
Abstract
Background:
The palliative care needs of people with advanced head and neck cancer pose unique complexities due to the impact the illness has on eating, speaking, appearance and breathing. Examining these needs would help provide guidance about developing relevant models of care and identify gaps in research knowledge.
Aim:
To identify and map out the palliative care needs and experiences for people with advanced head and neck cancer.
Design:
A scoping literature review following the methods described by the Joanna Briggs Institute.
Data sources:
An electronic search of the literature was undertaken in MEDLINE (Ovid), EMBASE and CINAHL covering the years January 1996 to January 2019.
Results:
People with advanced head and neck cancer often had palliative care needs but there was variability in the timing and access to relevant services. A high prevalence of interventions, for example hospital admissions were needed even during the last month of life. This was not necessarily negated with early engagement of palliative care. Dissonance between patients and family carers about information needs and decision-making was an additional complexity. Studies tended to be descriptive in nature, and often involved a single centre.
Conclusion:
This scoping review demonstrates the complexity of care for people with advanced head and neck cancer and the issues related to the current healthcare systems. Focus on appropriate referral criteria, increased integration and coordination of care and robust evaluation of specific care components seems key. Linkage between research and service design delivery across teams, disciplines and care settings seems pertinent.
Advanced head and neck cancer patients have specific challenges due to the impact of the illness on vital functions such as eating, speaking and breathing.
Identifying the palliative care needs of this specific cancer subgroup would help provide guidance about how services could best provide care.
Advanced head and neck cancer patients have a diverse range of palliative care needs, but there is variability in terms of access and timing to palliative care services.
Dissonance between patients and family carers about information needs and decision-making represent additional complexities.
Head and neck cancer patients frequently require acute interventions even during the last weeks of their life.
Tailored needs-based referral systems for advanced head and neck cancer patients may help address issues relating to access to palliative care services.
Models of care focused on increased integration and coordination across different care settings and multi-disciplinary teams may help address issues relating to frequent use of acute interventions during the last weeks of life.
Prospective multi-centre studies, potentially using mixed methods approaches, and focused on testing specific components of care may help further understand and tailor services more appropriately to meet needs.
Introduction
On a global scale, head and neck cancer is the sixth most common cancer, 1 representing a wide-ranging group of cancers arising from the epithelial lining of the upper aerodigestive track, and affecting the oral cavity including the lips; pharynx; larynx; paranasal sinuses and nasal cavity; salivary glands and middle ear. Within certain parts of the world, for example the United Kingdom (UK), the incidence of head and neck cancer is expected to rise by 50% over the next 20 years. This trend is attributed to more cases caused by Human Papilloma Virus (HPV). 2 Although there is variability depending on the underlying histology, the overall 5-year survival rate has remained at 40% to 65%, 3 due to factors such as advanced stage disease presentation and co-morbidities. Additionally, one in every five people with head and neck cancer will die within 12 months following diagnosis. 4 Worldwide, poverty and socio-economic deprivation impact on survival, raising concerns about inequalities or disparities in access to healthcare services, including palliative care provision.5,6
