
Abstract
Background:
Family and friends are key providers of care for people living with a long-term neurological condition. Neurological conditions are a significant global contributor to disability and premature death. However, previous research suggests carers often struggle to access appropriate support at end of life.
Aims:
This review sought to synthesise qualitative studies discussing end-of-life and palliative issues for informal carers supporting people living with neurological conditions.
Design:
This was a meta-ethnographic synthesis of 38 qualitative studies discussing end-of-life and palliative issues for informal carers supporting people living with long-term neurological conditions.
Data Sources:
Qualitative articles published after January 2010 in English, addressing carers of people with long-term neurological conditions with regard to palliative care, end of life and/or bereavement. Papers were excluded if it was not possible to separately assess the views of carers. Quality appraisal was not undertaken, but consideration was given to research context.
Results:
Across the papers, five key themes were identified: the future (un)certainties in the progression of life-limiting neurological conditions; an information paradox of not receiving the right information at the right time; access to support; carers’ roles in decision making around end of life; and maintaining continuity while facing change and disruption in day-to-day living.
Conclusions:
Given the broad agreement on the challenges faced by carers of people living with long-term neurological conditions, future research should consider opportunities to improve information and support for this group, and the development and evaluation of practical models of service delivery.
Neurological conditions are a significant global contributor to disability and premature death
Carers face particular challenges regarding the uncertainty of conditions and difficulty in accessing support
The review identifies key themes in the existing literature relating to future (un)certainties; information paradox; access to support; decision making; and continuity, change and disruption.
There is a need for better communication about the role of palliative care.
Given the relatively clear narrative regarding existing challenges and barriers, future research should address practical approaches to improving services, including models for service delivery.
Introduction
Neurological conditions are the leading global contributor to Disability Adjusted Life Years (DALY), a measure of the impact of disease on life expectancy and years spent living with disability. 1 In the UK, neurological conditions account for 20% of acute hospital admissions and are the third most common reason for people to access primary care. 2
Research suggests that family carers of people with life-limiting neurological conditions face a number of distinct challenges linked to the long-term nature of the conditions, the physical, cognitive and behavioural challenges, and the consequent care requirements.3,4 Caring for a person with neurological conditions may be made additionally complex by factors such as other co-existing conditions, broader social inequalities, individual illness experience, and the degree of access to formal and informal support.3,5–7 Carers of people living with long-term neurological conditions are likely to experience caregiving as intensive or ‘relentless’ and may be critical of services where they feel that the emotional implications of caring for someone who will die of their condition are not properly recognised or supported.8–10 Specific challenges have been associated with end of life care for people with neurological conditions and their carers and families, including living with complex conditions and uncertain disease trajectories, the lack of a distinct dying phase for some conditions and poor access to palliative care services. 11
Given that long-term neurological conditions are characterised by change and deterioration, people living with such conditions and their families engage with multiple health and care service systems. Responsive, easy to navigate services, combined with clear information and advice, are important markers of quality. However, health and social care practitioners may find it difficult to practice confidently for a variety of reasons, including the challenges of developing the skill and knowledge base required to respond to complex conditions that may only be seen infrequently.12–14 There are a number of pre-existing qualitative studies addressing challenges faced by informal carers of people with neurological conditions. Many of these studies address end-of-life care, but are usually disease- and/or setting-specific and often consider end-of-life care conjunction with other issues affecting carers. This review set out to synthesise the findings of these prior qualitative studies, in order to examine common themes regarding carers’ experiences and perceptions of end-of-life with a long-term neurological condition.
Methods
In line with institutional procedures, the [Institution Name] Ethics Committee was notified that this review was taking place on 7th March 2019.
Meta-ethnography is a systematic approach to the interpretative synthesis of qualitative evidence.15–17 Rather than seeking solely to summarise studies, meta-ethnography seeks to translate the findings from studies into each other, in order to build upon the qualitative characteristics of the original studies and to generate new theoretical knowledge. Meta-ethnography was chosen as an approach that would preserve the qualitative character of the original studies exploring end-of-life care. Noblit and Hare set out seven steps for meta-ethnography, which this study followed:
1. Getting started: The original idea for the study arose from an earlier local research project to explore neurological needs, which identified that carers and family members of people with long-term neurological conditions experienced challenges around end of life. [REFERENCE OMITTED FOR PEER REVIEW]. This study therefore set out to review the experiences and perceptions of informal carers of adults living with long-term neurological conditions regarding end of life.
