
Abstract
Background:
Research ethics committees are commonly perceived as a ‘barrier’ to research involving seriously ill children. Researchers studying seriously ill children often feel that committees view their applications more harshly compared to applications for research with other populations. Whether or not this is the case in practice is unknown.
Aim:
The aim of this study was to explore committees’ concerns, expectations and decisions for research applications involving seriously ill children submitted for review in the United Kingdom.
Design:
Content analysis of committee meeting minutes, decision letters and researcher response letters.
Setting/participants:
Chief investigators for National Institute of Health Research portfolio studies involving seriously ill children were contacted for permission to review their study documents.
Results:
Of the 77 applications included in this study, 57 received requests for revisions at first review. Committee expectations and concerns commonly related to participant information sheets, methodology, consent, recruitment or formatting. Changes were made to 53 of these studies, all of which were subsequently approved.
Conclusion:
Our findings suggest that committees review applications for research involving seriously ill children with the same scrutiny as applications for research with other populations. Yet, the perception that committees act as a barrier to this type of research persists. We suggest that this perception remains due to other factors including, but not limited to, the high levels of formatting or administrative revisions requested by committees or additional study requirements needed for research involving children, such as multiple versions of consent forms or participant information sheets.
What is already known about the topic?
There are a number of challenges to conducting research with seriously ill children.
Research ethics committees are considered to be one of the most significant obstacles to conducting research with seriously ill children or palliative care patients.
There is a perception that it is more difficult to gain approval to conduct research with seriously ill children than research with other populations.
What this paper adds?
Committees appear to assess research applications involving seriously ill children with the same scrutiny as research applications involving other populations. This is illustrated by the finding that most of the committee expectations and concerns about applications involving seriously ill children were similar to the expectations and concerns about applications involving adults or healthy children.
There is an apparent disconnect between what researchers feel is appropriate in terms of patient information sheets and consent forms and what committees expect, which may contribute towards the perception of research ethics committees as a barrier to research with seriously ill children.
Alternative sources for the perception that committees are a barrier to research with seriously ill children include, but are not limited to, the high levels of formatting or administrative revisions requested by committees or because of additional study requirements needed for research involving children, such as multiple versions of consent forms or participant information sheets.
Implications for practice, theory or policy
Joint workshops between researchers and committees should be held to develop guidance which could help researchers and committees recognise their own and the other stakeholders’ roles, responsibilities and expertise so that each party can achieve the shared goal of ensuring the highest standard of ethically conducted research.
Researchers should endeavour to attend committee meetings wherever possible to clarify issues raised by the committee. Countries that do not currently allow researchers to attend these meetings should consider this as an option to reduce the administrative burden and improve the dialogue between researchers and committees.
Introduction
Over 40,000 children are estimated to have a life-limiting condition or life-threatening illness in England. 1 If improvements are to be made in the care and treatment of these children, ongoing research is required.2–5 However, there are a number of challenges to conducting research with this population: timing difficulties associated with end-of-life research; limited funding and resources for palliative care research; and clinician hesitancy towards involving these children and their families in research studies.6,7 In addition, despite a shared goal for high-quality, ethically sound research, researchers report that research ethics committees and the associated regulatory approval processes pose an obstacle to the conduct of such research involving seriously ill children.6–8
Research ethics committees, alternatively known as human research ethics committees, institutional review boards or European ethics committees (hereafter referred to as ‘committees’), are a group of individuals who are responsible for reviewing research applications to ensure that internationally and locally recognised ethical standards are being met. 9 Similarly, it is the researchers’ responsibility to ensure that they are familiar with and that they comply with these recognised ethical standards when developing a research protocol. 10 After reviewing an application, committees assess the extent to which researchers have adhered to these standards and can approve the project, request a revision of the study proposal or reject the proposal entirely. 9
The perception of committees as an obstacle to research with seriously ill children is complex and multifaceted. There are many challenges in the application process itself, from identifying and completing the lengthy and cumbersome paperwork to meeting submission deadlines.11–13 Once the application has been submitted, researchers report feeling frustrated by the time taken to gain approval.14–16 This frustration persists in relation to the decision-making process as committees have been shown to differ in terms of the decisions and revisions requested when reviewing the same application.16–21 This makes it difficult for researchers to predict and therefore address committee concerns in advance of submitting their application. The perception that committees are a barrier may be heightened at this stage in the application process for some researchers as they feel that committees scrutinise applications utilising qualitative or experiential research designs more harshly than those using quantitative or clinical research designs.22–24 The same can be said for researchers working with seriously ill children, as some anecdotal reports suggest many researchers feel like the bar for gaining ethical approval for their research is set higher by committees. This article examines the potential sources of the perception that committees are a barrier to research with seriously ill children and considers how this perception might be changed through the joining of the two stakeholders (committees and researchers) around the common goal of ensuring the highest standard of ethically conducted research.
