
Abstract
Background:
Ethical issues arise daily in the delivery of palliative care. Despite much (largely theoretical) literature, evidence from specialist palliative care practitioners about day-to-day ethical challenges has not previously been synthesised. This evidence is crucial to inform education and adequately support staff.
Aim:
To synthesise the evidence regarding the ethical challenges which specialist palliative care practitioners encounter during clinical practice.
Design:
Systematic review with narrative synthesis (PROSPERO registration CRD42018105365). Quality was dual-assessed using the Mixed-Methods Appraisal Tool. Tabulation, textural description, concept mapping and thematic synthesis were used to develop and present the narrative.
Data sources:
Seven databases (MEDLINE, Philosopher’s Index, EMBASE, PsycINFO, LILACS, Web of Science and CINAHL) were searched from inception to December 2019 without language limits. Eligible papers reported original research using inductive methods to describe practitioner-reported ethical challenges.
Results:
A total of 8074 records were screened. Thirteen studies from nine countries were included. Challenges were organised into six themes: application of ethical principles; delivering clinical care; working with families; engaging with institutional structures and values; navigating societal values and expectations; philosophy of palliative care. Challenges related to specific scenarios/contexts rather than the application of general ethical principles, and occurred at all levels (bedside, institution, society, policy).
Conclusion:
Palliative care practitioners encounter a broad range of contextual ethical challenges, many of which are not represented in palliative care ethics training resources, for example, navigating institutional policies, resource allocation and inter-professional conflict. Findings have implications for supporting ethical practice and training practitioners. The lack of low- and middle- income country data needs addressing.
Keywords
Evidence from other areas of healthcare practice demonstrates that the ethical challenges discussed in the literature do not always accurately reflect the range of challenges that healthcare practitioners experience in real-world practice.
This phenomenon has not previously been systematically examined within palliative care.
Improving our understanding of the ethical challenges faced by specialist palliative care practitioners is needed to support staff in their day-to-day practice and to underpin evidence-based ethics training programmes in palliative care.
This systematic review identified ethical challenges in six themes: application of ethical principles; delivering clinical care; working with families; engaging with institutional structures and values; navigating societal values and expectations; and the philosophy of palliative care.
The range of ethical challenges faced by specialist palliative care practitioners exceeds the breadth of those detailed in palliative care textbooks and ethics resources.
The review found no data from low- or low middle-income country settings.
The broad range of ethical challenges identified suggests that training programmes and core texts in the field should expand their coverage to better support practitioners.
As most practitioners described highly context-based ethical challenges, tools that specifically include contextual data may be more appropriate when practitioners analyse their own cases.
The lack of data from low- and middle- income countries needs addressing as these are the settings with the highest levels of palliative care need, and many identified ethical challenges are context-specific and therefore may not be transferable between settings.
Introduction
In published literature, palliative care is associated with ethical challenges across varied aspects of clinical care.1–4 Challenge areas include, for example, withdrawing and withholding of interventions, 5 dignity and quality of care, 6 respect for autonomy 7 and palliative sedation.8,9 However, there is evidence from other areas of healthcare practice that the ethical challenges examined within theoretical literature do not accurately reflect the range of the dilemmas that healthcare workers report experiencing in real-world practice.10–12 Whilst this mismatch between lived experience and the theoretical academic literature has not previously been systematically examined within palliative care, there is some evidence suggesting it applies.13–15 Hermsen and ten Have, 13 for example, compared the ethical challenges reported by specialist palliative care providers with those found in the palliative care literature. They found 14 reported ethical challenges had no accompanying literature, and two topics with significant literature, including engaging with ethics committees, which were not reported in practice. 13
To the authors’ knowledge there is no project that has systematically collated the range of ethical challenges that are encountered within palliative care. Addressing this knowledge gap is important for the field going forward as training in the ethical aspects of palliative care is recognised as a priority and often requested by pracitioners.4,16 A thorough understanding of the ethical context practitioners work within is needed if educators are to generate evidence-based curricula that reflect real world contexts. Education activities can benefit from a robust grounding in the real-world experiences of learners as the relevance of educational material is a key factor in adult learner motivation, 17 and processing new material in relation to prior experiences contributes to learning efficiency. 18 Also importantly, as palliative care provision expands across the globe, there is a need to understand the nature and pattern of ethical challenges in differing global contexts. The palliative care global health literature currently contains little empirical engagement with ethical challenges within the field.19–21
We aimed to review and synthesise the literature to answer the research question: what ethical challenges do those working in specialist palliative care report experiencing in clinical practice?
Methods and analysis
We conducted a systematic review to identify and summarise empirical data on the ethical challenges specialist palliative care practitioners report experiencing. We used narrative synthesis, following the iterative framework from Popay et al., 22 adapted for a review which does not focus on an intervention. The integration of themes and content was guided by Thomas and Harden’s 23 ‘thematic synthesis’ approach.
The review protocol was designed and reported with reference to Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P). 24 We follow the PRISMA reporting guidelines for systematic reviews. 25 The protocol was prospectively registered with PROSPERO (CRD42018105365) 26 and published open access. 27 There were no deviations from the published protocol, outlined below.
Eligibility criteria
Inclusion and exclusion criteria are summarised in Table 1. As the commonly-used participants, interventions, comparisons, outcomes and study design (PICOS) system is not suitable for argument-based or empirical ethics reviews, 28 we used Strech et al.’s proposed adaptation: the Methodology, Issue, Participants (MIP) system. 28
Inclusion and exclusion criteria.
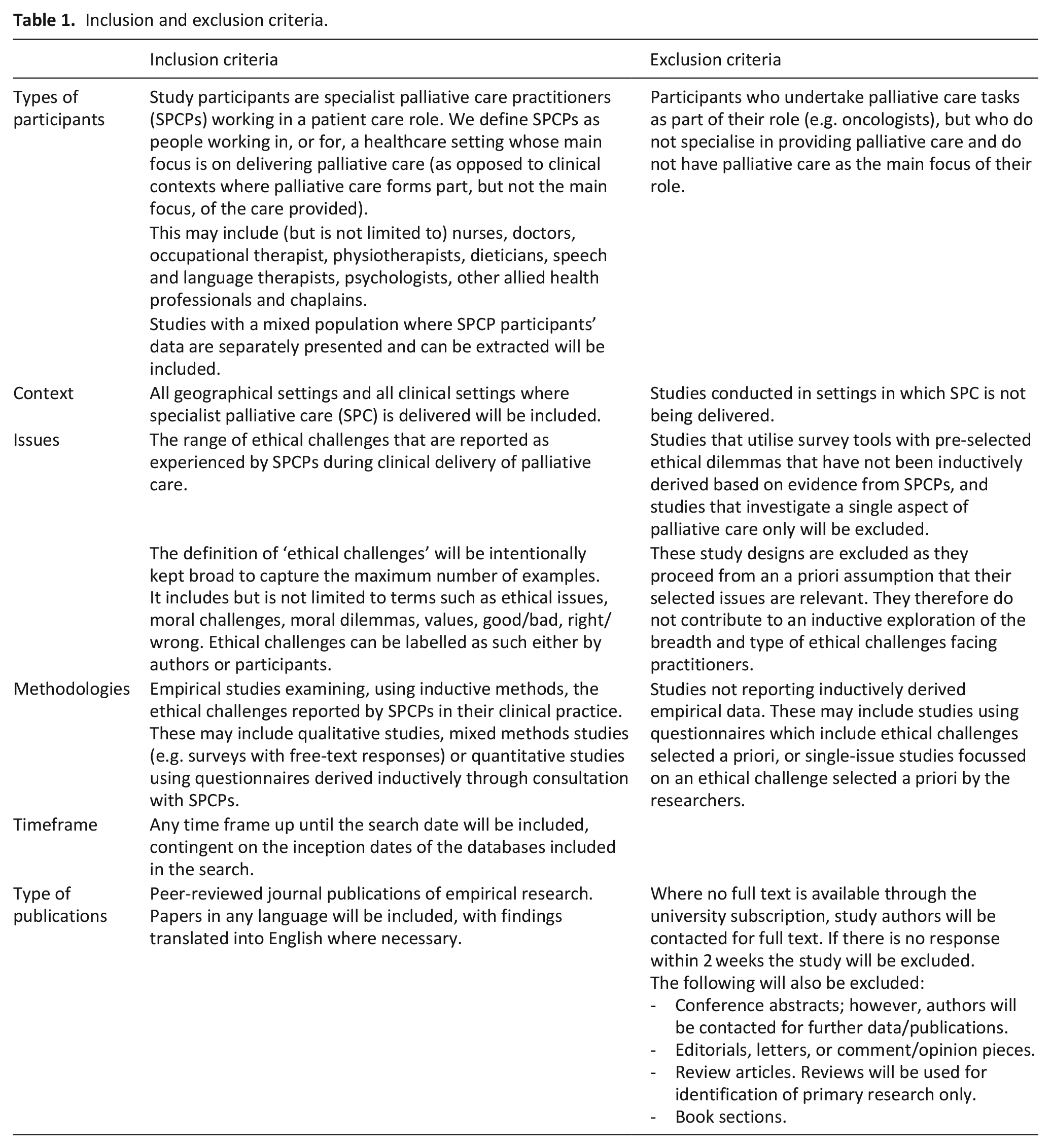
The review included peer-reviewed inductive studies which identify ethical challenges practitioners face in their real-world clinical practice, or secondary analyses of such data. Following Creswell and Plano Clark, inductive data, for the purpose of this review, is defined as that which derives from data collection efforts that occur independently from any attempt to validate a particular theory or hypothesis. 29 Studies that explored single topics in specialist palliative care practice selected a priori by researchers were excluded, as were studies that used a pre-determined list of ethical challenges. Whilst data from both these study types might contribute to describing ethical challenges in palliative care, both study types pre-suppose the presence of the challenges they focus on within the experiences of palliative care practitioners, which, as demonstrated by Hermsen and ten Have, may not be the case.13,27
To minimise bias and the omission of relevant international data, there were no language, geographical or timeframe restrictions, although the databases searched were in English.