2. Deciding what is relevant to the initial interest: The study sought to include all recent qualitative studies relating to informal carers’ experiences of end-of-life for adults with a long-term neurological condition. In devising a search strategy, the authors were conscious that there are several hundred neurological conditions, some of which are unlikely to be discussed in an end of life context (e.g. migraine). The search strategy therefore incorporated both the generic term ‘neurological’, and the names of specific long-term conditions where the previous research project suggested that there was existing palliative care literature. Papers focused on primary dementia (e.g. Alzheimers) were excluded on the basis that dementia is the subject of a relatively large, distinct body of caregiving literature.
In order to get a range of literature from medical, health and social science perspectives, the following databases were searched: Academic Search Complete, Allied and Complementary Medicine Database, Applied Social Sciences Index and abstracts, CINAHL Complete, MEDLINE, PsycINFO, Scopus, Soc Index, Web of Science. The search was initially carried out in November 2018, and updated June 2020.
The search was an abstract search for the following search strings, adapted as appropriate to the search engines for each database.
Search String 1: carer or caregiver
Search String 2: Neurological or Parkinsons or Stroke or Multiple Sclerosis or Huntington’s Disease or Motor Neurone Disease or Amyotrophic Lateral Sclerosis or Traumatic Brain Injury or Post-Polio Syndrome or Muscular Dystrophy or Multiple System Atrophy
Search string 3: End of life or palliative or bereavement or dying or death or hospice
