
Abstract
Background:
Patient empowerment, defined as ‘a process through which people gain greater control over decisions and actions affecting their health’ (World Health Organization) is a key theme within global health and social care strategies. The benefits of incorporating empowerment strategies in care are well documented, but little is known about their application or impact for patients with advanced, life-limiting illness(s).
Aim:
To identify and synthesise the international evidence on patient empowerment for adults with advanced, life-limiting illness(s).
Design:
Systematic review (PROSPERO no. 46113) with critical interpretive synthesis methodology.
Data sources:
Five databases (MEDLINE, Embase, CINHAL, PsycINFO and Cochrane) were searched from inception to March 2018. Grey literature and reference list/citation searches of included papers were undertaken. Inclusion criteria: empirical research involving patients with advanced life-limiting illness including descriptions of, or references to, patient empowerment within the study results.
Results:
In all, 13 papers met inclusion criteria. Two qualitative studies explored patient empowerment as a study objective. Six papers evaluated interventions, referencing patient empowerment as an incidental outcome. The following themes were identified from the interpretive synthesis: self-identity, personalised knowledge in theory and practice, negotiating personal and healthcare relationships, acknowledgement of terminal illness, and navigating continued losses.
Conclusion:
There are features of empowerment, for patients with advanced life-limiting illness distinct to those of other patient groups. Greater efforts should be made to progress the empowerment of patients nearing the end of their lives. We propose that the identified themes may provide a useful starting point to guide the assessment of existing or planned services and inform future research.
Keywords
Healthcare systems globally are faced with the challenge of how best to support growing older populations with complex medical and social needs.
Models of care incorporating patient empowerment strategies are being increasingly adopted in response to these population changes with the aim of alleviating the impact of morbidity on people’s lives and reducing the demands placed on health and social care services.
Little is known about the application or impact of empowerment strategies for patients with advanced, life-limiting illness(s).
To our knowledge, this is the first review to explore the concept of patient empowerment for adults living with advanced, life-limiting illness.
There are features of empowerment, for patients with advanced life-limiting illness, distinct to those of other patient groups. Key differences relate to the continued physical and psychosocial challenges this group encounter, producing contrasting patient empowerment foci.
Our review found no evidence of attempts to incorporate patient empowerment into the design or evaluation of services that support people with advanced life-limiting illness.
We would propose that the identified themes and conceptual model produced in review may provide a useful starting point to guide the assessment of existing services and development of a new dialogue surrounding patient participation in the design of services and interventions.
Background
The impact of the continuing rise in global average life expectancy is already apparent in many countries with growing older populations with complex medical and social needs.1–3 The concept of ‘patient empowerment’ has gained traction in recent years, responding to these population challenges with the aim of alleviating the impact of morbidity on people’s lives and limiting the demands high levels of morbidity place on health and social care services. 4
There are various definitions and applications of patient empowerment (termed ‘patient activation’, in some texts) used within healthcare, with the largest body of research in long-term conditions. Here, the empowerment paradigm involves patients reclaiming their responsibilities to improve and maintain their health, in parallel with a reformation of the patient–doctor relationship4–6 that encourages equitable partnerships over an authoritative dynamic. 7 Self-management and self-efficacy are key features within the majority of patient empowerment constructs, with a growing number of measures used in practice to assess, monitor and promote these qualities.5,8,9 There is increasing evidence that patient empowerment is effective and beneficial. Helping patients to achieve improved health states reduces the impact on services and engenders continued participation and motivation from healthcare professionals (HCPs) and patients.10,11 Consequently, patient empowerment has gained the attention of policy makers on a global scale, with mandates for, and investment into, initiatives and service structures to empower patients now commonplace.12–15
Existing empowerment tools and models assume a degree of reversibility to patients’ health states and/or the potential to inhibit the progression of a negative health state by means of improved self-care, lifestyle choices and relations with HCPs and services.5,8,11,16 From the perspective of advanced illness, when there is not the potential for health gains, or when disability impedes function and capacity to self-manage and forces dependency on others, these tools and models may cease to be appropriate. This results in this population being inappropriately assessed and subsequently underserved.
