
Abstract
Background:
When patients are likely to die in the coming hours or days, families often want prognostic information. Prognostic uncertainty and a lack of end-of-life communication training make these conversations challenging.
Aim:
The objective of this study is to understand how clinicians and the relatives/friends of patients at the very end of life manage uncertainty and reference time in prognostic conversations.
Design:
Conversation analysis of audio-recorded conversations between clinicians and the relatives/friends of hospice inpatients.
Setting/participants:
Experienced palliative care clinicians and relatives/friends of imminently dying hospice inpatients. Twenty-three recorded conversations involved prognostic talk and were included in the analysis.
Results:
Requests for prognostic information were initiated by families in the majority of conversations. Clinicians responded using categorical time references such as ‘days’, allowing the provision of prognostic estimates without giving a precise time. Explicit terms such as ‘dying’ were rare during prognostic discussions. Instead, references to time were understood as relating to prognosis. Relatives displayed their awareness of prognostic uncertainty when requesting prognostic information, providing clinicians with ‘permission’ to be uncertain. In response, clinicians often stated their uncertainty explicitly, but presented evidence for their prognostic estimates, based on changes to the patient’s function previously discussed with the family.
Conclusion:
Prognostic uncertainty was managed collaboratively by clinicians and families. Clinicians were able to provide prognostic estimates while being honest about the related uncertainty, in part because relatives displayed their awareness of uncertainty within their requests. The conversation analytic method identified contributions of both clinicians and families, and identified strategies based on real interactions, which could inform communication training.
Keywords
Honest prognostic communication with families of patients in the final hours and days of life is important for enabling a good death and for families’ preparedness for that death.
Prognostic uncertainty makes this communication challenging for clinicians and families.
Clinicians provided what we term ‘absolute categorical time estimates’ (suggesting a prognosis of ‘hours’ or ‘days’) and explained how that prognosis was reached, allowing them to reduce prognostic uncertainty without committing to an overly specific timescale.
When requesting prognostic information, relatives helped to relieve the burden of uncertainty for clinicians by alluding to their awareness that prognostication is a subjective judgement.
Clinicians and relatives could be direct about prognosis without explicitly referring to ‘death’ and ‘dying’, as references to time were understood by both parties as referring to prognosis.
This paper identified key practices for communicating prognosis with families of patients at the very end of life, such as explicitly stating the uncertainty while invoking expertise, and using absolute categorical time estimates when providing a prognosis.
These practices could be taught as part of communication training using clips of recordings from real-life interactions.
Background
Clinician communication with patients and their families is a core part of providing high-quality care for people with life-limiting illnesses, 1 and conversations with senior doctors and nurses who provide prognostic information may be particularly sensitive. Patients approaching the very end of life (likely to die in the coming hours or days) often cannot communicate and so relatives need prognostic information to help them make decisions and prepare for the patient’s death. Prognostic communication is linked with the likelihood of relatives being present when the patient dies 2 and how prepared they feel for the patient’s death.3,4
Research on how clinicians communicate prognosis with relatives of patients at the very end of life is limited. Interview studies have explored clinicians’ and relatives’ experiences of prognostic communication, finding clinicians used strategies such as repetition and tailoring, but that they often struggled to balance hope with honesty.5–8 However, there is a limit to the level of detail with which participants’ can recall these interactions, and clinicians’ and relatives’ recollections can differ. 2 To accurately examine these conversations, recording real interactions is required. This approach was taken in a study using conversation analysis to examine recorded interactions between healthcare professionals and people with dementia, in order to inform communication training. The training resulted in improvements in dementia communication knowledge, confidence and behaviour. 9
No previous studies have examined prognostic discussions in real interactions between clinicians and relatives of patients who are imminently dying in a hospice. This study uses audio-recordings of naturally occurring interactions to understand the communication practices used in these conversations.
Methods
This qualitative, conversation analytic study aims to answer the research question: how do senior, experienced clinicians and the relatives and friends of imminently dying patients manage uncertainty and reference time during prognostic discussions?
Setting
Participants were recruited from two inpatient wards at one UK hospice between September 2017 and November 2018. No authors were part of the hospice clinical team.
Participants
Specialist palliative care professionals, including consultants, specialist trainees with at least 3 months’ experience and senior nurses, were eligible to participate. Adult relatives and friends were eligible if they could engage in conversational English and were a main companion of a hospice inpatient judged by clinicians to be approaching the final hours or days of life and lacking capacity (at this point, relatives/friends become the key point of communication for clinicians). Data saturation was not relevant as conversation analysis involves in-depth analysis of small datasets; 10 we aimed to collect 30 recordings of conversations, as this small sample was feasible to collect and allowed a detailed analysis of cases.
Recruitment
Posters were displayed around the hospice, and study information was put in patient rooms to raise awareness of the research. When clinicians anticipated having an eligible conversation, they approached relatives for permission to participate and provided an information sheet. Relatives gave verbal consent to clinicians immediately prior to the conversation. The research team approached relatives for written consent at least 1 day later. Clinicians gave written consent when they joined the study, then again following each recording. If any person present in the conversation did not give written consent within 12 weeks, the recording was deleted.
Data collection
Clinicians audio-recorded conversations, all of which would have taken place whether or not the participants were involved in the research. Participants were told that if they felt uncomfortable, they could stop the recording.
Data analysis
Conversation analysis is an inductive, observational approach using recordings of naturally occurring interactions. This approach examines how social actions are organised and displayed through participants’ turns at talk. 11 A conversation analytic design was selected because it has been used widely in healthcare communication research and allows the identification of recurrent patterns in interactional practices. 12 We take the conversation analytic perspective that ordinary conversations are highly organised and that analysis should be based on evidence within the interaction, rather than external considerations such as broader social structures.13,14 By recording naturally occurring conversations, a conversation analytic design provides a closer representation of reality than more indirect data sources such as interviews.