Search strategy
We identified databases to search in conjunction with subject information specialists and by identifying which databases indexed journals containing key papers known to the research team. The following databases were searched on 19th December 2019: MEDLINE (Ovid interface, 1946 onwards), Philosopher’s Index (OVID interface, 1940 onwards), EMBASE (OVID interface, 1980 onwards), PsycINFO (OVID interface, 1806 onwards), LILACS (http://lilacs.bvsalud.org/en/, 1982 onwards), Web of Science (Clarivate interface, 1900 onwards) and CINAHL (EBSCO interface, 1937 onwards). Medline search terms (Table 2) were adapted for the other databases.
Medline search strategy.
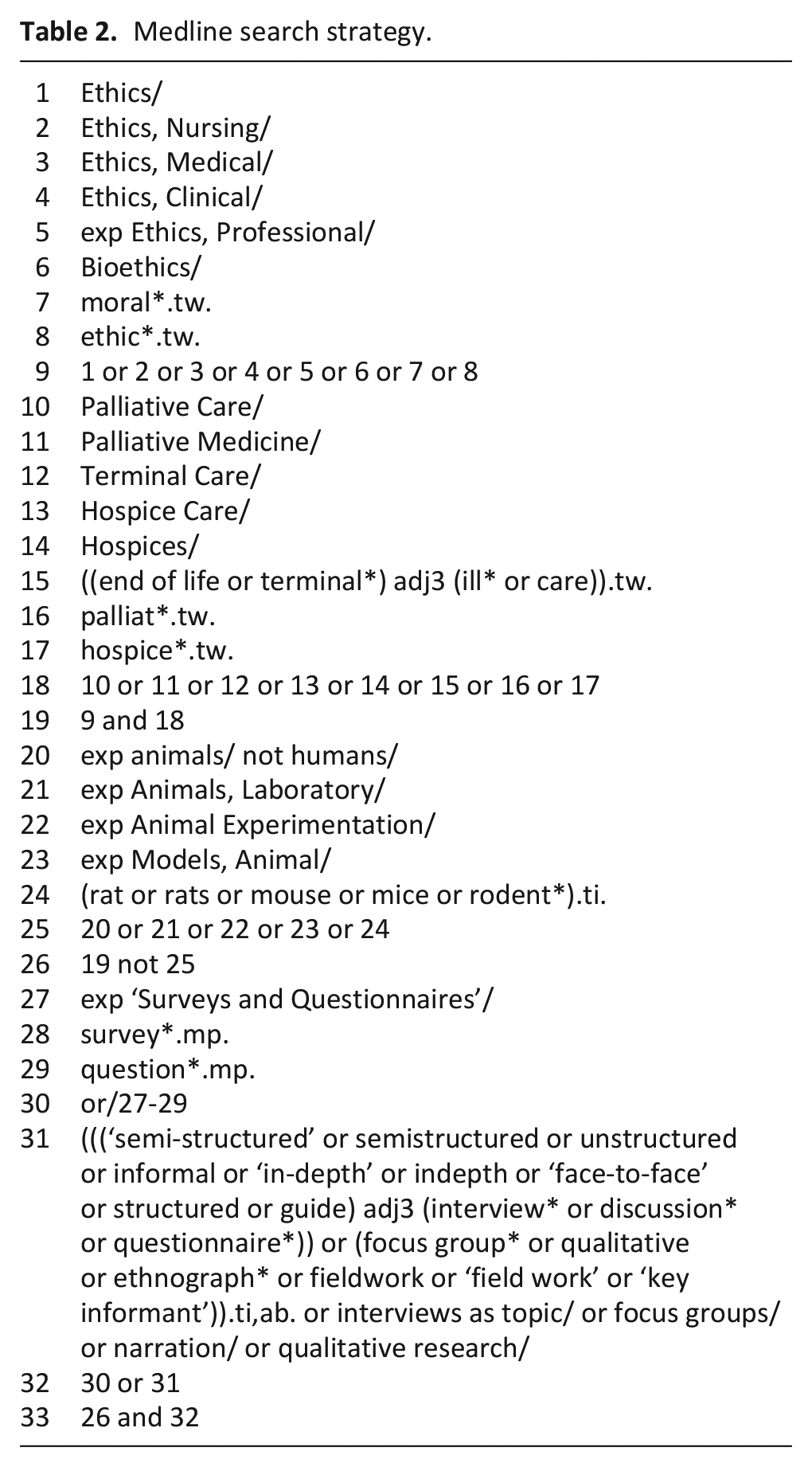
Initial scoping searches suggested that the search terms would return over 25,000 highly varied records, and that relevant inductive studies would use qualitative methods or mixed-methods surveys incorporating free-text responses. To capture the most relevant records we therefore used peer-reviewed methodological filters (Supplemental File 1) to refine the search results. The methodological filters were initially identified via the InterTASC Information Specialists’ Sub-Group Search Filter Resource. 30 Sentinel research outputs, known to the researchers prior the review, were tracked through the filter process and all were retrieved.
Reference lists of included papers were hand-searched. Corresponding authors of papers meeting the inclusion criteria were contacted and asked if they recommended other published work for review. Authors of conference abstracts were contacted for peer-reviewed data or follow-up publications if available, but no additional papers were identified. A grey literature search was not conducted. Cook et al. demonstrated that extensive grey literature searching did not benefit the review content of a palliative care systematic review despite requiring significant resources. 31
Search results were exported to, and collated and de-duplicated in, Endnote X9.2. 32
Selection process
Retrieved records were screened at title and/or abstract level by GS. A second researcher (MD) independently screened a random sample of 10%. 33 Differences in screening between GS and MD were discussed within the research team to clarify and refine inclusion/exclusion criteria. Study authors were contacted when further information was required. Contested papers were examined by a third reviewer (LS). The full texts of potentially eligible records were retrieved and independently assessed for eligibility by GS and MD.
