
Abstract
Background:
Constipation is a major problem for many older adults, more so for those who are receiving specialist palliative care. However, limited research reports the subjective experiences of constipation, despite evidenced differences between the healthcare professional and patient/carer perspective.
Aim:
The main aim of this study is to explore the experience of how constipation is assessed and managed within specialist palliative care from the patient, carer and healthcare professional perspective.
Design:
Exploratory, qualitative design, utilising focus groups and interviews, and analysed using thematic analysis.
Setting/participants:
Six focus groups with 27 healthcare professionals and semi-structured interviews with 13 patients and 5 family caregivers in specialist palliative care units across three regions of the United Kingdom.
Results:
Constipation impacted physically, psychologically and socially on patients and families; however, they felt staff relegated it on the list of importance. Lifestyle modifications implemented at home were not incorporated into their specialist palliative care plan within the hospice. Comparatively, healthcare professionals saw constipation solely as a physical symptom. Assessment focused on the physical elements of constipation, and management was pharmacologically driven. Healthcare professionals reported patient embarrassment as a barrier to communicating about bowel care, whereas patients wanted staff to initiate communication and discuss constipation openly.
Conclusion:
Assessment and management of constipation may not yet reflect the holistic palliative care model. A focus on the pharmacological management may result in lifestyle modifications being underutilised. Healthcare professionals also need to be open to initiate communication on bowel care and consider non-pharmacological approaches. It is important that patients and families are supported in self-care management, alongside standardised guidelines for practice and for healthcare professionals to facilitate this.
Constipation is a major problem for many older adults, more so for those who are receiving specialist palliative care.
The patient and caregiver perspective are largely unreported in the literature, despite differences between the healthcare professionals and patient’s reports of the impact and severity of constipation.
Constipation impacts on patients and families physically, psychologically and socially.
Healthcare professionals’ focus on the physical symptoms of constipation during assessment, leading to an overreliance on pharmacologically driven management.
Non-pharmacological techniques used by patients and families at home were not incorporated into the plan of care in this setting, potentially impacting on overall self-care management.
A holistic approach to constipation care is required to meet the needs of patients and families.
Healthcare professionals should routinely offer advice on non-pharmacological interventions alongside pharmacological interventions to patients as part of their plan of care.
It is important that patients and families are supported by healthcare professionals to take control of self-management and to more effectively use their own strategies.
Introduction
Constipation is a major problem, and significant concern, for many older adults. It is determined by unsatisfactory defecation due to infrequent stools, difficulty passing stools or the sensation of incomplete emptying. 1 Factors significantly related to the presence of constipation include a diagnosis of cancer, bed restriction and the need for personal assistance for toilet visits. 2 National and European clinical guidelines for the management of constipation for patients receiving palliative care3,4 identify key clinical messages including an essential comprehensive assessment, ongoing preventive measures, pharmacological and non-pharmacological management strategies of equal importance and particular attention during opioid therapy or in suspected cases of intestinal obstruction.
While approximately one-third of older adults are affected by constipation, 5 this increases to over two-thirds of people admitted to specialist palliative care.6,7 However, a longitudinal study found that admission to a specialist palliative care unit did not improve constipation symptoms, and prevalence significantly increased in the palliative care unit. 8 Specialist palliative care is offered within hospices in the United Kingdom for patients throughout the trajectory of a terminal illness, focused on improving quality of life through pain and symptom management, supporting the individual and their loved ones and advising on practical concerns. 9 Eighty percent of patients accessing specialist palliative care inpatient services in the United Kingdom have a diagnosis of cancer and typically are admitted as a planned series of short stays. 10
Evidence regarding the impact of constipation on patients is inconsistent and lacking within specialist palliative care. While a systematic review of four papers on older people’s experiences suggests physical, psychological and social impact, 11 data from an Australian Palliative Care database suggests that most palliative care patients were not unduly distressed by constipation. 12 Furthermore, underestimation of symptom intensity by healthcare professionals leads to increased risk of inadequate treatment, 13 and research in chronic pain has demonstrated incongruence between the patient experience and the healthcare professional’s assessment in the perceived importance and severity of constipation. 14 Limited research studies explore the patient/carer perspective of this distressing symptom and concomitant comparison to the healthcare professional perspective. To provide a holistic insight into the assessment and management of constipation, this article explores the experiences of the patient/carer and healthcare professional of constipation in specialist palliative care.
Methods
Design
An exploratory qualitative design was used with reporting guided by the Standards for Reporting Qualitative Research framework. 15 Focus groups were conducted with healthcare professionals to understand the experiences of assessing and managing constipation and individual or dyad interviews with patients and carers to capture individual experiences.