Limiter applied within the database: Published after 1 January 2010.
Inclusion criteria were that papers were English language, published since 2010, and based upon qualitative data collection and analysis from informal carers of adults living with neurological conditions. All or part of the research findings/analysis were required to address carers’ experiences or perspectives related to end of life, palliative care, dying and/or bereavement. Papers were excluded if they did not address carers’ perspectives; related solely to carers of children or of people with dementia; or if in- and out-of-scope material was grouped together in a way that did not allow for separate analysis (Table 1).
PRISMA flowchart.
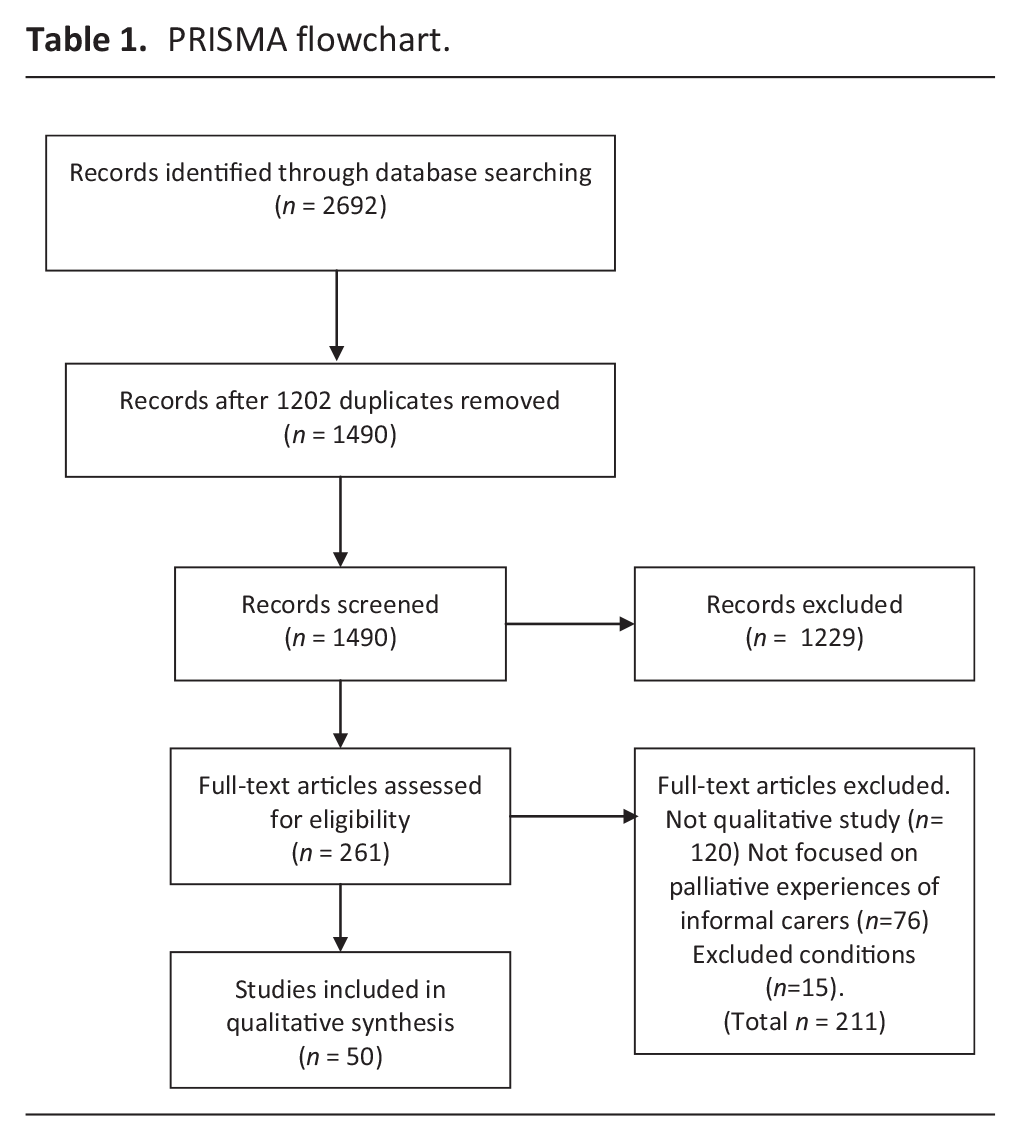
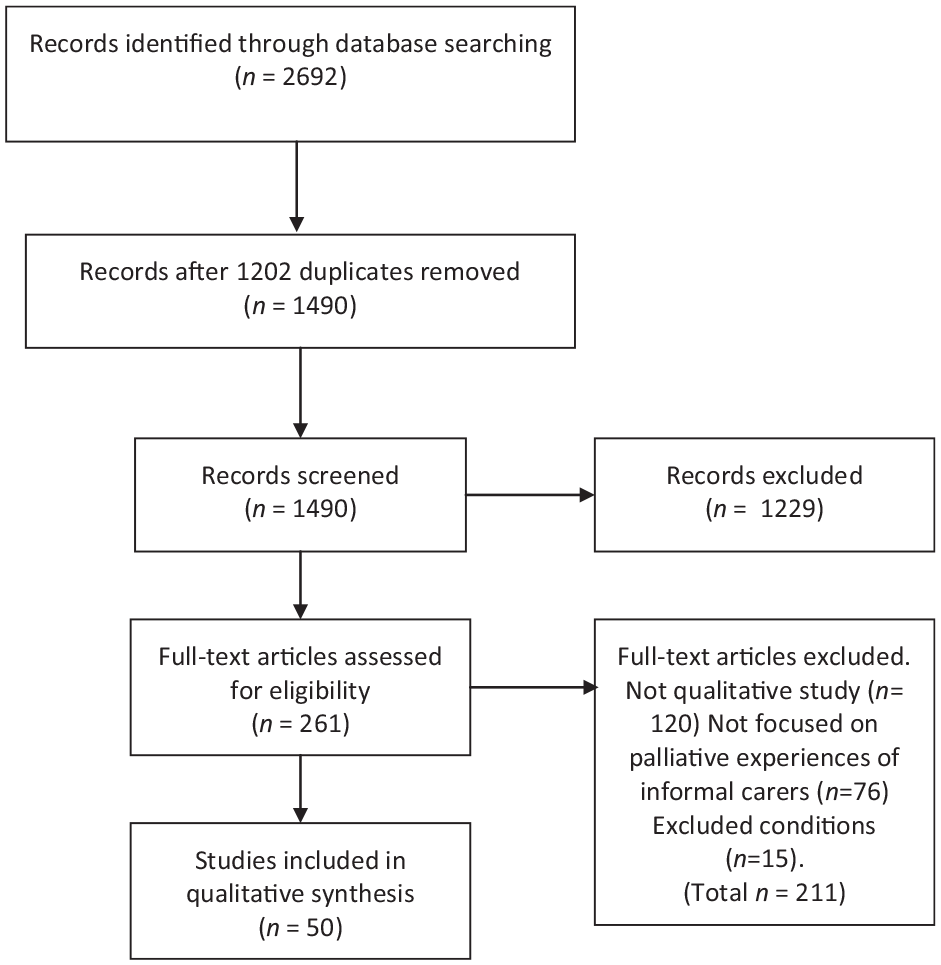
Abstract screening was undertaken by MT, with a random sample of 10% independently screened by MR to ensure inter-rater reliability. In line with other meta-ethnographic studies, it was often unclear at abstract screening whether papers met the inclusion criteria. 17 On full-text screening, a relatively high proportion ultimately proved to either not be qualitative research, or to not be focused upon the perspective of carers, and were excluded. Where papers included reference to carers’ perspectives on end-of-life, but this was not the sole focus of the paper, both authors discussed and agreed whether there was sufficient relevant material to include. Where there was more than one paper from the same study or sample, all were included, as they often addressed different aspects of end-of-life. However, this was considered in the analysis stages to avoid giving undue weight to multiple papers from the same study.