Compared with other cancers, the palliative care needs of people with advanced head and neck cancer pose unique complexities due to the impact the illness has on eating, speaking and breathing.7 –9 Head and neck cancer can be very visible, often causing facial disfigurement 10 and distorted or unintelligible speech. Patients have distinct care challenges and can require feeding tubes and tracheostomies to support their vital functions. Symptoms can cause significant psychological distress and social isolation and there is a higher risk of suicide compared with the general cancer population. 11 Earlier in the disease trajectory, family carers to those with head and neck cancer also report distress and unmet needs.12,13
Given the overall prognosis and potential for rapid demise for a significant proportion of head and neck cancer patients, it is important to consider support at the time of diagnosis for those with advanced disease. Understanding the palliative care needs and experiences of this vulnerable population is important to help devise relevant models of care and identify future research gaps. Although there have been two systematic reviews on unmet needs for advanced cancer patients,14,15 none have specifically focused on people with advanced head and neck cancer. Head and neck cancer brings unique challenges due to the anatomical location of the illness, and the fact patients are likely to experience significant symptom (physical and psychological) and healthcare burden regardless of what treatment course is chosen. 16 A scoping review is beneficial to examine broad areas and is particularly useful to report on the types of evidence which may inform practice or identify key gaps in the evidence. 17 The aim of this scoping review was to examine and map the palliative care needs and experiences for people with advanced head and neck cancer. As the research objective was wide-ranging, and the identified study designs were expected to be heterogeneous, a scoping review approach was deemed more appropriate compared with systematic review methodology.
Methods
Literature review question
The specific question to be addressed was:
What types of palliative care needs and challenges have been reported by people with advanced head and neck cancer, their family carers, and the healthcare professionals looking after them, in terms of their experiences and usage of healthcare services?
Design
The Joanna Briggs Institute Scoping Review framework was used to guide conduct of the review. 17 This framework represents well-established, detailed guidance, has previously been used to assess the quality of scoping reviews, 18 and helped, in part, frame the development of the PRISMA extension on the reporting of scoping reviews. 19
Search strategy
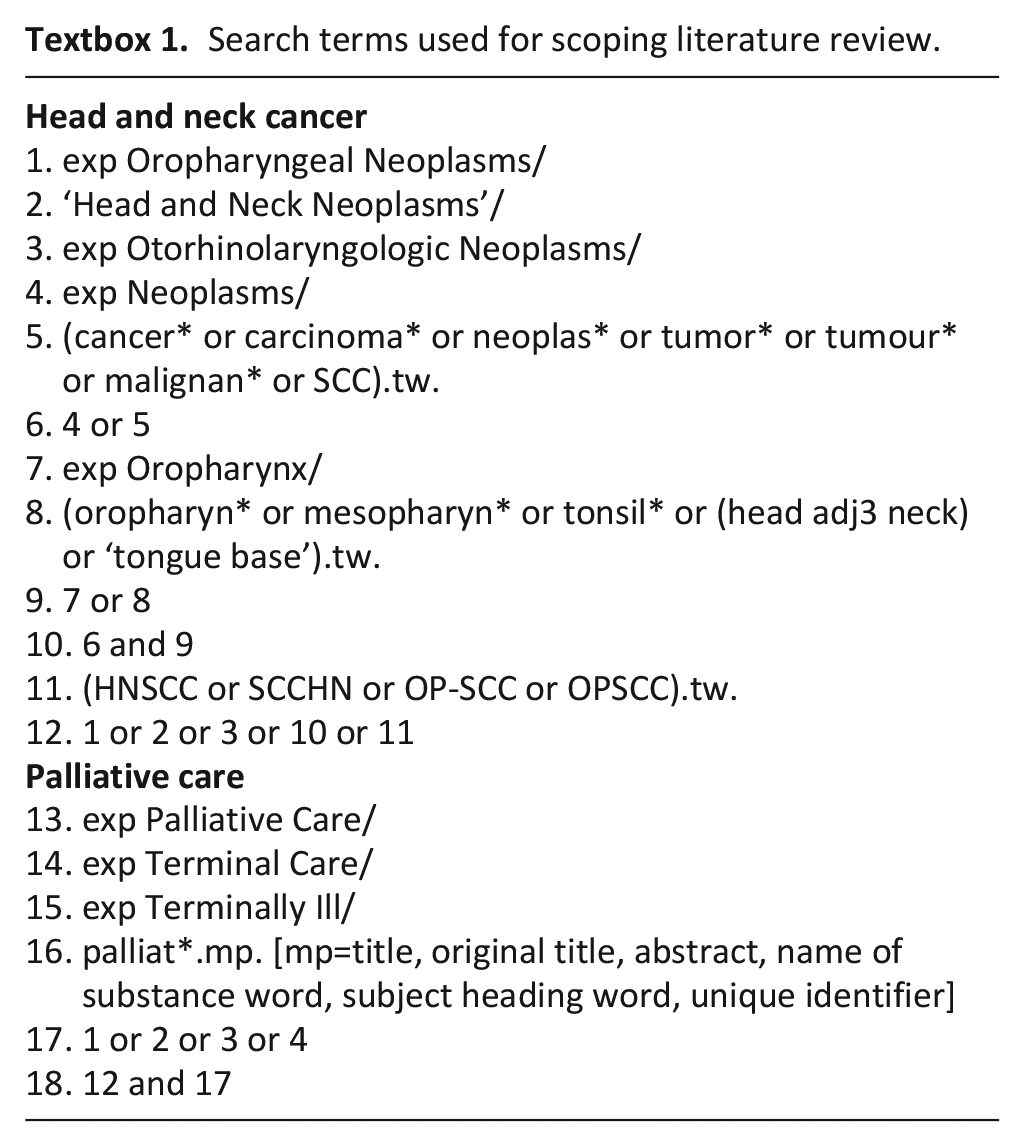
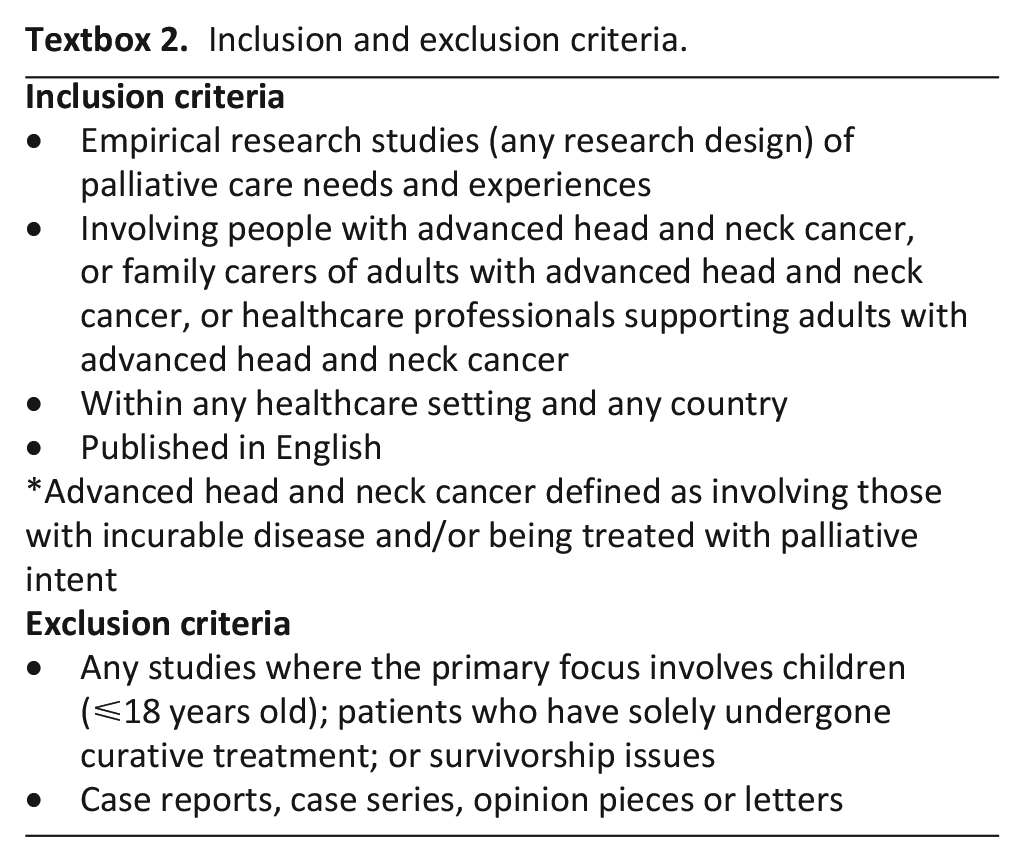
An electronic search of the literature was undertaken in MEDLINE (Ovid), EMBASE and CINAHL covering the years January 1996 to January 2019. It was undertaken using keywords and subject heading terms for ‘Palliative care’ and ‘head and neck neoplasms’ (Textbox 1) using specified inclusion and exclusion criteria (Textbox 2). The searches were initially run on 12th April 2017 and further updated on 8th February 2019. The full MEDLINE search is available in Supplemental Table 1 and the other searches are available on request of the corresponding author. Titles and abstracts were initially screened (CRM, QMH or MC) to identify potentially eligible papers and any areas of uncertainty were resolved by another reviewer (PD). The full manuscripts of potentially eligible papers were further independently screened against eligibility criteria by two reviewers (either CRM and PP, CRM and PC, HCD and PD), with a third reviewer (PD or CRM dependent on the team) resolving any conflicts of opinion, to determine a definitive list of included studies (Figure 1). No additional hand searching was conducted but references of the included papers were also screened for any other relevant papers that might have been missed by the search.
Search terms used for scoping literature review.
Inclusion and exclusion criteria.