Setting
Focus groups with healthcare professionals were conducted in three specialist palliative care inpatient units across Northern Ireland, England and Scotland, with, on average, 22 beds and admitting approximately 329 patients each year. Patient/carer interviews were conducted in one specialist palliative care inpatient unit in the United Kingdom.
Sampling
A purposive sample of healthcare professionals was invited to participate if they met the inclusion criteria (Table 1). Data were collected until theoretical sufficiency was achieved, which was identified as the point at which a sufficient range, complexity, subtlety, resonance and external validity had been reached to allow the research team to address the aim of the research.16,17 The research lead identified potential participants and provided study details and a consent form. If interested, healthcare professionals were asked to return their completed consent form to the researcher.
Inclusion/exclusion criteria.
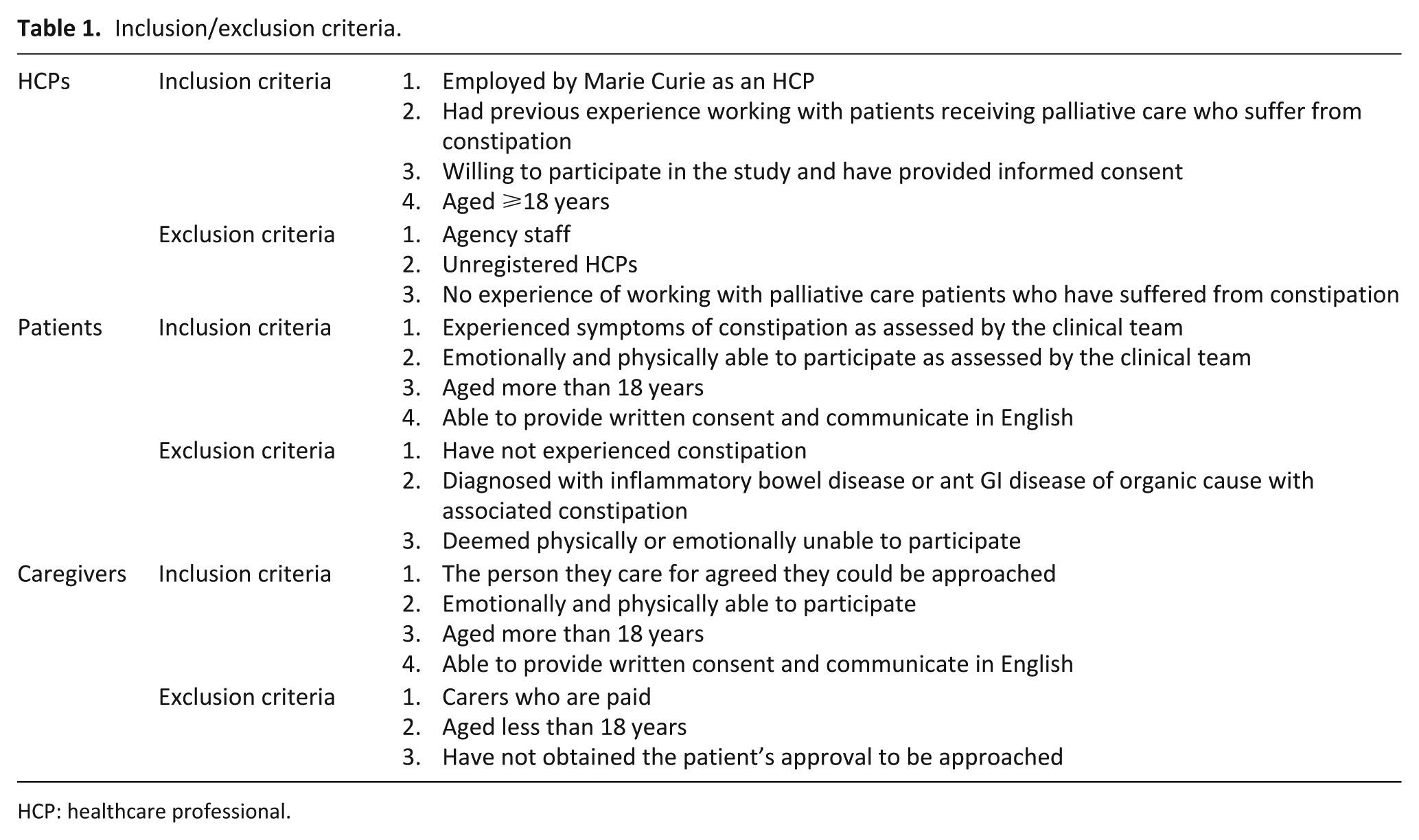
HCP: healthcare professional.