An assessment of study quality was not undertaken in deciding which studies to include or exclude. There are differing perspectives on the value of quality assessment in meta-ethnography, and even where quality assessment is used, reviewers do not necessarily exclude low-scored studies.17–19 Quality assessment of published qualitative research may be affected by discipline and journal, and may tend to be affected by word count limitations.17,20 Methodology and conceptual framing may ultimately be more relevant than quality in attempting to translate and synthesise studies. 17 In the latter stages of synthesis, we aimed to reflexively and rigorously consider the different methodologies and focus, and the possible consequences for our analysis
3. Reading the studies: Both authors read and re-read the selected articles to familiarise ourselves with the research studies’ context and focus, and their conclusions about carers’ experiences of end of life. Basic data about study design, setting and sample was extracted into a Table 2.
4. Determining how the studies are related. Initially, both authors independently read papers and identified key themes and supporting evidence. This was done through close repeated reading of the entire paper. We used a grid to extract the key themes developed by the original author(s), example quotations from study participants (if present), and our own reflective notes on the papers.
5. Translating the studies into one another. The authors discussed our analyses between ourselves and inductively identified what we considered to be the key overarching themes, through grouping related concepts extracted from the papers, with repeated reference back to the original text to ensure that meaning was not lost, and that core themes identified by the original study authors were captured in our over-arching themes.
List of included studies.

Because some papers were not solely focused upon carers and end-of-life, some themes identified within the papers were excluded from this review, such as those solely relating to patient or practitioner experiences. Other studies addressed the overall experience of caring, from pre-diagnosis to death. In studies of care for life-limiting illness, it is difficult, and perhaps somewhat artificial, to wholly distinguish between end-of-life and the broader context of care. However, upon discussion, and in order to preserve the focus on end-of-life, we decided to exclude analysis that seemed to be predominantly focused upon more general experiences of being a carer (e.g. financial strain), rather than upon anticipating or experiencing end of life.
6. Synthesising the translations. Noblit and Hare suggest that studies that are on very closely related topics may reciprocate or refute each other, while studies that do not overlap so closely may point to an overall ‘line of argument’ addressing a bigger picture than the individual studies address directly. 15 While few papers featured all of the five themes identified, across the spread of papers there appeared to be a largely consistent line of argument as to what it was to be a carer of a person with a neurological condition approaching the end of life.
7. Expressing the synthesis. This paper constitutes the expression of synthesis, and was written jointly between the two authors.
Results
Study characteristics
In total, 50 papers were included (see Table 2). However, in some cases there was more than one paper from the same data collection, and other papers utilised overlapping samples.21–23 Papers were predominantly based on data from North America, Australia or Western Europe, with participants typically recruited from hospitals, support groups and research databases. In some cases, recruitment of carers had been secondary to recruiting patient participants for other workstreams. Where relationship between carer and care recipient was specified, the majority were spouses or intimate partners. Most papers utilised semi-structured interviews.
Most papers were specific to one neurological condition, with 27 out of 50 focusing on Motor Neurone Disease/ Amyotrophic Lateral Sclerosis. This does not reflect the prevalence of conditions. Motor Neurone Disease is less prevalent and makes less of a contribution to global burden of disease than conditions such as stroke, Multiple Sclerosis and Parkinson’s, 1 suggesting that carer experiences of some common neurological conditions may be comparatively less well researched.
Five overarching themes were identified as set out at Table 3.
Key Themes.
