
Abstract
Background:
Volunteers make a major contribution to palliative care but little is known specifically about hospital palliative care volunteers.
Aim:
The aim of this study was to understand the role and experience of hospital palliative care volunteers.
Design:
Systematic review and narrative synthesis.
Data sources:
CINAHL, Embase, Medline, PsycINFO, PubMed and three dissertation databases were searched from inception to June 2019. A forward and backward search of included papers in key journals was also undertaken. Records were independently assessed against inclusion criteria by authors. Included papers were assessed for quality, but none were excluded.
Results:
In total, 14 papers were included. Hospital palliative care volunteers were mostly female, aged above 40 years, and training varied considerably. Volunteers faced unique challenges in supporting dying patients due to the nature of hospital care, rapid patient turnover and the once-off nature of support. Volunteer roles were diverse, with some providing hands-on care, but most focused on ‘being with’ the dying patient. Volunteers were appreciated for providing psychosocial support, seen as complementary to, rather than replacing the work of health professionals. Given volunteers were often required to work across multiple wards, establishing positive work relationships with health professionals was challenging. Divergent views about whether the volunteer was part of or external to the team impacted volunteers’ experience and perceptions of the value of their contribution.
Conclusion:
Hospital palliative care volunteers face unique challenges in supporting terminally ill patients. Volunteer support in hospital settings is possible and appropriate, if sufficient support is available to mitigate the challenges associated with complex, high-acuity care.
The demand for palliative care and hospice services worldwide is increasing, as a result of an ageing population and rising rates of chronic illness.
Volunteers are known for their positive contribution to hospice and palliative care services worldwide.
Volunteers have traditionally provided support in administrative and patient-related roles across a variety of settings, including at home, in stand-alone hospices and specialist palliative care units, and through palliative care services and organisations.
Hospital palliative care volunteers have unique training and support needs, such as orientation and training specific to each ward area, such as intensive care or oncology.
Hospital palliative care volunteers were most appreciated for the psychosocial support provided to terminally ill patients, an aspect of their role considered to complement, not replace the role of health professionals.
Working across multiple hospital wards and high patient turnover made establishing ongoing relationships with patients and staff difficult.
There were divergent views about whether the hospital palliative care volunteer was part of the healthcare team.
The hospital setting creates some challenges for the hospital palliative care volunteer, uniquely different from other care settings.
Further work is needed to more clearly define the relationship between health professionals and volunteers and to measure the impact of the hospital palliative care volunteer.
Introduction
The demand for palliative care and hospice services worldwide is increasing, including in inpatient hospital settings1,2 due to ageing and rising rates of chronic illness. 3 Worldwide, high proportions of people receive palliative care in, or die within, hospital settings. Nearly 30% of deaths in the United States, 4 54.8% of deaths in the United Kingdom 5 and 56.8% of deaths in Canada 6 occur in inpatient hospital settings. Rapid patient turnover 7 and a priority focus on early discharge 8 mean that even when terminally ill, people may not remain in hospital for long. Furthermore, with increasing specialisation, terminally ill patients may remain under the care of a non-palliative care specialist physician, related to their diagnosis, not specialist palliative care. Australian acute hospital deaths data demonstrated that only 22% of patients who died in hospital were under specialist palliative care, with others receiving end-of-life care from specialists from other fields, such as oncology, cardiology and general medicine. 9
Volunteers are known for their contribution to hospice and palliative care services, yet data related to the number of volunteers in hospice and palliative care services across countries are of poor quality, reported as gross volunteer numbers rather than as a proportion per population. 10 What is known is that there are nearly half a million hospice and palliative care volunteers in the United States 11 and 125,000 in the United Kingdom. 12 Palliative care volunteers have traditionally been associated with specialist palliative care provision, providing support in administrative and patient-related roles13,14 across a variety of settings, including at home, in stand-alone hospices and specialist palliative care units. What is less common is the support volunteers may provide to those who receive care in inpatient hospital settings.
Palliative care volunteers in home care, community and stand-alone hospice settings have been the focus of some research interest over the years, focusing on the nature of the volunteer role, 15 the experiences and motivations of volunteers, 16 the impact of volunteering on the volunteer, 17 ethical challenges associated with volunteering18,19 and volunteers’ interactions/relationships with professional staff. 20 A recent systematic review confirmed that the volunteer role was distinctly different from that of paid staff, such as health professionals, characterised by the social nature of the role and volunteer–patient relationships, across home care, hospice and palliative care unit settings. 13 Volunteers’ contribution through direct patient care has been shown to be beneficial to patients and families, 21 but again, the review included all care across home, hospice, inpatient or outpatient services and specialist palliative care settings. While the emerging role of the death doula across care settings, including inpatient hospital settings, has recently received attention, a review indicated that death doulas were not always linked with palliative care or hospice services; they may have previous health professional training and may also receive payment for services provided; 22 thus, their role is considered different to palliative care volunteers.
Recently, there has been attention given to developing the role of the palliative care volunteer within inpatient hospital settings. For example, the HelpForce initiative in the United Kingdom was established to promote the role and value of volunteering in diverse roles, including palliative care, within NHS hospitals. 23 Inpatient hospital settings have distinctive differences to other home, community or stand-alone hospice or palliative care services. This likely means the nature of palliative care volunteers’ role in inpatient hospital settings is also different. To date, no reviews have been conducted to systematically and comprehensively examine the role and experience of the palliative care volunteer in inpatient hospital settings.
Methods
Aim
The aim of this review was to examine the research evidence to answer the following question: What is the role and experience of palliative care volunteers in inpatient hospital settings?