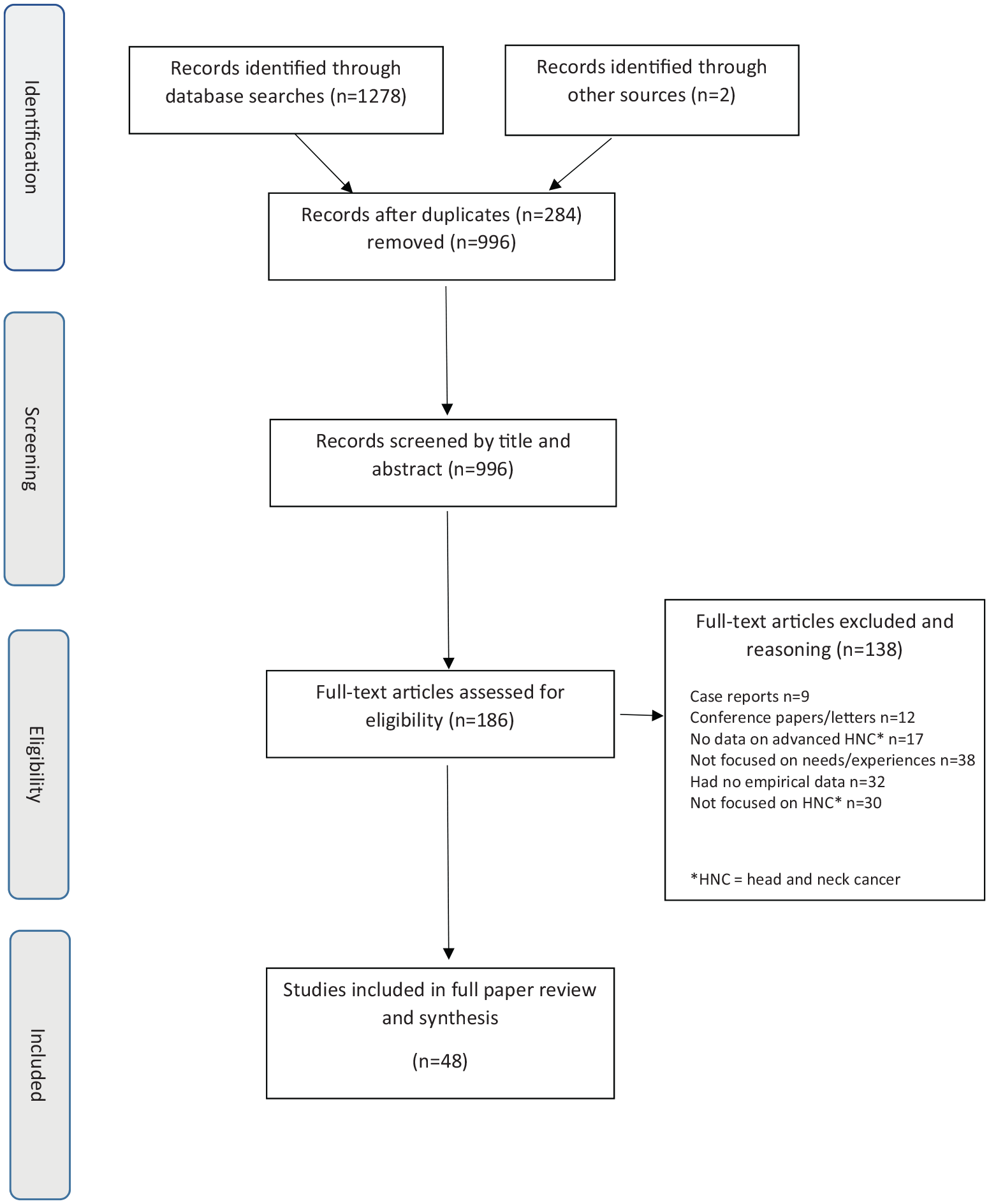
Flow diagram for the scoping review process.
Data extraction
Data was extracted using a specially designed proforma by one member of the research team (CRM, PP, PC or PD) and 75% were checked by a second reviewer (CRM or PD). Data was mapped out in a descriptive manner according to the following: setting, country, population characteristics, study design, intervention (where appropriate) and findings. The World Health Organisation’s definition of palliative care includes the ‘early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual’. 20 Therefore, prior to the search, the team had agreed key themes within the protocol based on the expert knowledge within the team, and anticipating the likely complexities relating to communication and need for interventions to support vital functions of relevance to people with head and neck cancer. These themes were: symptom control; psychological well-being; communication and/or decision-making; place of care and death and medical interventions at the end-of-life.
Data analysis
Following the data extraction, the studies were categorised to one or more of these themes based on their findings, and the themes revised accordingly, following review and discussion by members of the team (CRM and PD). Following this, the data was tabulated and synthesised within each of the final themes. The final themes agreed were:
overall palliative care need and access to palliative care services
physical symptoms
psychosocial and spiritual well-being
medical interventions in the last 12 months of life
communication and decision making
place of death.
Due to the wide range of different study methodologies, and in keeping with the accepted remit of scoping review guidance, specific quality appraisal was not conducted. 17 Instead, key study limitations, where documented within the manuscripts, were extracted to inform the synthesis of data within themes.
Results
Range of studies
From 1278 initial records, 185 papers were screened for eligibility, of which 46 were included in the full review. An overview of the characteristics of these 46 included studies is provided in Supplemental Table 1.
Studies were most commonly conducted in Europe (n = 23)8,22,23,29,31 –33,35,37,43 –45,47 –49,51,52,55,57,59,63 –65 with 12 being conducted in Asia,24 –28,34,40,42,45,53,61,62 nine in North America,30,36,38,39,41,50,54,57,58one in Saudi Arabia 21 and one in Australia. 60 Quantitative methods were used for the majority of the studies (n = 41) with four using qualitative methods29,36,52,65 and one study utilising mixed methods. 59 All the quantitative studies were descriptive or observational in nature (cross-sectional survey, case-control, or cohort studies). Ten studies were nation-wide studies25 –27,30,37,40,47,50,61,62,65 and four were based within a specific region.39,49,64 The remaining 32 studies were conducted within single institutions. Thirty-six studies focused purely on patients,21 –28,30 –41,45 –50,53 –55,57,59 –64 two on family carers alone,44,58 and two on healthcare professionals alone.43,65 A further four focused on both patients and family carers,8,42,51,52 and two on patients and healthcare professionals.29,56
For each key area, studies are presented in Tables 1 to 6; studies which have findings about more than one key area are reported separately within the different tables.
Overall palliative care needs and access to palliative care services for advanced head and neck cancer patients.
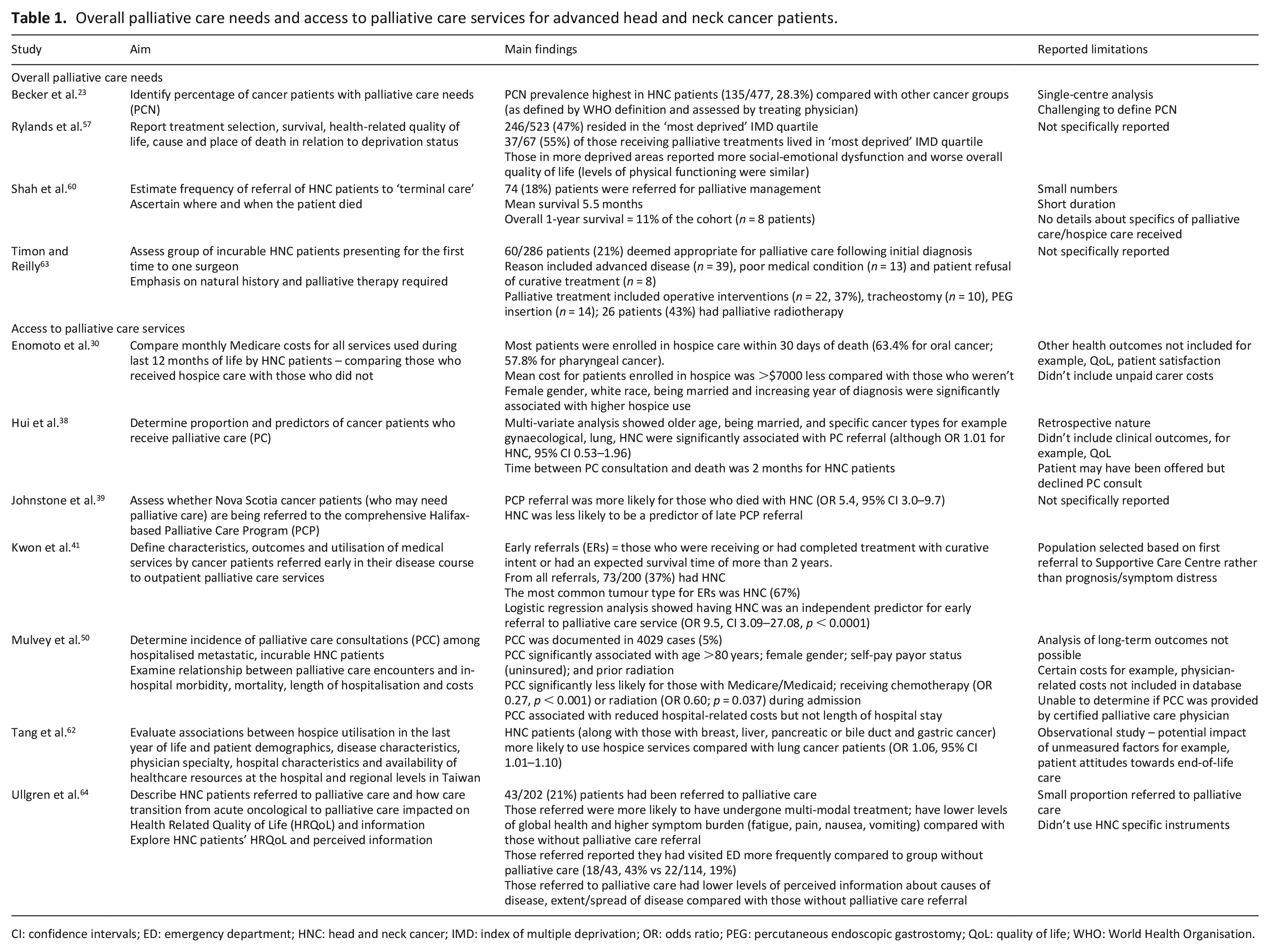
CI: confidence intervals; ED: emergency department; HNC: head and neck cancer; IMD: index of multiple deprivation; OR: odds ratio; PEG: percutaneous endoscopic gastrostomy; QoL: quality of life; WHO: World Health Organisation.