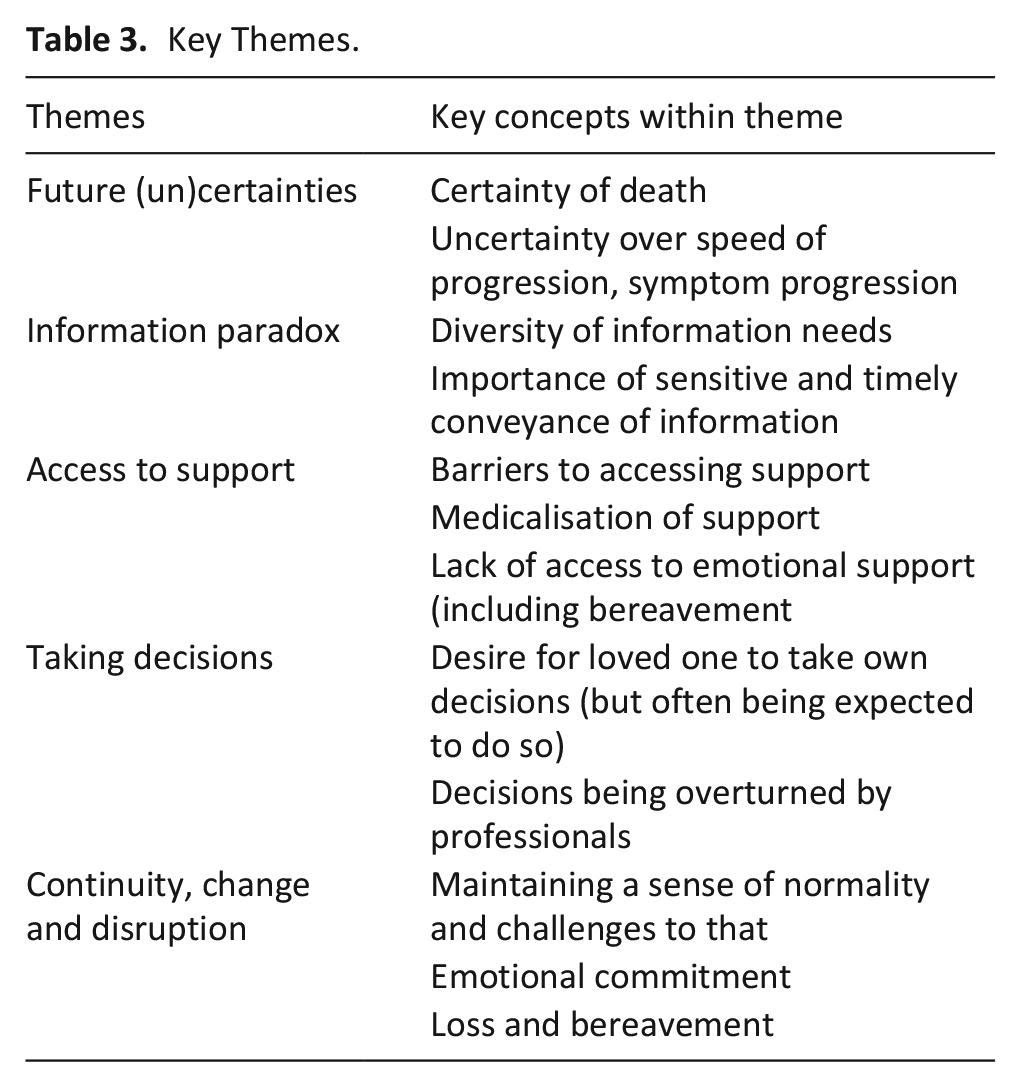
Future (un)certainties
Underpinning the accounts of informal carers were questions of certainty and uncertainty with regard to the progression and prognosis of neurological conditions and the proximity of death. Particularly within the papers focusing on Motor Neurone Disease, and advanced Multiple Sclerosis, carers were distressed and frustrated at a situation where they perceived their loved ones to have received a ‘death sentence’ (p. 290) 24 or to be ‘living in the shadow of death’ (p. 16), 6 yet simultaneously facing substantial uncertainty over when death would occur and what would happen in the meantime, resulting in a feeling of living in ‘limbo’ (p. 91).25–38 Some papers highlighted lack of certainty about the future deriving from lack of knowledge: for example, Fox reports that some carers were not aware that Parkinson’s was incurable. 7 A small number of papers reported cases where the carers and the person they cared for did not accept the certainty of death, for example, pursuing experimental treatments overseas.39,40 Among carers of people living with Huntington’s, the certainty of a degenerative life-limiting condition was seen as particularly difficult to bear, with suicide sometimes perceived as an understandable result. 41
Even within the context of a life-limiting condition, death itself was sometimes unexpected. Some papers reported that carers had anticipated a gradual decline, and were surprised by what they perceived as a sudden death.42–44 However, Veronese et al. suggested that carers often were aware from identifiable features that death was near. 45 The uncertainty entailed within neurological conditions was also sometimes contrasted to other conditions, although not consistently. Penrod used Amyotrophic Lateral Sclerosis as an example of an expected death trajectory, specifically contrasted to cancer and heart failure as mixed or unexpected death trajectories. 46 However, Gofton et al. argued that within palliative care, timelines for progression of neurological disorders are longer and more uncertain than those of oncology. 28 They highlight that uncertainty arises in several dimensions, including diagnosis, prognosis and disease trajectory, and is interrelated with inconsistency in information and support, and underlying existential distress from the situation itself.
