
Abstract
Background:
Preserving personal dignity is an important part of palliative care. Generally, autonomy, independency and not being a burden to others are emphasised for preserving dignity. Dignity has not been studied yet from the perspective of the growing group of patients with a migration background living in Western countries.
Aim:
To gain insight into (1) what patients – and their relatives – with a Turkish, Moroccan or Surinamese background, living in the Netherlands, in their last phase of life find important aspects of dignity, and (2) how care professionals can preserve and strengthen the dignity of these patients.
Design:
Qualitative thematic analysis of semi-structured interviews.
Participants:
A total of 23 patients and 21 relatives with a Turkish, Moroccan or Surinamese background were interviewed.
Results:
For respondents dignity encompassed surrender to God’s or Allah’s will and meaningful relationships with others, rather than preserving autonomy. Surrender to God or Allah meant accepting the illness, the situation and performing religious practice. A meaningful relationship meant being assisted or cared for by family members and maintaining a social role. Professionals could preserve dignity by showing respect and attention; guaranteeing physical integrity, hygiene and self-direction; and indirect communication about diagnoses and prognoses.
Conclusions:
Religion and appropriate involvement of family members are important aspects of dignity in the last phase of life, in addition to autonomy and independency. Care professionals need to take these factors into account in order to provide person-centred care.
Maintaining autonomy, independency and not becoming a burden to others are found to be important aspects of personal dignity.
The nature and quality of relationships with others can influence personal dignity of the patient.
A lack of insight exists into what patients with a migration background in the last phase of life find important for dignity.
Religion and being meaningful to others are more important for dignity among patients with a migration background in the last phase of life, than autonomy.
The concretisation of being meaningful to others differs between patients with a migration background and patients without.
Professionals could preserve dignity of patients with a migration background by showing respect and attention; attention for different needs regarding dignity; and guaranteeing physical integrity, hygiene, self-direction and indirect communication about diagnoses and prognoses.
Components of personal dignity might be culturally shaped, which should be included in theory about dignity in the last phase of life and taken into account when preserving dignity.
Care professionals should pay attention to different needs and wishes relating to dignity in the last phase of life among a diverse patient population.
Introduction
During the last phase of life, bodily changes, deterioration, pain and loss of independency can lead to impaired personal dignity.1–4 Strengthening and preserving personal dignity is therefore a prominent part of palliative care.4,5 Personal dignity refers to the subjective experience of dignity.6,7 Personal dignity includes the value we attach to ourselves and the value we think others attach to us. It encompasses valuing oneself as an autonomous being (intrinsic dimension) and valuing oneself in relation to others (extrinsic dimension).7–9 Autonomy, continuity of the self, independence and not becoming a burden are considered prominent aspects of dignity within existing models of personal dignity.1,2,4
Research on dignity has mainly been conducted in Western countries, only involving the ethnic majorities. 9 Although no research exists on dignity among patients with a migration background, studies among relatives of patients with a Turkish or Moroccan background in the Netherlands (not about dignity) show the importance of keeping hope alive and of the notion that Allah decides about life and death.10,11 These findings suggest patients with a migration background might emphasise different aspects for preserving dignity and that what dignity entails might be culturally shaped. In general, care professionals can influence the patient’s dignity in the last phase of life.2,3,12 Insight into what dignity means for patients with different migration backgrounds can help care professionals provide appropriate palliative care to these patients. 4 This is especially important because care professionals in Western countries experience difficulties giving palliative care to patients with a migration background.13–16
To meet this knowledge need, we formulated the following research questions, focusing on residents of Turkish, Moroccan and Surinamese origins, being the three largest migrant groups in the Netherlands:
What do patients – and their relatives – in the last phase of life, with a Turkish, Moroccan or Surinamese migration background find important aspects of personal dignity?
How can care professionals preserve and strengthen the personal dignity of these patients?
