
Abstract
Background:
Multidrug resistant pathogens are a large-scale healthcare issue. In particular, children with life-limiting conditions have a significantly increased risk of multidrug resistant pathogen colonization. Official hygiene requirements recommend children, who are colonized with multidrug resistant pathogens, to be isolated. In the context of pediatric palliative care, such isolation adversely affects the aim of social participation. To overcome this challenge of conflicting interests on a pediatric palliative care inpatient unit, a hygiene concept for patients colonized with multidrug resistant pathogens, called PALLINI, was implemented.
Aim:
The aim of this study was to identify the nurses’ attitudes and opinions toward PALLINI.
Methods:
Nurses (N = 14) from the pediatric palliative care unit were queried in guideline-oriented interviews. Interviews were analyzed qualitatively by means of content analysis.
Results:
The following four categories were identified: (1) safety, (2) effort, (3) quality of care, and (4) participation. All categories demonstrated ambivalence by nursing staff regarding PALLINI. Ambivalence arose from guaranteeing infection control versus noncompliance by the families, additional workload for patients with multidrug resistant pathogens versus lack of resources, impaired relationship with the parents versus enabling better care for the child, as well as enabling some limited contact versus the larger goal of genuine social participation. Despite this, nurses reported the importance of arranging everyday-life for the patients so that they experience as much social participation as possible.
Conclusion:
The implementation of a new hygiene concept is challenging. Despite positive reception of PALLINI from the nurses, ambivalence remained. Addressing these ambivalences may be critical to best implement the new hygiene concept.
Children with life-limiting conditions have a significantly increased risk for colonization with multidrug resistant pathogens.
Caring for patients with multidrug resistant pathogens requires the application of safe hygiene concepts often implemented as isolation.
Isolation reduces the quality of life of patients and their families.
The implementation of a complex hygiene concept that allows social participation for patients colonized with multidrug resistant pathogens results in ambivalence among the nursing staff.
The complex hygiene concept represents a significant challenge for nurses caring for children with multidrug resistant pathogens and requires additional time resources.
Advantages of the hygiene concept that can be easily integrated into the daily routine of the unit (e.g. the possibility of open doors) are assessed positively by the nurses.
The implementation of a complex hygiene concept for children colonized with multidrug resistant pathogens, which counters the concept of strict, single-room isolation, represents a challenge for nursing staff and triggers ambivalence. For successful implementation, these ambivalences need to be addressed and resolved.
Introduction
Children with life-limiting conditions have a significantly increased risk for colonization with multidrug resistant pathogens due to frequent hospital stays, numerous antibiotic treatments, presence of special devices (e.g. percutaneous endoscopic gastrostomy—tube, central venous catheter, and tracheostomy), and immunosuppression. 1 Especially in these severely ill children, multidrug resistant pathogens pose a significant threat. 2 In this regard, nosocomial transmission of pathogens, and in particular multidrug resistant pathogens, must be avoided on pediatric palliative care units.
According to the official hygiene requirements published by international authorities,3–6 children colonized with multidrug resistant pathogens must be isolated. In the context of pediatric palliative care, such isolation endangers the aim of social participation as defined by the World Health Organization 7 and may reduce quality of life for both the child and their family. 8 In particular, inpatients, who are isolated, do not have the opportunity to participate in the interdisciplinary treatment approach and the social togetherness of a pediatric palliative care unit. Considering the two different treatment objectives, the concept to prevent transmissions of multidrug resistant pathogens must be adapted to the framework of a pediatric palliative care unit while considering high safety standards.9,10
To overcome this challenge of conflicting interests (social participation vs prevention of nosocomial transmission), a hygiene concept for patients who are colonized with multidrug resistant pathogens, 11 called PALLINI, was established on a pediatric palliative care unit. PALLINI suggests that—instead of isolation—strict barrier nursing (see Figure 1) is applied to patients who are colonized with multidrug resistant pathogens.