Information paradox
While giving information to families at the time of diagnosis is crucial, studies highlighted that information-giving was inconsistent and at times inadequate.7,26,47 Carers gave examples of professionals sharing diagnosis in an insensitive manner, leading to a perception that the individual and family consequences of diagnosis were neither recognised nor addressed.7,24,34,48,49 Carer experience of poor, absent or delayed information about support services and resources resulted in feelings of isolation and additional strain.34,47,50
Despite the agreed importance of sharing information about end of life, carers reported difficulties in accessing information. At times this was due to variable practice in talking about end of life and related topics such as advanced planning and treatment options. 42 Carers were also often unsure who, from a multitude of professionals, they should approach to discuss end of life.7,23,24,50–52 Confusion about responsibility for sharing information about end of life could be exacerbated by factors such as poorly integrated services, lack of confidence amongst professionals and a lack of clarity about what had already been shared. 50
Paradoxically, some studies also highlighted risks associated with being given excessive information, such as information that was unwanted, poorly-timed, or poorly-delivered. 53 Factors such as culture, coping mechanisms and within-family relationships influence the kinds of information that families need and how they prefer it to be given.26,27 Carers have diverse information needs, which may change over time,54,55 which has significant implications for the ongoing assessment of carer information needs.
Access to support
Carers experienced a number of barriers in accessing support services and the identification of support needs was often overlooked by HCPs. Carers often experienced accessing services as longwinded or disjointed, especially when managing the process at critical points in their relative’s illness and care trajectory.7,10,48–50,52,56 The point of diagnosis was frequently cited as a moment where carers would have valued additional emotional and practical support.10,34,48,49,57 Through the course of long-term neurological conditions, families/carers consistently cited difficulties in accessing a range of support including, for example, infrequent contact with specialist clinics and opportunities for families to talk with professionals in depth;7,26,50,51 a lack of appropriate care services,23,36,56 a lack of a whole family approach to support 26 and poor access to palliative or specialist support services.5,7,26,47,50 Although specialist services were generally appreciated, as conditions progressed, carers and families sometimes felt isolated by a focus on symptom management at the expense of emotional, psychological and social support.24,51,58 Perceptions of ad hoc or poor communication meant that families were not always aware of potential support services until a crisis occurred or situations had deteriorated.23,56,59 Some families that required help found it difficult to accept help when offered or did not know what kind of support might be helpful.7,23,26,39,48,51 When family members began receiving formal care, the change in role for carers also at times caused tensions.37,52
Access to palliative care frequently occurred late in the illness trajectory.48,50,59 Poor awareness of palliative care services and frequent misperceptions that they were only for people who were dying or for people who had cancer, served as barriers to proactively accessing palliative care.7,10,50,59 If, or when, palliative care was received, carer/family member experiences were generally positive about their experience but, overall, improvements in communicating the role and purpose of palliative care combined with timely access to those services could contribute to supporting carers at a time of great stress.10,48,50,56,58 However, Aoun reported that an intervention offering dedicated support assessments for carers was welcomed. 60
The absence of bereavement support was notable, as was the experience of being suddenly cut off, following the death of their relative, from an often extensive network of health and social care professionals.10,34,48,56 Concerns for carers being overwhelmed by the stress of providing care, followed by the death of their relative, were cited as possible risk factors for complex and prolonged grief.23,48
Taking decisions
Carers’ experiences of end-of-life often involved decisions on behalf of their loved one, for example with regard to ventilation or gastrostomy, or supporting the drawing up of advanced care directives. A number of papers in this review specifically focused upon such decisions. Carers typically wished their loved one to take key decisions themselves, yet in practice this did not always occur.22,40,43,56,61 Sometimes, the progression of neurological conditions meant that the care recipient was less able to take or communicate decisions, requiring the carer to take a greater role.5,21,22 Ray highlighted that some care recipients did not want to discuss end of life. 42 In other cases, the urgency of situations overtook decisions.25,40,43,58 At times, carers were asked to overturn decisions their loved one had already made, for example to accede to a professional’s views on attempting resuscitation.34,40,42,45,58 Documentation of decision making was perceived as helpful, but carers reported an ongoing need for input to ensure that documented decisions were implemented.22,25,40,56