Methods
Design
We performed a qualitative study using semi-structured interviews which provides in-depth exploration of participants’ experiences. 17 We worked together with migrant network partners and two ethnic-matched bilingual interviewers with Turkish and Moroccan backgrounds during all stages of the study. 18 One interviewer had experience with spiritual counselling, the other with executing questionnaires for research. They received a half-day training in interview skills before data collection started, about how to translate dignity and interview techniques to structure interviews and gain in-depth information for research purposes. An interviewer with a Surinamese background was not needed, because most Surinamese residents in the Netherlands speak Dutch.
Participants
We used purposive sampling to reach a population with almost equal numbers of each ethnic background and gender, and diversity in age and disease; so a large diversity of perspectives could be obtained. We defined patients in the last phase of life as having an incurable disease and/or being in a palliative phase. According to the illness trajectories of Murray et al. 19 this concerned patients in their last 3 months up to 8 years of their lives.
We recruited participants in two hospitals, chosen out of convenience, through palliative teams and the oncology-, lung diseases- and neurology departments. We also recruited through nursing homes with culture-sensitive wards and/or multi-cultural populations from a list of migrant elderly facilities, 20 a general practitioner and our migrant network partners. Physicians, imams, nurses and key informants of these institutions and networks either told us which patients to approach in person or gave the patients and relatives a language-matched information letter, after which we approached the interested patients and relatives by phone. We informed the patients that the interview would be about feelings of dignity in their current situation and the future. We avoided terms such as ‘the last phase of life’, ‘palliative care’ and ‘incurable disease’, because they were seen as daunting by our migrant network partners.
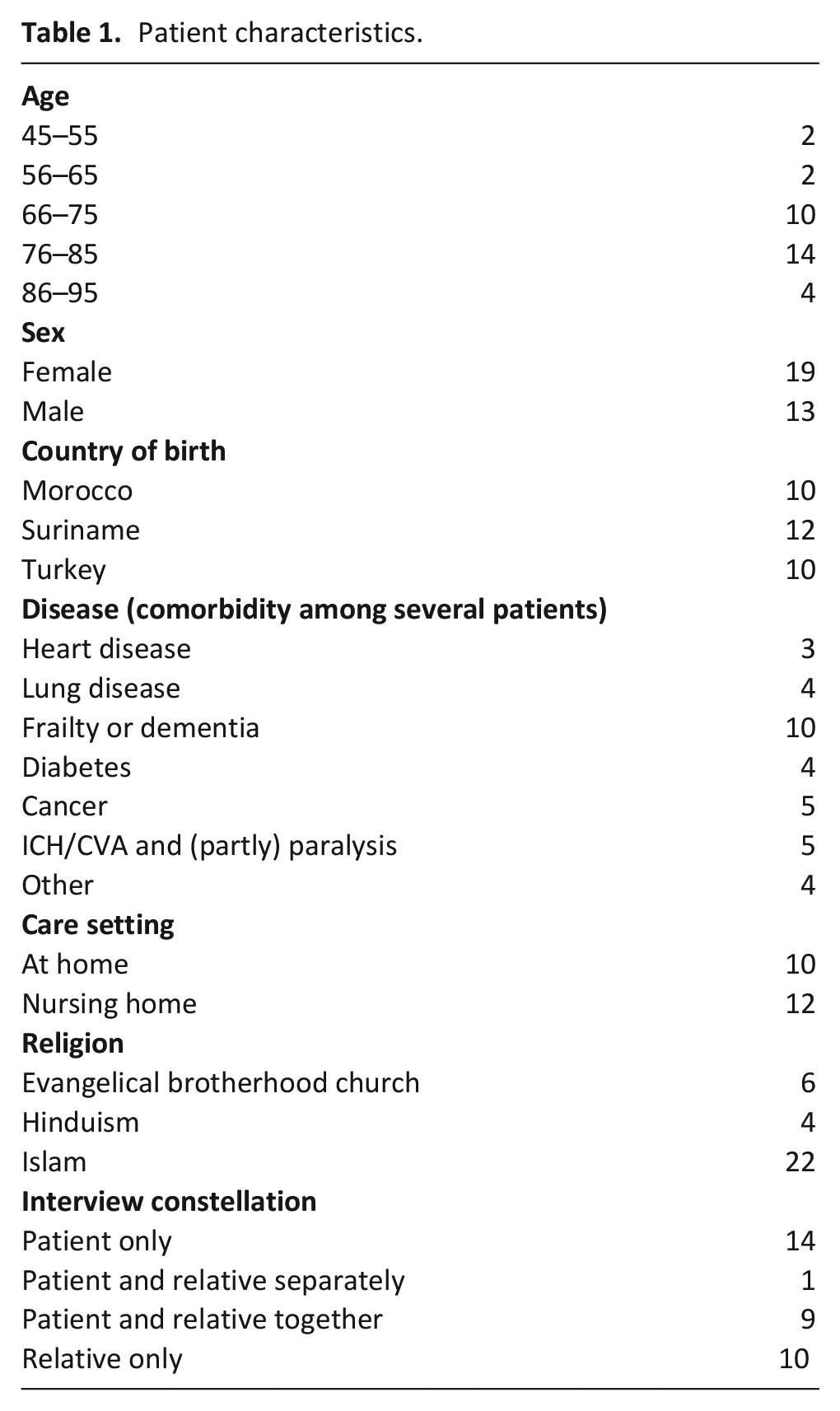
We collected data about 33 patients with a Turkish, Moroccan or Surinamese (with Creole and Hindustani) background in their last phase of life, by interviewing 23 patients and 21 relatives. The interviews were carried out in different constellations: patient only, patient and relative together or separately and relative only (See Table 1 for further details).
Patient characteristics.
Data collection