Data extraction and management
Data extraction was undertaken independently by GS and MD, using a pre-piloted data extraction form. No data disagreements emerged. Data items extracted from included studies were: (1) citation details including title, publication year and journal; (2) study setting, methods, participant characteristics, sample size; (3) specified definition/conceptualisation of ethical challenges; (4) the study’s key findings, themes and sub-themes; and (5) sources of potential bias including funders and evidence of reflexivity. There was no missing data.
Data synthesis
We conducted an adapted narrative synthesis following the relevant framework stages described by Popay et al., 22 namely: developing a primary synthesis, exploring relationships within and between studies, and assessing robustness of the synthesis. Preliminary synthesis development included identifying and tabulating both textual descriptions of studies and study participant-derived data. Thematic synthesis based on Thomas and Harden’s framework 23 was then used, iteratively utilising the three stages of this approach: line-by-line coding of the text presented in the Results sections of the papers; development of descriptive themes; grouping and organisation of descriptive themes into higher-level analytical themes. Relationships within and between studies were explored (informed by concept mapping), including a focus on possible patterns related to study or participant characteristics such as geographical location, care setting and professional background. GS led the synthesis with regular discussions with MD and further discussions with EB, RH and LES until consensus around identified themes was reached. The robustness of the synthesis was enhanced through adopting this highly collaborative approach and the use of systematic methods to assess study quality (MMAT 2018) 34 and the final synthesis output (GRADE-CERQual). 35 As the review aimed to map the ethical challenges reported by specialist palliative care practitioners, we did not carry out theory development.
Risk of bias (quality) assessments
Scoping searches suggested that relevant studies would use qualitative and mixed-methods designs. To allow comparison of study quality, the Mixed-Methods Assessment Tool (MMAT) 2018 34 was used, with each study being scored independently by two reviewers (GS and MD). The MMAT focuses primarily on the methodological aspects of assessed studies, which aligns with the GRADE-CERQual recommendations for choosing a quality assessment tool. 36
To assess the quality of the review findings we applied GRADE-CERQual, 35 which provides a systematic framework for assessing confidence in individual review findings, based on consideration of four components: (1) methodological limitations, (2) coherence, (3) adequacy of data and (4) relevance.
Results
After de-duplication, the electronic searches, hand-searching and author contact identified 8074 individual records. A total of 7905 records were excluded at title and/or abstract level. About 170 abstracts were available only in Spanish or Portuguese and were assessed by MD, a native Spanish speaker also proficient in Portuguese. Only one record, published in Mandarin from Taiwan, was retrieved that did not have an English, Spanish or Portuguese language abstract. This was assessed by a native Mandarin speaker who was briefed on the inclusion criteria for the review and was excluded at the abstract stage. About 169 records were screened at full text, with 13 meeting the inclusion criteria (Figure 1). Reference lists of these papers were hand-searched. Ten additional records were found but excluded at the abstract stage.
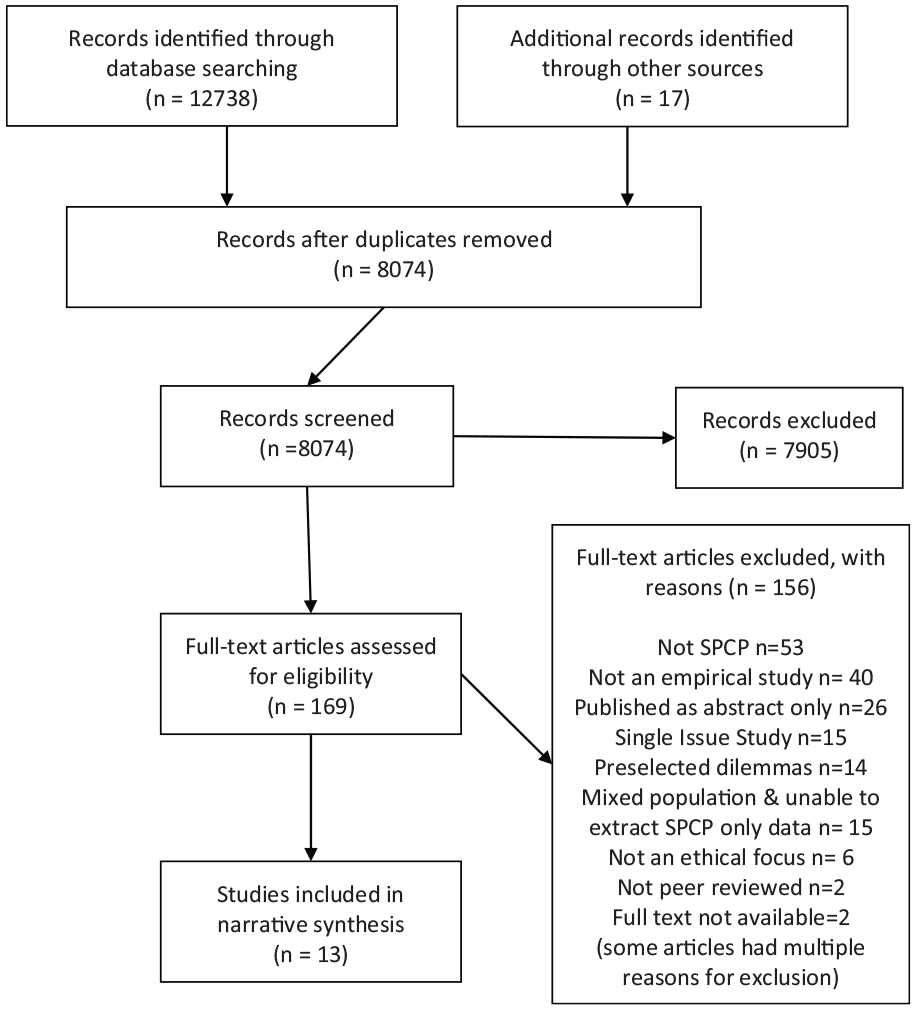
PRISMA flowchart.
All papers were published in English. The reported studies represented research from multiple international settings: Brazil,37,38 Canada, 39 Germany,40,41 Mexico, 15 the Netherlands, 13 Portugal, 42 Sweden, 43 Taiwan 44 and USA.45–47 Studies were published between 2000 and 2017; see Table 3 for details.
Included study details.