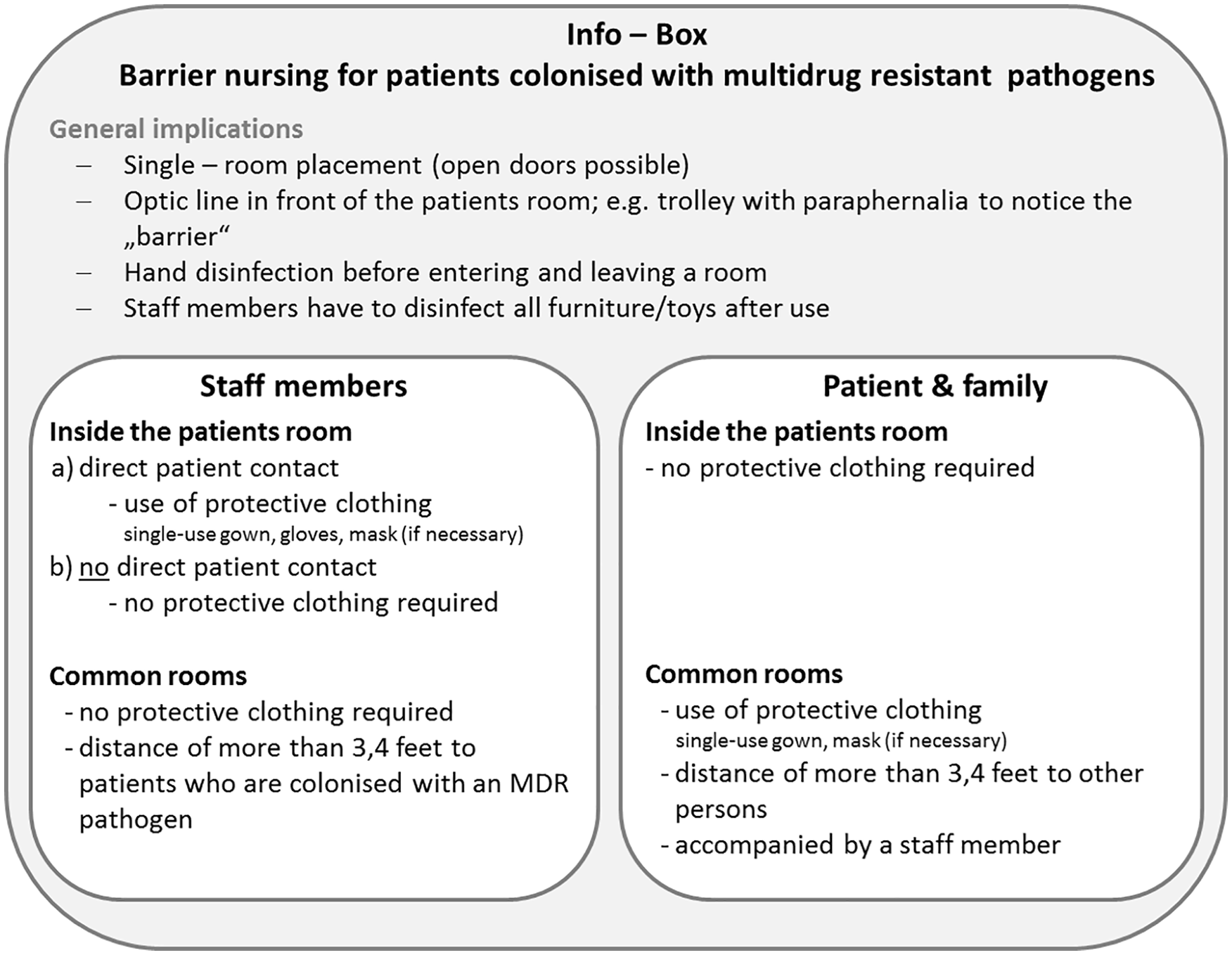
InfoBox “Barrier nursing.”