Design
A systematic review and narrative analysis was used, with reporting guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses: The PRISMA Statement. 24 Narrative synthesis was deemed most appropriate due to the descriptive nature of the research question and heterogeneity of included studies and data. 25
Inclusion and exclusion criteria
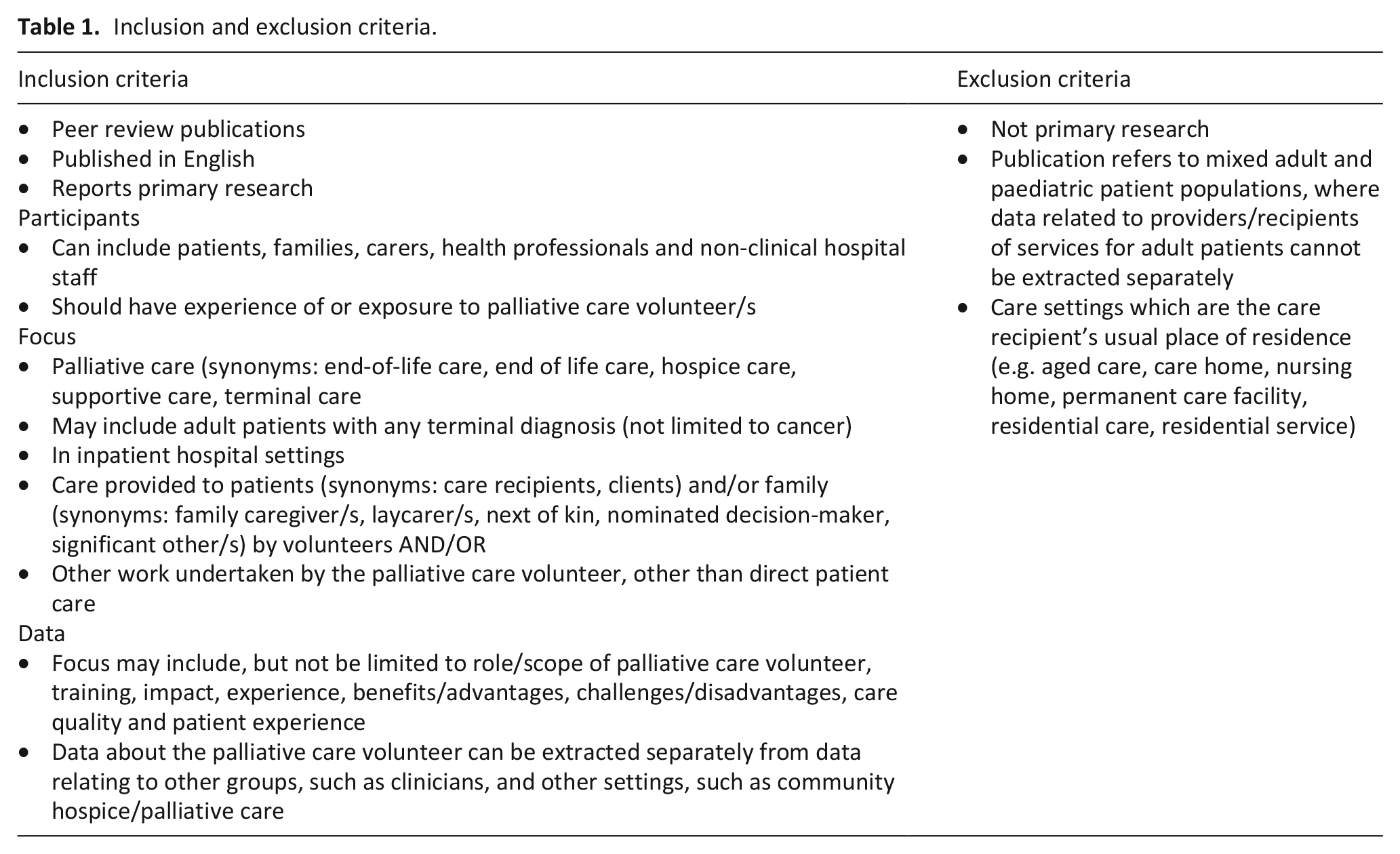
The focus of this review was palliative care volunteers in inpatient hospital settings. This concept and context guided the development of inclusion and exclusion criteria (Table 1).
Inclusion and exclusion criteria.
Search terms
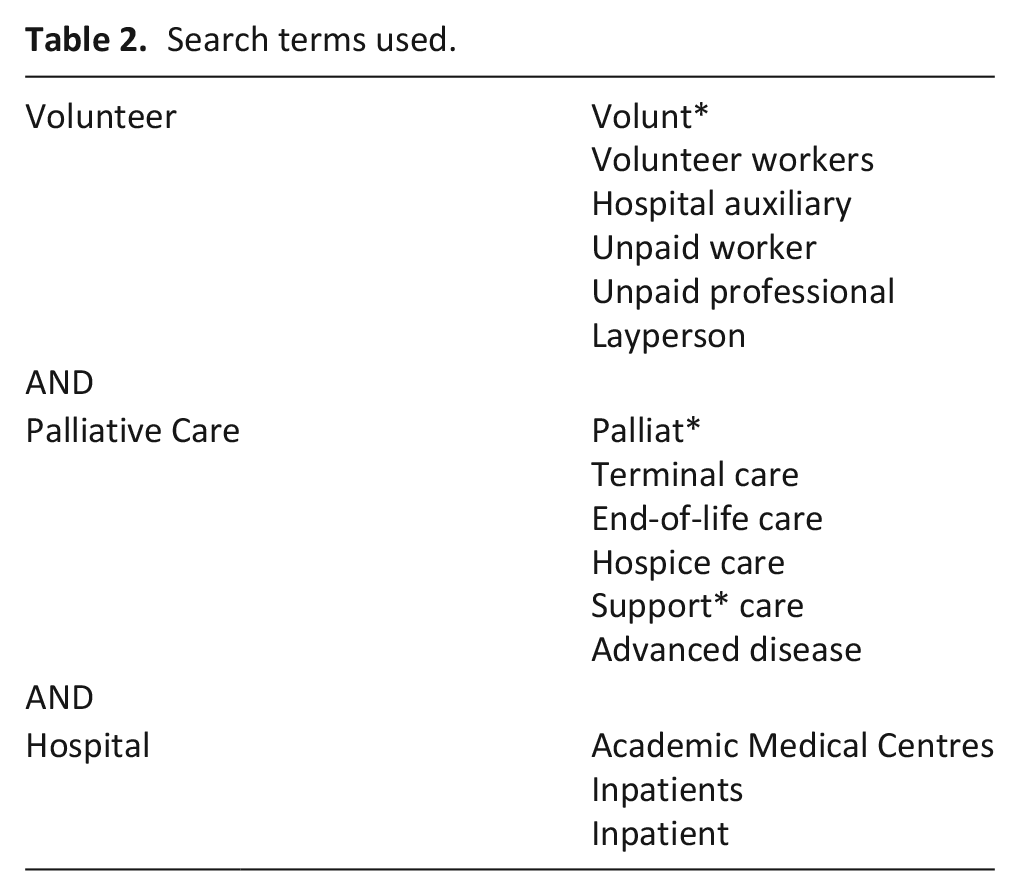
Database-specific search terms, MeSH headings and synonyms to describe three concepts of ‘volunteer’, ‘palliative care’ and ‘hospital’ were used with Boolean operators in the search for literature (Table 2). The full search strategy for each database is provided in Additional file 1.