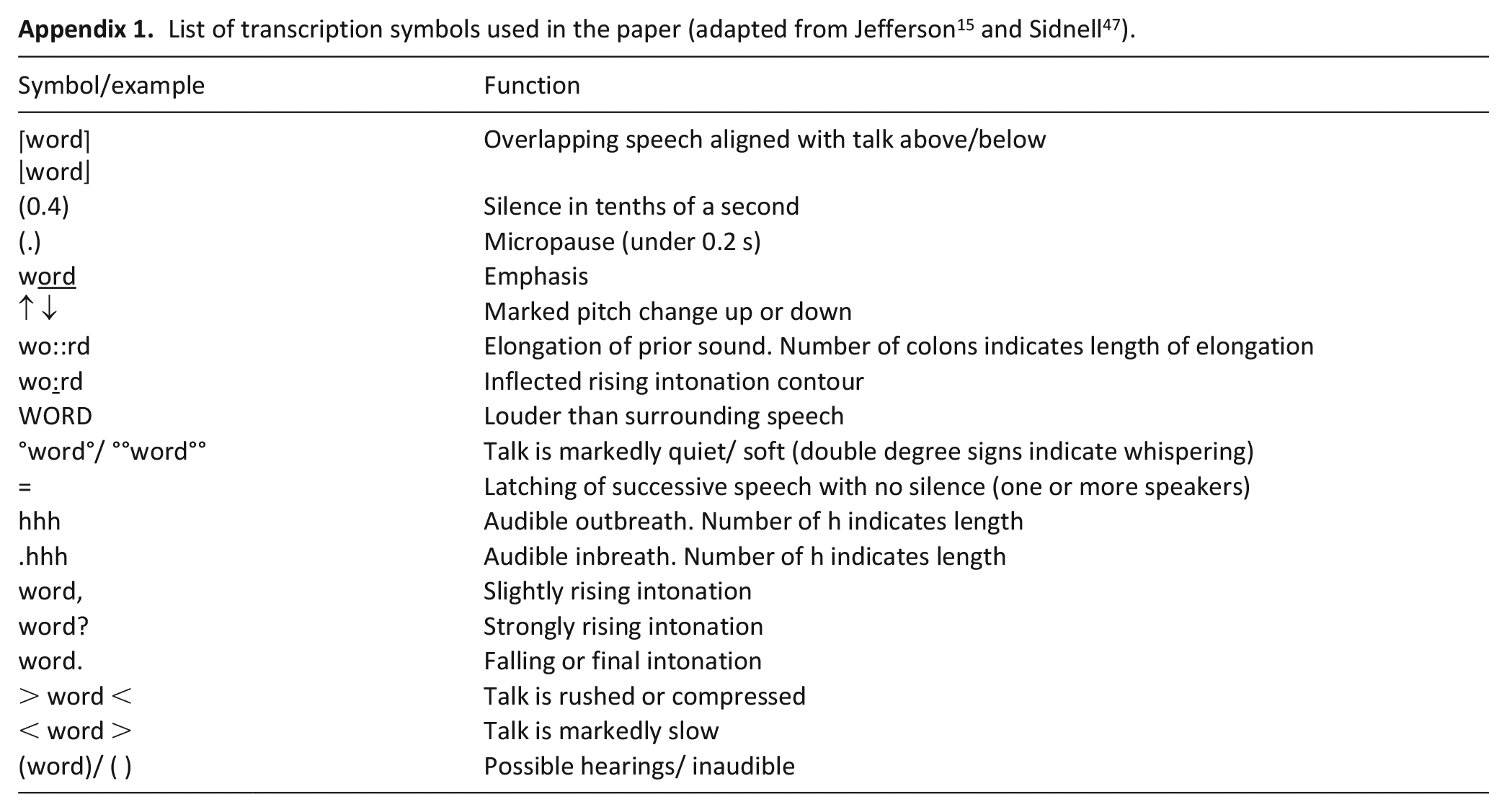
Data were transcribed using the Jeffersonian transcription system 15 (see Appendix 1). This system captures more detail than traditional transcription, including temporal aspects and details of how words are spoken, such as overlap and pitch. All identifiable features have been replaced with pseudonyms.
Extracts were included in the analysis if they were identified by the research team as involving a relative/friend requesting information about when a patient was likely to die (referred to as ‘time estimate requests’), or clinician volunteering this information. Time estimate requests were not necessarily in question formats, but rather performed the action of eliciting prognostic information. To increase rigour, in addition to the core analysis, data were presented in meetings with other conversation analysts.
Ethical issues
Safeguards previously suggested by hospice patients, carers and staff 16 were followed, including not recruiting severely distressed patients/relatives, increasing awareness of the study using posters and allowing participants time to reflect on their participation before providing final consent. Ethical approval was granted by the University College London Research Ethics Committee (Ref. 11519/001).