Physical symptoms in advanced head and neck cancer patients.
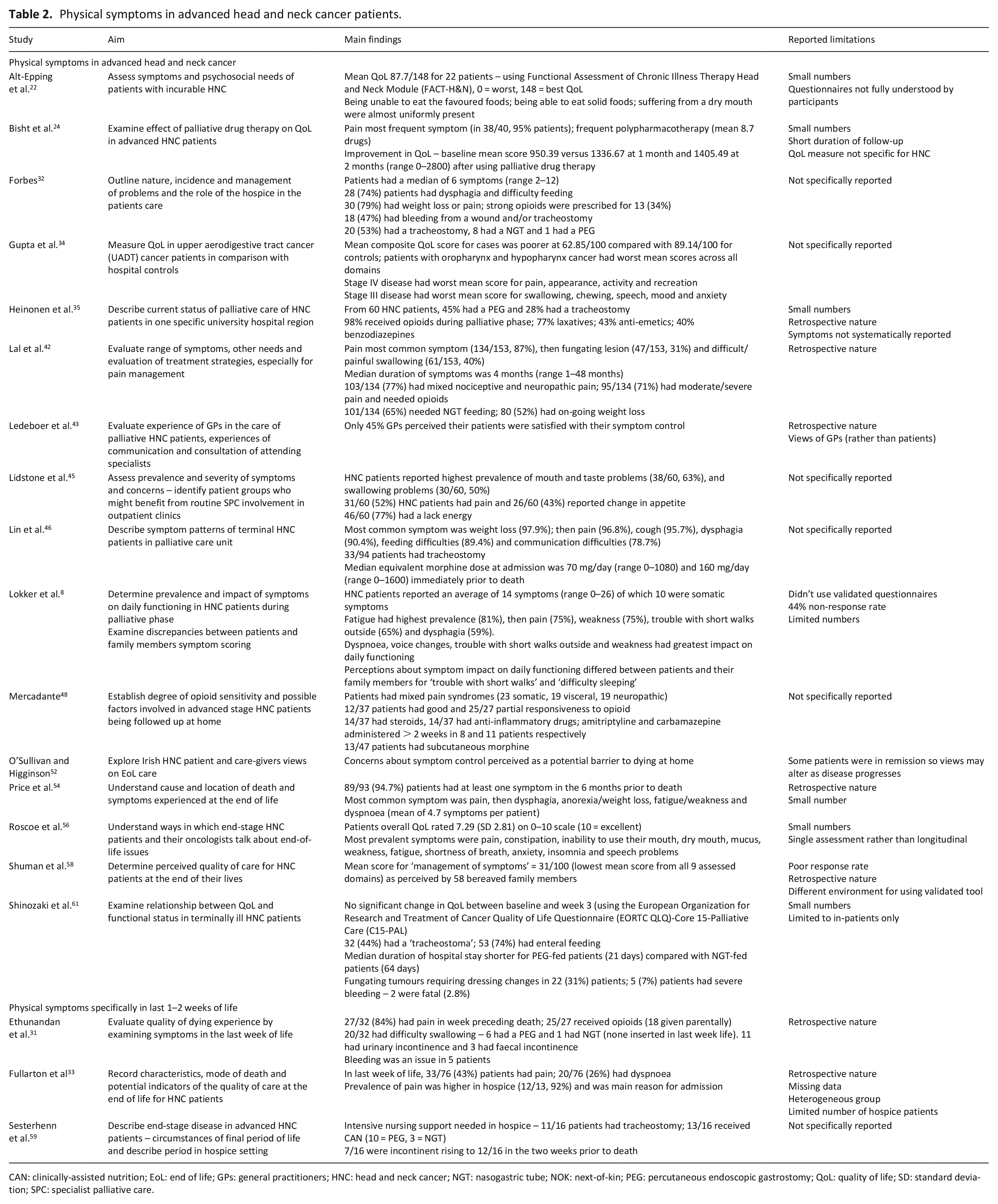
CAN: clinically-assisted nutrition; EoL: end of life; GPs: general practitioners; HNC: head and neck cancer; NGT: nasogastric tube; NOK: next-of-kin; PEG: percutaneous endoscopic gastrostomy; QoL: quality of life; SD: standard deviation; SPC: specialist palliative care.
Psychosocial and spiritual well-being in advanced head and neck cancer patients.