Methods
Participants and setting
In total, 258 applications of children (aged 0–18 years) with life-limiting conditions and life-threatening illnesses reviewed by committees between March 2011 and March 2016 were identified in the UK National Institute of Health Research Clinical Research Network portfolio. Applications were included if they involved children and young people with life-limiting conditions or life-threatening illnesses. As is common in paediatric palliative care research in the United Kingdom, our definitions of ‘life-limiting’ or ‘life-threatening’ were based on the definition outlined by Fraser et al. 1 in combination with conditions listed in the 10th Revision of the International Classification of Diseases (ICD-10) codes included in Hain’s directory of life-limiting conditions. 25
All eligible chief investigators (n = 178) were contacted for permission to view the minutes of the committee meeting where their application was considered, as well as any subsequent correspondence, including decision letters and researcher response letters.
Analysis
Descriptive information, including study type, intervention type and the committee opinion for each submission, was extracted from the Integrated Research Application System and committee meeting minutes and analysed for frequency. Contingency chi-square tests were conducted to establish whether there was a statistically significant difference in committee opinion at first review based on study and intervention type.
Content analysis was used to systematically apply content categories to meeting minutes and letters.26,27 Categories were based on the Governance Arrangements for NHS Research Ethics Committees (GAfREC)28,29 requirements for favourable opinion (approval of the research proposal). All documents were independently coded by A.E.B. and K.V. to determine the frequencies of each category. The research team met regularly to review coding and resolve any discrepancies. Researcher response letters were analysed for frequency of researcher agreement or disagreement with committee concerns, as well as whether or not revisions were made by the researchers to comply with committee concerns. Results were tabulated and descriptive statistics utilised where appropriate.