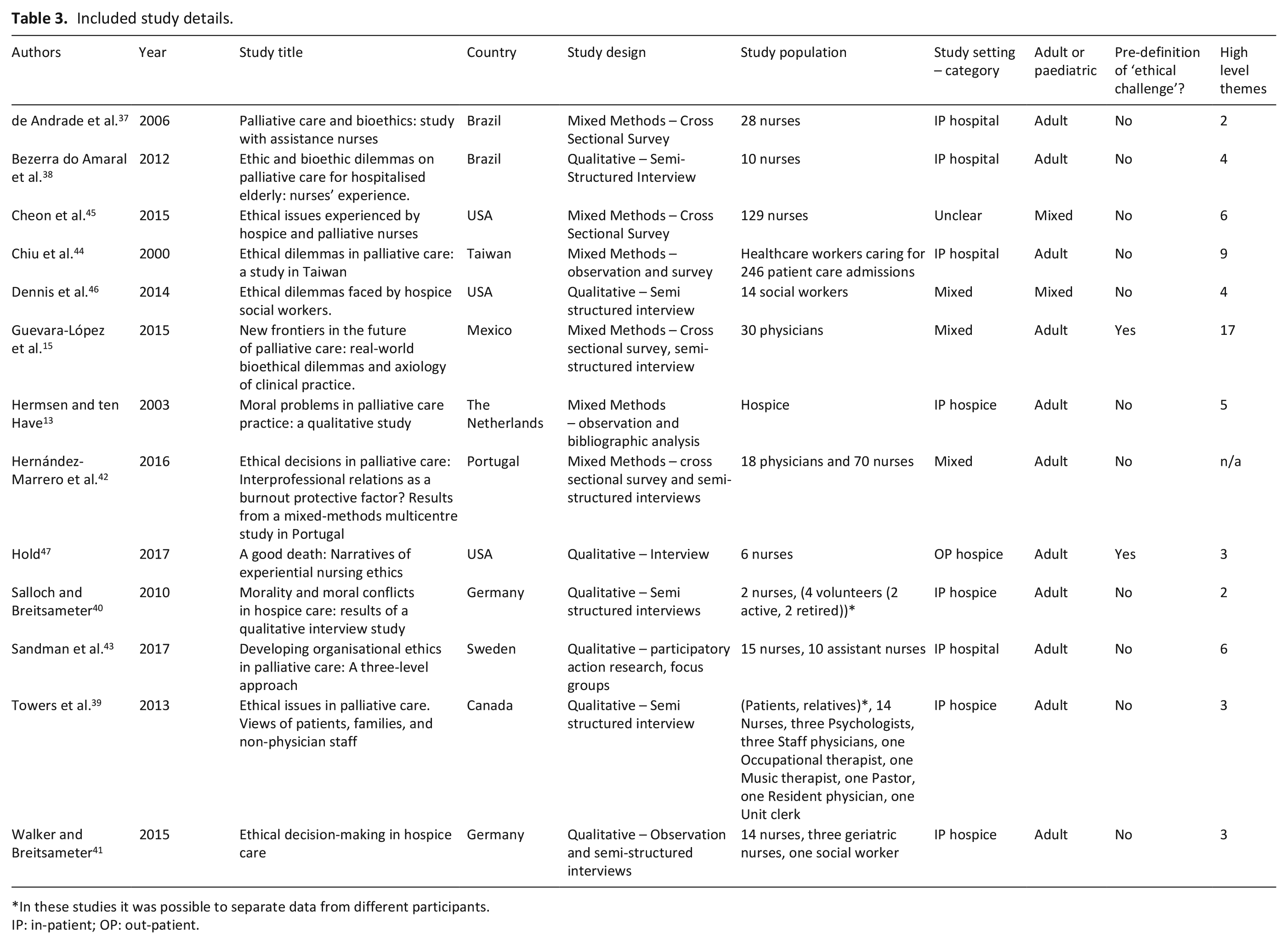
In these studies it was possible to separate data from different participants.
IP: in-patient; OP: out-patient.
Study quality assessment
All studies were dual evaluated by GS and MD using the MMAT 2018. 34 One study, de Andrade et al., 37 required discussion with a third reviewer (LS) as to which sections of the tool were appropriate. There were no disagreements in assessment. See Figure 2 for the MMAT evaluations.
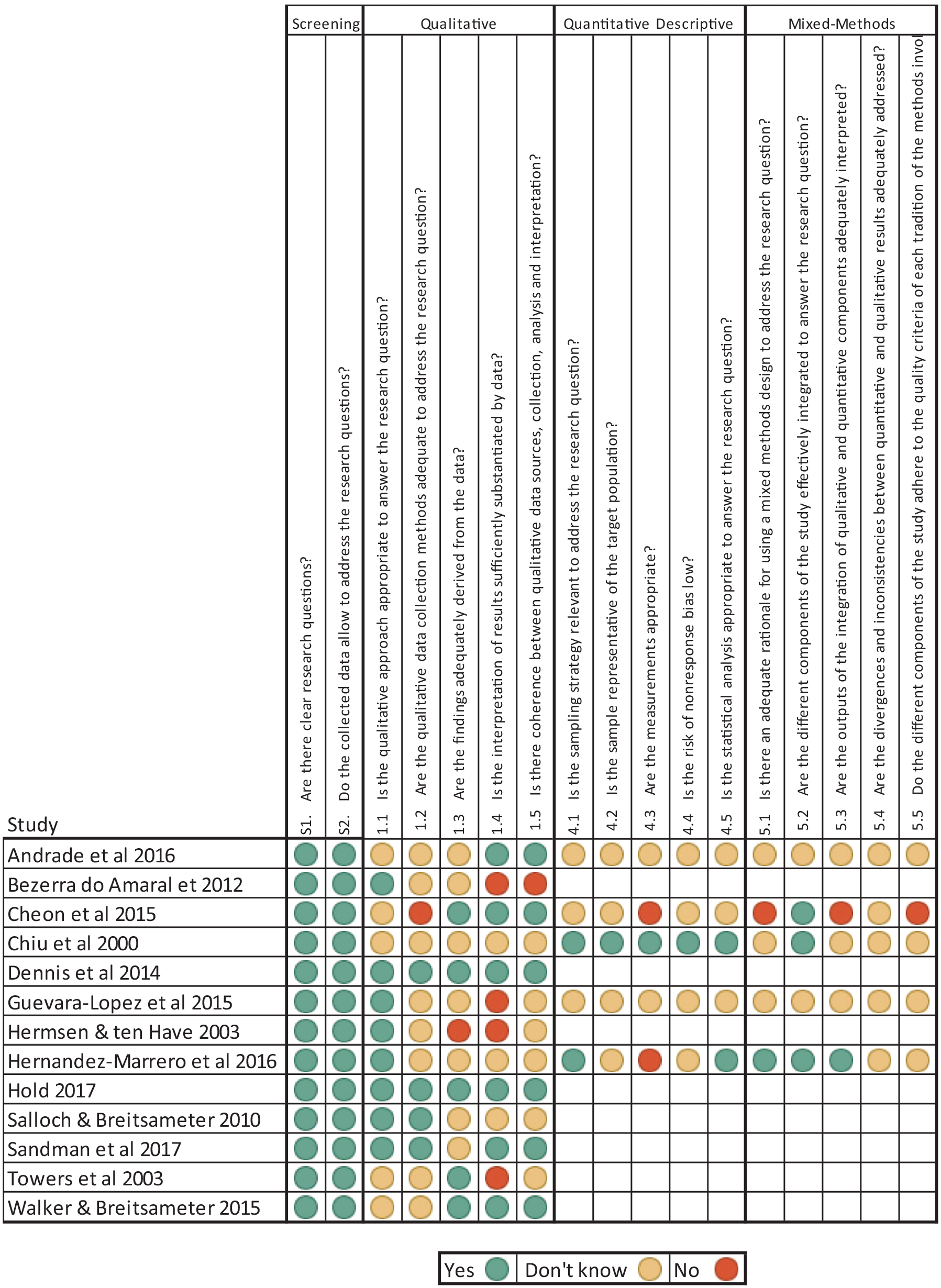
MMAT evaluations for included studies.