Results
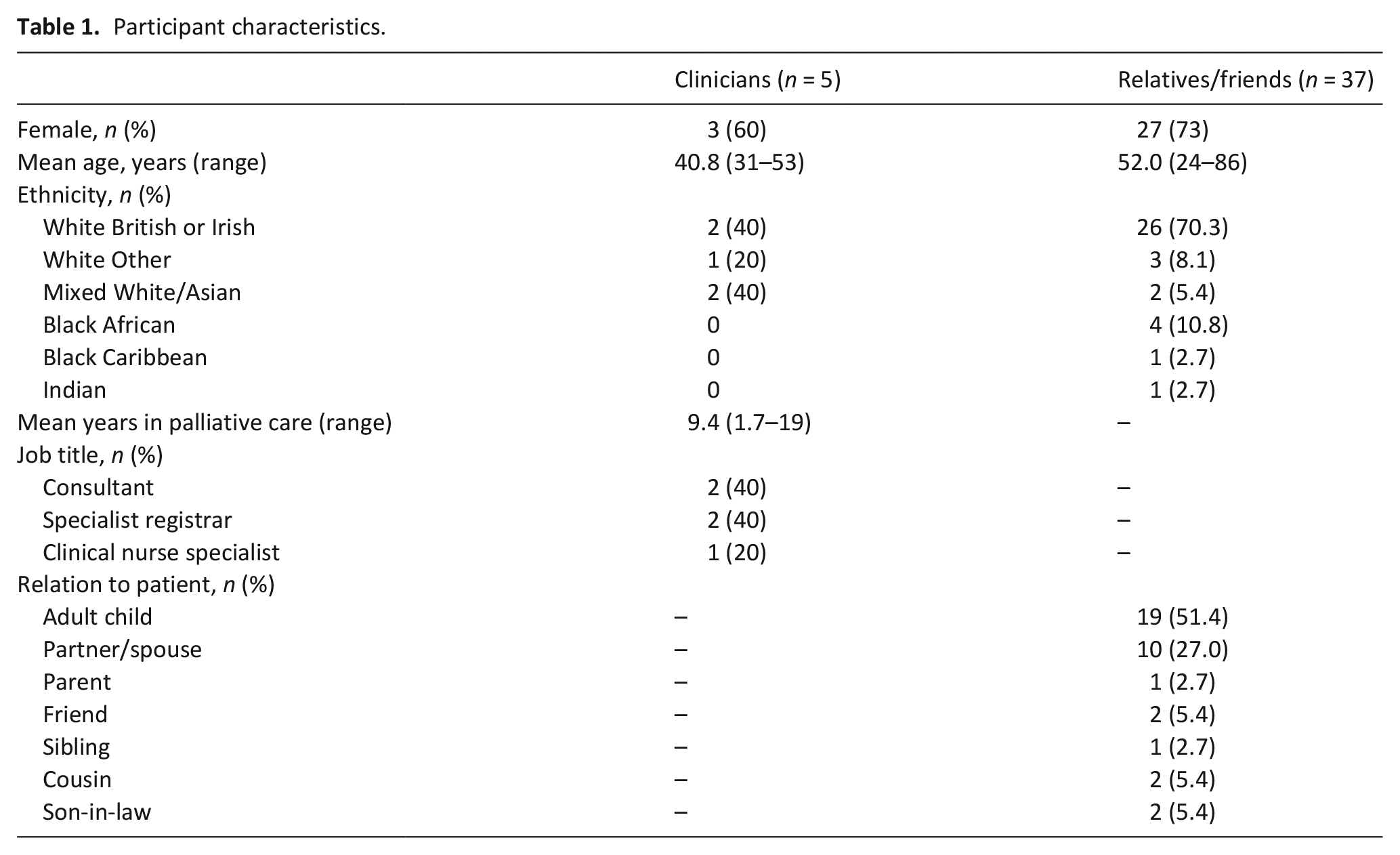
Twenty-nine conversations were audio-recorded, of which 23 involved prognostic discussions. No clear differences were identified between those conversations that did and did not contain prognostic talk; however, families regularly spoke with clinicians and so prognosis may have been discussed previously. The average length of the 23 recordings containing prognostic talk was 18 min 45 seconds (range = 06:11–34:44). These recordings included five clinicians and 37 relatives/friends (see Table 1).
Participant characteristics.
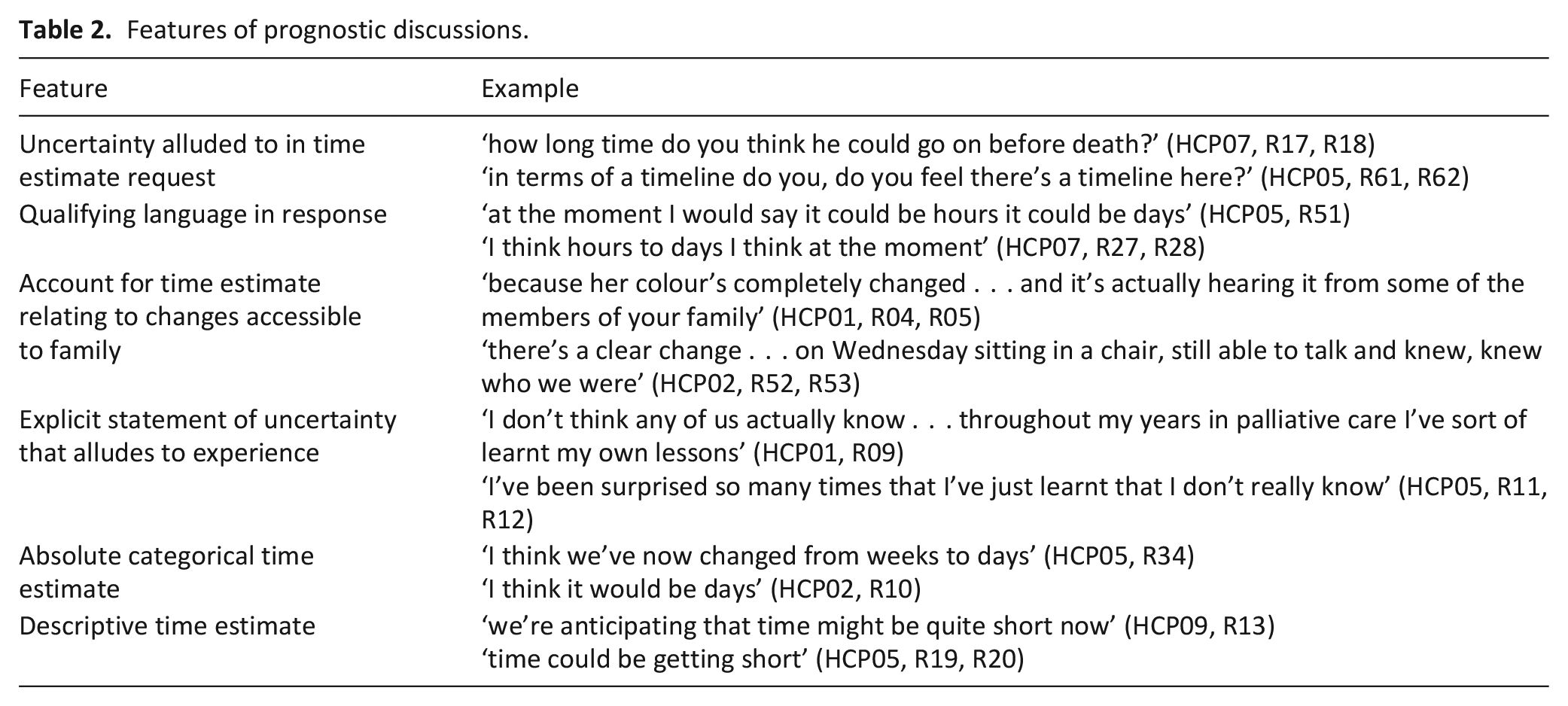
The analysis identified how uncertainty was managed, how time was referenced, and the directness and explicitness of references to prognosis. Extracts from recordings are provided throughout. Table 2 provides further examples of key features from other conversations in the dataset.
Features of prognostic discussions.
Uncertainty in requests and responses
Relatives displayed awareness of uncertainty in their time estimate requests. They somet imes addressed this directly, prefacing their requests with phrases such as ‘obviously timescales are impossible to predict’ (HCP01, R02) or ‘I know it’s only a rough guess but . . .’ (HCP02, R10). More often, though, relatives alluded to this with the wording of their requests. Evidence of this practice is seen in Extract 1, a conversation between a consultant (HCP) and daughter (DAU) of a patient. They had been discussing the patient’s sleepiness when the daughter received a phone call. This extract came immediately after the call.
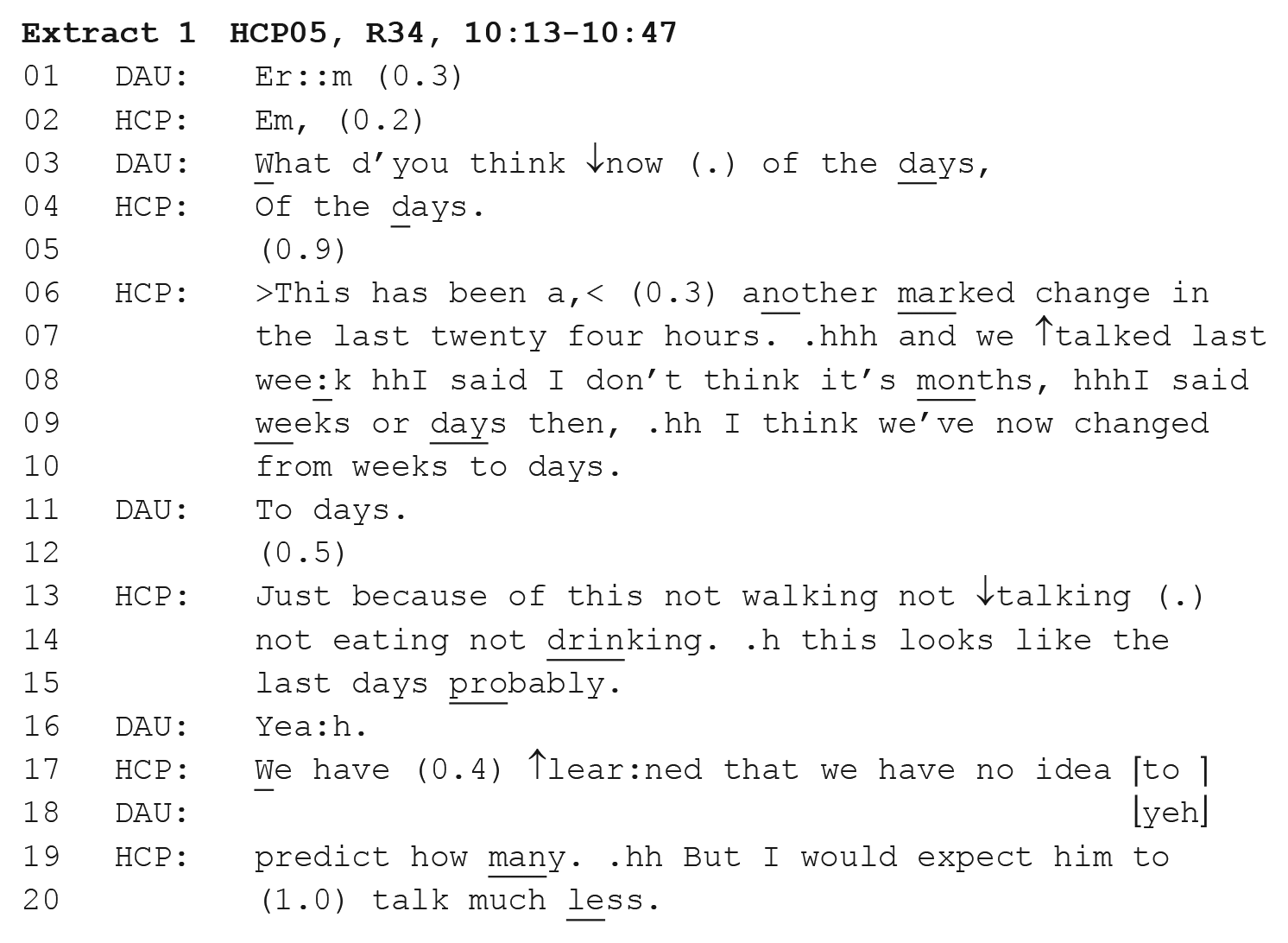
The time estimate request is made at line 3. Here, the daughter asks, ‘what do you think’, framing the request as seeking an opinion not a statement of fact. Opinion-seeking formats of requests were found throughout the dataset, with other relatives asking what clinicians ‘expect’, ‘feel’ or ‘see’. Requests for subjective opinions and explicit displays of awareness of the prognostic uncertainty demonstrate the collaborative nature of these conversations, as relatives effectively gave clinicians ‘permission’ to be uncertain in their answers. The uncertainty alluded to in relatives’ time estimate requests was reflected in clinicians’ responses in the following three ways.