Healthcare professionals within the hospice who were external to the research team acted as gatekeepers to screen patients. A purposive sample of patients experiencing constipation and admitted to a specialist palliative care unit in the United Kingdom, and their informal caregivers, were invited to participate (Table 1). Data were collected until theoretical sufficiency was achieved.16,17 Eligible patients were approached by a nurse with study details and a consent to be contacted form. If they consented, they received a phone call from the Researcher (D.M.), and the study was explained. Patients were also asked if their main carer could be approached. If consent was obtained, they were contacted to undertake a joint or independent interview.
Data collection/processing
Focus groups were held from November 2016 to January 2017. Each focus group included between three and six participants to allow for discussion on variation of experience relative to the topic. 18 Focus groups were held by the researcher (D.M.) within the specialist palliative care units during work hours and, with permission, digitally recorded. A note-taker was present to capture information and observations arising from the discussion. A demographic questionnaire was completed before the focus group. The focus group schedule (Appendix 1) focused on experiences of constipation assessment and management from the perspectives of healthcare professionals. Each focus group proposed to last 45–60 min.
Interviews with patients/carers were undertaken by the researcher (D.M.) from February to July 2017. Interviews were arranged at a time convenient to the participant. An interview schedule (Appendix 1) was developed from the core elements of the UK National Clinical Guidelines on constipation 3 to capture the participant’s understanding and experiences of constipation assessment and management. Interviews were expected to last 15–30 min, including a demographic questionnaire and were audio recorded with the participant’s permission.
All audio files were password protected and sent for transcription outside the research team. Once transcribed, a 10% randomly selected sample was checked for transcription errors.
Data analysis
An emic viewpoint was collected from patients/caregivers with lived experience of a phenomenon, whereas an etic perspective was collected from people who are experts and stakeholders in the area but not directly living with the phenomena, that is, healthcare professionals. 19 Therefore, analysis of data was undertaken sensitively with consideration of how constipation was interpreted by the participant who was experiencing the symptom compared to the participant who was treating the symptom. A thematic analysis was undertaken by D.M., S.M. and F.H., guided by Braun and Clark’s framework. 20 Patient/Carer and healthcare professional data were analysed independently, and selected quotes were indicative of a range of views presented by participants. Triangulation occurred through the integration of focus group and interview data during the interpretation stage. 21
Rigour