Search terms used.
Search strategy
A search of Cumulative Index Nursing and Allied Health (CINAHL) Complete, Embase, Medline, PsycINFO and PubMed databases was undertaken, since inception of the databases till June 2019. ProQuest Dissertations and Thesis Global Search, Networked Digital Library of Theses and Dissertations (NDLTD) and Open Access Theses and Dissertations (OATD) databases were searched for theses related to the topic. A simultaneous manual search of key journals in the field, including Palliative Medicine, BMC Palliative Care and American Journal of Hospice and Palliative Medicine was undertaken to ensure all suitable publications were located. A backward search of the reference lists of all included papers and forward search of those papers citing included papers were undertaken.
Search outcome
All records retrieved from the database searches were downloaded into EndNote (Version X9) and de-duplicated. These records were uploaded to Covidence, a web-based software platform that streamlines the production of systematic reviews and allowed authors to independently screen citations, undertake text review and together, resolve reviewer conflicts. 26
Quality assessment
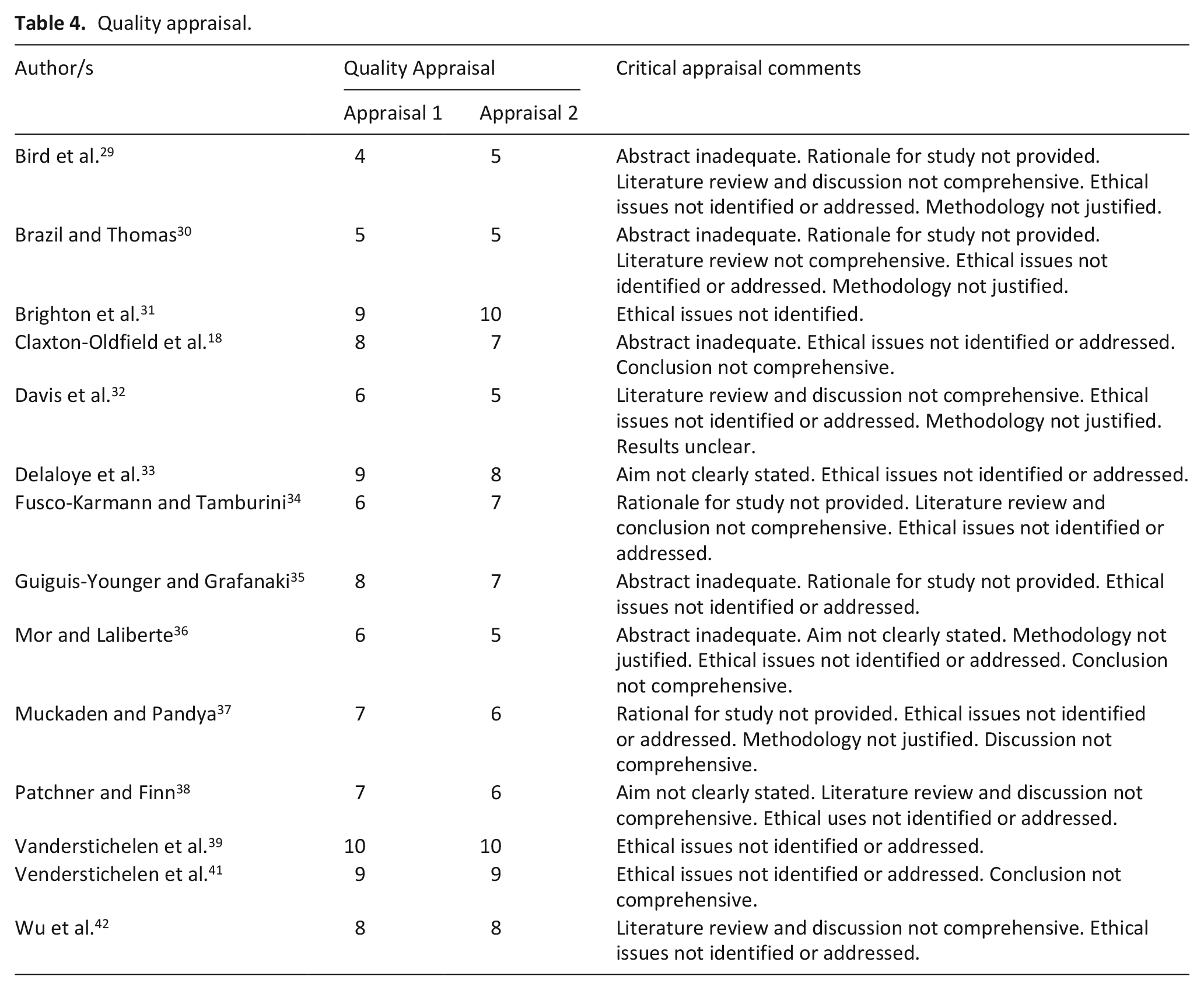
The quality of each included paper was independently assessed by the authors using an evaluative framework suitable for qualitative and quantitative research. 27 Given the small number of papers meeting the inclusion criteria, an a priori decision was made not to exclude papers based on quality appraisal scores, but instead to use the quality assessments to describe the quality of the research evidence in this area.