Qualifying language
Clinicians used qualifying language in their prognostic statements, framing their estimates as opinions and reflecting language used in time estimate requests. For instance, in Extract 1, the clinician prefaces their prognostic estimate with ‘I think’ (line 9). In this context ‘I think’ is used tentatively, expressing uncertainty and softening the assertion. 17 Similar language was seen throughout the dataset (see Extract 2 and Table 2), and all estimates were preceded by such qualifiers. Pre-positioned epistemic stance markers are suggested to help recipients align themselves to what is coming. 18 In this case, the qualifying language indicates to relatives in advance that the clinician’s prognostic estimate should be understood as a general idea, not a precise forecast. Following the estimate, the clinician uses the qualifier ‘probably’ (line 15), further downgrading certainty. Cautiousness is also reflected in references to ‘days’ rather than giving a specific number (described in detail in the ‘Time references in requests and estimates’ section).
Explicit statements of uncertainty
In addition to using qualifying language, clinicians made explicit statements about prognostic uncertainty. This is seen in Extract 1 (lines 17–20) as the clinician states ‘we have no idea to predict how many’. Suggesting that the clinician has ‘no idea’ could be a threat to their authority, but it is framed as being based upon the whole medical team (‘we’) and something that has been ‘learned’ from experience rather than due to a lack of expertise. The implication is that a less experienced doctor may give a more specific answer, but the clinician is experienced enough to know this cannot be accurately predicted.
Accounting for the estimate
During prognostic talk, clinicians could not rely solely on their authority or expertise because this was weakened by their uncertainty. They therefore needed to provide evidence of how they reached their conclusions.19,20 Clinicians explained their prognostic estimates to relatives, usually referring to changes in the patient’s functioning. This is seen in Extract 1 as the clinician accounts for the estimate prior to answering in lines 6 and 7 and then following the estimate in lines 13 and 14. The clinician describes how the patient is now ‘not walking not talking, not eating not drinking’. These changes had been established by both the clinician and daughter earlier in the conversation, reflecting a pattern in the data for the evidence presented being accessible to relatives. Relatives’ epistemic access is therefore increased, 21 and the prognostic estimate is presented as somewhat collaborative.
Time references in requests and estimates
In Extract 1, the clinician gave their prognostic estimate in ‘days’. This was typical of the ways prognostic estimates were provided, as clinicians referred to ‘hours’, ‘days’ or ‘weeks’. Raymond and White 22 describe such time references as ‘absolute’; they are shared concepts that anyone can understand (as opposed to event-related, for example, ‘on your birthday’). Raymond and White use the term ‘absolute counted’ to refer to time references that calculate the time until an event in units (e.g. ‘in two hours’). The time references in our data use units but do not specify the number of hours, days or weeks. Instead, they resemble the categories used in prognostic tools such as the Prognosis in Palliative care Study predictor models (PiPS-A and PiPS-B). 23 We therefore refer to these as ‘absolute categorical’ time references. Absolute categorical references have the benefit of giving relatives a unitised prognostic estimate, but do not commit the clinician to a specific time that is likely to be inaccurate.
Absolute categorical time estimates were given in the majority of conversations, but there were exceptions. In four conversations, clinicians responded to time estimate requests with more descriptive time references. The time estimate requests in these conversations did not project a time-based response as strongly. For instance, one relative asked, ‘how do you see the progression with him now?’ (HCP01, R09). In these conversations, the responses involved an extended period of talk in which they discussed changes in patients’ functioning, and what to expect in the coming days. Relatives did not push for a specific time estimate and so clinicians’ prognostic statements remained descriptive. Clinicians therefore matched the specificity of their responses to the specificity of relatives’ time estimate requests.