PALLINI—hygiene concept for patients colonized with multidrug resistant pathogens
PALLINI entails that all patients of the unit are screened for colonization with multidrug resistant pathogens prior to or during admission. If screening results are missing on the day of admission, patients who are at risk of multidrug resistant pathogens colonization (e.g. tracheostomy, device, transfer from surgical units) are cared for using barrier nursing until screening results are available (on average 48–72 h). Standard precautions are applied to each patient contact. In patients who are colonized with multidrug resistant pathogens, barrier nursing will be continued, but patients are allowed to participate in social activities (e.g. music-therapy, art-therapy, or playing with others) on the unit wearing gowns and applying strict hand disinfection. The attending nurse supervises compliance with these targeted precautions. Concerning PALLINI and the concept of barrier nursing specifically nurses have to (1) inform and instruct patients, parents, and visitors regarding the regulations of barrier nursing (e.g. by use of an educational film) (2) monitor that families and visitors apply the regulations of barrier nursing correctly, and (3) coordinate the attendance of members of the psychosocial team, who accompany the family in the common room. Nurses, therefore, play a key role in the process of realization of PALLINI. Prior to the implementation of PALLINI on the pediatric palliative care unit, all staff members of the different professions are educated and trained concerning the concept of barrier nursing, modes of transmission of multidrug resistant pathogens, and the prevention of nosocomial infections. As well as all new staff members are educated as part of their incorporation.
A first proof of safety of PALLINI has been provided in a pilot study. 12 Results of this pilot study show a high prevalence of multidrug resistant colonization on admission to the unit (18%) and no nosocomial infection caused by multidrug resistant pathogens. 12
The hygiene concept PALLINI requires changes in the daily care routine on the unit and causes additional effort for all staff members. These changes are particularly relevant for the nurses because, compared with other staff members, they have the most contact points to the patients and families. Thus, they are most involved in a successful realization of PALLINI. Therefore, the purpose of this study is to identify the attitude and opinion of nurses toward PALLINI. This knowledge can be used to facilitate the implementation of PALLINI on a pediatric palliative care unit and in other pediatric palliative care settings.
Methods
Design and setting
This study was conducted using a qualitative research approach with topic-based and open data collection through guideline-oriented interviews in conjunction with structuring qualitative content analysis. Interpretative analyses were characterized by inductive and deductive category formation.
The study sampled a population of nurses of a pediatric palliative care unit. This unit is not a children’s hospice but a separate, self-reliant palliative care unit in a tertiary care children’s hospital. It comprises eight beds in single rooms and offers intensive pediatric palliative hospital care but not respite care. Every year, approximately 200 admissions with life-limiting conditions are treated on the unit. The mean age of the children treated on the unit is 9.5 years, and they mainly suffer from conditions originating in the perinatal period; diseases of the nervous system; congenital malformations, deformations, and chromosomal abnormalities or endocrine, nutritional and metabolic diseases. 13
Participants
Nurses were purposively selected if they were a member of the nursing team of the pediatric palliative care unit. They were eligible for participation if they worked at least 3 months on the unit. In order to achieve a heterogeneous sample, both nurses with less work experience and those with many years of work experience were included in the study. Written consent was obtained from each participant after a thorough explanation of the purpose and method of the study had been provided. Participation was voluntary.
Data collection
Semi-structured interviews were conducted by a female research assistant (A.H.-P.; MScN) with proficient experience in qualitative research between September and November 2018 in the workplace at time convenient for participants. First, participants were asked to generally recall their experiences and understanding of the PALLINI concept. Next, open-ended questions were asked about specific aspects of their experiences, such as “What has changed in your everyday work due to PALLINI? What works well, what doesn’t work well within the concept?” Participants were encouraged to respond freely to each question. The interviewer listened without interruption and asked further questions for a deeper understanding. All interviews were audiotaped and anonymized transcribed verbatim. After interviews with 14 nurses, the data collection process was closed, because no new themes were expected.
Data analysis
Influenced by a positivist coding approach, a qualitative content analysis 14 was performed on the transcribed data using the software MAXQDA, Version 18.0. 15 For category development based on the literature, a deductive lens was used. Through reflection, an inductive coding approach was followed with the intent of identifying what was important to participants from their own perspectives, rather than using a pre-defined structure.
First, two researchers (A.H.-P. and P.S. (PhD, MScN, qualified in qualitative research)) read through each interview several times. Working independently, they extracted all statements related to the study topic from the interview transcripts and determined the meaning of each. They then discussed their findings and jointly grouped the statements into categories and subcategories. Across all categories, one key topic could be identified. To check for accuracy and resonance with their experiences, results were returned to participants. All processes in the analysis, all categories and subcategories and the key topic were confirmed through discussion with the co-authors (J.W., C.H., and B.Z.).