Data extraction
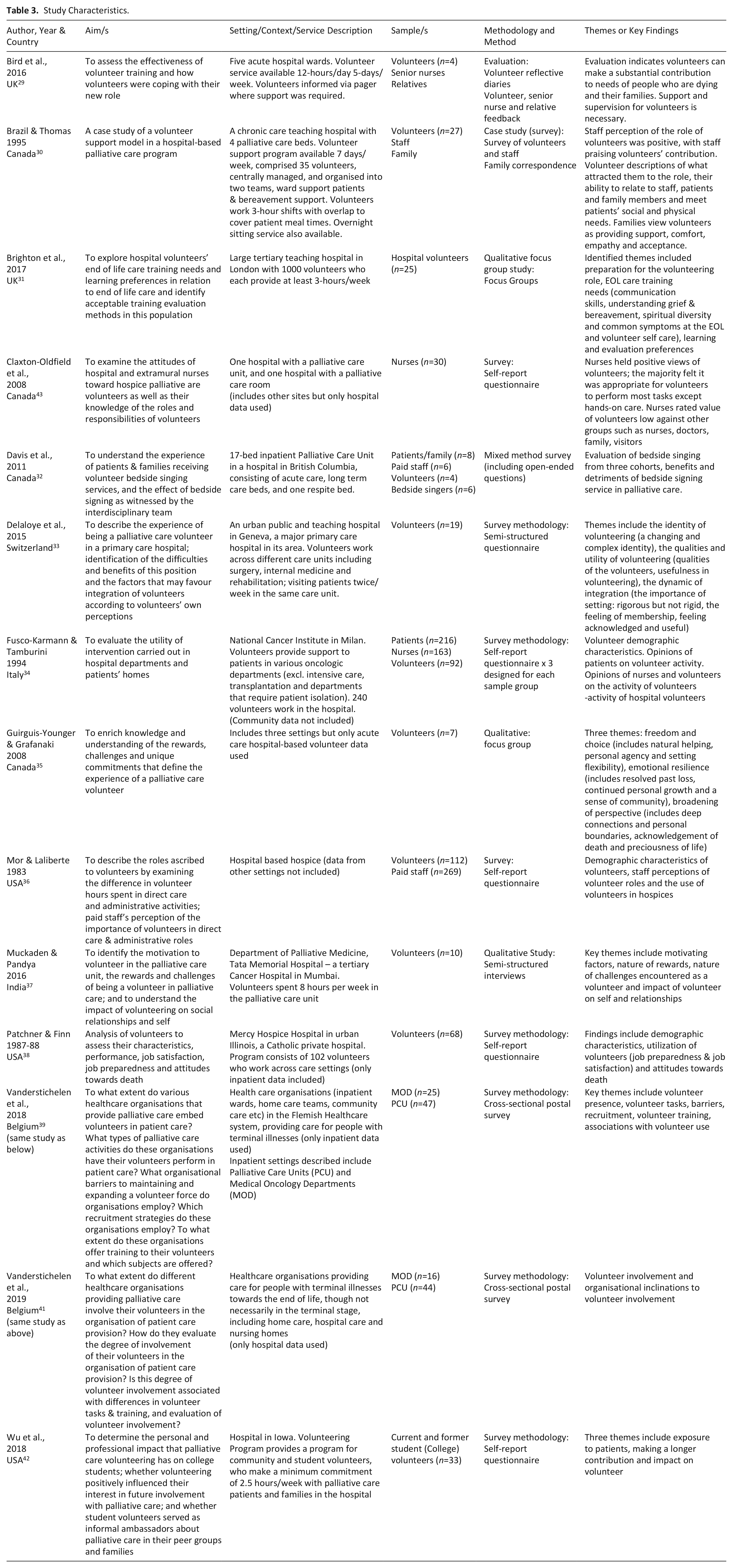
Data were extracted and charted into an evidence table detailing key features, including authors, year of publication, country, purpose/aim, setting and context, sample, study design, data collection method/s and key findings (Table 3). Where a study included data related to other settings, only hospital data were extracted.
Study Characteristics.
Data analysis and synthesis
Narrative synthesis was used to synthesise and report the findings. Narrative synthesis has been described as an approach that relies primarily on the use of words to explain and summarise synthesis findings. 25 Given the heterogeneity of data between the included studies, this was considered the most appropriate approach. Findings were initially grouped according to theme and/or sample group by one author (M.J.B.), then reviewed by the second author (C.W.), discussed and revised until both authors agreed were agreeable. In relation to synthesising data describing the role of inpatient hospital palliative care volunteers, a post hoc decision was made to use Swanson’s middle-range theory of caring 28 to guide synthesis. The first author (M.J.B.) then synthesised the findings narratively, with the second author (C.W.) confirming the synthesis.
Results
The outcome of the database search is presented in Figure 1.
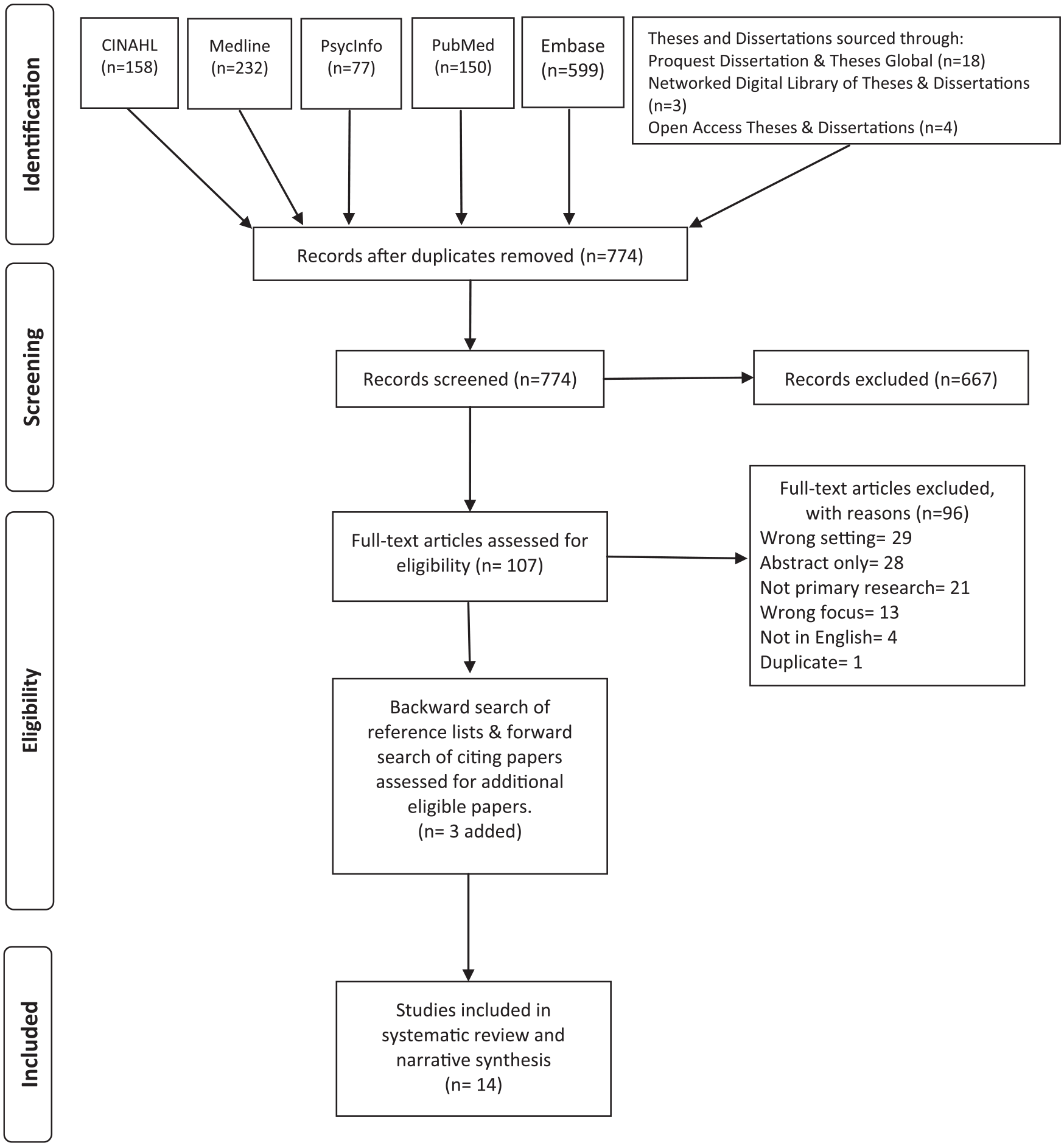
Search outcome.