This review intends to appraise the international evidence surrounding definitions and/or concepts pertaining to patient empowerment for persons living with advanced, life-limiting disease, with the aim of understanding whether patients can still be ‘empowered’ in the context of advanced, terminal illness and/or whether these patients fall outside of the measures, models and services designed around the current understanding and constructs of ‘patient empowerment’.
Research questions
How has empirical research defined ‘patient empowerment’ for adults in the advanced stages of a life-limiting illness.
What factors/themes are associated with patient empowerment for adults in the advanced stages of a life-limiting illness.
Which interventions or exposures seek to support or promote patient empowerment for adults in the advanced stages of a life-limiting illness.
Methods
Design
We followed systematic review best practices to formulate a search strategy underpinned by study objectives and inclusion criteria, as specified in our registered protocol. 17 Which is combined with critical interpretive synthesis 18 methodology to integrate data across studies.
Critical interpretive synthesis methodology, developed by Dixon-Woods et al., 18 is an iterative approach designed to appraise and synthesise complex and heterogeneous quantitative and qualitative evidence, in a bid to develop a novel definition, concept or theory. We specifically selected this method for its ability to inform the review question, identification and selection of evidence, as well as synthesis of evidence. The orientation of critical interpretive synthesis towards theory generation makes its practice distinct from that of meta-ethnography and other qualitative synthesis methods.
We adopted this methodology based on the findings of our initial scoping of the literature, which aimed to identify empirical research on empowerment for adults in the advanced stages of a life-limiting illness This exercise identified a small body of literature of methodological heterogeneity, highlighting the challenges of attempting to collate and synthesise evidence where the phenomenon of interest is not well specified and where evidence is very heterogeneous in both type and purpose. These findings, and our aim to contrast our results with existing evidence on empowerment for other patient groups and to build conceptual understanding, informed our decision to conduct a critical interpretive synthesis, rather than use traditional aggregative review methodology. This enabled insights into the concepts underpinning empowerment to emerge through an iterative, dynamic and critical synthesis of the literature.
Search strategy
Search terms (Appendix 1) were generated from the existing research and theoretical literature surrounding patient empowerment and activation.4,6,16,19,20 We subsequently trialled various combinations of concept headings and search terms before settling on a broad search strategy, accepting that we would obtain a large volume of papers of high specificity and low sensitivity.
Screening papers for inclusion was performed by D.W., with queries pertaining to inclusion discussed with F.E.M.M.
Data sources
The following databases were searched from inception to week 2 March 2018: MEDLINE, Embase, CINAHL, PsycINFO and The Cochrane Database of Systematic Reviews. We also searched Grey literature (Open Grey Database), reference lists of included papers and relevant systematic reviews identified during screening. Pre-determined inclusion and exclusion criteria were applied during screening.
Inclusion criteria
Empirical research included descriptions of, or references to, patient empowerment within their results, irrespective of whether empowerment featured in the objectives of the study. Included studies report solely on adult patients (>18 years of age) with end-stage, advanced, terminal and/or life-limiting illness and/or who were defined as receiving non-curative management or palliative care support. We utilised the master search strategy developed by Sladek et al. 20 to support the capture of literature relevant to palliative care in general medical journals.
We included studies incorporating a mix of participants, including informal carers and HCPs, only in circumstances where patient reported data could be separated and extracted. In recognition of variations in service provision and healthcare constructs internationally,21,22 we selected to focus on features of empowerment specific to patients.
For the purposes of the interpretative review, we retained and kept separately papers, identified during screening, that were clearly concerned with aspects of patient empowerment but included participants with a mixture of both advanced life-limiting disease and a range of other disease states/stages. These papers were later used to compare empowerment themes between the other disease groups and patients with advanced life-limiting disease to support the dialectic processes of the interpretive review.