Interviews were conducted between December 2017 and June 2018, and according to language preferences of the interviewees. XV interviewed all Surinamese participants, and four patients and three relatives with a Turkish or Moroccan background in Dutch. The bilingual interviewers conducted the remaining interviews in Turkish, Berber and/or Arabic. XV verified the first two interviews of the interviewers were carried out correctly and provided in-depth insights. The interview guide was based on literature and interviews with eight key informants, such as Islamic spiritual counsellors, care consultants and social workers. We first asked participants about perspectives on dignity and what influences it, and then about relationships with others, the society, and the future. For ‘dignity’, we used ‘waardigheid’ in Dutch, ‘haysiyet’ and ‘değerli(lik)’ in Turkish, and ‘karama’ and ‘qima’ in Arabic. When participants did not understand the word dignity directly or how it related to their situation, we used other words, such as feeling ‘worthy’, ‘appreciated’, ‘valued’, or ‘small’ as synonyms for ‘(un)dignified’. Eventually, all participants were able to reflect on dignity, however, some patients didn’t seem to know or understand their illness or its seriousness.
Interviews were audio-recorded, and subsequently transcribed and translated simultaneously. Data collection was continued till data saturation of the main themes was reached.
Data analysis
We used inductive thematic analysis, 21 which encompasses familiarisation, identifying a thematic framework, indexing, charting, mapping and interpretation. To guarantee rigour of the study, 22 four transcripts were discussed among XV, JS, MT, MO and the interviewers. XV and MT developed a coding system, coded two interviews individually in an inductive manner and then compared and adjusted the codes. XV coded the rest of the transcripts. Codes were united in overarching themes, which were partly distilled from the literature about dignity. 23 For example, preserving hope was coded as a subtheme of ‘being meaningful to others’, as respondents saw preserving hope as something that others did to support patients. As input for the themes, we used scientific literature about the patients’ dignity,1,2,5,8 dignity and culture12,24 and culture and palliative care. 11
XV, JS and MO discussed codes and corresponding quotes for each theme separately, and XV finalised the meaning of the codes. Resulting descriptions of the main findings were checked for accuracy with the interviewers.
Ethical considerations
The medical ethical committee of the Amsterdam University Medical Centers/University of Amsterdam declared that this study did not require their approval, according to the Dutch Medical Research Involving Human Subjects Act. 25 Participants were informed of the aims of the research and their legal rights. We obtained written informed consent before or directly after the interviews. We used codes to guarantee participants’ anonymity.