Characteristics of included studies
In total, 14 papers met the inclusion criteria and were included in this review, 2 from the same project. Included studies and their characteristics are summarised in Table 3. Studies published between 1983 and 2019 were conducted in Belgium (n = 2, reporting different aspects of the same study), Canada (n = 4), the United States (n = 3), the United Kingdom (n = 2), and one each from India, Italy and Switzerland. Study designs included survey (n = 9), qualitative (n = 3), mixed method (n = 1) and an evaluation study (n = 1). Quality scores for included studies ranged from 4 to 10 (maximum possible score 11), with both reviewers independently appraising each paper similarly (Table 4).
Quality appraisal.
Five studies describe palliative care volunteer services in dedicated palliative care wards or beds within hospitals,30,32,37,38,43 and nine report volunteer roles/services provided across multiple wards of hospitals.29,31,33–36,39,41,42 Eight studies report data collected from palliative care volunteers,29–31,33,35,37,38,42 one reports data collected from health professionals, 43 two studies report service-level data from the one study39,41 and three report data from multiple sources, including volunteers, health professionals, patients, family and service-level data.32,34,36 When combined, these studies provide data from 422 volunteers, 468 health professionals, 220 patients and 4 family members.
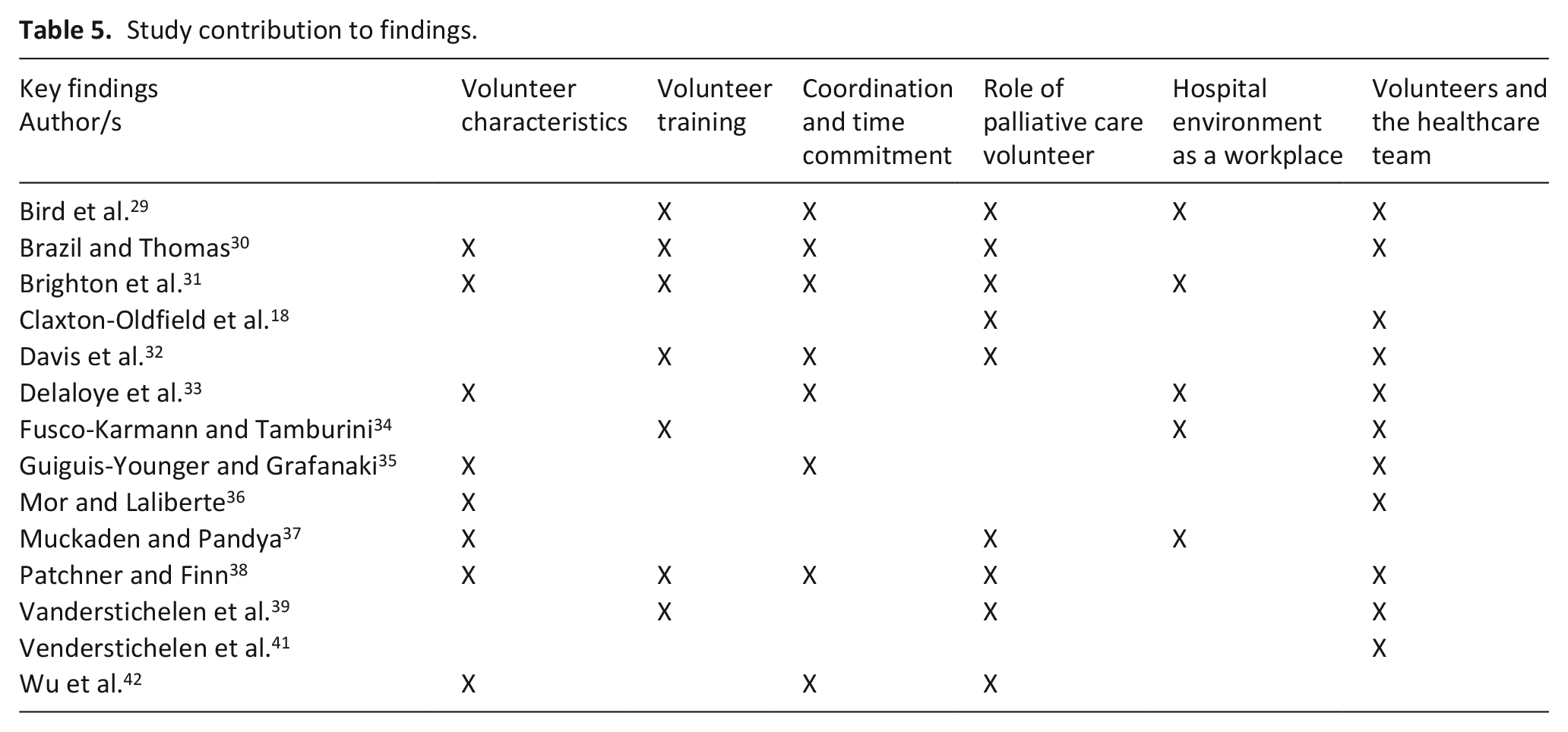
First, the characteristics of volunteers, training provided and coordination of volunteer services in hospitals are described. In subsequent sections, the unique role of palliative care volunteers in hospitals and the important context of the hospital as the volunteers’ workplace are presented (Table 5).