Ethics
The study was registered with Research and Development within UCL Great Ormond Street Institute of Child Health. Written consent was obtained prior to the collection and analysis of any research application. Researchers’ details were redacted by the Health Research Authority where requested.
Results
Overview of included applications
Out of 178 chief investigators contacted, 97 provided consent for the study team to review their committee applications and correspondence, giving a response rate of 54.5%. Of these, the Health Research Authority was able to provide committee meeting minutes for 77 applications (91%). These form the basis of the analysis.
Decisions at first review
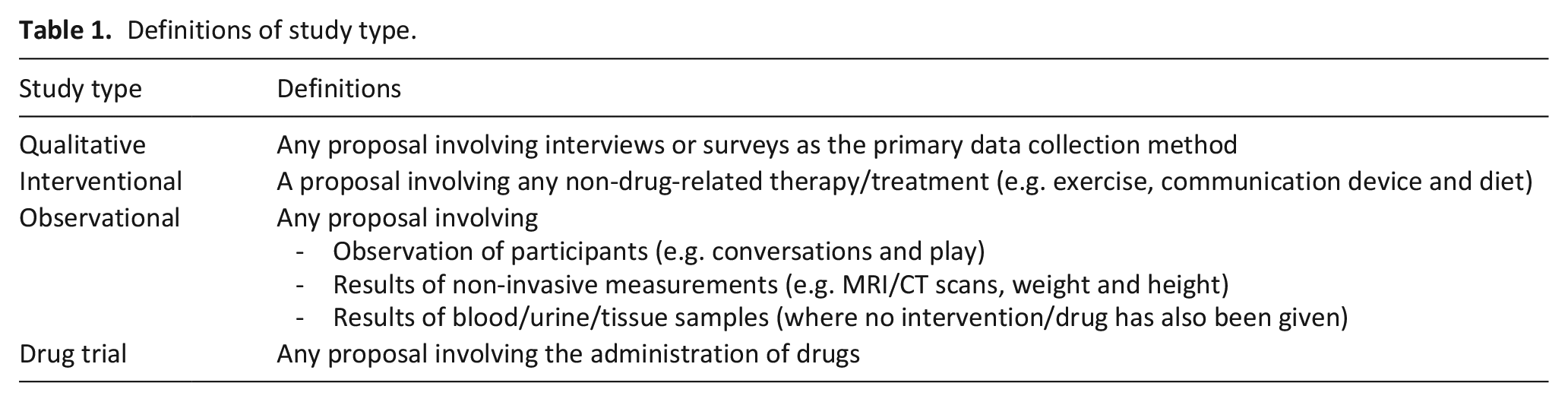
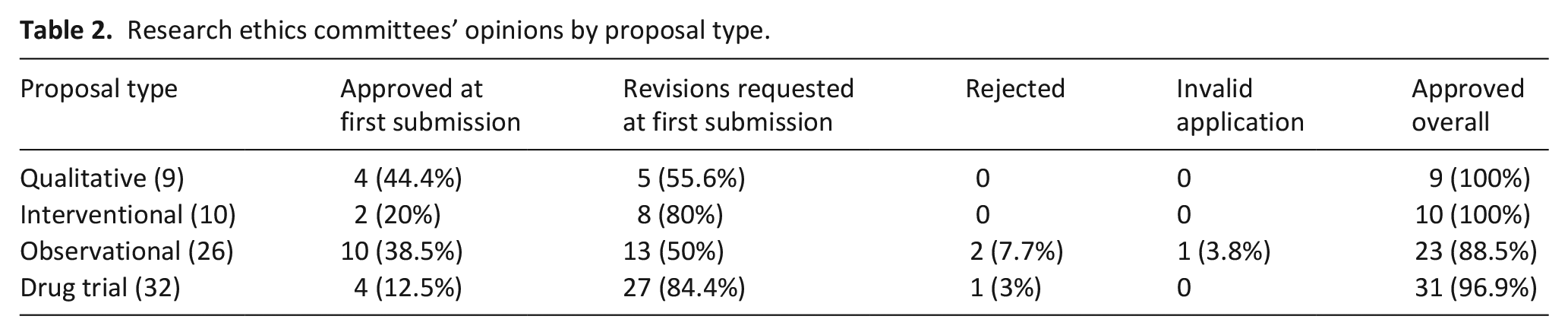
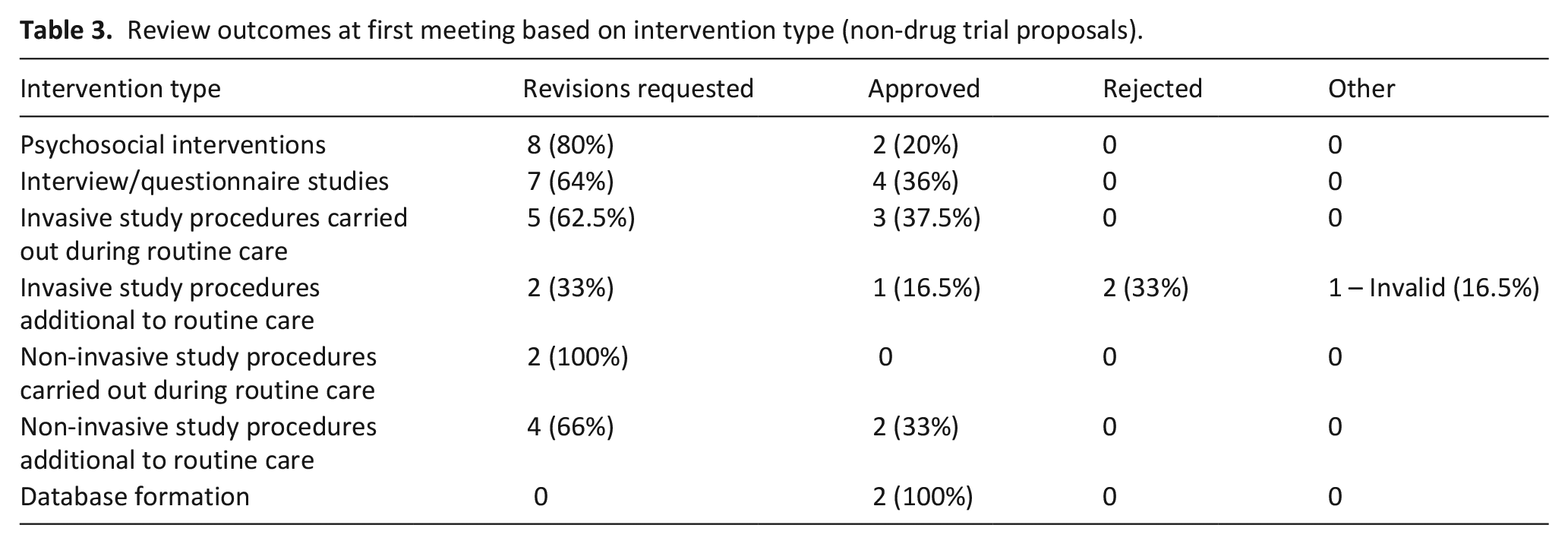
Overall, 9 qualitative applications, 10 interventional applications, 26 observational applications and 32 drug trials were included in the analysis (see Table 1 for definitions of study types). Just over two-thirds of applications (68.8%) received an initial request for revisions rather than being approved at the first committee meeting (outlined in Tables 2 and 3). Requests for revisions at first review were higher for drug trials or interventional studies than for qualitative or observational studies, though this was not statistically significant (p = 0.231). Although almost all interventional studies received revision requests, the frequencies of these requests varied depending on the intervention (p = 0.075). The exception to this outcome was two studies that aimed to create databases, both of which received approval at the first committee meeting. Of note, no studies were approved if the researchers were absent from these first committee meetings (see Table 4).
Definitions of study type.