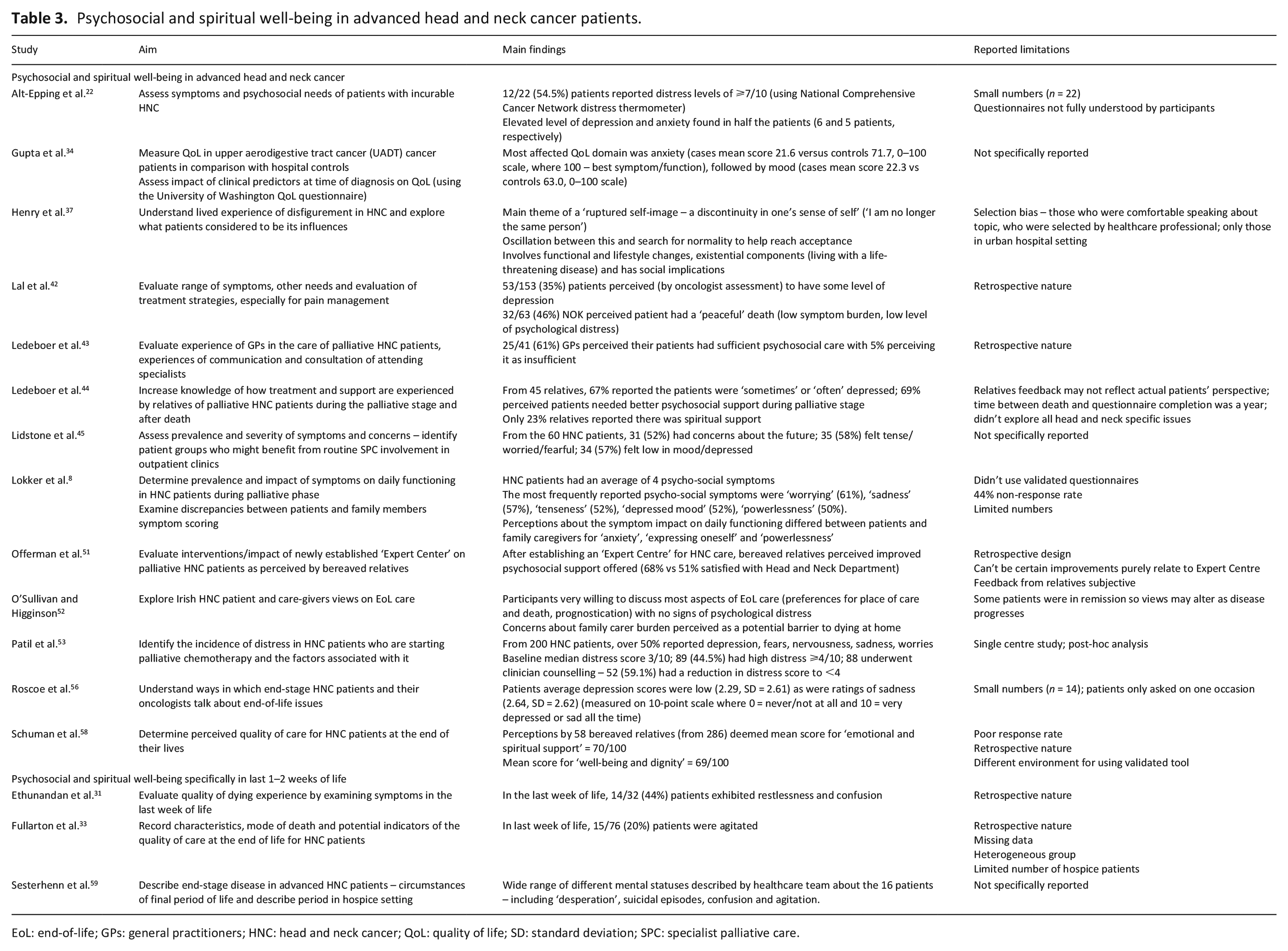
EoL: end-of-life; GPs: general practitioners; HNC: head and neck cancer; QoL: quality of life; SD: standard deviation; SPC: specialist palliative care.
Medical interventions with advanced head and neck cancer patients in the last 12 months of life.
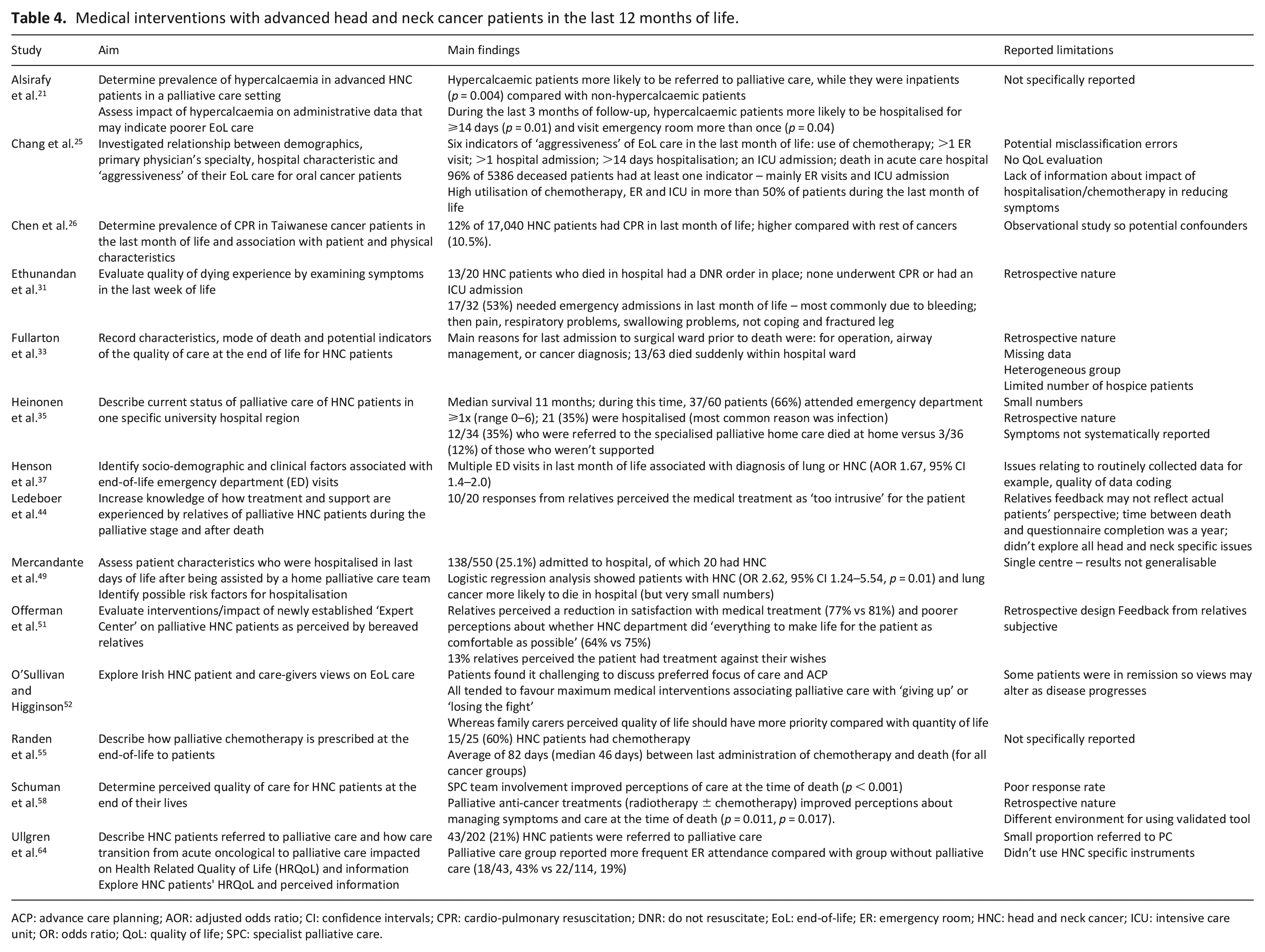
ACP: advance care planning; AOR: adjusted odds ratio; CI: confidence intervals; CPR: cardio-pulmonary resuscitation; DNR: do not resuscitate; EoL: end-of-life; ER: emergency room; HNC: head and neck cancer; ICU: intensive care unit; OR: odds ratio; QoL: quality of life; SPC: specialist palliative care.
Communication and decision-making issues in advanced head and neck cancer patients.