Results
We found religion, being meaningful to others and autonomy the most important aspects of dignity. Care professionals can preserve patient’s dignity by giving care with love, attention and respect and ensuring considerate communication.
Religion
The religious perspective – that Allah or God decides about life, illness and death – helped many patients to surrender to what is predestined and meant that having to deal with dependency felt less, or not at all, undignified for them. This religious perspective was an important part of dignity for Turkish and Moroccan participants. When we asked them about dignity after they shared their experiences with dependency, they immediately mentioned the predestination, while most Surinamese patients did so only when explicitly asked about religion.
Interviewer: So, you take it as God has predestinated it. It doesn’t increase or decrease your feeling of dignity? Respondent: No, it really doesn’t. It is how it is predestinated. If dying is predestinated, than that is what it is. You cannot do anything to change that.. you have to believe in your fate, you have to believe in.. That is how God has meant it, God gives peace, nobody can deprive you from that. (Moroccan patient, #15)
When prompted further about this, surrendering to Allah’s will also appeared as a prescription for facing difficulties in life, and thus as dignified behaviour. A patient explained purification will occur when one is able to surrender to Allah’s predestination. Acceptance itself, then, can be something to strive for to become purified.
In the Islam it is said that when you are sick, that is a purification. You get purified. It is a test. It is a very tough test and yes, how are you dealing with it? Have you accepted it? Do you find it difficult? When you have accepted it, then it counts as a purification. Then the sin, so to speak, that you.., those will be erased. And that also gives you that.. That makes you stronger again. (Moroccan patient, #19)
Accordingly, control of the self and the emotions regarding the disease or situation appeared to be important for maintaining dignity. Complaining about symptoms or the situation is an infringement of one’s dignity. The patients’ prayers and this surrender to Allah also appeared as an inducement for visits from the community and can strengthen dignity of the patient by recognition of this practice.
Interviewer: So you didn’t lose your dignity? It was not influenced?
Respondent: It is from Him (Allah). You’ll become sick and after that you’ll die, that’s the way it is. We’ve got nothing to say about that, that’s what we believe in. I do not believe in such things (that illness could impair his dignity); In such situation, I am not focusing on my own feelings. I don’t do that. (Turkish patient, #23)
Interviewer: So you are saying that his experience of dignity, and the maintenance of dignity originates from his faith?
Respondent: Yes, faith, and moral support. [..] The neighbors and friend were so used to coming, that they just wanted to hear a prayer from him and they just came for that. Some of them said ‘I have come now, but I will come again later.’ So we always had visitors. He always prayed to God. Everyone said: ‘Ok quiet, we want to hear the man himself, that he is praying for us. It wasn’t hard at all, he really was a special person. (Turkish relative, #31)
In line with the importance of religion for dignity, participants viewed religious practice as important to preserve dignity. Religious practice concerned rituals, praying or singing with a priest, reciting the Quran and adhering to specific rules. One Surinamese patient mentioned religious practice induced her mental strength, which was important to stay true to her convictions (autonomy), and consequently strengthened dignity.
The spiritual counselor can come and visit me. We can sing together. We can pray together. To give you mental strength. (Creole-Surinamese patient, #2)
Later in the interview this respondent explained the relevance of this mental strength.
When a human being does not have mental strength, then you are a follower, then you do not have dignity. (Creole-Surinamese patient, #2)
Being meaningful to others
Respondents considered feeling connected and being meaningful to others – family, friends, other nursing home residents, care professionals or the community – as important for personal dignity. When such relationships were hindered or declined, dignity was impaired. In this relational context, the maintenance of a social role was important for preserving dignity: being recognised as someone’s (grand)parent or uncle/niece. One Surinamese relative mentioned this included performing the actual activity belonging to that role.