Study contribution to findings.
Characteristics of volunteers
Volunteers were primarily female and aged above 40 years. The overall mean age of volunteers, as reported in three studies,30,33,38 was 52 years, with combined age range as reported across four studies30,31,33,38 of 15–82 years. Other studies reported volunteers’ age as 45 years and above, 37 or with more than one-third (36.6%) aged between 41–64 years. 36 For those studies that reported the gender of volunteers,30,31,33,35–37,42 76.5% of volunteers were female.
Volunteer training
Seven studies29–32,34,38,42 provide detail about the duration of initial training provided to hospital palliative care volunteers, ranging from one full day, estimated at 7.5 h, 32 to 32 h of training completed over 2 months. 38 In two studies, initial training is followed by either an opportunity to shadow an experienced volunteer for a 2.5 h long shift before volunteering independently 42 or an apprenticeship lasting 15–30 days, where the new volunteer worked under the supervision of an experienced volunteer. 34 Some studies described ongoing education for volunteer in the form of bi-monthly group meetings, annual half-day workshop and programme retreat, 30 group volunteer supervision meetings every 15 days and attendance at monthly meetings where information was provided and skills developed through an in-service programme. 34
When describing hospital palliative care volunteer training programmes, none of the studies identified the content of training that specifically applied to inpatient hospital settings. However, several studies reported that training programmes included a focus on the volunteer role, including the principles of palliative care29,34 and hospice, 38 principles and governance of volunteering,29,34 volunteer needs, position and roles within care, 39 death, dying, grief and bereavement,30,34,38 and spirituality.29,31 Training also extended to topics relevant to volun-teering in the inpatient hospital setting, including hospital ward-specific orientation and additional education about the ward,30,42 universal precautions, including the management of patients with infectious conditions, 30 hand hygiene, 39 manual handling,31,39 the adult and the young patient in the hospital and teamwork. 34 Factors specific to understanding patient needs and care included pain and symptom control,29,30,34 physical care, 30 including assisting with eating and drinking, 31 listening and communication.29–31,34,38,42
Coordination and time commitment of volunteer services
Of the eight studies that described the coordination of volunteer services, six reported that the volunteer service was coordinated by one person, such as a volunteer coordinator,35,38 volunteer manager, 29 volunteer designated as team leader, 30 a psychologist 33 or music therapist. 32 Volunteers were described as working 2.5- to 4-h shifts29,30,38,42 with one study describing a volunteer service that operated 7 days/week from 10 am to 9 pm 30 and another provided services 5 days/week from 8 am to 8 pm. 29 In one study, volunteers were informed through pager of where support was required across the hospital, 29 and in another, volunteer hours overlapped to correlate with patient meal times, and overnight volunteer services were available when a patient’s death was imminent. 30 In other studies, volunteers attended their allocated ward twice per week, 33 or weekly for a duration of 2 32 or 3 h/week.30,31
Role of palliative care volunteers in hospitals
Nine studies describe the role of hospital palliative care volunteers.29–32,37–39,42,43 Descriptions of volunteer roles encompassed patient-related and administrative roles, underpinned by the need to maintain patient confidentiality and exercise discretion when working in sensitive situations. 29 The patient-related roles were mapped on to Swanson’s middle-range theory 28 of caring, which describes five distinct caring processes: (1) Knowing, (2) Being With, (3) Doing For, (4) Enabling and (5) Maintaining Belief, as a way of providing a logical structure to the synthesised data. Knowing describes striving to understand, in terms of the meaning for another, centring on the one being cared for, with a goal of understanding the reality of the other. 28 Several studies describe the role of volunteers listening to the needs of patients29,30,38 and families, 38 also described as a ‘listening ear’. 42
Being With describes the process of being emotionally present for another, sharing feelings and conveying ongoing availability; being there. 28 Volunteer roles were described as including showing understanding and compassion appropriate to individual needs, 29 being a supporter and friend, 30 engaging in supportive counselling for patients and families, 37 singing for patients and families at the bedside 32 and being a supportive presence.37,42 Reading to patients, spending time with patients and family and taking photos of patient and family hands as mementos for family were also described. 42
Doing For is about doing for another what he or she would do for themselves, if possible. 28 This process accounted for the largest number of descriptors of the role of the volunteer, with a focus on practical supports. 43 The volunteer role was described as including communicating concerns about the patient, family or carer to staff 29 and signalling the need for communication between patients, families and health professionals, 39 assisting with discharge, 31 guiding and transporting patients through the hospital.37,39 Running errands, 38 helping with chores and phone usage, doing laundry 39 and food preparation38,39 were also described. In the study by Vanderstichelen et al., 39 hands-on care tasks, such as assisting with meals and feeding,30,38,39 providing back and/or heel rubs, 30 helping with hygiene, turning and repositioning, toileting, dressing, and assisting patients to take medication, were also described, yet there were differences in the degree to which volunteers were able to perform these tasks. Despite the breadth of tasks decribed, two studies indicate that there was not clear consensus on the appropriateness of vounteers undertaking these tasks. Organisational data indicated that volunteers in palliative care units within hospitals were more likely to perform hand-on care tasks, such as assisting with hygiene, toileting and repositioning, than volunteers located in medical oncology departments. 39 Similarly, despite hands-on patient care being described as part of the volunteer role, in one study, half of the health professional respondents felt it was not an appropriate task for volunteers. 43
Enabling is about providing information and explanations, offering emotional support in the form of validating the person’s feelings. 28 In some studies, the role of volunteers extended beyond listening and being with, to include activities focused on supporting and validating the person. Volunteers conducted support group meetings, sought opportunities to raise awareness about cancer, 37 provided guidance and support to patients by signposting them to the appropriate professional, 29 provided psychosocial and spiritual care to patients and families,31,39,43 and bereavement support for families. 43
Maintaining Belief involves holding the other in esteem, believing in them and sustaining faith. 28 Only one study’s description of the volunteer role aligned with maintaining belief. Volunteers who provided singing at the bedside of patients, according to the patient’s choice and spiritual direction were described as offering support to patients in transition, struggling with living or dying. 32
Administrative or non-patient-related roles described in the studies, and which did not map onto Swanson’s theory, included coordination of volunteer services, 30 clerical duties, 38 conducting awareness programmes on important days, such as World Hospice Day, fundraising, 37 acting as a hospital guide and promoting the volunteer companionship service among health professionals. 29
The hospital environment as a workplace
The unique nature and challenges working in a hospital setting, either across multiple wards or a dedicated palliative care unit in a hospital was described in five studies. Despite volunteers feeling satisfied with their role compared to their expectations,
33
there were inherent challenges in providing a volunteer service across a whole hospital site: . . . We need a better system to let us know what wards need us and to let us know where the patients are. (volunteer 3)
29
The necessity for constant adaptation to the shifting context of acute care wards made the volunteer role complex.