Ethics
This study was approved by the Ethics Committee of the Witten/Herdecke University, Germany (ID 207/2017) and was conducted in accordance with the principles laid down in the Helsinki Declaration.
Results
A total of 14 out of 20 eligible nurses gave their written informed consent to take part in the study. A total of eight interviews were conducted (four individual interviews, three interviews with two nurses and one interview with four nurses). All participants were female and on average they had worked on the unit for 5.8 years (SD = 2.8; range 1–8 years). Two participants were in leadership positions (one unit manager and one division manager). The duration of the interviews varied from 35 to 60 min.
Regarding the opinions and attitudes of nurses toward PALLINI, the following four categories (1) safety, (2) effort, (3) quality of care, and (4) participation and the key topic of ambivalence were identified (see Table 1).
Ambivalence by the nurses within the four identified categories.

Safety
All nurses state that PALLINI contributes to the safety of patients and families as well as staff members. It seems important to them that the transfer of pathogens to other patients is minimized by correctly following the regulations of barrier nursing. However, safety is only guaranteed if everybody on the unit follows the rules of PALLINI—staff, patients, families, and visitors. Noncompliance to the concept (e.g. unclosed gowns, siblings in the common rooms/garden without gowns) presents a threat to the safety: Well, I think that it’s extremely difficult and also very/ I think it’s most annoying of all when there are siblings present, they are always in the garden without a gown. You can’t look after them that quickly, because then all I would do is check on the siblings. And I can’t do that. (MA 03, Abs 25)
The nurses state that it is “impossible” to observe everything outside the patients’ rooms and to monitor the compliance with the concept of barrier nursing. In their view, there is an increased risk of pathogen transmission when a patient or family member leaves the room. Therefore, some nurses state that they tend to keep the children and their families in their room instead of encouraging them to leave the room; “[. . .] no very, very rarely. That is hardly done anymore.” (MA 03, Abs 14). Thus, the option for the patient to leave their room to participate in social activities in the unit “gets lost.”
The consideration between safety when PALLINI is applied according to protocol and the risk of nosocomial transmission in case of noncompliance underlines one challenge within the implementation of PALLINI. If, due to noncompliance, safety can only be guaranteed by keeping the patient in the room, isolation is the consequence (see Table 1).
Interestingly, it was identified in many interview sequences that the participating nurses did not differ in their parlance between “barrier nursing” due to a multidrug resistant pathogen and “isolation” due to influenza, for example, in both situations they use the word “Iso” (short form for “isolation” in German). This parlance provides a hint that PALLINI is not always followed and in certain situations it is still accepted that patients with multidrug resistant pathogens remain isolated: And I think that’s problematic already, that they can’t really participate in this concept [of the unit as a whole], which we offer here, anymore, as soon as they are in the Iso [here referring to “barrier nursing”], I mean, and I always think that’s a pity. On the other hand, it’s also important that we isolate them and protect the other children and also protect ourselves, of course. B1: Simply for my own safety, but also for that of the other patients on the unit. (MA 04, Abs 15)
Effort
The implementation of barrier nursing involves additional effort for the nurses. Even if PALLINI and, especially, the regulations of barrier nursing were received positively, the implementation “makes everyday life more difficult.” More “communication” with parents and within the team, more “organization and coordination,” and also more “material” is required. The extra material (e.g. disposable gowns and disposable tableware) is considered negative by the nurses particularly due to additional work, the increase of garbage and expenses: a lot of extra work and a lot of waste. And then the waste bag is full, and then the gowns are all gone, and then everyone is just upset. (MA 02, Abs 52)
Furthermore, the participation of the parents of children colonized with multidrug resistant pathogens during meals in the common room represents a recurring challenge. In order to ensure that the regulations for barrier nursing in the common room are adhered to, staff members of the psychosocial team accompany the parents. Nurses are responsible for the organization: Then it’s my job to inquire, “is there a colleague of the psychosocial team, can it take place, yes, no, how many ‘Isos’ do we have, do they all want to eat in the common room?,” so what kind of extra work is that for me? That’s organizational stuff [. . .] That’s a hell of overtime. (MA 09, Abs 177)
Nurses compare their role to ensure compliance with PALLINI with a “watch dog” and perceived this as incriminating and exhausting: [. . .] because, basically, we are responsible for it, because I have also had the experience that the parents don’t inform their visitors at all, they just come to visit and we have to do that and constantly have to go back to it all the time [. . .] that’s just really exhausting. (MA 04, Abs 44)
