission rates. Accurate prognostication for frail elderly patients with multiple comorbidities has been a longstanding challenge, making it difficult to predict the appropriate timing for of a palliative care bed application for end of life care.2,15,28 Overall prognostication by clinicians is poor 37 and is less reliable with a longer expected survival (i.e. 6 months vs 1 month).19,23,38 Traditionally, the trajectory of “end-stage” cancer patients has been easier to predict than for non-malignant diseases, where acute exacerbations can temporarily worsen functional status but patients may stabilize.27,28,35 As a result, despite being “end-stage,” those with advanced non-cancer disease may be excluded from short-term palliative care beds which prioritize patients with a predictable life expectancy of short months such as in cancer patients.
Patients with more than one special care need, particularly behavioral monitoring or requirement for a therapeutic surface, were also found to have lower rates of palliative care bed admission. This finding may be attributed to the fact that hospice and palliative care units may not be well-equipped to handle these needs due to limited resources.38,39 Unfortunately, the resultant alternative of patients with complex care needs dying in acute care is more costly to the health care system. Recent data show that 60% of Canadians die in acute care whereas 15% die at home. 4 Our regional community services are often regarded as robust, compared to other regions in the country; despite this, data repetitively indicate 71.9% of palliative patient deaths occur in hospitals. 5 In our study, 30% of patients who applied to a palliative care bed did not receive a placement there. While their care setting at time of application was not captured, based on the above statistic, it is likely that they died in the acute care setting. This has major implications not only on utilization and costs to the healthcare system, but also on prioritizing patient-centered care if dying patients are not receiving care at end of life in their preferred setting of choice.
Limitations
The palliative care bed application system is an administrative tool, which cannot capture other factors that influence rates of admission specific to individual patient circumstances, such as caregiver factors. Another limitation is that our study did not account for patients who may have been accepted to a palliative care bed but not admitted because they died before a bed became available. Furthermore, data for referrals and admissions are not comprehensive, in that they represent only regional referrals through the system and not paper applications. This data also only represent a short period of time in Toronto, which has a large multicultural urban and suburban population.
Finally, this study only identifies patients who sought palliative care by requesting access to a facility for ongoing palliative care (palliative care bed). We do not have data on whether those patients accessed palliative care services in the community prior to seeking admission to a palliative care bed. As well, managing advanced malignant and non-malignant diseases using palliative care principles and practices should be within the domain of all health professionals and should not, in many cases, require the involvement of specialist palliative care. Nevertheless, placement in a specialized palliative care facility may be requested when care at home is not feasible, either due to symptom management concerns or due to care needs that exceed the capacity of the family caregiver.
What this study adds
Our study is the first to examine characteristics of patients who are referred and accepted into palliative care beds. We found a significant inequity between patients with and without cancer, representing a potential system-level discrepancy that needs to be addressed. Other factors that appeared to affect equality of access were functional status, anticipated prognosis, and presence of care needs. However, patients with the poorest performance status and prognosis, who were over-represented in the non-cancer group, tended to be disadvantaged in terms of acceptance for admission. Future studies investigating more specific patient characteristics relating to clinical variables and support requirements may provide more insights into the disparities observed in this study. Additionally, information regarding the timing from application to acceptance or admission into palliative care beds would help in understanding patients’ changes in care needs toward the end of their disease trajectory.
Footnotes
Appendix
Diagnoses of patients referred to a palliative care bed.
| Diagnoses | n | Percent |
|---|---|---|
| Cancer | 1862 (68.0%) | |
| Gastrointestinal | 535 | 19.53 |
| Lung | 358 | 13.07 |
| Hematological | 147 | 5.36 |
| Breast | 138 | 5.04 |
| Ovarian | 122 | 4.45 |
| Prostate | 108 | 3.94 |
| Genitourinary | 92 | 3.36 |
| Brain | 90 | 3.28 |
| Other | 272 | 9.93 |
| Non-cancer | 878 (32.0%) | |
| Dementia | 231 | 8.43 |
| Cardiac disease | 147 | 5.36 |
| Stroke | 118 | 4.31 |
| Lung disease | 87 | 3.18 |
| Renal disease | 73 | 2.66 |
| Liver disease | 48 | 1.75 |
| Other | 174 | 6.35 |
Three Diagnoses missing.
Author contributions
All authors: (i) Made a substantial contribution to the concept or design of the work; or acquisition, analysis, or interpretation of data. (ii) Drafted the article or revised it critically for important intellectual content. (iii) Approved the version to be published. (iv) Have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics
This study was approved by Research Ethics Board at the University Health Network, Toronto, Ontario (Study ID: 15-9561).
Data management
All data submitted complies with Institutional ethics board requirements and applicable government regulations.