33
Time and space limitations due to the large volume of patients made maintaining continuous follow-up a challenge
37
and was enough to result in volunteers leaving the service: We have so few volunteers [in intensive care], because they either don’t stay because it is a very traumatic situation, or it’s not what they were expecting. (volunteer, intensive care)
31
Rapid patient turnover and short length of stay in hospital meant ongoing relationships with patients was not always possible, increasing the pressure on them to make an impact: He died a few days later, but I just kept thinking in my mind, I hope the last conversation I had with him, it was good. (volunteer, surgical)
31
The brevity of relationships also meant volunteers felt ill-prepared: So I just said ‘Hi, how are you doing today?’ Like that. And then he started crying. (volunteer, chaplaincy)
31
Others described the negative consequences of not having any preparatory/background to guide their patient interactions: Uh, it was just . . . had I known how serious the prognosis was, I would have handled the situation differently. So you know, it’s very difficult going in cold sometimes because you can end up really putting your foot in your mouth. (volunteer, chaplaincy)
31
The lack of specific guidance or preparation for volunteers to help them understand what is needed and what they were able to do with the terminally ill person may help to explain how health professionals perceived their usefulness. Volunteers were ranked most positively for their role in providing psychosocial support, but less positively for more practical activities, such as diverting activities, help in transport and help in nourishment; potentially related to volunteers’ knowledge of the patient and their specific needs. 34
Volunteers and the healthcare team
Health professionals and volunteers from 11 studies provided data describing the role of hospital palliative care volunteers as part of the healthcare team. Organisational data from Belgium indicated that hospital palliative care volunteers were more often utilised in hospital-based palliative care units than medical oncology wards.
39
Organisational barriers to volunteerism in included finding suitable volunteers, the time investment and workload required to integrate volunteers into the organisation.
39
Despite data suggesting volunteers were regularly informed on how patient care was organised, volunteers were rarely invited to contribute to how patient care was organised, nor did volunteers have decision-making rights.
41
These findings suggest that hospital palliative care volunteers were viewed as providers of specific care, not viewed as equal to members of, or part of the healthcare team. Issues related to interaction between volunteers and members of the healthcare team were also identified: What I find a bit complicated is that the healthcare team changes all the time, so that I am always dealing with new people. (volunteer 10)
33
I wish the staff were more accommodating. (volunteer 1)
29
After the greetings, I’m left to myself. You have to try to understand by yourself how the care unit works. (volunteer 19)
33
The frequent change in teams, volunteers’ perceived difficulty in integrating their role with the healthcare team and lack of continuity with patients led to a sense of invisibility and difficulty in evaluating the role: . . . to accept this impression of usefulness, the difficulty to appraise the effects of the visit for the patients . . . (volunteer 19)
33
Volunteers themselves, however, reported an appreciation for the positive relationships with other volunteers and health professionals in the hospital setting,
38
describing the quality of the welcome received in wards at 8 out of 10.
33
Similarly, other volunteers expressed appreciation for being part of a community: I very much appreciate that we work as a team . . . it takes some time to develop a relationship with the nursing staff, but once you have that, you are definitely part of a team. (volunteer, acute care)
35
. . . It takes time to become integrated . . . What I like most is the complicity and discussions I can have with the healthcare team. We help each other. . . It is very often constructive. (volunteer 18)
33
The view of health professionals about volunteers, however, was mixed. Health professionals generally had positive views of volunteers
43
and their contributions.
30
Volunteers were considered helpful often, specifically in providing moral support to patients and saving time for health professionals.
36
Similarly, nurses rated volunteers positively for the psychosocial support they provide and their role in providing information.
34
When reflecting on volunteer usefulness, health professionals also commented: Just them being there really works and it’s a great bonus. (Sister 3)
29
I find it very useful when a patient has nobody. (Sister 2)
29
In terms of ‘value’, however, volunteers were ranked 8 out of 10, behind nurses, family, pharmacists, doctors, spiritual advisors, social workers and friends,
43
indicating that their contribution to the healthcare team was not highly valued. The impact of volunteer bedside singers also received mixed reviews.
32
While some health professionals describing the volunteer bedside singers as ‘very calming and soothing’, others commented: . . . [their] energy often feels/seems awkward. . . they have not integrated smoothly into the team. I would like to see them engage with all the team and include nursing.
32
The negative feedback was justified by comments to indicate the volunteers ‘crowd the place’ 32 and needed to work with health professionals to review ‘the timing of the visit’, 32 suggesting that for volunteers to be perceived positively, they must not impede other ward or health professional activities.
Discussion
This systematic review has identified that the role of hospital palliative care volunteers is uniquely different to other hospice and palliative care settings due to the short or once-off nature of interactions with terminally ill patients. The volume of research evidence in the included studies that describe volunteers’ actions of ‘being with’ terminally ill patients highlights not only the importance of this aspect of volunteer work but also exemplifies the aspects of volunteers’ role they found most satisfying. Ideally, the patient–volunteer relationship would be determined as a result of a process of specifically matching volunteers to patients according to measures of personal compatibility 39 and consideration of relational chemistry. 44 But in the hospital setting, the rapid patient turnover associated with hospitals 7 and limited time volunteers have with each patient and shift, means the opportunity to build relationships with patients, founded upon ongoing and close contact like in other palliative care settings 40 is likely not possible. Even so, providing one-off or short-term support to a terminally ill patient is likely better than no support at all.