Especially when several children with an multidrug resistant pathogen are on the unit at the same time, this “monitoring” and “watching” adds to their workload. In addition, the efforts of communication are intensified when the nurses are not sure whether the parents (and visitors) have understood the concept of barrier nursing, due to their current burdensome situation or due to language barriers: It unfortunately happens with families who have a migration background because they often do not understand our language. They read it or they see the educational film [. . .]; we had that the other day with a dad who said: “A beautiful film, a beautiful film.” But he didn’t understand the message. He then went with the gown into the [patients] room, still with the gown on to the child, then outside in the hallway. Unfortunately they do not apply it [the barrier nursing]. And then you have to check again and again and that’s really difficult. (MA 07, Abs 29)
All these additional tasks are associated with an increased expenditure of time, which is lacking for the nurses: [. . .] and I as a nurse don’t have the time to sit next to her all the time and observe, what did she touch, what do I have to wipe off [. . .] Sometimes this is just a side issue for me, where at that moment the other patients on the unit are more important to me. (MA 09, Abs 175)
The time required to monitor families regarding the compliance of PALLINI is lacking due to the care needs of other patients, and the nurses regret, but acknowledge, this (see Table 1).
The nurses also have to weigh the additional effort of themselves and the child and the benefit for the child if, for example, a child can only hold out in a wheelchair for half an hour: [. . .] and because my own time in patient care is simply limited, that’s why I’m less frequently taking patients out of their room in their wheelchair and a gown. I wouldn’t do it, if there wasn’t any help or a volunteer going for a walk or something else, I wouldn’t do it anymore, just because it’s too time-consuming and the cost-benefit calculation doesn’t work afterall. So they stay in their room and sit there in their wheelchair and listen to some music, but they don’t have any social participation anymore. (MA 06, Abs 74)
Due to this conflict of investing time so the patient with a multidrug resistant pathogen can participate, and the lack of (time) resources that might negatively affect the care of other patients, the nurses regard the concept of barrier nursing as “good, but not practical.”
Quality of care
Given that the concept of barrier nursing allows one to enter the room without wearing protective clothing (if no direct patient contact is intended) and to leave the patient’s room door open, the nurses state that, compared with a regular isolation, the concept of barrier nursing facilitates the care of patients: So, if you just have a conversation in passing, this happens regularly. And I think it’s very pleasant that you show yourself as you are. If you do not have direct patient contact and just stand in the room, not touching anything and just standing there as a nurse without a mask and a gown. (MA 06, Abs 22)
The possibility of “open doors” enables the patient to participate in the everyday life on the unit while staying in the room. In certain situations, when nurses weigh up the strain versus benefit for the child, they would decide on leaving the door open instead of bringing the child into the common rooms with a mask. For example, leaving the door open was identified as a good option for patients who have to wear a mask in the common rooms due to a multidrug resistant pathogen colonization in the nose/throat but do not accept the mask. In addition, when the parents are not present an open door allows more participation: I think it is very pleasant when the music therapists say: We will play the piano in the hallway for everyone to hear. B2: Exactly, and I also think the majority have the doors open. And especially when children are unaccompanied, then I wouldn’t close the door either. B1: In that case, if it is possible somehow, we often move the kids towards the door, if the cable is long enough and so on. B2: Or at least have them face outside, that they see us standing here in this area. (MA 06, Abs 118)
Secondary, the open doors enable a better monitoring of the children: [. . .] This also makes a lot of things a bit easier for us, because when children are ventilated for example, we do have the opportunity to open the door, so we are able to hear the ventilation or the children crying. [. . .] (MA 07, Abs 85)
On the downside, the nurses state that due to the concept of barrier nursing, the focus of care moves much more toward compliance with the hygiene guidelines and, thereby, hinder the relationship level especially with the parents. Topics concerning the parents shift to the background and more time is spent explaining and monitoring compliance with the hygiene regulations. In these situations, the attitude shifts from “benevolent empathetic” toward “being the police.” This impaired relationship with parents contrasts the advantage of better care and enhanced participation of the child (see Table 1).