Findings quality assessment
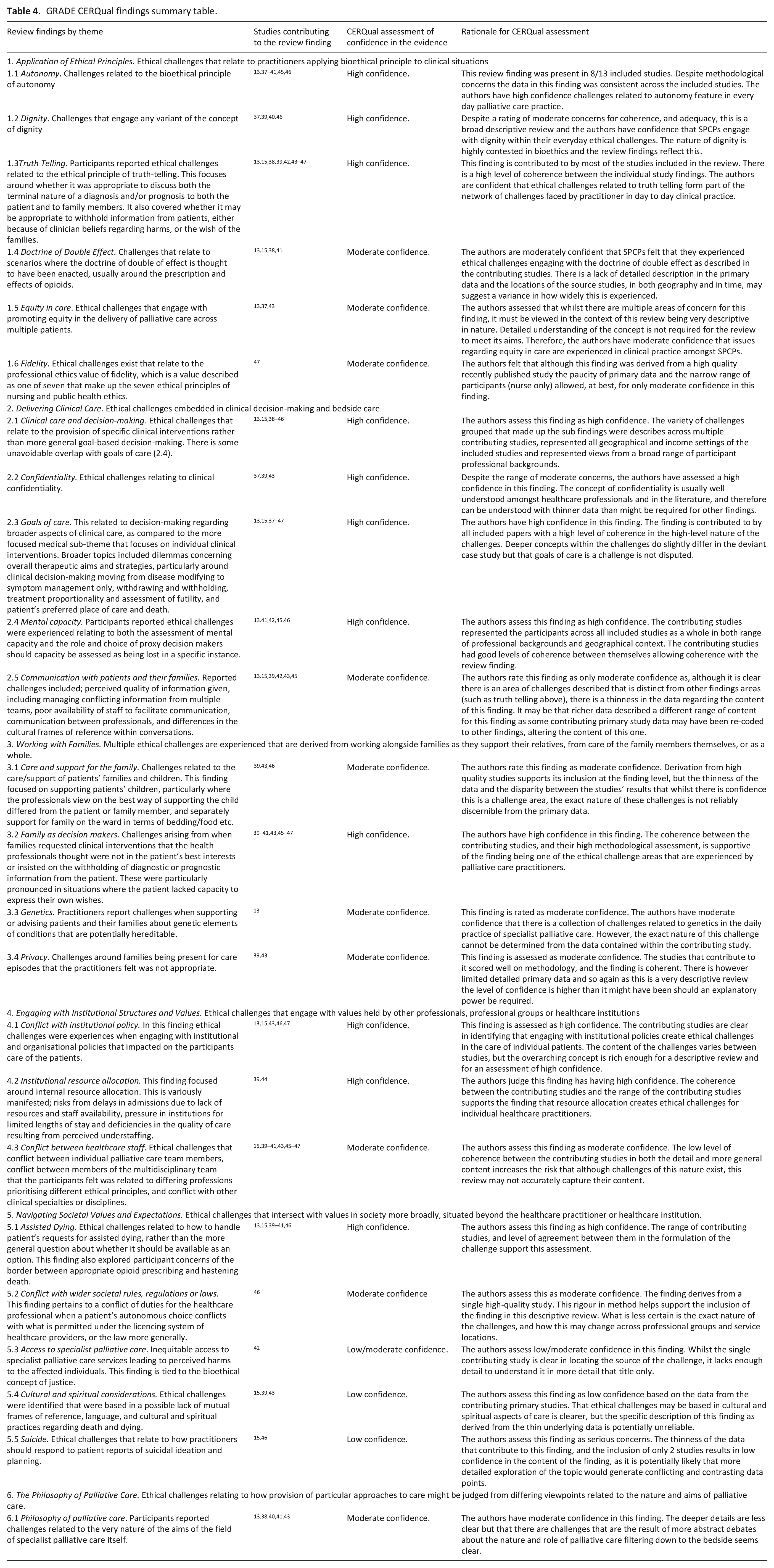
Summary GRADE-CERQual review findings are presented in Table 4. For all findings, all contributing studies were assessed as directly relevant using GRADE-CERQual guidance on assessing relevance. 44 Therefore, we used the same approach used in other GRADE-CERQual assessment areas35,48–50 to assess bias towards particular geographical location, professional background or timeframe. The GRADE-CERQual assessments suggest that reasonable confidence can be taken that the ethical challenges we identified exist in day-to-day practice. For the full assessment table, see Supplemental File 2.
GRADE CERQual findings summary table.
Themes
The ethical challenges reported in the included studies were organised into six major themes with sub-themes (Table 4): the application of ethical principles; delivering clinical care; working with families; engaging with institutional structures and values; navigating societal values and expectations; and the philosophy of palliative care.
Overall, ethics was felt to be a major feature of participants’ roles, adding difficulty and complexity.
‘Again and again, it’s morals and ethics that make things so difficult. It’s not the job. It’s those two packages that can sometimes be quite a burden’ (Nurse, Germany, p590)
40
Challenges were widely distributed across the included studies with relation to geography, professional background and publication date. There were very few differences in the patterns of challenges across differing country settings. An exception is that ethical challenges focusing on use of alternative medicine were reported only in a study from Taiwan, where there are high rates of patient use of traditional Chinese medicine. 44 Comparison of challenges between different professional backgrounds demonstrates only a few unique challenges. In one study physicians identified ethical challenges in clinical decision-making regarding antibiotics prescribing and fluid replacement. 15 Engaging with the principle of fidelity was identified only in one nursing study. 47 Conflict with wider societal regulations and professional licensing was documented only in a Canadian study that focused on social worker experiences. 46
Application of ethical principles
Findings in this theme relate to practitioners’ reflections on established bioethics principles within their clinical work. Sub-themes were autonomy; dignity; truth-telling; doctrine of double effect; equity in care and fidelity.
Autonomy
This finding was reported by 8/13 studies.13,37–41,45,46 Participants reported multiple related challenges: how best to support patients in making autonomous decisions and protect patients from coercive influences including from family members, how to respond when patients made decisions that the practitioner judged would increase harm/risk to the patient41,46 or to others 41 or that conflicted with professional judgement of what was in their best interests and therefore beneficence,40,41,46 or with the personal values of the staff caring for them.40,46,47
‘I am responsible for the person who entrusts himself to me, and I need to understand his wishes. That doesn’t mean that I think everything is right, but that’s my problem.’ (Nurse, Germany, p323)
41
Dignity
Dignity was a focus of challenges in three studies.37,40,46 For some participants dignity was tied to patient autonomy and the challenges of respecting it,37,40,46 with one participant describing it in terms of patients’ rights to choose riskier options, ‘the dignity of risk’ (Social Worker, USA, p957) 46 Participants in two studies felt that dignity was also related to empathetic and equitable terminal care and not leaving patients alone at the end of life.37,40 In a German study, participants described how euthanasia was directly opposed to a death with dignity, and felt that patient dignity was supported by organisational and practitioner opposition to the provision of euthanasia. 40
Truth-telling
Challenges related to truth-telling were reported in 10/13 studies.13,15,38,39,42–47 Challenges related to a patient’s diagnosis,15,38 or prognosis, particularly if this was judged to be short,38,39,44,46 and occurred when either practitioners or families decided whether it was appropriate to inform a patient or to withhold this information. Participants in several studies identified the conflict with patient autonomy in the case of withheld information.13,38,42,45,46 Other dilemmas involved probity or veracity, describing administration of covert medication, 46 or the inclusion of misleading information on medication requisitions to alter whether the patient, hospice or insurance company paid for them. 47
‘We have had several families who don’t want the patient to know the diagnosis, the prognosis, or that they are in hospice’. (Nurse, USA, p10)
45
Doctrine of double effect
4/13 included studies13,15,38,41 reported ethical challenges related to the administration of medication to relieve symptoms and participants’ concern that this may shorten life.
‘There was one patient who was in a lot of pain and had morphine prescribed . . . [and] administered and the patient went (. . .), the blood pressure was inaudible, and slowly the patient deceased’ (Nurse, Brazil, p20).
38
Equity in care
This finding derives from three studies.13,37,43 Participants encountered challenges when trying to treat patients equitably, with ‘fair treatment’ and without discrimination and with respect to their rights. 37
‘Do not discriminate against the patient at any time, always seek to provide an equal service’ (Nurse, Brazil, p4926)
37
Two studies identified found that clinicians’ judgements of a patient’s behaviour as ‘good’ or ‘bad’ could affect equity in care and judgements of this nature were felt to be ‘problematic,’ impacting practitioners’ relationships with patients.13,43 In a Dutch ethnographic study the observer describes a patient that regularly ‘flies into a rage’ and uses abusive language and how because of this the nurses have trouble feeling ‘sympathy’ for the patient and her situation (p268). 13
Fidelity
Fidelity refers to the value of remaining true to a profession’s values and focus on the patient. Nurses in the USA-based contributing study reported that this principle is challenged when other stakeholders interfere with the nurses’ commitment to patients. 47
Delivering clinical care
Findings in this theme focused on dilemmas surrounding the provision of patient care, including clinical decision-making. Five sub-themes were identified: clinical care and decision-making; communicating with patients and families; confidentiality; goals of care; and mental capacity.