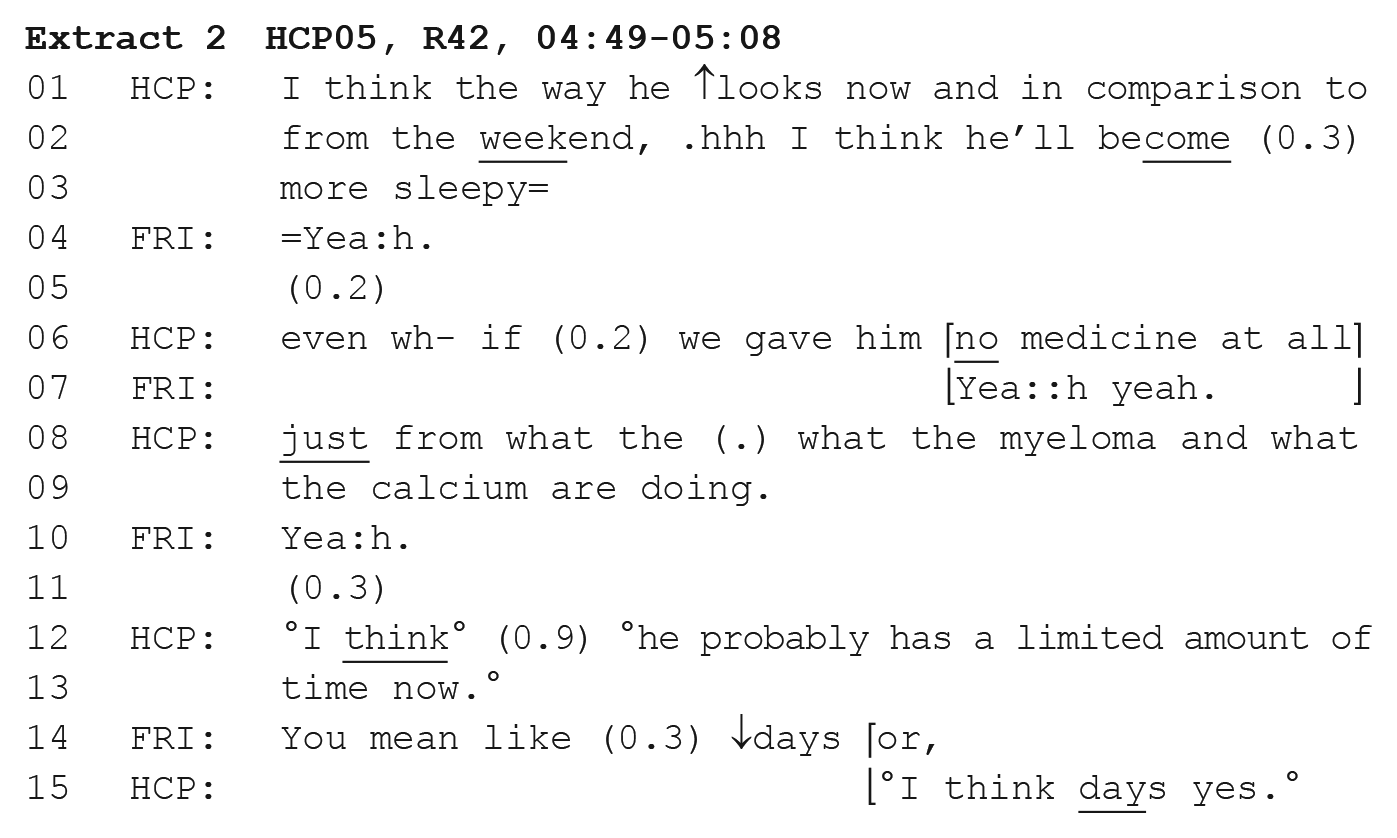
Further examples of descriptive estimates occurred when clinicians initiated prognostication. Relatives initiated prognostic discussions with time estimate requests in 17/23 cases. In the remaining six cases, clinicians made unelicited prognostic statements. These initial statements were descriptive, as demonstrated in Extract 2, a conversation between a consultant (HCP) and friend of a patient (FRI). At lines 12 and 13, the clinician states, ‘I think, he probably has a limited amount of time now’. Descriptive prognostic estimates referenced time being ‘short’ or ‘limited’ or in one case that ‘it does feel very imminent’ (HCP01, R04). In Extract 2, the friend responds to this immediately with a more specific time estimate request, ‘you mean like days or’, and this elicits an absolute categorical time estimate from the clinician.
These initial descriptive prognostic statements from clinicians appear to be used to introduce the topic of prognosis and forecast the upcoming short prognosis. They are therefore more cautious than those elicited by time estimate requests. However, in all six cases of clinicians making unelicited prognostic statements, descriptive estimates were later upgraded to absolute categorical time estimates, either through a request from the relative or the clinician pursuing prognostic talk.
Directness and explicitness of references to prognosis
The ways in which time estimate requests were made and responded to reveal the orientation of relatives and clinicians towards relatives’ rights to prognostic information. When relatives initiated prognostic discussions, requests were generally direct without accounting for why they wanted prognostic information (see Extract 1). Clinicians did not solicit further information from relatives to confirm what they wanted to know. Both relatives and clinicians therefore treated relatives as having a strong entitlement to the information.24,25
Despite the displayed rights to prognostic information and the directness of time estimate requests, explicit references to death were rare. Across the 23 cases of prognostic talk, only one relative used the word ‘death’, none used ‘die’ or ‘dying’ and clinicians only used these terms in two cases. Instead, as demonstrated by Extracts 1 and 2, they referenced time (e.g. ‘of the days’, Extract 1; ‘time may be very short’, Extract 2). However, this did not cause interactional difficulties and references to time were understood by clinicians and relatives as referring to time to death. The context of when and where these conversations took place (within a hospice when the patient was lacking capacity), as well as the interactional context (often following talk about deterioration), allowed enough mutual understanding for there to be no need to explicitly refer to death.
Outside of direct talk about prognosis, there were some explicit references to dying. These occurred when describing the dying process in a general, depersonalised way, or discussing practicalities about the patient’s death. For example, in Extract 3, the consultant (HCP), daughter (DAU) and son (SON) of a patient had been discussing taking their father’s body abroad when he dies.