Exclusion criteria
To capture generalisable features of empowerment in this patient group, we excluded studies with single decision-specific foci, for example, decisions to withdraw dialysis and advance care planning for single-disease groups. Conference abstracts and non-empirical papers were also excluded. There were no language limitations.
We excluded fatally flawed papers identified using the quality appraisal criteria (as cited by Dixon-Woods et al. 18 ):
Are the aims and objectives of the research clearly stated?
Is the research design clearly specified and appropriate for the aims and objectives?
Do researchers provide a clear account of the process by which their findings were produced?
Do the researchers display enough data to support their interpretations and conclusions?
Is the method of analysis appropriate and adequately explicated?
Each potentially included paper was scrutinised, using these criteria, and discussed by at least two of the authors (D.W., J.B. and F.E.M.M.) before deciding on inclusion or exclusion.
Synthesis
First, we considered the context and potential influences and assumptions that underpinned the results related to empowerment. Second, we contrasted the data against the retained purposive selection of papers that included a mixture of participants with both advanced life-limiting disease and a range of other disease states/stages. We contrasted papers to observe and address any gaps, to ensure that the papers solely describing our population of interest were adequately addressing the subject matter, while also constantly testing and challenging our emerging theories against the available evidence for other patient populations. Third, we mapped the results to a variety of existing frameworks and models of empowerment originally designed for patients with long-term conditions and/or non-specific patient groups.4,5,16,23,24 This process, which involved repeated evaluation and testing of the data, created opportunities to observe whether interpretations altered when applying a variety of perspectives during the mapping process. This exposed the contrasting features of empowerment for our population of interest when compared to the patient groups represented by the models and frameworks. The mismatch between existing models and our data demonstrated the inadequacy of the models in describing patient empowerment in advanced disease and prompted our generation of a new conceptual model.
Of the included studies, 25% were randomly selected and dual coded (J.B. and D.W.) to enhance reliability alongside regular meetings to discuss all aspects of the design and conduct of this review (D.W. and F.E.M.M.).
Results