Participation
PALLINI allows maintenance of an important concept of pediatric palliative care, that is, to enable social participation for the patients with multidrug resistant pathogens and their families: [. . .] it was a nice Sunday, so I said ‘let’s take all the kids outside’ and then we just sat out here with all the ‘Iso kids’, all of them on their patios, with their visitors and so on, and that was really lovely. It was a nice atmosphere too. We just had music/ someone brought music, we just turned it up a little and didn’t do more than that. We all just sat and talked and that was so beautiful. (MA 03, Abs 103)
Such situations are reported with gladness and are perceived as “wonderful” and “lovely” by the nurses.
However, despite the possibilities of barrier nursing, nurses also state that “there are restrictions that I regret, because this method does not work with our concept [of care on the unit]. And I think that’s a pity.” (MA 04, Abs 123). For example, an informal contact with a patient with multidrug resistant pathogens, as holding them in the arms or positioning them on the hallway, is only possible to a limited extent or almost impossible. The nurses regret this, because they want to establish as much participation and contact as possible.
The nurses also indicated that informal contact with the parents diminished and that the parents “hole up” in the patient’s room—partly due to social exclusion by other parents: I think it depends on the family. And also on how you are treated in the common room. Are you being treated quite normally, or are you getting strange looks saying: “you are not allowed to touch anything, you have germs.” That’s what I think, and if that goes wrong once and in a negative way, then they don’t come out. (MA 06, Abs 69)
Certainly, the nurses are aware that wearing a gown in the common rooms of the unit is a sign of the current “multidrug resistant pathogen status” to the other parents and staff members. Therefore, the reality of social engagement on the unit may be experienced differently to the ideal participation that is desired by the nurses using this approach. While PALLINI allows normality and participation to a certain extent, the nurses remain ambivalent because this ideal cannot be reached (see Table 1). They perceive high safety standards and participation as conflicting goals: Of course, somehow we’re an intensive care unit (ICU) and have to deal with it hygienically [like an ICU], on the other hand we should somehow be something different, something that lives and that promotes a sense of community. But that doesn’t match. (MA 06, Abs 63)
Discussion
Concerning the nurses attitudes and opinions regarding PALLINI, the following four categories were identified from the interviews (1) safety, (2) effort, quality of care, and (4) participation. All four categories address an ambivalence of the nurses regarding the hygiene concept, as reported by Tiedtke et al. 16 Overall, PALLINI is received positively, but the application is challenging. In spite of the additional work and organizational difficulties due to the concept of barrier nursing, the nurses reported prioritizing social participation for patients with multidrug resistant pathogens as possible, with awareness of enhancing quality of life.
Main findings
A consistently reported obstacle to providing more social participation was the conflict between prioritizing safety and social participation. Participating nurses reported that they experienced a high level of ambiguity, which has also been reported in other studies in adult palliative care.17–19 In particular, the nurses repeatedly pointed out the obstacles of PALLINI implementation.
To warrant safety of hygiene concepts in the pediatric setting, parental participation 20 and, in this study’s context in particular, parents’ compliance with the regulations of barrier nursing are necessary. If this is not guaranteed, there is an increased risk of pathogen transmission. In consequence, often children with multidrug resistant pathogens and their families are isolated and not treated in line with the PALLINI concept. This may also be the reason why the nurses do not differ in their parlance between barrier nursing and isolation. This shows the sizable challenge of the implementation of the new hygiene concept which tries to realize two—by former experiences—contradictory goals.