At one point she said: ‘You don’t appreciate me anymore.’ Shocking. I said: ‘What do you mean by that?’ Well, she cooked for us. She lost that. And with that, her love, her worth as a mother that cared for her children, was gone. Doing grocery shopping herself. Doing something for her surroundings. That was gone. Mother who always cooked for her children, it was not possible anymore. (Hindustan-Surinamese relative, #12)
Receiving moral support and (daily) visits or calls from family and the community, and serving food to and receiving food from visitors were important elements of meaningful relationships. For Turkish and Moroccan patients and relatives, another important element was to give each other hope about things they could do in the future, such as pilgrimage or visits to the country of birth, even though such plans might seem unrealistic.
My husband said then ‘Let’s go to Hadj when I will get better, and when we go this year, then I will give money for Berat’s (fictitious name) ticket, then he will bring us there, with a car for disabled..’ etcetera. I want to let you do Hadj, you have done too much for me. But I thought to myself ‘He is lying here so sick, how are we going to do it?, but I said to him: ‘Yes, Insha Allah are we going, my man.’ I thought like: ‘That man cannot stand up, has a diaper underneath him. How?’ (Turkish relative, #31)
Assistance and being cared for by family members instead of care professionals also contributed to personal dignity because such acts seemed an expression of patients’ worth in the relationship. Many patients and relatives viewed taking care of elderly or loved ones as a valued norm, and moving the patient into a nursing home was a violation of this norm.
Then (when her nieces are visiting) I feel like I’m on top of the world [..] Because I am happy that I’ve got them. Because I’ve got two boys and two girls. All four do the laundry for me. (Creole-Surinamese patient, #3) She really wanted to stay at home. That she found really awful, that her children have put her here (in the nursing home). She found that not nice. Every time we (her children) are here she says: ‘I don’t want to stay here.’ She says: ‘You are my children right, you should take care of me.’ That is not nice for her. (Turkish relative, #27)
For some patients, understanding the impossibility of relatives completing these tasks and them having their own lives, was enough for them to maintain their dignity. For others, the patient’s dignity was infringed because of their own opinion or the opinions of the community on unfulfilling these care duties, which in one case was due to lack of knowledge or (dis)belief about the disease.
We cannot be part of the community anymore. The gossip, it drives me nuts (crying tone). They say: ‘He has dumped his wife there and he is just gallivanting on his own.’ They only see the appearance, nobody knows the inner. Interviewer: Do you have fears regarding her dignity in the last phase of life? Respondent: They come from outside, impair her feeling of dignity and also mine. I relinquished from the mosque, I do my prayers here. (Turkish relative, #28)
Autonomy
Losing autonomy was hard for all patients, due to needing help for self-care and bathing, inability to choose their own day-schedule, having to wait for care professionals, and the consequences of care coming too late. Mostly Surinamese patients, however not all of them, mentioned these aspects also impaired their dignity.
Interviewer: How could you feel more dignified? Respondent: If only I had a wheelchair with a motor. Then I can push a button and I am gone. Because I had a mobility scooter when I lived at home. [..] Interviewer: ‘So you always have to be pushed forward by someone? Respondent: Yes, by someone else. And when that person is not in the mood for it.. I have always found people that gladly pushed me. My children, my son-in-law. (Creole-Surinamese patient, #3)
Keeping a certain degree of self-direction about the continuation of treatments or unhealthy habits, such as smoking, in the last days or weeks contributed to personal dignity for patients of all groups. Surinamese participants mentioned active participation in conversations about treatments and care plans and timely and continuous discussion of continuation of treatments as relevant to dignity.
Strategies to protect autonomy and dignity mainly included abstaining from thinking or talking about having a life-threatening disease or the future. This was often explained as Allah/God deciding about illness and death.
Caregiving with love, attention and respect
Participants mentioned caregiving, by care providers, done with love, attention and respect preserves dignity, including personal attention, time for social interaction, building a relationship, frequent visits and sympathy. Respect encompassed using formal language, approaching the patient as an adult, having an appropriate attitude towards a diminished sense of self-direction in times of vulnerability and respecting privacy to deal with emotions or pain.