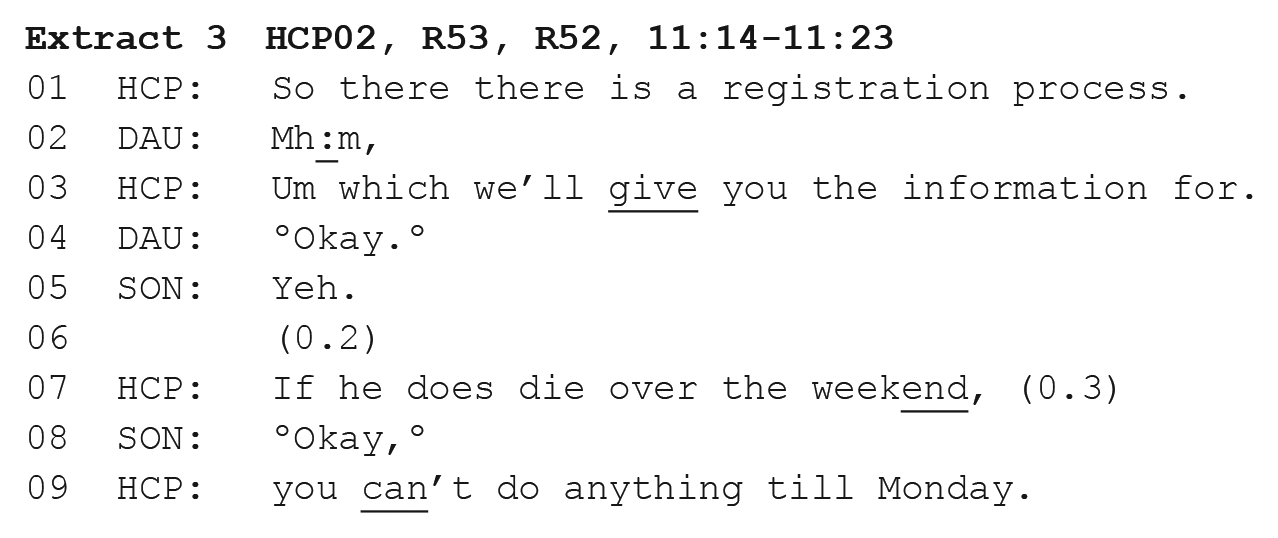
While the HCP directly refers to the patient’s death in line 7, it is in reference to practical arrangements following death and is discussed hypothetically and not in the context of prognostication.
Discussion
Key findings
This is the first study to record conversations between clinicians and relatives of hospice inpatients at the very end of life. Our analysis suggests that uncertainty is managed collaboratively by clinicians and relatives. Relatives often showed evidence that they were aware of prognostic uncertainty and related challenges, supporting previous evidence of this awareness from interview and survey studies.26,27 An example of this was the design of time estimate requests as seeking opinions rather than facts, minimising the apparent burden of the request. 28 A similar finding was seen in Pino and Parry’s study of hospice consultations with patients; 29 however, in that study, there was more work to ‘prepare the conversational environment’ for a prognostic estimate, including doctors checking patients’ existing knowledge and readiness. This difference may reflect relatives’ stronger entitlement to prognostic information and increased clinician responsibility to provide it at the very end of life. Prognostication is an ongoing process 30 and so the content and style of prognostic communication must be adapted over time.
Prognostic uncertainty and a lack of confidence and training are key barriers to clinicians initiating prognostic conversations.31,32 Our findings demonstrate how experienced clinicians negotiated uncertainty in end-of-life conversations with families. Clinicians used qualifying language to present their estimates as opinions rather than precise predictions, and provided descriptive or categorical time estimates rather than a specific timeline. They explicitly stated their uncertainty, presenting their willingness to do so as a result of years of experience. Despite this uncertainty, clinicians provided estimates and justified these with evidence. When a diagnosis (or in this case prognosis) is uncertain, clinicians have been found to back up their assessments with evidence, as the uncertainty demands they provide evidence of how they reached their conclusions.19,20 This use of evidence of changes to patient functioning supports previous findings that clinicians highlight patients’ deterioration to cultivate prognostic awareness.32 –34
When clinicians provided unelicited prognostic estimates, they began with cautious, descriptive statements before upgrading to absolute categorical estimates. This reflects a responsibility for clinicians to ensure families have a clear understanding of patients’ prognoses at the very end of life, as well as a general preference for speakers to upgrade from descriptive references to more specific ones in everyday conversation.35,36
During prognostic discussions, direct references to death and dying were rare. Instead, within the conext of these discussions, references to time were understood by both clinicians and relatives as relating to prognosis. Outside of prognostic discussions, these terms were used when referring to practical arrangements following the patient’s death. This reflects findings from paediatric palliative care consultations where death was only made explicit when not referring to the specific individual or where death was ancillary to the focus of the discussion. 37
Practical implications
Communication guidelines suggest that clinicians should provide prognostic information and explain uncertainty.38,39 The findings in this paper build on these guidelines and enable us to provide concrete strategies for doing so. First, it is possible for clinicians to state explicitly that prognosis is uncertain without losing their status as ‘experts’. They can do this by explaining that their experience has shown them that prognosis is uncertain and describing the changes they have seen that led them to the prognostic estimate. Using absolute categorical estimates such as ‘days’ allows clinicians to provide a prognosis without giving a precise estimate. Therefore, while probabilistic estimates may be slightly more accurate than categorical over the course of the illness trajectory, 40 absolute categorical estimates may be more useful to relatives at the very end of life. Further research is needed to explore how clinicians use these terms and whether there is a shared understanding of what they mean between clinicians and relatives.