In line with Lincoln and Guba’s 22 recommendations, steps were taken to increase trustworthiness of the findings. A reflexive journal was maintained. The researcher was from a non-nursing background and had no prior connections with the specialist palliative care unit or staff. Relationships were established through multiple points of communication. A thick description supported transferability, an audit trail determined dependability, and credibility was established by feeding back to participants, and analysing contradictory/negative cases.
Ethics
Full University Research Ethical Approval was obtained (Application 16/WM/0352), and hospice research governance approval was obtained at each site. The study was explained to participants in writing and verbally and informed consent collected. Participants were informed about their right to withdraw, confidentiality and the disclosure of sensitive information. Lone worker and distress protocols were in place, and a support pack was provided to all participants. Anonymity ensured no participant could be identified.
Results
Patient/carer profile
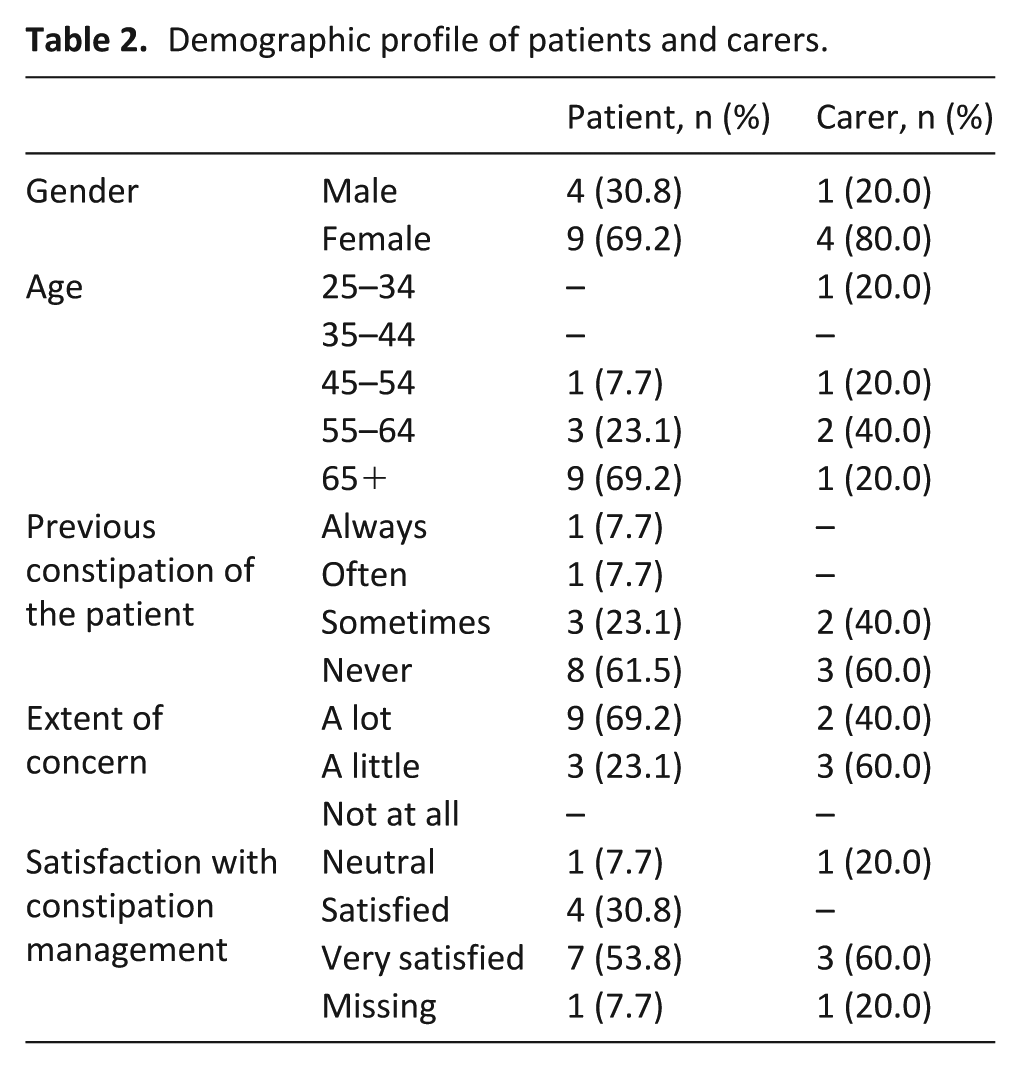
The gatekeeper identified 66 patients who met the eligibility criteria. Reasons for exclusion included severity of illness (n = 34), unwillingness to participate (n = 11) or patients were being discharged (n = 5). Of the 16 patients who consented, three died prior to interview. Thirteen patients and five carers agreed to be interviewed (Table 2). Nine patients (69.2%) were receiving opioids, and 11 (84.6%) were prescribed laxatives. Carers had been providing care between 1 and 5 years to a parent (n = 2, 40%) or spouse (n = 3, 60%).
Demographic profile of patients and carers.
Healthcare professional profile
Twenty-seven healthcare professionals participated across six focus groups. All participants were female, and more than half were employed as nurses. The most common qualification was a Bachelor’s degree, and approximately, half had received post-qualification training in constipation. The mean length of employment within the specialist palliative care unit was 5 years, and the mean length of experience within specialist palliative care settings was 8 years (Table 3).
Demographic profile of HCPs.
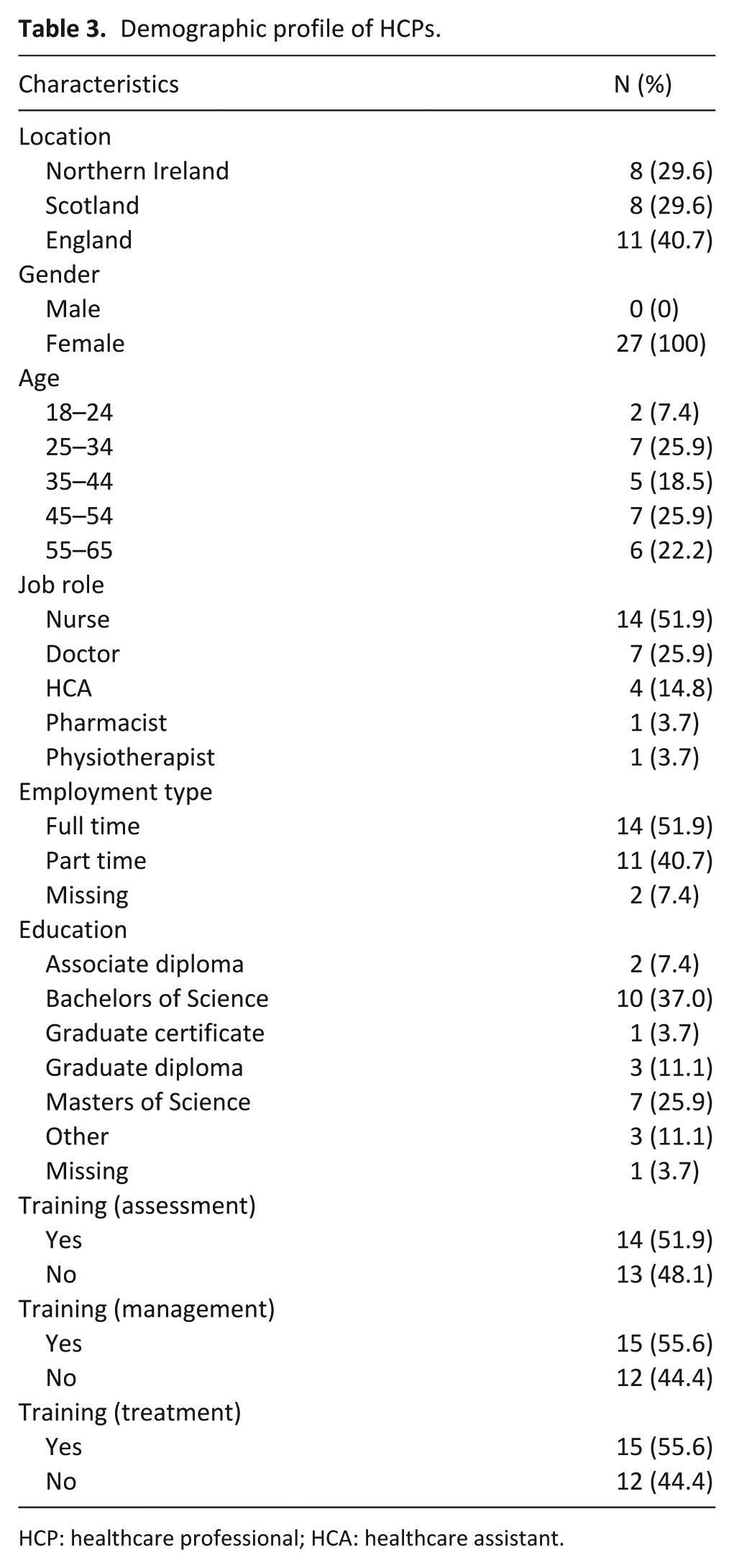
HCP: healthcare professional; HCA: healthcare assistant.
Main findings
Three themes were drawn out from the data: (1) constipation under-recognised as a multifaceted symptom, (2) the physical focus on constipation assessment with less emphasis on psychosocial aspects and (3) pharmacological management of constipation dominates in specialist palliative care.
Theme 1: constipation under-recognised as a multifaceted symptom
Patients reported a complex, multifaceted symptom with physical, psychological and social impli-cations. Physically, constipation caused pain, bloating, cramps, appetite suppression, bleeding and tearing. Psychologically, patients reported being short tempered, feeling dread when going to the toilet, anxiety that exacerbated other conditions and embarrassment running to the toilet constantly but with no bowel movement. Socially, patients felt trapped, not wanting to leave the nearby bathroom and the lethargy resulting from constipation reduced their desire to socialise:
They need to realise the impact it has on the patient and how distressing it can be. Most people think constipation will just pass, I’ll be okay. But when you’re living with it, it can be distressing. Patient_8, pg7 You are completely housebound until the dam breaks. You are scared of going somewhere and something happening. Patient_3, pg3
Prior to admission to specialist palliative care, carers played a key role in the monitoring and management of constipation using pharmacological (using laxatives and/or enemas), lifestyle and diet changes (such as increased fibre and fluids). They were acutely aware of the impact on the patients psychologically and on their social well-being, negatively affecting their quality of life, which also had repercussions on the caregiver’s life. For example, anxiety was experienced during hospital trips to help the patient with the pain caused by constipation. However, despite the holistic impact of constipation, patients/carers perceived it to be relegated on the list of importance by healthcare professionals, and the onus of responsibility was on them to remind staff of their concerns:
It has stressed him out, which means his anxiety levels have been raised and [his] breathing is affected, which has a knock-on effect on the family, because that’s where we come into play. As a result, it has been stressful for us. Carer_4, pg1 But [suppositories] was our management of it. I suggested it. I had read up on it and I suggested. We managed it ourselves. Carer_2, pg5
Healthcare professionals approached constipation in terms of the physical bowel movements, reporting a straightforward, perceived easy-to-manage symptom in relation to what they perceive as more complex symptoms that is expected within specialist palliative care due to the high prescription of analgesics, notably opioids. They reported the physical manifestation of the symptom of primary importance and approached assessment and management from an objective measurement of bowel movement rather than a subjective assessment of a patient’s expectations of bowel frequency, stool volume and consistency. One nurse identified anxiety as a potential effect; however, no healthcare professionals reported the social impact:
Constipation is often seen as a simple thing . . . It’s pretty straight forward. Nurse, FG1, pg23 Patients are on opioids and we do have a lot of patients come in, particularly in the community, who are not on laxatives. Nurse, FG2, pg9
Patients/carers believed healthcare professionals lacked an understanding and awareness of the severity and holistic impact of constipation on their lives, which they believed resulted in it being given less priority than other symptoms. They also felt responsible for reminding the healthcare professional of the importance of the symptom by initiating the conversation and the need for follow-up in its management. However, constipation remains difficult to talk about for both the patient, carer and for some healthcare professionals with most consultations typically focused on the characteristics of the disease. Healthcare professionals recognised that the assessment of constipation was tool driven, with management predominately focused on pharmacological responses. When discussing training on constipation, healthcare professionals perceived it to be either missing or as a small component within a larger curriculum:
I don’t think staff take much account when [a bowel movement] does happen. They’re not asking me very often if I had a bowel movement, or how was it? P8, pg4 I feel like I have had, not actual training, nothing online like e-learning or like that but a lot of us have learned somewhere. Nurse, FG4, pg7
Theme 2: physical focus on constipation assessment with less emphasis on psychosocial aspects
Assessment involved an objective review of physical symptoms, comprising a physical examination, recording a bowel history, identification of physical symptoms and completion of an assessment tool, such as the Bristol Stool Chart. Physical assessment dominated the conversation, with only a few participants noting preventive strategies, such as medication review and dietary considerations. Healthcare professionals indicated a potential challenge in ensuring compliance with taking laxatives reporting that sometimes, patients preferred to suffer from constipation ‘so they’re not incontinent’ (FG1, pg14). Despite recognition that outside the specialist palliative care setting, the family and patient largely self-managed the condition privately, upon entry to the inpatient setting responsibility for managing the condition was transferred to the multidisciplinary team, with the nurse often taking a lead role:
It’s theoretically a multi-disciplinary approach, including the patient and family. But I think it tends to fall to the nurses and the doctors. Nurse, FG4, pg6
While healthcare professionals reported a comprehensive assessment, patients/carers felt it was something staff did not take much account of, with one carer recalling that it was not mentioned until the patient raised it as a concern. Patients noted that the healthcare professionals were reluctant to bring up the topic, attributing this to be an embarrassing and personal symptom, noted by only briefly inquiring into current laxative use or not mentioning constipation until it was actively raised by the patient:
Well they didn’t say, ‘Do you need one?’ As in a suppository. No, it would be more just basically, ‘Have you been?’ and I would say ‘Yes’ and that would be it’. Patient_3, pg8 I don’t think it was ever mentioned until you [the patient] mentioned it. Carer_2, pg8
The challenge of initiating communication with patients was one of the main contributory factors perceived by patients as the under-appreciation of the severity of the symptom. However, patients felt that staff should help normalise the conversation and reduce anxiety by explaining that it is very common and what symptoms to anticipate:
When families are there . . . they are very embarrassed and want you to walk out of the room. Nurse, FG1, pg12 I would sometimes volunteer the information and then they would record it. But you think, if they’re not asking me, maybe they’re not thinking that it’s of any great importance. Patient_8, pg5
Theme 3: pharmacological management of constipation dominates in specialist palliative care
It was found that management was predominantly pharmacologically driven, with many healthcare professionals referring to a preferred laxative, despite awareness that there is no evidence for one laxative over another.