My mother was a dignified woman. A proud woman. Then, you do not, as a stranger to her, talk to her as a child. I have seen this kind of things. These were the things of which I thought ‘Send them all out. I will do it myself. Yes, ‘Hey missy..’ You know, with a tone of which you think, just shut up. It is a grown-up woman. Treat other people decently. Pay attention to norms and values. (Hindustan-Surinamese relative, #12)
Respect also included respect for physical integrity by covering the patient’s naked body parts during washing, treating the body carefully and hygiene. Hygiene included regularly bathing and for some a clean space for purity of self for religious practice.
Considerate communication
Indirect language when speaking about diagnosis, prognosis and the end of life can preserve dignity. Participants often considered direct language to be too harsh for the patient and also an insult to their belief system. Adaptation of language to the conviction that God/Allah decides about life and death and refraining from judgements about (Islamic) religion was seen as contributing to trust and dignity.
For example, doctor Stephanie (fictitious name) knows that my mother is dying. She tells it to her (mother) in a beautiful way and says to her ‘Yes miss El Amrani (fictitious name), we did our best.. But, everybody has his dossier, for example the dossier is black, you cannot improve it. You will go, but that does not say anything. There are also people that are healthy and that pass away.’ She tells her ‘I am in the next room and my heart might stop.’ She gives her an example, that says, it is less. So everyone will die. Not ‘Only you will die, I will live long, I am healthy and. . .’ [..] Yes someone is healthy and could come under [..] a bus, and dies. That is a good way to slap the person that is dying a little less.. the slapping is hard, but less hard. (Moroccan relative, #22)
Discussion
Main findings
Becoming dependent on others and the frightening prospect of further loss of autonomy and deterioration is hard for all patients. However, for many patients in our study surrendering to God/Allah and being cared for by family is most important for maintaining dignity. The themes can play a concurrent role in valuing oneself as an autonomous being (intrinsic dimension) and valuing oneself in relation to others (extrinsic dimension). For example, by being able to surrender to Allah – accepting the situation, having patience and praying – dignity is maintained in relation to oneself (intrinsic), and enforced by relational and communal recognition (extrinsic) of this practice. When one is not able to surrender, dignity can be impaired on both dimensions. Maintaining autonomy in order to maintain dignity seems more important for patients with a Surinamese background than for Turkish and Moroccan patients, whereas religion seems to play a more important role in the extrinsic dimensions of dignity, as well as functioning as a prescription for surrender, for Turkish and Moroccan patients.
Strengths and limitations
Our findings could have been influenced by the fact that some patients were not aware of the seriousness of their illness. However, by nondisclosure we respected the wishes of the patients and family and were still able to get insight into the meaning of dignity by asking about their dignity in their current situation, the future, and their (hypothetical) last days of life. Additionally, Surinamese participants may have elaborated more on religion or other cultural aspects when interviewed by an ethnic-matched interviewer, who may easier relate to their views and its origins. The strength of this study is that we made use of well-trained ethnic-matched bilingual interviewers with the Turkish and Moroccan participants, thus encouraging them to speak openly about their experiences and feelings in their own language.
What this study adds
The main concepts in our study – religion, being meaningful to others and autonomy – were also found in studies on dignity among patients of majority populations in Western countries,1–5 however, the order of importance and concretisation of these concepts were different. The quality and nature of relationships is important for the dignity of all patients,1,7 however among patients with a migration background, being meaningful to others often meant being cared for by family members and recognition of a social role, whereas in previous studies among majority populations, it often meant not becoming a burden, providing a reciprocal contribution and sometimes performing the act of the social role.1,2,4 Our findings resonate with findings among palliative patients in Taiwan, 22 despite them not being migrated, in which a person’s social role is preserved by children who serve their parents when they are sick. These participants and those in our study originate from collectivist cultures,13,24,26 which may suggest that most persons from collectivist cultures may have similar ways to preserve dignity. However, being a minority population itself could also explain our findings, when people value relationships with group members. Furthermore, our findings may not be relevant for other people with migration backgrounds.