Research ethics committees’ opinions by proposal type.
Review outcomes at first meeting based on intervention type (non-drug trial proposals).
Frequencies of research ethics committees’ decisions at first meeting based on researcher attendance.

Data on researcher attendance only available for 72 studies; p-value = 0.4512.
Committee concerns and expectations
The major committee concerns and reasons for requesting a revision of a research application are outlined in Figure 1. Overall, most concerns are related to the content of the participant information sheets or methodological or procedural issues. Generally, the committee expected more detailed participant information sheets. They commonly raised concerns about incomplete or missing information sheets, the inclusion of unnecessary information or information sheets that contained formatting errors, such as grammatical or typographical mistakes. Committee comments relating to methodological or procedural issues demonstrated an expectation for clearer study aims, a more detailed description of the collection and analysis of data, and a justification of the methods proposed.
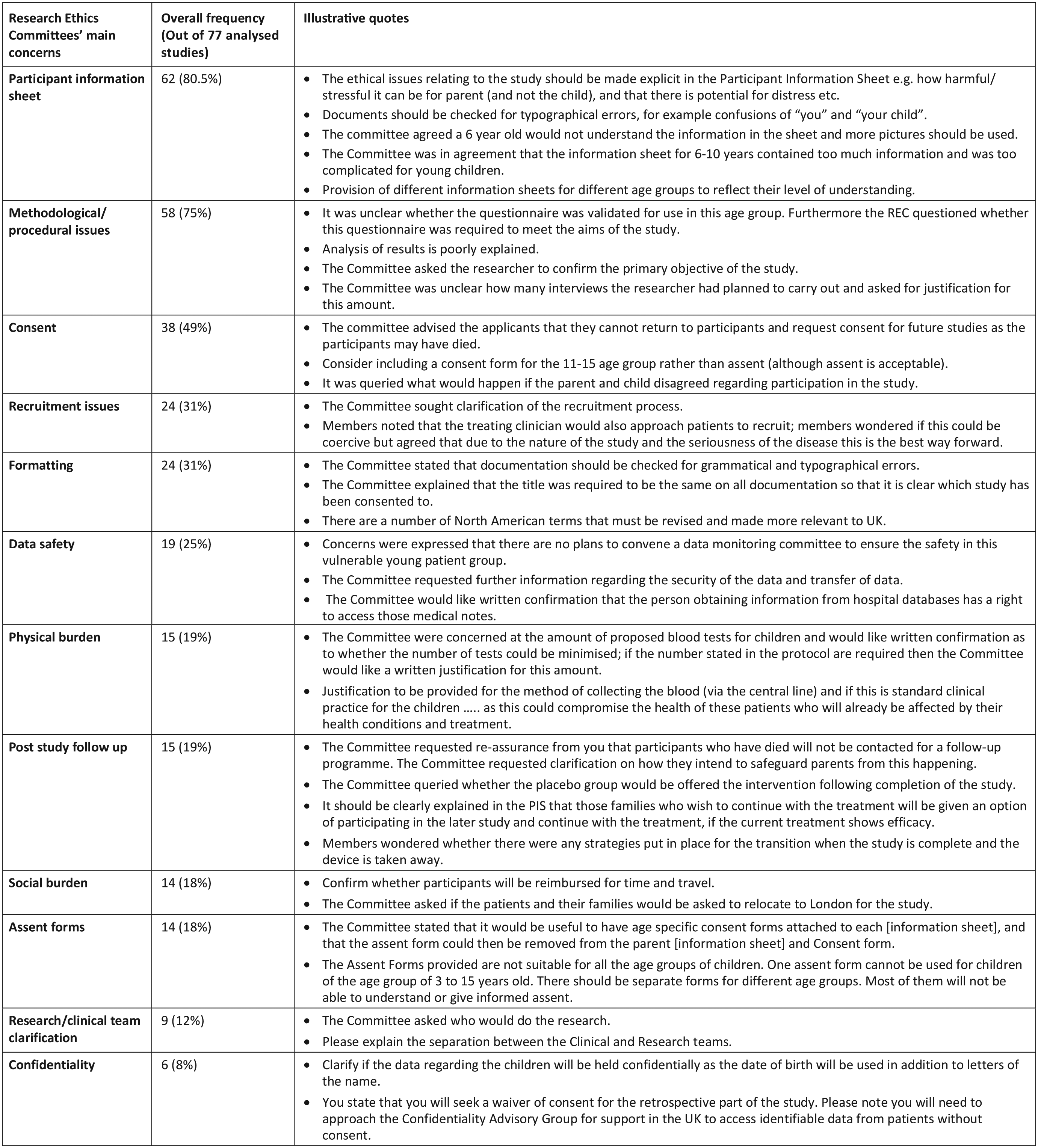
Frequencies of research ethics committees’ main concerns overall and illustrative quotes.
Notably, general formatting errors were the fourth most common concern and occurred as frequently as recruitment issues, accounting for 31% of all comments. Committees expected researchers to provide complete paperwork, to check applications for grammatical and typographical errors, to explain acronyms and to avoid the use of overly technical language.
The least common concerns raised by the committees related to inadequate data storage or protection of participants’ confidentiality and the need to properly clarify the research and/or clinical teams. In addition, committees rarely raised concerns about the physical or social burden that research participation would place on participants and their families (raised in 15/77 and 14/77 applications, respectively).