23
Tailoring treatment was discussed pharmacologically: however, many healthcare professionals also reported consideration of the patient’s preference, including what was palatable:
Treatment choices, how you would individualise that depending on your patient. Whether the oral or rectal route is available, or can they only manage small volumes of liquid. Pharmacist, FG3, pg16
While healthcare professionals were aware of lifestyle modifications being a factor in the treatment of constipation, they believed that they were constrained in their implementation due to the reality of the patient’s clinical condition. Healthcare professionals acknowledged that perhaps they were not incorporating the patient experience and perspective as much as they could do when managing this symptom:
You can’t always implement the lifestyle modifications. You can’t get people as mobile and you can’t get them to take the volumes of fluid or make changes to their diet, less so than someone who is well. Pharmacist, FG3, pg4 We are very good at pharmacological interventions but more focus on what the patient can do for themselves and other non-pharmacological interventions would be useful. Nurse, FG4, pg14
At home, patients/carers managed constipation using both pharmacological and non-pharmacological approaches. Patients/carers discussed lifestyle modifications positively, aware of the importance of diet and exercising within their limits. While some reported the specialist palliative care unit did consider aspects such as diet and mobility, many believed more needed to be done to support changes in these lifestyle factors. Moreover, a lack of explanation about the pharmacological approach left patients/carers with questions and doubts on the effectiveness of the treatment process:
What they told me to do with the laxatives, didn’t work. I mean, I told them it didn’t work . . . I did mention it all the time . . . they just said take more laxatives and that was their answer to everything. Patient_9, pg4 He is used to managing it at home and he’s perfectly capable of managing it, so I suppose he just thought I’ll just keep doing it myself. They certainly never mentioned it. Carer_2, pg8 I would eat more fruit at home if I was constipated at all; all I had to do was eat an orange. Patient_5, pg3
Patients were unaware of which laxatives they were taking and sometimes felt excluded, resulting in patients reporting a loss of sense of control and independence in the management of a private symptom:
You lose your responsibility for yourself while you’re here. P1, pg7 I don’t know what the names are, because there’s nothing on the tablet. P5, pg4-5
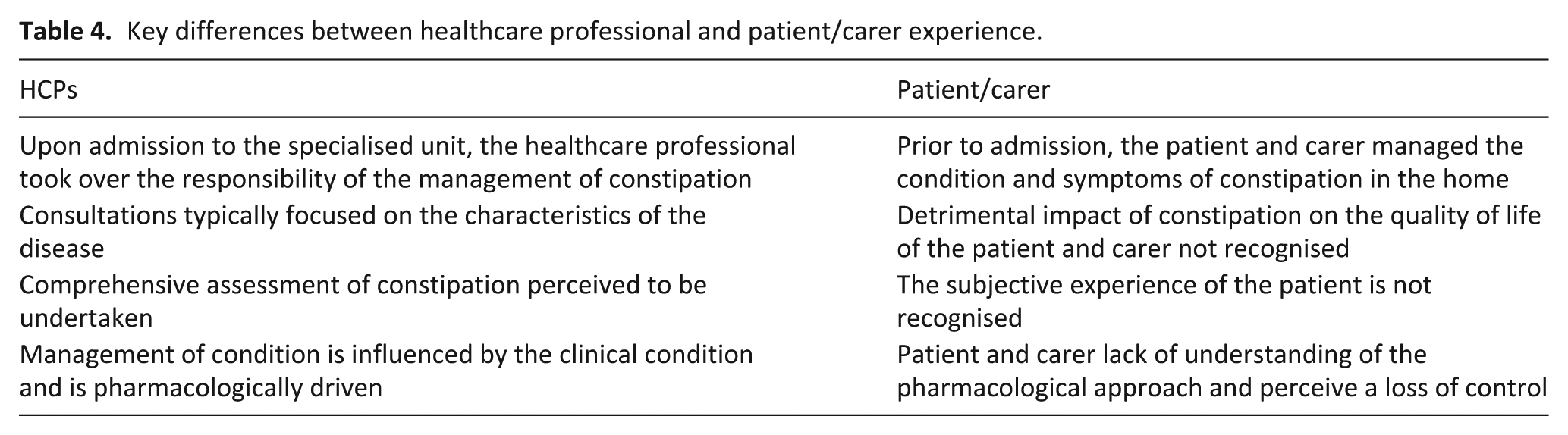
An overall summary of the key differences between the healthcare professionals and patient/carers is outlined in Table 4.
Key differences between healthcare professional and patient/carer experience.
Discussion
Main findings
This study explored the healthcare professional and patient/carer experience of the assessment and management of constipation in inpatient specialist palliative care settings. This research highlighted a difference from two perspectives on the perceived impact of constipation for patients, which is consistent with international research 24 (Table 4). However, this study also adds the perspective of the caregiver who experienced both a psychological and social impact because of the patient’s symptom and played a key role in its management at home. While healthcare professionals, patients and carers recognised that constipation is a difficult and uncomfortable topic to discuss, it was recognised as an important symptom to assess and manage.
Healthcare professionals focused on physical symptoms, while patients/families reported the physical, psychological and social impact. Healthcare professionals reported a comprehensive assessment compared to patients who felt this symptom was given lower priority. Management was pharmacologically driven, and non-pharmacological techniques used by patients and carers at home were not clearly incorporated in the specialist palliative care plan, leading patients/carers to lose self-control in the management process. It was not that healthcare professionals were averse to non-pharmacological treatment but that the focus of assessment was on physical clinical elements, and questions existed around the appropriateness of some non-pharmacological approaches for palliative care patients/environments. Healthcare professionals perceived patient embarrassment as a barrier to communicating about bowel care, whereas patients wanted staff to initiate communication and discuss constipation openly.