Religion appears to be more important for dignity compared to findings among majority populations in previous studies, and loss of autonomy and the consequences of needing help seems to be less important, especially for the Islamic patients. Religion may serve as a way to maintain dignity and cope with illness,1,2,27 but it might also be that these patients lean towards a specific perspective on dignity, the religious form of human dignity,28,29 meaning that human beings have an intrinsic worth, are sanctified and under protection of God. Protecting this dignity by religious practice and care by others is then more important during illness than other aspects related to rational freedom 28 – such as loss of autonomy, being a burden etcera – often found in studies about personal dignity.1,2,4,5 The differences between the Surinamese and the Turkish and Moroccan groups could be explained by differences regarding religion itself: the importance of religion in daily (communal) life or to follow specific rules; or the religious views on care and the end of life being different. Other aspects could also (additionally) play a role, such as differences in health literacy 30 and different acculturation or integration processes because many Surinamese residents speak Dutch and share the same religious background with the Dutch (Christianity).
Our findings provide insight into how care professionals can preserve the dignity of patients with a migration background in the palliative phase, which includes aspects of dignified care also found in other studies and aspects specifically for patients with a migration background. In the Netherlands, many doctors speak openly about the end of life. 31 Indirect communication about the end of life can establish trust in care professionals, and shows respect for the patient’s view on life. The relational dimension of dignity can be attended by establishing a relationship with the patient and preserving the patient’s relationships with others. Caregivers could discuss with relatives how to shape care for the elderly or loved ones, in such a manner that their values stay intact, for example, by focusing on how they can still provide care and attention when the patient resides in a nursing home. Caregivers could show respect for the patient’s religion by explicitly asking what is important regarding the religion and its rituals. These findings should be incorporated in training for care professionals to provide culture-sensitive palliative care.
Conclusion
To our knowledge, this study is the first on personal dignity in the last phase of life among patients with a migration background. The main difference between our findings and those in other studies is that for these patients, surrender to God or Allah and religious practice, and/or being assisted or cared for by family members is more important for maintaining dignity than maintaining autonomy or not becoming a burden. This implies what is important for dignity is partly culturally shaped. Care professionals should pay attention to these specific differences and needs in diverse patient populations.
Supplemental Material
Reactie_METC_-_niet_WMO_plichtig_A1_17.358_d.d._10_augustus_2017 – Supplemental material for A dignified last phase of life for patients with a migration background: A qualitative study
Supplemental material, Reactie_METC_-_niet_WMO_plichtig_A1_17.358_d.d._10_augustus_2017 for A dignified last phase of life for patients with a migration background: A qualitative study by X de Voogd, MG Oosterveld-Vlug, M Torensma, BD Onwuteaka-Philipsen, DL Willems and JL Suurmond in Palliative Medicine
Supplemental Material
SRQR – Supplemental material for A dignified last phase of life for patients with a migration background: A qualitative study
Supplemental material, SRQR for A dignified last phase of life for patients with a migration background: A qualitative study by X de Voogd, MG Oosterveld-Vlug, M Torensma, BD Onwuteaka-Philipsen, DL Willems and JL Suurmond in Palliative Medicine
Supplemental Material
Topic_list_english – Supplemental material for A dignified last phase of life for patients with a migration background: A qualitative study
Supplemental material, Topic_list_english for A dignified last phase of life for patients with a migration background: A qualitative study by X de Voogd, MG Oosterveld-Vlug, M Torensma, BD Onwuteaka-Philipsen, DL Willems and JL Suurmond in Palliative Medicine
Footnotes
Authorship
All authors contributed to the conceptualisation and design of the study and analysed and interpreted data. XV collected data and drafted the manuscript. MO, MT, DW, BO and JS contributed to the revision of the manuscript. All authors approved the final manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMw (The Netherlands Organization for Health Research and Development) [grant number 80-84400-98-332].
Data
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.