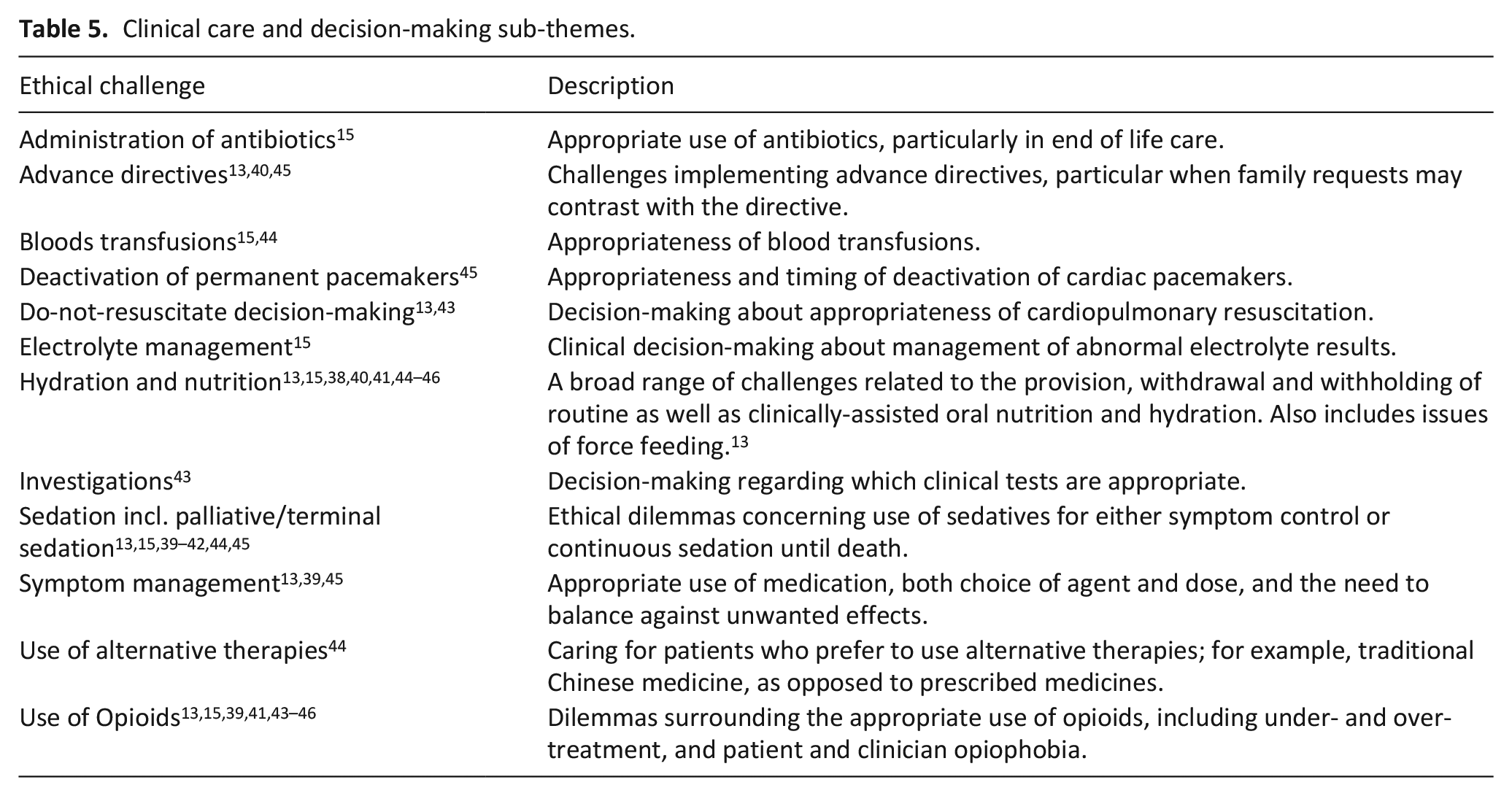
Clinical care and decision-making
This sub-theme relates to specific clinical interventions or decisions (Table 5), some of which overlap with challenges reported in Goals of care.
Clinical care and decision-making sub-themes.
Confidentiality
3/13 included studies described challenges relating to confidentiality of information.37,39,43 All three studies reported participants’ belief in the importance of maintaining patient confidentiality, particularly in respect to loved ones. 43
‘During my assistance, I preserve patient privacy and maintain the confidentiality of the information I know about him [. . .] they are essential for the humanization of care’. (Nurse, Brazil, p4926).
37
Goals of care
All 13 studies reported ethical challenges relating to broader clinical considerations such as dilemmas concerning: withdrawing and withholding clinical interventions in the terminal phase39–41,45; patients’ preferred place of care and death42,44; overall therapeutic aims and strategies 44 – particularly moving from disease-modifying to symptom-management-focused care; and treatment proportionality alongside assessments of futility.13,15,37,38,40,43,45,47 These challenges arose from practitioner interaction with multiple actors: patients, families, palliative care colleagues and external clinicians.13,15,37,40,43,45,47 A particular subset of these challenges related to treatment decisions or requests which were in conflict with expressed patient views. 45 For example, in a German study the nurse participants viewed decision-making as to whether a patient should receive active life-prolonging therapy or more traditional palliative treatment as a ‘central ethical problem’. 43
Mental capacity
In 5/13 studies, participants detailed ethical challenges concerned with the assessment of mental capacity and/or the role and choice of proxy decision makers for patients lacking decision-making capacity.13,41,42,45,46 For example, the authors of a USA study detailed challenges related to nurses identifying who was the correct person to be involved in decision-making and how to handle family conflict. 45
Communicating with patients and families
Communication challenges were reported in 6/13 studies13,15,39,42,43,45 and included: inadequate quality of patient information (as perceived by practitioners), poor availability of staff to facilitate communication, 39 poor inter-professional communication, 39 differences in the cultural frames of reference within conversations, 43 and managing conflicting information from and between multiple teams. 45
‘The provider offers unrealistic goals at the end of life, and continues treatment, often saying it is the family’s wishes, when the family does not have all of the information to make a realistic choice.’ (Nurse, USA, p9)
45
Working with families
In multiple studies, participants described ethical challenges derived from caring for the family and/or family involvement in patient care.13,37,39–41,43,45–47 Findings are in four sub-themes: care and support for the family; family as decision makers; genetics; and privacy.
Care and support of the family
In 3/13 studies39,43,46 participants reported challenges related to the care and support of the family. This included when adult patients do not want their illness discussed with their children
46
:
‘A lot of times, parents won’t let us talk about [dying] with [children]. We can’t mention that word. . . But the kids are ready to talk about it. They need to talk about it. But a lot of times parents aren’t ready for that.’ (Social worker, USA, p956).
46
Another challenge related to negotiating conflict between a family’s and patient’s wishes or support needs when it is not possible to satisfy both. Participants described how the patient must come first. 39 A further challenge related to practicalities such as provision of overnight camp beds or food for families, and alongside this, which staff members’ responsibility it is to address these. 43
Families as decision makers
Ethical challenges related to families’ role in decision-making were reported in 7/13 studies.39–41,43,45–47 Most participants detailed challenges arising from families requesting clinical interventions that health professionals thought were not in the patient’s best interests,41,43,45–47 or insisting on withholding diagnostic or prognostic information from the patient, 45 particularly in situations where the patient lacked capacity to express their own wishes.45–47 Participants highlighted additional challenges of balancing supporting the family with responding to unrealistic demands, and prioritising the patient where disagreements occurred.39,41,43,45–47
‘Patients are sometimes very passive, so the family decides for the patient. Or the patient agrees with the family just to please them. Our priority is the patient but we have to deal with the family also. If we get to the point they don’t agree, it’s the patient first.’ (Nurse, Canada, p1629)
39
Genetics
In one study participants described the challenge of how to advise and support patients and families regarding genetic testing for conditions with an inheritable component. 14
Privacy
In two studies39,43 participants reported concerns regarding the potential lack of privacy when families are involved in the care of patients.