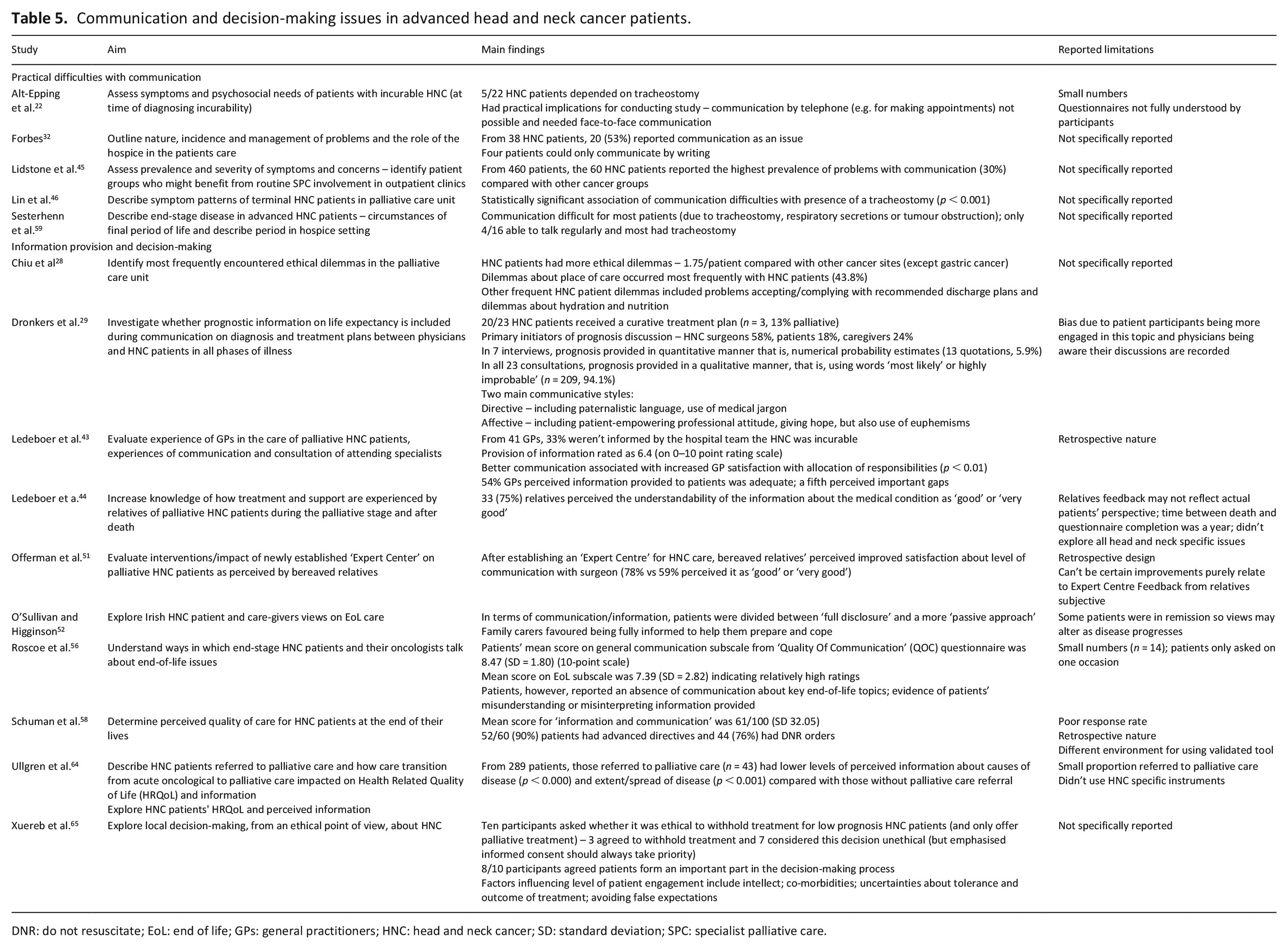
DNR: do not resuscitate; EoL: end of life; GPs: general practitioners; HNC: head and neck cancer; SD: standard deviation; SPC: specialist palliative care.
Place of death for advanced head and neck cancer patients.
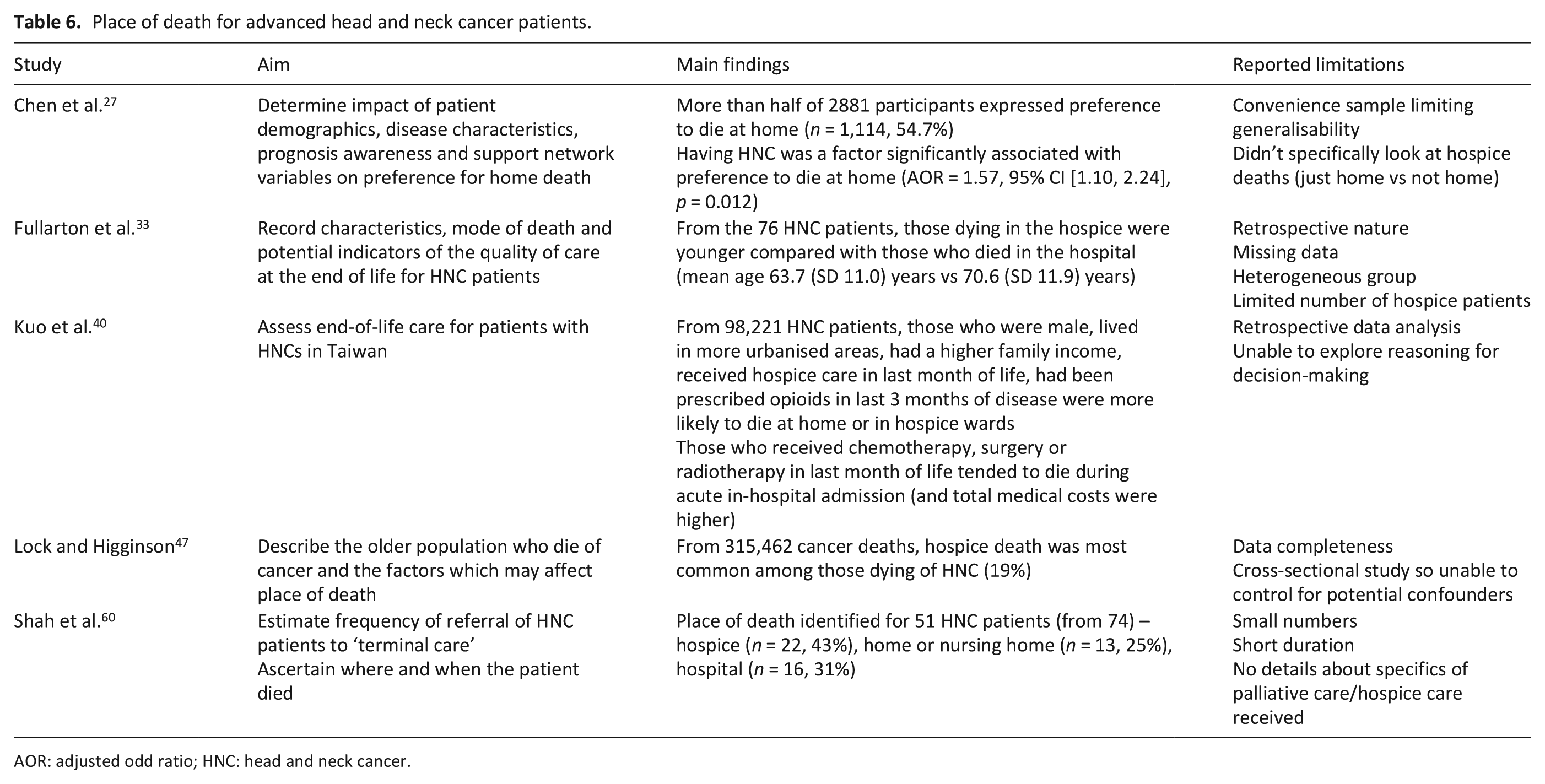
AOR: adjusted odd ratio; HNC: head and neck cancer.