Committee concerns specific to children and young people
In addition to identifying general concerns for the reviewed applications, the committee meeting minutes also identified a number of concerns specifically relating to the inclusion of children with serious illnesses. One of the key issues specific to this population related to the use of child-friendly language, particularly in participant information sheets. Committees expected researchers to ensure that the language used in participant information sheets was appropriate for the various groups of children in their applications. They often requested that researchers simplify the language used and avoid the use of ‘harsh’ or clinical terminology. Pictures or diagrams were expected for younger children. Ensuring the information supplied in information sheets was age-appropriate was also noted (see Figure 1).
In addition, committees made a number of comments relating to consent and assent for children with serious illnesses. Seven applications received comments pertaining to the need to gain consent or assent from participating children, though there was little consensus noted on an appropriate age for consent or assent provision in these children. In addition, four committees required researchers to clarify what would happen if parents and children disagreed on providing consent to participate. Other committee concerns related to the complexity of consent forms for children, with committees often expecting researchers to create separate consent forms for different age groups.
Finally, child-specific recruitment concerns were also commonly identified by committees, with many committees expecting researchers to involve the child’s senior treating clinicians in the recruitment process, both to facilitate appropriate participant identification and to minimise potential distress. Yet, when this recruitment method was used, two committees commented on the potential for coercion. The committee, however, did not require a change of recruitment plan.