‘Maybe you don’t want the loved ones to be present in all situation [i.e. in caring for the patient’s intimate hygiene] . . . he also took pictures of some wounds . . .’ (Nurse, Sweden, p145)
43
Engaging with institutional structures and values
Data in this theme related to institution-level decision-making or context, covering three sub-themes: conflict between healthcare professionals; conflict with institutional policies; and institutional resource allocation.
Conflict with institutional policies
Ethical challenges were experienced engaging with institutional policies that impacted on patient care, as found in 5/13 studies.13,15,43,46,47 Examples included: institutional policies prohibiting euthanasia in a jurisdiction where it is permitted 13 ; medication availability and gaps in formularies 47 ; gaps in insurance coverage preventing optimal management 47 ; and routine do-not-attempt-resuscitation orders rather than individual decision-making. 43
‘And sometimes, I get resistance from the company that I work for because it (the medication) is not in the formulary. So the ethic part comes in: Who am I supposed to be taking care of? The patient? Or the bottom line of my company that I work for? And it’s very difficult. And there have been many times when I’ve been so vocal about it that I’ve actually gotten in trouble from the company, not from my families.’ (Nurse, USA, p13)
47
Institutional resource allocation
Participants in 2/13 studies39,44 reported challenges related to institutional resource allocation, including: risks from delays in admissions due to lack of resources and staff availability, 39 pressure to discharge due to policies limiting lengths of stay, 44 and deficiencies in care quality due to perceived understaffing.39,44
‘There are many patients here who just want to go home to die, but they cannot get the resources they need, so they are stuck here for their last days. They are frustrated about being here and they have trouble feeling dignified with all that is going on around them’ (Psychologist, Canada, p1629).
39
Conflict between healthcare professionals
8/13 studies15,39–41,43,45–47 described the challenges of managing conflicting views between individual palliative care team members,15,40,41,46 other members of the multidisciplinary team, 46 and other clinical specialties or disciplines.39,43,47 Conflicts were often described in terms of different individuals or professions prioritising different ethical principles. 46
‘After a discharge had been developed and approved by the primary care provider and patient/family, a specialist walking into the room and told the patient that he preferred another plan and offered dialysis’ (Nurse, USA, p9)
45
Navigating societal expectations and values
Ethical challenges within this theme relate to broader societal or cultural values, legal and regulatory frameworks, and political landscapes that impact on day-to-day work.
Assisted dying
Participants in 6/13 studies13,15,39–41,46 described ethical challenges related to how to handle patients’ requests for assisted dying.13,15,40,46 In a Dutch study, staff reported that hospices’ opposition to euthanasia was a challenge, as euthanasia was available in other care settings.
13
Institutions not performing assisted dying also was described as helping protect SPCPs from an ethical dilemma:
‘You know, there’s a lot of people who . . . think [assisted suicide] is perfectly fine . . . personally I don’t agree with [assisted suicide]. So, to me, that presents a dilemma. I mean, I’m off the hook because, of course, we don’t do that. . .’ (Social Worker, USA, p963)
46
Participants in one German study were concerned about when opiate prescribing might be considered to overlap with ‘active assisted dying’. 41
Conflict with wider societal rules, regulations or laws
This sub-theme arose in one study, 46 in which practitioners described a conflict of duties for the healthcare professional when a patient’s autonomous choice conflicted with what is permitted under the licencing system of healthcare providers, or the law more generally.
‘Any place [other than the hospice residence], we might be able to let a person do [whatever they want] but, because we’re licensed and we have under law assumed responsibility for the care and safety of these people, our responsibility has to supersede what the patient really wants to do.’ (Social worker, USA, p960)
46
Access to specialist palliative care services
Lack of equity of access to palliative care services created ethical challenges for participants in one study. 42
‘the fairness of the system . . . many patients simply can’t afford being cared for by a specialized palliative care team such as ours because they don’t have the money to pay for it.’ (Nurse, Portugal, p726)
42
Cultural and spiritual considerations
3/13 studies15,39,43 identified ethical challenges related to culture and spirituality. In a Swedish nursing study participants described these challenges as relating to a lack of mutual frames of reference or language which could affect the staff/patient relationship. 43 The other two study reports did not provide details of the particular nature of the challenges.
Suicide
In two studies participants described challenges when patients reported suicidal ideation and planning.15,46
‘I have had patients that have told me that they have a suicide plan, and my response is [to say] “Stop talking unless you want me to file whatever I have to file and make you stop.”’ (Social worker, USA, p963)
46
Philosophy of palliative care
Challenges in this theme, which arose in 5/13 studies, related to practitioners grappling with the principles and aims of specialist palliative care.13,38,40,41,43 While these principles were not described in detail, participants described concerns about whether planned activities of care (such as life-prolonging treatment) 43 were appropriate in palliative care.41,43
‘Is it simply against the guiding principles of palliative care if I don’t only give him liquids now, but solids too?’ (Nurse, Germany, p326)
41
‘. . .but when you come in the morning and there you find, like, 10 bowls of blood samples . . . what is this. . . is this the ER? We want it to be a palliative care ward.’ (Nurse, Sweden, p144)
43
Nurses in a Brazilian study expressed views about the remit and goals of palliative care that were notably different to the mainstream understanding of the field, for example:
‘The patient does not need to know that he/she has a terminal illness, does not need to know that he/she has only a few days to live, does not need to know that there is no cure for his/her illness, does not need to know any of this.’ (Nurse, Brazil, p19)
38
A broader ethical challenge in this sub-theme relates to the position specialist palliative care should take in relation to euthanasia and/or physician assisted suicide. Participants in Germany felt that opposition to these practices is important to maintain patient dignity, perceived as a key focus of palliative care. 40 Dutch participants described a challenge occurring when patients make a request for euthanasia in the hospice as it is available in other care settings but not there. 13 No study contained data supporting euthanasia within palliative care.
Discussion
Main findings
This review is the first systematic synthesis of the ethical challenges that specialist palliative care practitioners report encountering in their everyday clinical practice. We identified 13 studies from nine countries, and a wide range of ethical challenges across six main themes with 23 sub-themes. To the authors’ knowledge there are no similar systematic reviews in palliative care or other clinical fields, and therefore direct comparison is not possible.
Our findings have important implications for palliative care education. As educational curricula are not often publicly available, we examined the contents of specialty textbooks to understand the ethical challenges usually covered in palliative care ethics teaching. The breadth of the challenges we identified is striking: our findings are broader than those contained within the ethics chapters or sections in the ‘ethics’ sections of major palliative care textbooks (see Supplemental File 3 for a list of chapter titles).51–55 This reflects the findings of Hermsen and ten Have’s13,14 project examining this discordance. All topics in these textbooks are represented in the synthesis but not vice versa. The breadth of topics is also broader than the United Kingdom specialist palliative medicine physician training curricula. 56
Hermsen and ten Have were the only researchers to use a bioethicist to observe workplace challenges. Although we have only included in the review the 31 challenges that were reported by practitioners within a hospice setting, across their full study they identified a total of 35 challenges across five research settings, far more than any other of the studies included in this review. 13 It may be that the bioethicist observer identified scenarios as containing ethical challenges where a clinical practitioner might not have. This raises the possibility that not all of these challenges impact clinical care, or alternatively, that practitioners lack the training to recognise the full range of ethical challenges in the workplace. If ethical challenges are observer dependent, relying on practitioners’ viewpoints alone means certain challenges will be lost. As a consequence, there may be ethical challenges that are important to patients and carers but are missed by practitioners. A study of patients and carers in a single palliative care service in the UK illustrates this concern, describing the ethics of hope as a major finding, which is missing from these review findings. 57 Further research is needed that focusses on patient and carer experiences of ethical challenges and triangulates the perspectives of specialist palliative care practitioners, ethicists, patients and carers.