Some papers highlighted barriers to carers being involved in good quality decision-making. At time, uncertainties about prognosis and lack of knowledge about services and interventions meant carers and the people they cared for felt they did not have the necessary knowledge to take informed decisions.32,38,54 Some studies pointed to a need for ongoing flexibility regarding decision making, taking decisions in the moment.33,47 Young people and non-spousal carers sometimes reported exclusion from formal decision making.61,62 A move into residential care could result in a further change to decision-making roles, with the carer becoming less involved in decision making. 26
Maintaining continuity while facing change and disruption
Families, including carers, placed a high value on maintaining a sense of normality in a context where life was far from normal, they were facing unfamiliar and hard-to-predict challenges, and prior understandings of family and relationship norms were disrupted by continual change.27,33–36,47,48,53 It was important for family carers to strive to preserve significant personal, couple and family continuities wherever possible37,38,53 and to try to establish a routine in order to preserve some sense of control. 63
However, there were significant challenges for families in their efforts to preserve continuities. Taking on roles and responsibilities that had been the responsibility of the person living with the long-term neurological condition added to workload. Often, spouse/partner carers became solely responsible for all aspects of the household, representing a disruption to established roles and an additional demand on time. 63 Alternatively, formal carers or other professionals coming into the home could result in a loss of personal or family space. 64 The growing likelihood of providing complex care meant that carers’ own needs risked becoming incidental and carers often experienced guilt if they expressed or tried to realise their own needs.31,53,63 Complex care provided against a backdrop of change and uncertainty reduced the time available to retain important continuities such as hobbies, work or maintaining friendships and family relationships. 63 Extra effort was involved to engage in activities with the person with long-term neurological conditons.29,30,62 Wider family and friendship networks suffered as time, energy and the resources to invest in maintaining those relationships was compromised by the demands of providing care. 26
Commitment to the relationship and loving the person living with the condition was a key motivation for providing complex and often relentless care.29,31,37,47 A study of carers for relatives with Amyotrophic Lateral Sclerosis found that the diagnosis drew some families together but pulled others further apart – the latter occurring more frequently amongst families who avoided emotional content in their communication. 24 But inevitably, the challenges associated with caring affected relationships. Caring spouses and partners expressed feelings of existential loneliness as they felt unable to share their experiences, worries and thoughts with their spouse/partner, including how the neurological conditions was impacting on each other.5,26,31,51 Physical and emotional changes such as pain, reduced mobility, muscle weakness and low mood impacted on the extent to which the person with the condition and their partner could respond to physical closeness and intimacy which, combined with a changing role from partner/spouse to carer, affected sexual and intimate relationships.48,63 Changes in a person’s behaviour or mood could have a significant impact on partner relationships and also the wider family and friendships.26,35,49
Anticipated loss and perpetual loss was identified as the backdrop for carers of people with long-term neurological conditions,35,48,63 creating an intensely challenging situation for them both and their families. Bereavement for some carers was preceded by distressing and difficult end of life experiences44,56,64 which carried the risk of a long-lasting effect on the bereaved person. Difficult end of life experiences risked exacerbating feelings such as remorse, blame and guilt as to whether they or others could have done more. 63 Research has suggested that those spouses/partners who had difficulties accepting that their partner’s condition was terminal were more likely to subsequently have prolonged and complex grief reactions. 48 Those people who were isolated in their caring role may be more at risk of feeling abandoned or unsupported in bereavement. 10 Overall, access to bereavement support was patchy and identified as a priority area of need, especially for carers of people with conditions which have tended to be overlooked in the bereavement literature (for example, Parkinson’s Disease).10,34
Discussion
This review addressed the experiences of carers of people with long-term neurological conditions regarding end-of-life. Although papers addressed a range of different issues, the interpreted line of argument highlighted themes of: the future (un)certainties in the progression of life-limiting neurological conditions; an information paradox of both too much and too little information; access to support; carers’ roles in decision making around end of life; and maintaining continuity while facing change and disruption in day-to-day living.