Researchers’ responses
Researchers’ response letters were available for 27 applications that required a response (47%) and contained a total of 279 responses to the committee comments. On average, each letter from a research team contained responses to 10 committee comments. Almost 72% of the time (200/279 responses), researchers made changes to the study application based on the committee concerns and expectations; most commonly for issues relating to participant information sheets (as shown in Table 5). For 53/279 committee comments, researchers were only required to justify their procedures or methodology, with no changes to documentation or study procedure required.
Frequencies of researchers’ responses.
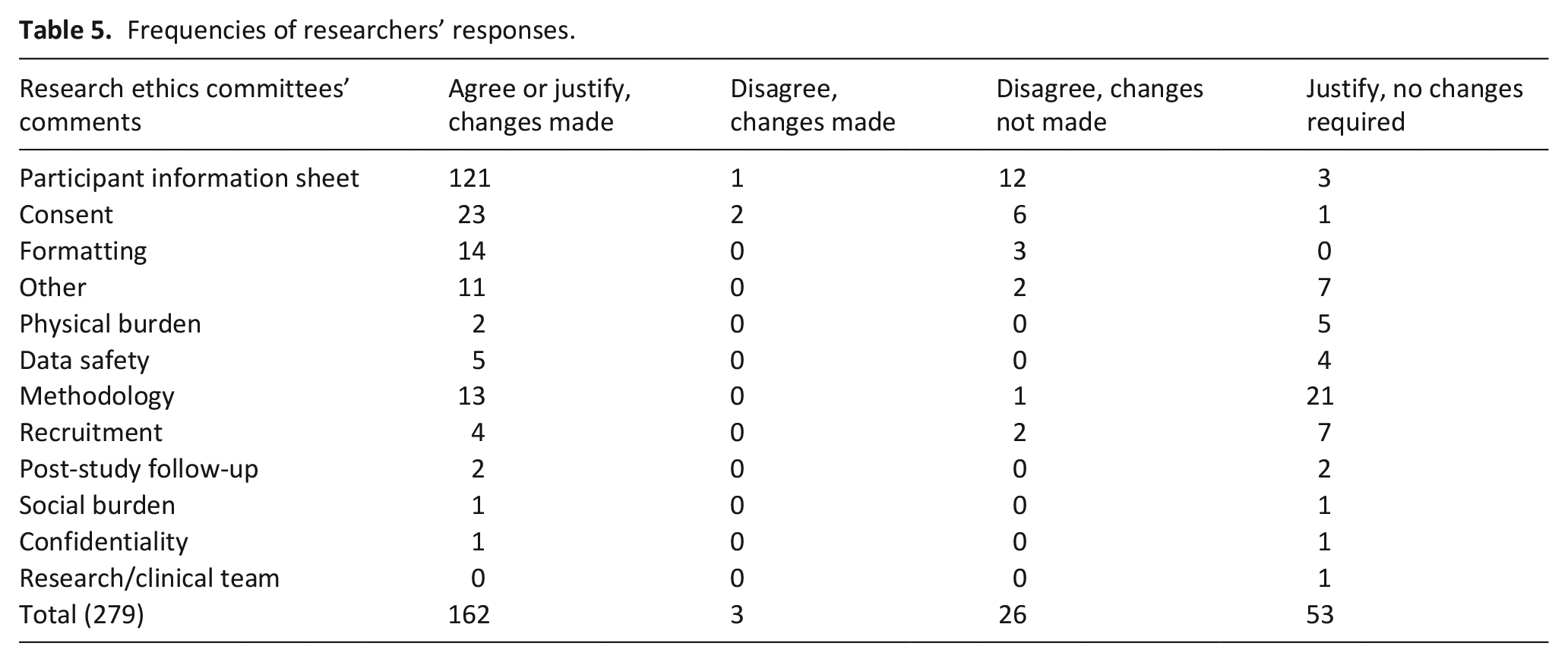
In total, 15 of the 27 researchers who provided a response letter disagreed with one or more of the committees concerns or expectations. These disagreements usually related to committee concerns for participant information sheets or consent forms. These disagreements occurred 29 times (10% of all responses made by researchers). For 26 of these 29 comments, researchers did not make the changes requested by the committee, either because of researcher preference or because of non-negotiable requirements of the study (e.g. the inclusion of international phone numbers or specific participant screening tools).
As revealed in the committee minutes, many of the committee concerns which researchers responded to at the meeting were not listed in the committees’ decision letters and therefore did not require a written response from the researcher.