We found ethical issues related to the philosophy of palliative care and whether certain clinical activities were appropriate in palliative care. While this is perhaps not surprising in a relatively young field, these findings reiterate how the demarcation and definition of specialist palliative care can differ between settings/contexts and over time. This is reflected in ongoing debates surrounding the definitions of palliative care58–63 and the shift to integrate palliative care alongside curative treatment. 58
That participants expressed concern that opioids may shorten life in larger doses is also interesting. There is good evidence that appropriately titrated opioids do not shorten life.64–66 This finding highlights the ongoing challenge of promoting safe prescribing and the safety of opioids more generally, among colleagues, patients, and the public more broadly.
None of the studies we identified were undertaken in a low or low/middle-income setting. 10/13 were undertaken in high income countries,13,39–41,43–47 and 3/13 in two upper-middle-income countries, Brazil,37,38 and Mexico. 15 This represents a significant evidence gap as 6.38 billion people live in low or low-middle-income countries 67 and there may be specific ethical challenges that practitioners caring for patients in these settings face that are not represented within our findings. This concern is supported by the findings of a recent non-systematic review on the experiences of patients from non-Western and minority cultural backgrounds when using hospice and palliative care services, which highlighted multiple findings with clear normative elements that were prominent in low-income settings. 68 Cultural differences across geographical locations have also been shown to impact on physicians’ experiences of ethical challenges. 69 Although we did identify some challenges related to cultural and spiritual aspects of care, it is perhaps unexpected that these topics were so infrequently represented.
The findings of this review have clear implications for ethics support services and palliative care training. We identified challenges that were predominantly related to specific scenarios or contexts rather than the general application of broader ethical principle frameworks. This finding of a context-focus is in line with systematic reviews examining ethics within dementia care70,71 and nursing, 72 as well as individual studies in general practice, 11 community pharmacy, 73 Canadian hospitals, 74 renal medicine, 12 pain medicine 10 and generalist end of life care.75–79 The focus on detail has been termed ‘microethics’, and proponents argue that this is the level at which most ethically challenging decision-making occurs. 80 This contextual structure is important when considering how to support and manage ethical decision-making in the healthcare environment. Practitioners are often taught to analyse case-based scenarios using principle-based frameworks such as Beauchamp & Childress’ ‘Four Principles’ approach.80,81 However, our findings support the use of alternative approaches which explicitly consider context-based facts, such as the Seedhouse grid, 82 or the Four Quadrants approach. 83 In addition, outcome-based ethical assessment frameworks such as utilitarianism, virtue ethics, and ethics of care,84–87 more easily incorporate individual context than do a priori, rule-based, deontological frameworks.
Finally, only a relatively small proportion of the challenges reported by participants related directly to clinical decision-making about individual patients. Challenges were located across the care environment, from the bedside through institutional and societal values to national-level policy. Those wishing to engage with ethics within palliative care when aiming to improve care at the bedside must therefore acknowledge the impact of these multiple levels. This has relevance to palliative care ethics education, which often relies on patient case-based teaching.80,88 Care must be taken in the writing of cases to include themes that are located away from the bedside.
Strength and limitations
Strengths in the design of the review include its systematic approach; lack of language, geographical, or date restrictions in the search protocol; the inclusion of LILACS to better capture non-English language research; and quality assessment of both included studies and review findings. However, study design decisions are also associated with potential limitations. First, the search strategy used methodological filters. Pilot filtered searches were evaluated for study loss using pre-identified sentinel studies; all were returned by the search strategy. However, it remains possible that relevant studies were missed due to misclassification in the registry or novel methodology. Second, searching in English only might also mean that relevant articles not published in English and indexed only in non-English databases were missed.
Third, the contributing studies often did not contain detailed description of the nature of the ethical challenges reported. Our review is similar to other broader healthcare ethical challenge reviews in that in depth analysis of every challenge was not possible. 89 Two papers with lower MMAT scores reported a small number of ethical challenges with insufficient explanatory context to accurately include them in the synthesis. These challenges were: existential suffering care, 13 unbearable suffering, 13 motivation, 13 paediatric palliative care, 13 patients feeling a burden to their families, 39 quality of care, 13 quality of life, 13 research with terminally ill patients, 13 responsibility, 13 and role as a researcher. 13
Finally, quality assessment of qualitative research and its outputs is a contested area, with multiple tools available and poor correlation between methods. 90 The MMAT contains fewer criteria to assess study quality than methodology-specific tools and may lead to an incorrect over- or under-assessment of a study’s inherent bias. However, we did not exclude studies based on their MMAT assessments and believe the ability to directly compare studies of differing methodologies was useful. The GRADE CERQual approach helps to systematise the assessment of the findings of the review but is underpinned by researcher judgement, allowing for possible mis-categorisation.
What this study adds?
This is, to our knowledge, the first review to systematically detail specialist palliative care practitioner-reported ethical challenges and has important implications for palliative care and ethics training. The identified ethical challenges are far broader than those included in current major textbooks in the field. These challenges are located at diverse levels, from the bedside up to national policy. We found no data from low and middle-income settings where the majority of the world’s population live and die. Finally, this review, through the breadth of data synthesised, demonstrates the utility of robust methodologies within empirical bioethics. That the review identified ethical challenges that are not included in the major textbooks reinforces the need for this approach alongside theoretical aspects of bioethics, if the aim is more ethically-informed clinical care.
Further research is needed to explore patients and carers’ perspectives, the nature of the individual challenges identified in this review, and how these may vary across settings and countries.
Supplemental Material
sj-pdf-1-pmj-10.1177_0269216320974277 – Supplemental material for Real-world ethics in palliative care: A systematic review of the ethical challenges reported by specialist palliative care practitioners in their clinical practice
Supplemental material, sj-pdf-1-pmj-10.1177_0269216320974277 for Real-world ethics in palliative care: A systematic review of the ethical challenges reported by specialist palliative care practitioners in their clinical practice by Guy Schofield, Mariana Dittborn, Richard Huxtable, Emer Brangan and Lucy Ellen Selman in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_0269216320974277 – Supplemental material for Real-world ethics in palliative care: A systematic review of the ethical challenges reported by specialist palliative care practitioners in their clinical practice
Supplemental material, sj-pdf-2-pmj-10.1177_0269216320974277 for Real-world ethics in palliative care: A systematic review of the ethical challenges reported by specialist palliative care practitioners in their clinical practice by Guy Schofield, Mariana Dittborn, Richard Huxtable, Emer Brangan and Lucy Ellen Selman in Palliative Medicine
Supplemental Material
sj-docx-3-pmj-10.1177_0269216320974277 – Supplemental material for Real-world ethics in palliative care: A systematic review of the ethical challenges reported by specialist palliative care practitioners in their clinical practice
Supplemental material, sj-docx-3-pmj-10.1177_0269216320974277 for Real-world ethics in palliative care: A systematic review of the ethical challenges reported by specialist palliative care practitioners in their clinical practice by Guy Schofield, Mariana Dittborn, Richard Huxtable, Emer Brangan and Lucy Ellen Selman in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge Alison Richards for her help developing search strategies and Dr Huey Yen Chia for her help screening the Mandarin Chinese language abstract.
Authorship
G.S. and L.S. conceived of the review; L.S., G.S., E.B. and R.H, designed the review protocol; G.S. and M.D. conducted the literature searching, screening and quality assessment, with supervision from L.S.; G.S. led on drafting the manuscript; all authors were involved in data interpretation, critically revised the manuscript for important intellectual content and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: G.S. is supported by a Wellcome Trust Research Award for Health Professionals (208129/Z/17/Z). L.S. is funded by a Career Development Fellowship from the National Institute for Health Research.
Ethics and consent
This manuscript is of a systematic review and as such no ethical approvals are required.
Data sharing
There is no additional data associated with this review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.