Guidelines also suggest avoiding euphemisms and to instead use terms such as ‘death’ and ‘dying’ where appropriate. 39 In this study, clinicians rarely used these terms during prognostic discussions, but did not avoid them completely. The analysis revealed that clinicians can be open about death without referring to it explicitly, particularly when families themselves have used implicit language in their time estimate requests. They can do this by referencing time and monitoring families’ language for signs of shared- or misunderstanding. Previous studies have shown that some family members felt clinicians were too vague or avoided prognostic talk,6,41 while others felt that they could be blunt.42,43 This strategy may therefore be particularly helpful to cultivate prognostic awareness in a sensitive manner.
Palliative care experts have expressed a need for evidence-based guidance on end-of-life communication with caregivers. 44 In response to this need, strategies identified in this paper could be taught in communication training, using clips from real interactions to demonstrate useful practices (consent was obtained to use recordings in this way). Using recordings of actual interactions has benefits over traditional communication models, as they provide more realistic examples than using hypothetical situations in role-plays. 45
Limitations and future research
This study was based in a hospice and findings may not be generalisable to other settings. The patients being discussed had lost capacity and were in the final days of life, meaning families may have had increased prognostic awareness. In settings such as intensive care units where there is more focus on treatment, this awareness might be reduced. Therefore, while it was not necessary to use words like ‘dying’ in the current study, more explicit language may be needed in other settings. Further research into discussions of prognosis in different settings is needed.
In order to identify examples of good practice in communication, this study focused on senior clinicians from one hospice. However, excluding less experienced clinicians meant that we could not assess how experience may affect communication practices. While the dataset covered over 430 minutes of conversation, further recordings are needed in different hospices and with a range of healthcare staff to gain a fuller understanding of prognostic discussions.
It is possible that participating in research may have changed clinicians’ and relatives’ behaviour. A previous study found some hospice patients, carers and staff had concerns that video-recording could make them feel uncomfortable. 16 However, in a study of hospice patients who had previously had a consultation video-recorded, none felt the recording made them less willing to talk. 46 Furthermore, in the current study, audio-recording was chosen over video because it is less intrusive than video-recording.
Conclusion
Our analysis revealed the ways relatives, friends and clinicians discuss prognosis in conversations at the end of patients’ lives. The majority of relatives and friends were aware that prognosis was uncertain and displayed this to clinicians. Terms such as ‘dying’ did not necessarily need to be used explicitly, as references to time being short were understood by families as referring to prognosis. This paper identified strategies used by clinicians to manage uncertainty, including explaining how a prognosis was reached, using absolute categorical time estimates and presenting statements about the uncertainty as coming from experience and expertise. These strategies could be implemented as part of end-of-life communication training for clinicians.
Footnotes
Appendix
List of transcription symbols used in the paper (adapted from Jefferson 15 and Sidnell 47 ).
| Symbol/example | Function |
|---|---|
| ⎡word⎤⎣word⎦ | Overlapping speech aligned with talk above/below |
| (0.4) | Silence in tenths of a second |
| (.) | Micropause (under 0.2 s) |
| w |
Emphasis |
| ↑ ↓ | Marked pitch change up or down |
| wo::rd | Elongation of prior sound. Number of colons indicates length of elongation |
| wo |
Inflected rising intonation contour |
| WORD | Louder than surrounding speech |
| °word°/ °°word°° | Talk is markedly quiet/ soft (double degree signs indicate whispering) |
| = | Latching of successive speech with no silence (one or more speakers) |
| hhh | Audible outbreath. Number of h indicates length |
| .hhh | Audible inbreath. Number of h indicates length |
| word, | Slightly rising intonation |
| word? | Strongly rising intonation |
| word. | Falling or final intonation |
| > word < | Talk is rushed or compressed |
| < word > | Talk is markedly slow |
| (word)/ ( ) | Possible hearings/ inaudible |
Acknowledgements
We would like to thank all relatives, friends and clinicians who took part in the study. We are grateful to our co-investigators: Adrian Tookman, Philip Lodge, Ruth Parry, Barbara Wood and Dori-Anne Finlay. We would like to acknowledge Marie Curie for providing funding for the Marie Curie Palliative Care Research Department.
Authors’ note
R.A. is a researcher in conversation analysis with a psychology background. S.B. is a conversation analytic researcher and speech and language therapist. P.S. is a palliative care researcher and consultant. J.L. is a palliative care researcher with a psychology background.
Author Contributions
All authors were responsible for the study concept and design. R.A. was responsible for the acquisition of the data; R.A. analysed and interpreted the data with input from S.B.; R.A. drafted the paper; P.S., J.L. and S.B. made revisions. All authors read and approved the final version of the manuscript.
Data management and sharing
Data sharing is not possible as it would compromise participant confidentiality and we do not have permission from participants to share full transcripts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Marie Curie Chair in Palliative and End of Life Care grant (Grant MCCC-FCH-13-U). P.S.’s and R.A.’s posts are supported by the Marie Curie Chair in Palliative and End of Life Care grant funding; J.L.’s post is supported by the Marie Curie core and programme grant funding (Grants MCCC-FCO-16-U and MCCC-FPO-16-U). The funder played no role in the collection, analysis and interpretation of data, in the writing of the report or in the decision to submit the article for publication. The Division of Psychiatry is supported by the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
Research ethics and consent
Ethical approval for the study was granted by the UCL Ethics Committee on 18 July 2017 (Ref. 11519/001). All participants provided written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.