Outcomes of committee review following revisions by researchers
In total, 57 applications required changes to meet committee concerns and expectations. After changes were made, 53 (93%) were approved. Of the four applications that were not approved, three were rejected because the researchers did not make the changes expected by the committee, and one was deemed an invalid application because of incorrect paperwork.
Overall, the vast majority of the research applications reviewed by committees received overall approval to conduct the research (94.8%), either at the first committee meeting or at a subsequent meeting after an initial request for revisions.
Discussion
Main findings
The perception that research ethics committees act as an obstacle to research with children at the end of life has been evident in the literature for over 15 years.6–8 Despite this commonly held belief, this is the first study to empirically explore whether committees actually are a barrier to research with seriously ill children. Our findings suggest that while the metaphorical bar to gaining ethical approval is indeed high, with many obstacles to meet both before and after submission, it is not insurmountable, particularly when researchers are aware of and can address the committee’s expectations and key concerns.
What this paper adds?
The process of gaining approval to undertake a research study involves two key stakeholders: researchers and the committees who review their applications. Although the roles, responsibilities and expertise of these stakeholders differ, they have a common purpose to conduct high-quality, ethically sound research.
The primary role of committees is to ensure that all research applications, regardless of study or intervention type, are ethically sound, of a high quality, and that the dignity, rights and well-being of participants are protected. 28 However, there is a perception that the review process differs depending on the type of study being reviewed,22–24 with anecdotal evidence suggesting that research applications involving seriously ill children are viewed with greater scrutiny than applications for research involving other populations, such as adults or healthy children. This perception does not appear to be supported by our findings. First, the overall approval rate for applications included in this study (94.8%) is consistent with the overall approval rate within the United Kingdom for all research applications submitted for committee review within the same time period. 30 Second, we found that many of the concerns and expectations for applications involving seriously ill children were similar to those involving adults or healthy children.
The majority of the committee expectations and concerns identified in this study focused on having detailed participant information sheets, obtaining informed consent, having justified study methods and procedures and ensuring a clear and unbiased recruitment plan. These committee expectations and concerns are very similar to those identified in studies involving adults and healthy children, where the main committee concerns are related to informed consent,31–34 confidentiality,31,35–37 scientific design31,32,34,35,37,38 and recruitment.31,35,38 These findings suggest that the review process is equivalent, at least in terms of the types of decisions made and concerns and expectations expressed, for applications involving seriously ill children as well as applications involving other populations.
When submitting a proposal for committee review, researchers are primarily responsible for ensuring their research is methodologically sound and clearly explained, and that any associated paperwork, such as information sheets or consent/assent forms, are appropriate to the specific needs of their potential participants. In addition, researchers are also responsible for shouldering the administrative burden of the submission, ensuring that their submitted applications and the associated paperwork have been proofread and are submitted in their entirety. This way, the committees assessing the applications can appropriately discharge their responsibility for assessing the ethical quality of the research. However, 31% of all committee comments documented in minutes and correspondence with researchers related to formatting or administrative matters (e.g. grammatical or typographical errors, incorrect versions of paperwork), as opposed to errors considered to be ethical in nature.
We would suggest that this high percentage of requests regarding formatting and administrative matters contributes to the perception of committees as a barrier to research, as researchers become frustrated and disheartened when they feel they are constantly required to make changes, they perceive to be ‘nit-picky’ rather than ethical.33,39 We also wonder if it is possible the role of committees, as well as current research administration and paperwork requirements, no longer meets the needs or contributes to researchers and committee members shared goal for conducting high-quality ethically robust studies. We recommend that future research focus on how to move research review and approval processes forward to harmonise them with the current climate of ethically complex research.
Another important responsibility for researchers in the United Kingdom is to attend the committee meeting where their proposal is being reviewed. Our findings indicate that no studies were given approval at first committee meeting if the researchers were not present at this meeting. Attendance at this meeting allows for open dialogue between researchers and committees, enabling many issues to be discussed and resolved then and there rather than requiring a formal written statement on behalf of the committee and a written response from the researchers. In light of this finding, we would recommend that countries which do not currently offer researchers and committees the opportunity to discuss and resolve issues or concerns before a decision is made, offer it.