There was a strong sense of ‘uncharted territory’ – long-term neurological conditions were outside the range of expected experience. As a consequence, carers struggled to balance maintaining existing continuities, within the context of an unpredictable trajectory of change and against the emotional backdrop associated with diagnosis of a long-term neurological condition. One of the inevitable limitations of carer research is that it tends to homogenise the needs of carers. This review has highlighted diversity and the variability of information needs. Not all carers wanted the same information at the same time. Carers did not always know what services were available and sometimes only realised what would have been helpful to them retrospectively, suggesting a greater need to engage with carers in order to understand and meet individual needs. Many studies highlighted carers’ frustrations at being expected to navigate services with little signposting. In other cases, support interventions may themselves have represented a significant loss of continuity – for example, accepting that gastrostomy insertion meant that the individual would not eat again, with consequent impact on family life and friends; or the emotional and relationship challenges involved in accepting respite care or domiciliary care.32,39,53,54,65
In attempting to make sense of this unfamiliar context, carers at times contrasted neurological conditions to other life-limiting diagnoses, particularly cancer. This occurred both within practical discussions of information and service provision (e.g. that palliative care was frequently perceived as being primarily for cancer care), and within conceptual discussions of disease trajectories.10,46,59 Carers appeared to perceive end-of-life with a neurological condition as being worse than other end of life experiences. It is possible that this simply reflects carers’ familiarity with neurological conditions: many carers may not have been in a position to make a true comparison with other end-of-life experiences. Nonetheless, carers perceived that the end-of-life care their loved ones was receiving was worse than it ought to be, sometimes resulting in a sense of guilt or regret. 56 Some aspects of negative comparison, such as uncertainty over prognosis and timing, are inherent to some of the neurological conditions involved. However, many of the practical points of dissatisfaction, such as poor access to services, difficulty knowing who to talk to and end of life care decisions not being respected, could be addressed by improving palliative pathways and protocols and improving access to bereavement services.
Carers often acted as an information broker, transmitting information between the person being cared for and health and social care practitioners, and this responsibility often increased as the condition deteriorated.10,21,23,52,53 At times of crisis, carers were often responsible for attempting to ensure that stated wishes on issues such as resuscitation were respected.22,42 The majority of studies included in this review focused on a single carer, typically a partner. However, within the findings, a number of papers highlighted the complexities of managing information and addressing end-of-life care and decision-making within a family network, for example disagreements between relatives over the correct course of action, attempts to shield children from potentially distressing information, and ambiguity over the role of non-spousal carers.6,23,24,26,37,40,61,62,66 This suggests a potential need for further research into the experience of different types of carers at end-of-life, as well as the interactions between different individuals within families and other networks providing informal care.
Strengths and limitations
This was a metaethnographic review that considered a range of qualitative papers on carers’ experiences of end-of-life care with neurological conditions, identifying key, cross-cutting themes within the literature. However, data collection within identified papers took place mainly within the ‘Global North’, predominantly with spousal carers, and studies often used similar approaches to recruiting participants. It is therefore likely that the experiences of some groups of carers – those in the Global South, non-spousal carers and those not in contact with formal support organisations, among others – are underrepresented here. The review consciously omitted dementia, and the search strategy may also have overlooked papers on some less common neurological conditions. These are limitations on our findings.
Conclusion
The findings of this review suggest that informal carers supporting people with progressive neurological conditions at end of life face particular challenges with regard to uncertainty, variability and discontinuity. Progressive neurological conditions did not align with carer expectations of how end of life ‘should’ be, and end of life services were often perceived to be designed for other conditions, typically cancer. As highlighted by Gofton et al., carers were often dealing with multiple dimensions of uncertainty, some of which were inherent to the condition while others derived from inconsistent access to information and support. 28 Carers struggled to maintain a sense of continuity in the face of these challenges, and as their loved one’s conditions progressed, were often increasingly expected to take a role in key end-of-life decisions. Although the majority of studies primarily focused on a single carer, typically a partner, neurological conditions often had impacts across a much wider family network, with complexities around the sharing of information.
Most papers that made recommendations for action concluded with a general call for earlier and easier access to information, carer support and palliative care. However, Bentley and O’Connor suggest that, given the specific complexities of neurological conditions, it may be more appropriate to embed palliative approaches in neurological care. 50 One intervention study that aimed to improve palliative care for people living with neurological conditions and their carers found that in practice, an approach based around having a team to help co-ordinate services and signpost was frustrated by a fundamental lack of other services. 53 Other studies that focused on specific end-of-life interventions such as advanced care plans and non-invasive ventilation found that lack of awareness by other professionals was sometimes a problem, resulting in issues such as inappropriate attempts to resuscitate.22,43 However, another study found that carers welcomed targeted support assessments. 60
Given the relatively clear narrative regarding existing challenges and frustrations, there is a need for future research focusing on the practical delivery of improved services for carers of people with long-term neurological conditions. There are a number of potential models for doing so, and this is likely to be dependent on the local service context. A key consideration to explore would be the extent to which carers require access to support with specific knowledge of neurological conditions, or whether adaptations can be made to existing carer and palliative services to improve their response to the needs of people living with neurological conditions and their carers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.