Increasing parent compliance with the safety regulations presents an additional effort nurses are confronted with. The additional workload of PALLINI conflicts with the lack of time for education and for the monitoring of families reported by nurses. Again, this is comparable to the results of studies on multidrug resistant pathogens in adult palliative care.16,21–24 This has also been reported by Godsell et al. 21 who conclude that time resources are insufficient for educating and monitoring the correct use of protective clothing. The extra effort required for implementation of more complex hygiene concepts is not yet integrated into the compensation system of hospitals, although there are several international studies that recommend an appropriate nursing staff—patient ratio to enhance compliance with hygiene standards25,26 and consequently increase quality of care. 21
An additional barrier to implementation of PALLINI that the nurses in our study perceived was a negative impact of PALLINI in their relationship with parents. This negative impact toward the relationship between staff members and patients has also been reported in a recent study from Tiedtke et al. 16 in the field of palliative and geriatric care and by Godsell et al. 21 in the field of hospital care. A well-working partnership with parents has previously been identified as an important issue in pediatric nursing.27,28 Especially in the field of pediatric palliative nursing, a well-working partnership between nurses and parents is of utmost importance, because in the multidisciplinary team, nurses have a crucial role regarding the 24/7 continuity of care. 29 Within the multidisciplinary team, nurses are the staff members with the most patient contacts. Equally they are mostly the first contact for parents when it comes to questions concerning the care of their child on the unit as well as in the home care setting. Therefore, an impaired relationship with parents affects the quality of care. Lee 27 even identified a well-working partnership as being necessary for the nurses’ work satisfaction, and Godsell et al. 21 depict that a good relationship with the patients (and families) is fundamental for the compliance in barrier nursing.
However, positive aspects of PALLINI were also identified. Nurses reported PALLINI has positive impact on the quality of care. Unlike in prior studies,22,30–32 no delays in the provision of care for patients with multidrug resistant pathogens were reported. This may be due to the possibility of open doors and to enter a patient’s room without wearing protective clothing (if no direct patient contact is intended). The nurses have repeatedly pointed out the positive impact of these two aspects for the quality of care. These two aspects can be applied easily in other pediatric palliative care settings as well as other pediatric health care facilities, and would lead to an improved quality of care for patients colonized with multidrug resistant pathogens. Furthermore, social participation for patients, who are colonized with multidrug resistant pathogens, and their families would be enhanced and consequently social exclusion could be decreased.
Overall, applying PALLINI allows increased social participation. Reduced health care provider/patient contact in isolated patients,5,30,32–34 resulting in a negative impact on the patients’ mood due to the isolation,19,35,36 can therefore be prevented. However, the nurses continue to desire more participation and contacts to the families.
It will be an important task in the implementation of complex hygiene concepts for patients colonized with multidrug resistant bacteria to identify strategies to overcome certain ambivalences by the staff members and to provide more resources in order to be able to realize even more participation, which is the main goal of pediatric palliative care. 8
Strength/limitations
Anonymous interviews conducted by a member of the research team allowed nurses to honestly state their opinion about PALLINI. Results capture the core issues in the nurses’ application of the hygiene concept. The identified categories are therefore comparable to other hygiene interventions in other pediatric palliative care settings. However, this study is limited by the limitations inherent in qualitative research such as transferability and generalization. Furthermore, results of this study cover just the nurses’ point of view. Further research should be done to determine the perception of the affected families and other pediatric palliative care professionals regarding hygiene concepts for patients colonized with multidrug resistant pathogens. This explorative study, nevertheless, emphasizes the need for ongoing discussion and further research on best practice for addressing multidrug resistant pathogen infections in the pediatric palliative care setting.
What this study adds
A social-participation focused hygiene program was considered positively by the nurses; however, results of this study demonstrate that complex hygiene concepts represent a challenge for the nurses and require additional time resources.
Footnotes
Acknowledgements
We would like to thank the study participants for their time and openness in discussing this complex topic. We also thank Donnamay Brown for English editing.
Author contributions
P.S., J.W., C.H., and B.Z. contributed for the study design; the data acquisition was done by A.H.-P.; the data analysis was done by P.S. and A.H.-P.; the article was drafted by P.S. and A.H.-P.; critical revision of the article was done by J.W., C.H., and B.Z.; and the approval of the manuscript version to be published was done by P.S., A.H.-P., J.W., C.H., and B.Z.
Data management and sharing
The data sets used and analyzed during this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the German Federal Ministry of Education and Research (grant no. 01GY1713).