Overall palliative care need and access to palliative care services
There were 11 studies reporting on these areas (Table 1). Studies suggest that 18% to 21% of all people with head and neck cancer received palliative management following diagnosis,56,63 with a higher rate seen for those residing in more deprived areas. 57 There was some evidence that access may be lower than need, however, with one study estimating 28.3% of hospital in-patients had relevant needs. 23
Head and neck cancer patients were more likely to receive palliative care or prompt a referral to palliative care services than other cancer patients38,39,41,62 due to the high degree of symptom burden. 64 Timing of referral to palliative care teams varied, with two studies suggesting that head and neck cancer patients were referred early,39,41 and one study observing late referral, that is, in the last 30 days of life. 30 Higher rates of access to palliative care services were observed among those with HNC who were older, white and female.30,50
Patients’ physical symptoms
Nineteen studies included a focus on this area (Table 2). Patients reported a diverse range of symptoms8,32,54 with the most recent study reporting patients had an average of 10 somatic symptoms. 8 Pain was commonly reported (prevalence ranging from 40% to 95%)8,24,31 –33,42,45,54,57 and one study described it being worse for those with more advanced disease. 34 Pain could be complex in nature, require multiple medications including the frequent use of opioids.24,31,35,42,48 Fatigue or lack of energy (prevalence ranging from 77% to 81%) and weight loss were also frequently reported.8,45,46,54,57 Other symptoms were wide-ranging including difficulty eating or swallowing, dry mouth, incontinence, bleeding, dyspnoea, fungating lesions, change in appetite, cough, communication difficulties, constipation, retained mucus and insomnia.8,22,31,32,33,42,45,46,54,57,61 One study described the intensity of nursing care needed to support patients, in part due to symptom control. 59 Patients’ concerns about adequate symptom control were perceived as a barrier to whether or not they would be able to die at home. 52
From the family carers’ viewpoint, pain, inability to eat and tumour fungation were reported to be the most distressing symptoms. 42 Bereaved relatives perceived there was scope to improve on symptom management, 58 a view shared by General Practitioners. In one study, only 45% General Practitioners perceived their patients had been satisfied with the level of symptom control. 43
Patient’s psychosocial and spiritual well-being
Sixteen studies included a focus on this area (Table 3). The reported prevalence of psychological distress varied.8,21,33,44,52,55 In the two larger studies (with more than 100 patients), more than 50% expressed psychological symptoms such as ‘worrying’, ‘fears’, ‘sadness’, or ‘depressed mood’.8,52 Being a burden on family carers was one specific concern raised. 51 Within a further study, over a third (35%) of people with head and neck cancer were perceived to have some level of depression by their oncologist. 41 Psychological symptoms manifesting as agitation or confusion were also reported during the final weeks prior to death.28,32,58
In terms of psychosocial support and care, one study reported that 25/40 (61%) of General Practitioners perceived their patients had received sufficient care. 42 Perceptions from family carers varied. In one study, the ‘emotional and spiritual’ support was rated more highly (and hence needs better met) compared with management of physical symptoms. 57 In another, however, almost 70% bereaved relatives perceived improved psychosocial support was needed during the palliative phase of illness, 43 which led to the development of an ‘Expert Centre’ to help address these unmet needs. 50
No study specifically focused on spiritual well-being. One qualitative study explored the ‘lived experience’ of having disfigurement and described the subsequent existential impact. 35 A further study reported only 10/45 (23%) bereaved relatives perceived spiritual support for head and neck cancer patients had been provided. 43
Medical interventions in the last 12 months of life
Fourteen studies had a focus on medical interventions (Table 4). Generally, having head and neck cancer was associated with a high prevalence of ‘intensive’ interventions, especially in the last month of life. These interventions included emergency department attendance, cardio-pulmonary resuscitation, hospital admissions, intensive care admissions and ongoing chemotherapy.25,26,31,35,37,55,64 Factors associated with hospital admission included the presence of hypercalcaemia, 21 respiratory or airway management issues,31,33 infection 35 and problems relating to bleeding, pain and swallowing difficulties. 31 Hospital admission could still occur frequently even when palliative care teams were involved. 64 Two retrospective studies, conducted after death, reported that having head and neck cancer was associated with a greater risk of dying in hospital,25,49 although one study had very small numbers. 49
Differing views were reported about the appropriateness of interventions. Patients could favour maximum medical interventions 52 and bereaved relatives perceived the palliative anti-cancer treatments improved symptom management. 58 On the other hand, however, bereaved relatives reported that treatments had been ‘too intrusive’ or not in keeping with the patients’ wishes.44,51
Communication and decision-making
Fifteen papers including a focus on communication and decision-making for head and neck cancer patients (Table 5). Five papers focused more on the prevalence of the practical difficulties and issues relating to poor speech.12,32,45,46,59 Issues relating to communication were more common compared with other cancers, 45 especially if the patient had a tracheostomy.22,46,59
Ten of the papers focused on communicating information and decision-making.28,29,43,44,51,52,56,58,64,65 An interview study of medical professionals in Malta, explored ethical factors influencing decision-making about treatment. The majority who were interviewed (7/10) perceived the need to provide full treatment for people with head and neck cancer, even if the prognosis was poor. Most agreed, however, that the patient formed an important part in the decision-making process. 65 In a study assessing the communication of prognosis between healthcare professionals and patients, different ways were recognised. These included the use of numerical probability estimates, qualitative language or a combination of both. 29 Although perceptions by patients and/or family members about the quality of communication could be good,44,51,57,58 there were reports of patients misunderstanding or misinterpreting information. 56 One study described poorer levels of understanding about their illness when patients were known to palliative care teams. 64 Within another qualitative study, dissonance between patient and family members’ information preferences was described. Patients varied between wishing for ‘full disclosure’ and a more ‘passive approach’ whereas family carers favoured being fully informed. 52 Further communication and decision-making challenges included the information transfer between different healthcare teams 43 and the ethical complexities that can arise relating to hydration and nutrition. 28
Place of death
Five studies focused on place of death, of which two were population-based40,47 and three were smaller cohort studies (two having less than 100 patients) (Table 6).27,33,60 From the population-based studies, a Taiwanese study reported over 70% head and neck cancer patients died in the acute hospital. 40 By contrast, the other study, conducted within the UK, suggested that head and neck cancer was associated with an increased likelihood of dying in a hospice compared with other cancers. 47
Discussion
Summary of main findings
Compared with other cancers, this scoping review confirms head and neck cancer patients often have complex palliative care needs, especially if there is a high degree of symptom burden. Variability in the timing and access to palliative care services, however, is recognised. Dissonance seen between patients and family carers, specifically about information needs and decision-making, are additional recognised complexities. A high prevalence of interventions such as emergency department attendance and hospital admissions occur for patients with advanced head and neck cancer even during the last weeks of life. Sole engagement with palliative care services does not necessarily negate this.
Research in this area has tended to be via single centre, quantitative studies. Few qualitative studies have been conducted with advanced head and neck cancer patients and none have focused purely on the spiritual well-being of head and neck cancer patients. There were no interventional studies identified.