The review identified a lack of clarity about the volunteer’s role in inpatient hospital settings; and whether volunteers were part of, or complementary to the healthcare team. Previous research has demonstrated that volunteers appreciate having a clearly defined role, underpinned by orientation and initial and ongoing training opportunities to support their role and guide actions.40,45 In the hospital environment, however, given that volunteers are required to work across multiple wards, role descriptions and training must also consider the nuances and unique differences of various wards to give volunteers optimal opportunity to contribute in a meaningful way. This includes careful consideration of the relationship between the volunteer and the health professional team and how they may best work together to benefit the patient.
The relationship between volunteers and the healthcare team was not always clear, leading to lack of role clarity for volunteers. The need to feel included and to belong to a team, 46 and to feel that one’s work is viewed as important 47 was key to volunteers and contributes to positive perceptions of their role and work environment. 46 Feeling included fosters positive outcomes,16,48 leads to positive attitudes and behaviours, such as altruism, affective commitment and task performance 49 and contributes to a sense of belonging, feeling appreciated and a sense of control. 16 These factors, underpinned by organisational ‘nurture’ characteristics, are modifiable to improve volunteerism in organisations. 48 The findings also suggest, however, that there is discord between volunteers and health professionals about the contributions of volunteers. Health professionals most appreciated volunteers when their role was deemed not to replace, but rather to complement the role of health professionals. Hence, clearly specifying the role and scope of the volunteer, and that volunteers do not replace paid workers, 50 such as health professionals, is important. Volunteers occupy a unique space, different from that of health professionals and family caregivers, contributing to the uniqueness of their role in supporting the terminally ill person 40 and this provides volunteers with a unique position from which to support to the terminally ill person. When their focus was on providing psychosocial support, the findings indicate volunteers’ contributions were more readily accepted by health professionals, affirming their role as complementary to that of health professionals. Given the importance of person-centred responsive care, it need not be solely provided by health professionals to have impact. 44
Strengths and limitations
This systematic review is the first to examine the role of the palliative care volunteer in inpatient hospital settings. While more is known about volunteers working in home-based, community and stand-alone hospice and palliative care settings, this paper provides evidence to specifically explicate the unique role, perceptions and challenges of the palliative care volunteer in inpatient hospital settings. The search was comprehensive and broad in terms of databases, year range and study design, to ensure the search captured all relevant research evidence, published in English. It is possible that relevant research published on other languages may have been missed.
Given that only 14 papers met the inclusion criteria, none were excluded on the basis of quality scores. As a result, the findings of this review were derived from research papers of diverse quality. Of note, none of the included papers explicitly identified and addressed ethical issues, and in half of the papers, the methodology was not justified. Given many of the papers were conducted in single settings, with small samples, and without overt controls for confounding factors, the generalisability of the findings on the role and experience of the palliative care volunteer in hospital settings is limited.
Recommendations for future research
It is important to note that multiple studies were identified during the screening process, which were likely to have met the inclusion criteria, but were abstracts.51–57 This suggests that there may be more activity/initiatives related to hospital palliative care volunteers than was included in this review. Second, given the moderate quality of research papers included in this study, comprehensive description of the literature, clear and detailed methodology, including identification and consideration of how ethical issues were addressed, should be prioritised for future research publications in this area.
It was not possible from this review to ascertain or measure the impact of hospital palliative care volunteers. Given that more people are dying in inpatient hospital settings, it is, therefore, likely that the need for hospital palliative care volunteers is also likely to increase. Future research should seek to measure the impact of hospital palliative care volunteers on terminally ill patients and their families, health professionals and the healthcare team.
From the included studies, only four family members were included in one study. Given that family members may either receive direct support from volunteers or by proxy of the care provided to the dying person, further research is also necessary to explore the experience of families in receipt of direct or proxy care from volunteers, as well as measure the impact of hospital palliative care volunteers on family members.
Future research must be robust, use strong research designs to answer research questions. Ideally, further research would seek to measure cost-effectiveness, efficacy and impact of hospital palliative care volunteers. Mixed method designs that include several outcome measures should be used with larger and multiple sample groups are needed to build the understanding of the role and experience of hospital palliative care volunteers.
Conclusion
Volunteers working in inpatient hospital settings face unique challenges associated with supporting terminally ill patients in settings/wards where the focus of care is not palliative care. Given the nature of hospital care and patient turnover, there was limited opportunity for volunteers to build ongoing relationships with patients. Rather, volunteers were more likely to provide once-off support to terminally ill patients, with little to no prior preparation or information about the terminally ill person to guide the support provided.
While health professionals most appreciated for the psychosocial support volunteers provided for patients, there was no clear and definitive description of the volunteer’s role in inpatient hospital settings, increasing the complexity of the volunteer’s experience. Despite the desire for positive and inclusive working relationships with health professionals, volunteers were not always viewed as part of the healthcare team, with health professionals preferring volunteers not to provide hands-on care, but rather provide psychosocial support that is complementary to the work of health professionals.
What this study adds?
This study provides evidence of the uniquely different experience and role of hospital palliative care volunteers, compared to the role of palliative care volunteers in other settings. Volunteers were most appreciated for the psychological support they provide to terminally ill patients, even when the hospital environment and context limit opportunities to develop ongoing therapeutic volunteer–patient relationships. The evidence is less clear about whether the volunteer is viewed as part of the healthcare team or complementary to it.
Supplemental Material
Additional_File_1.__Database_search_strategy_and_outcomes_17072019 – Supplemental material for ‘It’s not what they were expecting’: A systematic review and narrative synthesis of the role and experience of the hospital palliative care volunteer
Supplemental material, Additional_File_1.__Database_search_strategy_and_outcomes_17072019 for ‘It’s not what they were expecting’: A systematic review and narrative synthesis of the role and experience of the hospital palliative care volunteer by Melissa J Bloomer and Catherine Walshe in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank Caroline Gibson, Faculty Librarian at Lancaster University, UK, for her invaluable assistance with the database searching.
Authorship
Both authors (M.J.B. and C.W.) contributed equally to the conception of review, review design, database search strategy, review and selection of studies, quality appraisal and synthesis of data. M.J.B. led manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Endeavour Executive Leadership Award from the Australian Government Department of Education and Training, awarded to the first author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.