Previous research reported limited patient distress relating to this symptom; 12 however, the findings of this study suggest that constipation has a wider, holistic impact across multiple facets of daily living resulting in social, psychological and physical concerns. Clinical assessment is the cornerstone of individualised patient care and, in palliative care, assessment should be underpinned by the palliative approach which considers physical, psychological, social and spiritual concerns. 25 However, this study found that while assessment from healthcare professional’s perspective was comprehensive, the objectively driven focus on the physical elements of the condition resulted in patients/carers feeling their social and psychological needs were not understood, and the symptom was not prioritised until the patient raised it as a concern. Comprehensive assessment in palliative care is not only about focusing on the whole person, taking a bio-psychosocial perspective, but also ascertaining the individuals own understanding of their illness and personal situation. It could be argued that perhaps healthcare professionals do not appreciate the relevance of this approach for this particular symptom. This highlights the need to draw attention to the wider impact of constipation for both the patient/carer and for healthcare professionals to tailor their approach to incorporate these aspects. One suggestion for tailoring assessment to incorporate the patient experience and voice, which would identify the holistic impact for the patient, comes from the growing literature around the use of patient-reported outcome measures (PROMS). Within palliative care, the incorporation of PROMS into routine clinical practice indicates improved patient outcomes at both an individual and systems level.26,27 This general approach is supported by a systematic review on constipation in specialist palliative care which reported the importance of an assessment that includes the patient’s subjective experience of constipation alongside objective measures obtained through a physical examination. 28
Healthcare professionals demonstrated good knowledge and emphasis on pharmacological management; however, the importance and application of other lifestyle modifications received less attention in this setting. This is despite the clinical guidelines on constipation management in palliative care, 3 highlighting the importance of non-pharmacological strategies, including optimising toileting, privacy, diet and fluids and mobility. It is important to apply a whole person philosophy of care for patients/families, as international research indicates that patients/carers place importance in a holistic, person-centred approach to symptom management in palliative care, 29 and clinical guidelines indicate that patients want to be involved in decisions about treatment and care. 30 Contemporary healthcare policy, alongside academic literature within palliative care consistently emphasise the need to ensure patient/family engagement.31–33 Many concepts exist, such as co-production, self-care management and shared decision-making, which can be supported through education of patients/carers. 34 According to Johnston et al., 35 ‘self-management in palliative care is about supporting the patient to be given the means to master or deal with their illness or the effects of their illness themselves’ (p. 8). There is a dearth of evidence to understand the contribution of self-management support not only related to the assessment and management of constipation but more widely within palliative care. It is important that not only are patients/families prepared and supported to have a voice for self-management and to more effectively use their own strategies but also that healthcare professionals are able to facilitate this.
Similarity can be drawn from the discussion around the total pain concept36–38 and findings which demonstrated that pain assessment was suboptimal in that the subjective experience and other psychological, spiritual and social aspects were not noted. A key lesson which can be applied to constipation is the importance of assessment and management through a multidimensional lens that allows for the appreciation of all possible causes and influences.
Strengths/weaknesses
A key strength is the rigour used to capture and triangulate the emic and etic experiences of constipation, capturing the care recipient and provider perspective. However, caution is also required with interpretation, as there are two distinctive reports; one of the participants reporting the personal experience of constipation, and one of participants providing care as part of their professional role. Data from different healthcare professionals were analysed together; however, the goals of care for nurses and medics may vary. It must also be acknowledged that patients/carers were only selected from three inpatient units across the United Kingdom, and those who participated may be more comfortable talking about constipation or may be at a different stage of illness than those who were excluded by the gatekeeper; therefore, not reflective of patients deemed too unwell to participate.
What this study adds
Assessment and management of constipation in the United Kingdom may not yet reflect the holistic palliative care model for patients and families. Healthcare professionals need to consider non-pharmacological approaches and enable/facilitate the continuation of self-care management strategies and key learning and views of patients and caregivers. Healthcare professionals need to be open to initiating communication on bowel care and shifting the mindset from physical to a holistic understanding of the impact of living with the condition.
Footnotes
Appendix 1
Acknowledgements
The authors would like to thank Professors Mike Clarke, Jo Coast, Max Watson, Dr John MacArtney, Ms Rachel Perry and Mrs Eileen Wright for their contribution to the wider research project from which this manuscript was developed.
Author’s Contribution
All authors contributed to the conception and design of this work, acquisition, analysis and interpretation of data or drafting and revising it critically for intellectual content. All authors have approved the version to be published.
Data sharing
Further data can be accessed by contacting the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Full ethical approval was obtained from the Office for Research Ethics Committees Northern Ireland (ORECNI) (application no. 16/WM/0352). Governance was provided by each specialist palliative care unit.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by a research grant awarded to Prof. Sonja McIlfatrick by Marie Curie UK (grant no. MCCC-RP-16-A20993).