What this study adds and implications for practice and research
The key questions facing palliative care services surround the identification of who is in greatest need of referral, how these individuals should be identified, and what model of care should be provided. 66 These questions are particularly pertinent for head and neck cancer patients who undoubtedly have palliative care needs, but for whom the method of identification and the optimum model of care provision is less clear. Our review shows variability in access to palliative care services with some patients receiving referrals late and certain groups, such as older, white, female patients, more likely to be referred.
In view of the ‘scarcity of palliative care resources, 66 there are a number of potential ways to help identify which head and neck cancer patients would most benefit from palliative care input. Specific ‘triggers’ are recognised to help prompt palliative care consults in the emergency department, in-patient wards 67 and from oncology services. 68 These are generic tools aimed to screen a large population, however, rather than having been specifically validated within the head and neck cancer remit. More individualised ways to help illustrate patients concerns include the use of Holistic Needs Assessment (HNA) tools, 69 and Patient Reported Outcome Measures, of which a vast array have been used within head and neck cancer. 70 The Patient Concerns Inventory (PCI) is an item-prompt list specifically used to guide head and neck cancer clinical consultations including wider multi-professional engagement. Although extensively used globally, its focus of use has been with curative head and neck cancer patients, but it has potential to be adapted. 71 Further research into which ‘screening’ tool or method would be most appropriate for initiating palliative care referral for head and neck cancer patients seems pertinent. Furthermore, clarity about how best to incorporate specific staging indicators for those recognised to be ‘high risk’ 72 in additional to individual patient needs would seem beneficial.
As well as establishing equitable referral methods, defining an appropriate model of integrated care is needed. This poses a further challenge for advanced head and neck cancer patients. Our review indicated there was a high level of interventions needed and a reliance on hospital-based care even during the last weeks of life. This finding may relate to issues arising from the use of feeding tubes and tracheostomies to help sustain vital functioning, and the fact that hospital admissions were commonly related to breathing or airway difficulties. Issues such as these can be challenging to manage in a community setting. More widely, ‘treatment related incidents’ such as those relating to other interventions, for example, urinary catheters or nasogastric tubes, are a recognised factor prompting patient safety incidents during ‘out-of-hours’ care. 72 Additionally, obtaining timely access to care can be a challenge. 72 Solely relying on engagement with palliative care services is not sufficient to alleviate these issues. 64 Instead, the focus may be needed within a number of areas. Firstly, there is a need to increase integration and co-ordination between different multi-disciplinary teams to avoid ‘silo’ working patterns. 64 Additionally, enhanced collaboration between teams 73 would potentially help ensure timely access to specialist knowledge is more readily available. Finally, ways to help upskill healthcare professionals supporting patients within the community, and specific training about the management of tracheotomies and feeding tubes may help alleviate the need for hospital care.
Another important finding from this study was the dissonance between patient and family carer views about information needs and decision-making. Generally, unmet informational needs are recognised within advanced cancer as a whole, 15 as well as earlier in the head and neck cancer disease trajectory. 74 Additional complexities arise due to the many issues surrounding communication, that is inability to directly verbalise and uncertainty about the best way to communicate prognosis. Furthermore, the discussions about goals of care and the optimal ways to consider patient preferences are especially challenging in advanced disease as the treatment can be intensive and the outcomes uncertain. 16 One national cohort study identified that 10% of people with head and neck cancer initially treated with ‘curative’ intent died within the first 12 months following diagnosis. 75 Initiatives such as the ‘Making good decisions in collaboration’ (MAGIC) improvement programmes have been tested in early cancers involving the head and neck. 76 An ‘Option Grids’ approach, which involves using easy-to-read decision aids with patients and healthcare professionals comparing treatment options, has also been assessed in the head and neck cancer context. 77 Future research could focus on ways to engage advanced head and neck cancer patients and family carers more fully in shared decision-making needs, being mindful of the appropriate timing, differing information needs and the cultural sensitivity of these discussions.
In terms of research methodology, the majority of studies were quantitative observational studies conducted within single institutions. There were no interventional studies and there was only one mixed methods study, despite the unique benefits this approach can bring. 78 Additionally, only one study explored the spiritual or existential impact of the illness. There is a real need to develop prospective multi-centre studies, using both quantitative and qualitative approaches. As well as gaining a greater understanding of needs and experiences, testing specific components of models of care would be beneficial. A broader approach to assessing holistic care, including the spiritual component, would also be important.
Strengths and limitations
This scoping review followed an established systematic method and examined a breadth of different experiences and needs for a particularly complex subgroup of cancer patients. Our search included studies from a diverse range of countries and cultures and hence has wide-ranging relevance.
There were, however, limitations to this review. We did not conduct hand searching of key journals and grey literature was not included. Our definition of ‘advanced cancer’ was qualitatively defined rather than using specific disease staging criteria and we did not conduct additional searches using ‘place of death’ as a key search term. Additionally, we only included English language publications. In view of all these factors, some sources of data may have been overlooked. We did not focus on family carer needs per se but accept that this is an important area and would represent a focus for future study. Finally, we did not include a quality appraisal of all included studies, as within the remit of scoping reviews, risk of bias/quality appraisal is not generally recommended. 17
Conclusion
This scoping review has demonstrated the complexity of care for people with advanced head and neck cancer and that there are issues related to the current healthcare systems. Specific focus is needed about the optimum way those in greatest need should be identified and referred to palliative care services. Additionally, further clarity and assessment about the particular model of integrated care is required, which can address the diverse symptom needs, the communication needed to further inform decision-making, and the frequent use of interventions and issues that can arise ‘out-of-hours’ relating to these. Linkage between research and service design delivery across teams, disciplines and care settings seems key for future success.
Supplemental Material
Supp_Table_1_Study_characteristics_REVISED_15.07.2020 – Supplemental material for The palliative care needs and experiences of people with advanced head and neck cancer: A scoping review
Supplemental material, Supp_Table_1_Study_characteristics_REVISED_15.07.2020 for The palliative care needs and experiences of people with advanced head and neck cancer: A scoping review by Catriona R Mayland, Qiaoling Marilyn Ho, Hannah C Doughty, Simon N Rogers, Prithvi Peddinti, Praytush Chada, Stephen Mason, Matthew Cooper and Paola Dey in Palliative Medicine
Footnotes
Acknowledgements
We wish to thank Dr Cathy Hubbert for her contributions to the larger study’ steering group meetings and Mr Dominic Macarevey for his input on behalf of the Aintree Head and Neck Patient and Carer Research Forum.
Authors contributions
C.R.M. and P.D. conceived and designed the study with specific contributions from S.R.N. and S.M. Q.M.H., M.C. and C.M. completed all the searches and conducted the initial screening. Full manuscript reviews were conducted by C.R.M., P.P., P.C., H.C.D. and P.D. C.R.M. and P.D. analysed and interpreted the data. C.R.M. drafted the manuscript and all authors have approved the submitted version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding for this study was provided by Liverpool Clinical Commissioning Group ‘Research Capability Funding’ as part of a larger research project. This funder did not have a role in the study design, collection, analysis or interpretation of the data nor in the writing of the manuscript. Dr Catriona Mayland is funded by Yorkshire Cancer Research.
Ethics
As this study represents a scoping literature review, not formal ethics approval was required.
Data management and sharing
Further information about the search strategies are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.