Improving the dialogue between these two stakeholders might also help to repair the disconnect between what researchers feel to be appropriate in terms of consent forms and participant information sheets and what committees perceive to be sufficient or appropriate. For instance, committees frequently requested different versions of participant information sheets depending on the child’s age and condition. They also commented on the complexity of the language used and the types of information provided in the children’s information sheets, often suggesting that information be simplified or pictures be used to better explain what would occur. Similar to their concerns for participant information sheets, committees also commonly requested that researchers create different consent/assent forms based on the ages of the participating children. The requirement of these additional documents for research involving seriously ill children, while necessary, likely contributes to the perception that committees are a barrier to research with this population.
Although such issues surrounding assent/consent forms and participant information sheets are addressed by committees in current guidance,40–43 researchers continue to remain unclear or may disagree with the suggestions offered in the guidelines. It may be that current guidance is not fit for purpose or is not available in a format that is easily accessible for researchers. In addition, current guidance may not take into account the experience and expertise of the researchers, or the fact that their information sheets or consent forms have often been developed in consultation with seriously ill children and their families through a formal or informal process of Patient and Public Involvement (PPI). We therefore suggest committees undertake joint workshops with researchers to develop guidance that simultaneously ensures adherence to evidence-based ethical principles while allowing for flexibility to meet the unique needs of the children in the study.
Study limitations
There are three limitations to consider when interpreting our findings. First, and most significantly, this study focused solely on applications submitted to committees in the United Kingdom. Having said this, we recognise the areas in which the approval process is likely to differ between the United Kingdom and other countries and we identify possible areas for improvement in those countries that adopt different systems. Second, given that the number of National Institute of Health Research studies in this population is small, our ability to reach statistical significance was limited. However, all of the applications were of high quality, having been competitively funded either nationally or internationally. Third, almost all of the applications were approved after first resubmission, which may reflect a willingness on the part of the chief investigators with more positive outcomes to reply. That said, 5% of the applications included in this analysis were rejected at first meeting. Notably, this rate is similar to the percentage of study applications rejected by committees across the United Kingdom during the study period, 30 so we do not believe this as a significant concern.
Future research could involve surveying or interviewing researchers and clinicians conducting research with this population to explore in more depth the anecdotal accounts suggesting that committees are a barrier to their research. Such qualitative enquires could help refine the possible sources behind the perception that committees are an obstacle to research with seriously ill children and allow targeted interventions to overcome them.
Conclusion
There is a perception within the paediatric research community that research ethics committees act as a significant barrier to research with seriously ill children. While our findings would suggest that committees review applications with seriously ill children with the same level of scrutiny as they do applications involving adults, the perception that committees act as a barrier to research with this population persists. It is possible that this perception arises from the high levels of formatting or administrative revisions identified in this study or from the additional study requirements needed for research involving children, such as multiple versions of consent forms or participant information sheets. Moving forward, efforts should be made to improve the dialogue between researchers and committees so to make each stakeholder aware of their own and others’ key roles, responsibilities and expertise. In so doing, the ethical approval process might be made easier, the perception of committees as a barrier to research reduced and both stakeholders reunited in their common goal of ensuring that research with seriously ill children be ethically sound and of the highest quality.
Footnotes
Acknowledgements
The authors would like to thank Matt Rogerson, Ian Nickson, Vanessa Poustie and the Health Research Authority for their assistance in the extraction and retrieval of the applications included in this analysis.
Author contributions
All listed authors have made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data; drafted the article or revised it critically for important intellectual content; approved the version to be published; and participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Data sharing
Data used in this project are not available for review without prior written consent from the Health Research Authority and the chief investigators of each study.
Ethical approval and informed consent
Research ethics approval was not required as no participants took part in this study. The study was registered with the Research and Development Department within UCL Great Ormond Street Institute of Child Health.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: A.E.B. and K.V. have no conflicts of interest to declare. M.B.-L. is an invited editor for a special edition of Palliative Medicine; however, she has recused herself from editorial decisions related to this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: A.E.B. is supported by the National Institute for Health Research (project code 540193); K.V. is supported by Great Ormond Street Children’s Charity (project code 510858) and M.B.-L. is supported by funding from the True Colours Trust (grant code G25 511830 2LGA). This research was supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) North Thames at Bart’s Health NHS Trust. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. This research was also supported by the Health Foundation and the NIHR Great Ormond Street Biomedical Research Centre.