A total of 20,591 papers were screened, but only 13 papers met our inclusion criteria after quality assessment (Figure 1). Countries represented across the 13 papers were the United Kingdom (n = 5),25–29 the United States (n = 3),27,30,31 Australia (n = 3),31–33 Ireland (n = 2),27,34 the Netherlands (n = 1) 35 and Norway (n = 1). 36 There were seven qualitative studies and six mixed method studies, the characteristics of which are summarised in Tables 1 and 2, respectively.
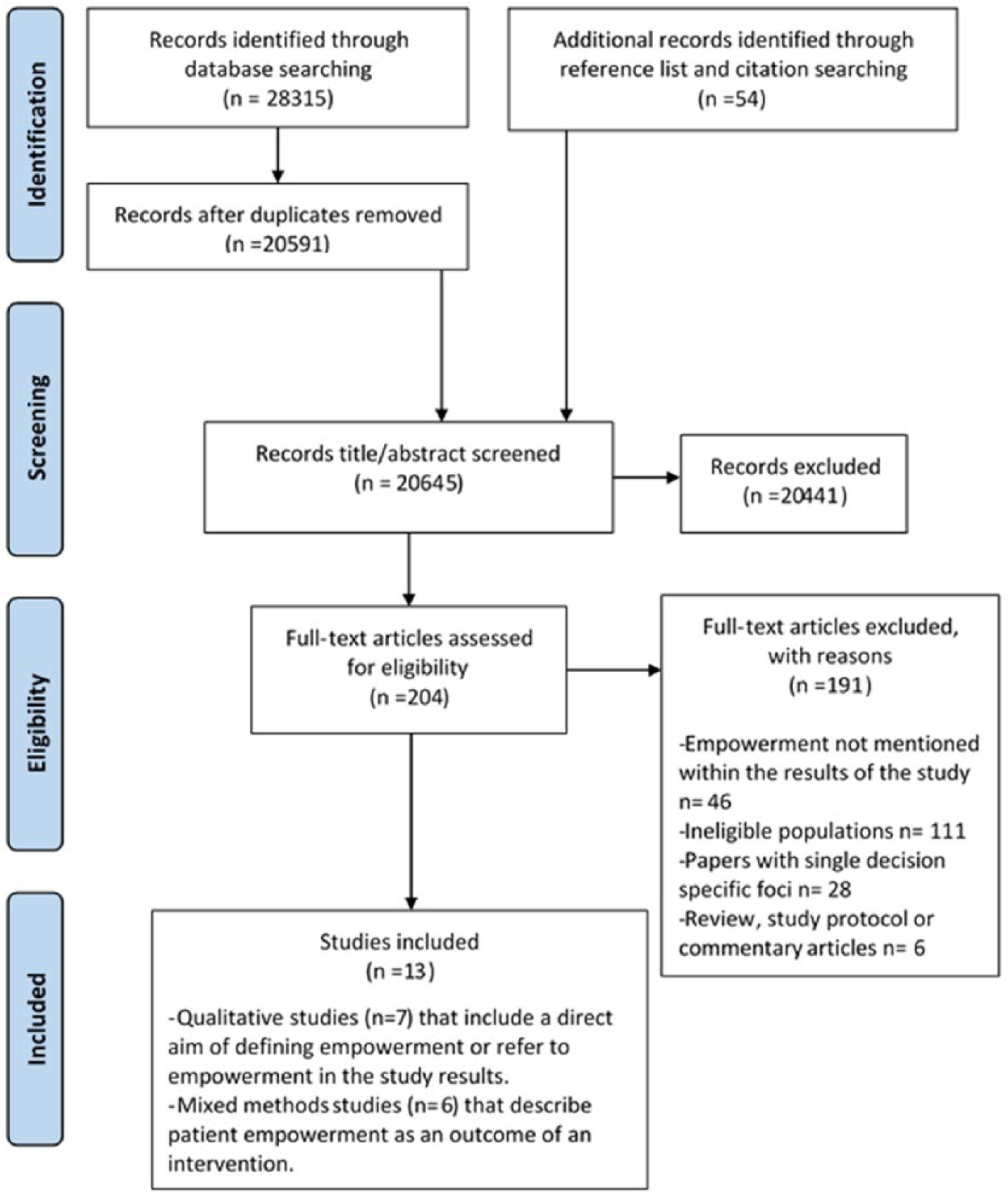
PRISMA flow diagram.
Qualitative studies – results.
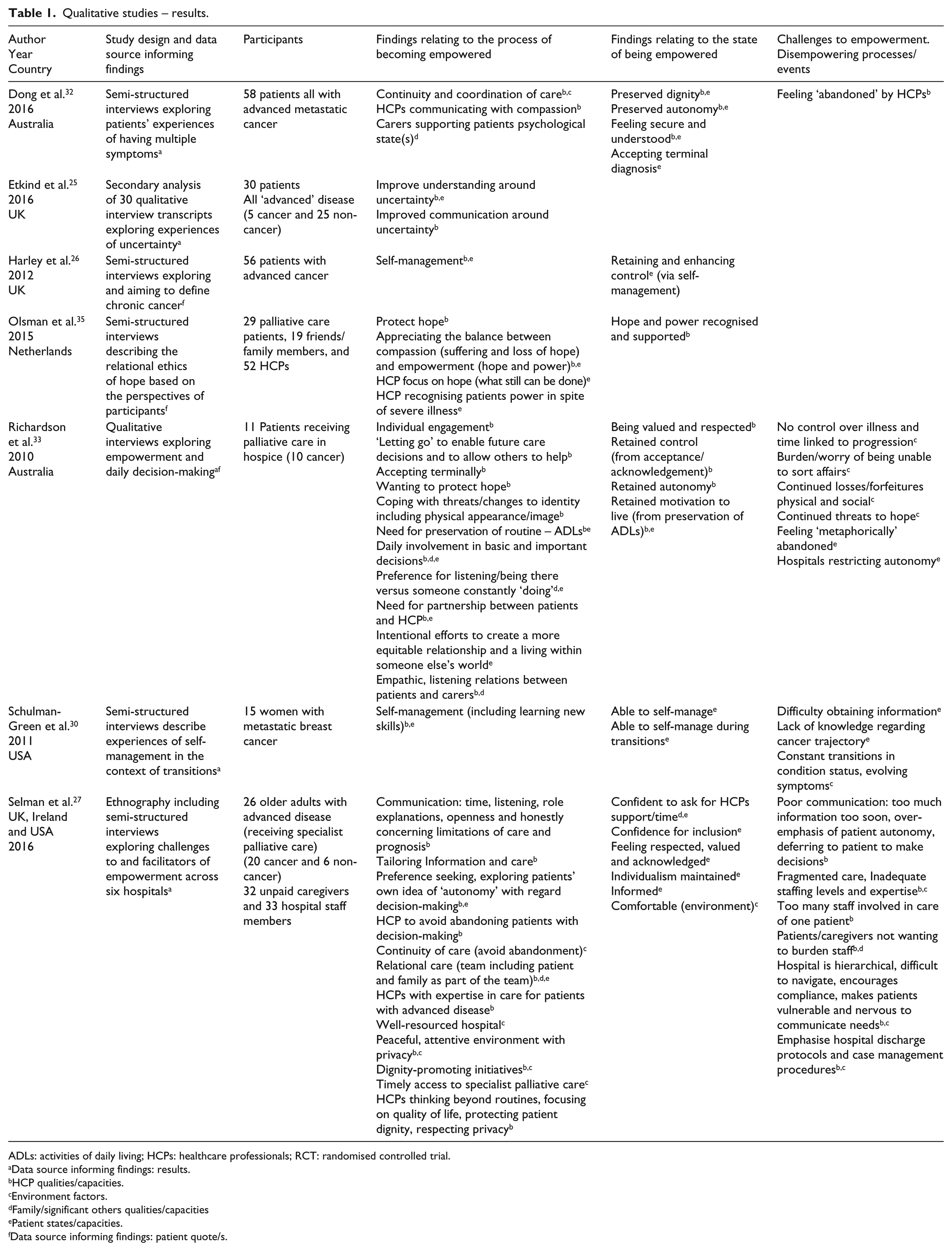
ADLs: activities of daily living; HCPs: healthcare professionals; RCT: randomised controlled trial.
Data source informing findings: results.
HCP qualities/capacities.
Environment factors.
Family/significant others qualities/capacities
Patient states/capacities.
Data source informing findings: patient quote/s.
Mixed methods studies- Results.
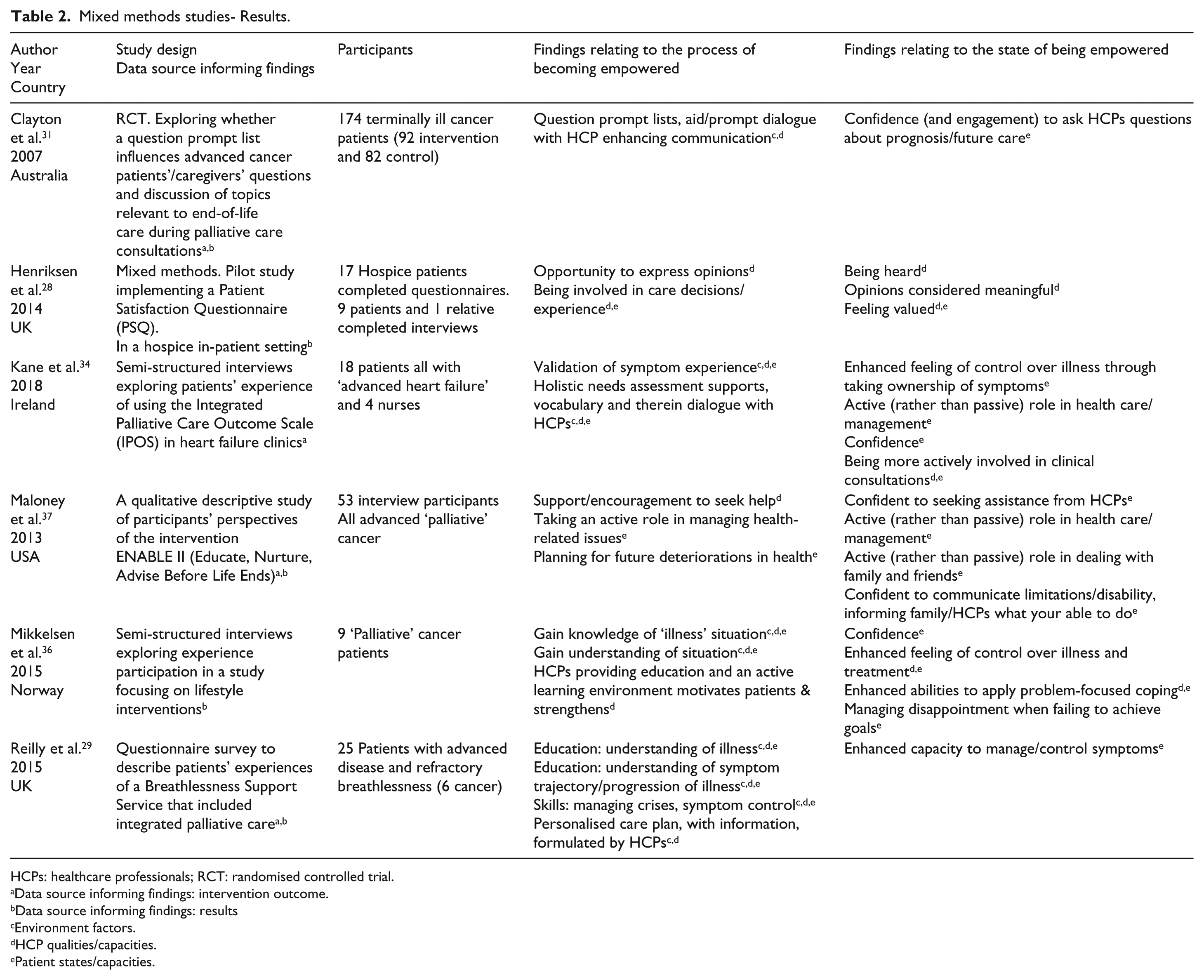
HCPs: healthcare professionals; RCT: randomised controlled trial.
Data source informing findings: intervention outcome.
Data source informing findings: results
Environment factors.
HCP qualities/capacities.
Patient states/capacities.
Data were of three types: patient quotes,27–29 the author’s words when discussing the study results25, 26, 29–33, 35–37 and the reported outcome/s of interventions. Of the 13 studies, 7 included participants with cancer diagnoses, while the remaining 6 included a mix of cancer and non-cancer patient groups. No discernible differences were identified between the cancer and non-cancer groups with respect to patient empowerment.
Two papers had the stated aim of exploring empowerment in our population of interest.27,33 We were unable to identify any interventions designed with the specific aim of empowering patients with advanced disease. Six papers evaluated interventions, referencing patient empowerment as an incidental outcome.28,29,31,34,36,37 The remaining five papers, referencing empowerment within their results, were qualitative studies exploring living with multiple symptoms, 32 experiences of uncertainty, 25 the concept of chronic cancer, 26 relational ethics of hope 35 and experiences of self-management. 30
The interventions associated with empowering patient outcomes included single-component interventions (Question Prompt Lists, Patient Satisfaction Questionnaires and a Patient-Reported Outcome Measure) and complex interventions (Breathlessness Support Service, lifestyle interventions and multi-component educational and care management palliative care intervention).
Our critical interpretative synthesis generated five overarching themes, illustrated in Table 3 (Appendix 2) and discussed in the following. The proposed conceptual model (Figure 2.) illustrates the interplay and relationships of these themes.
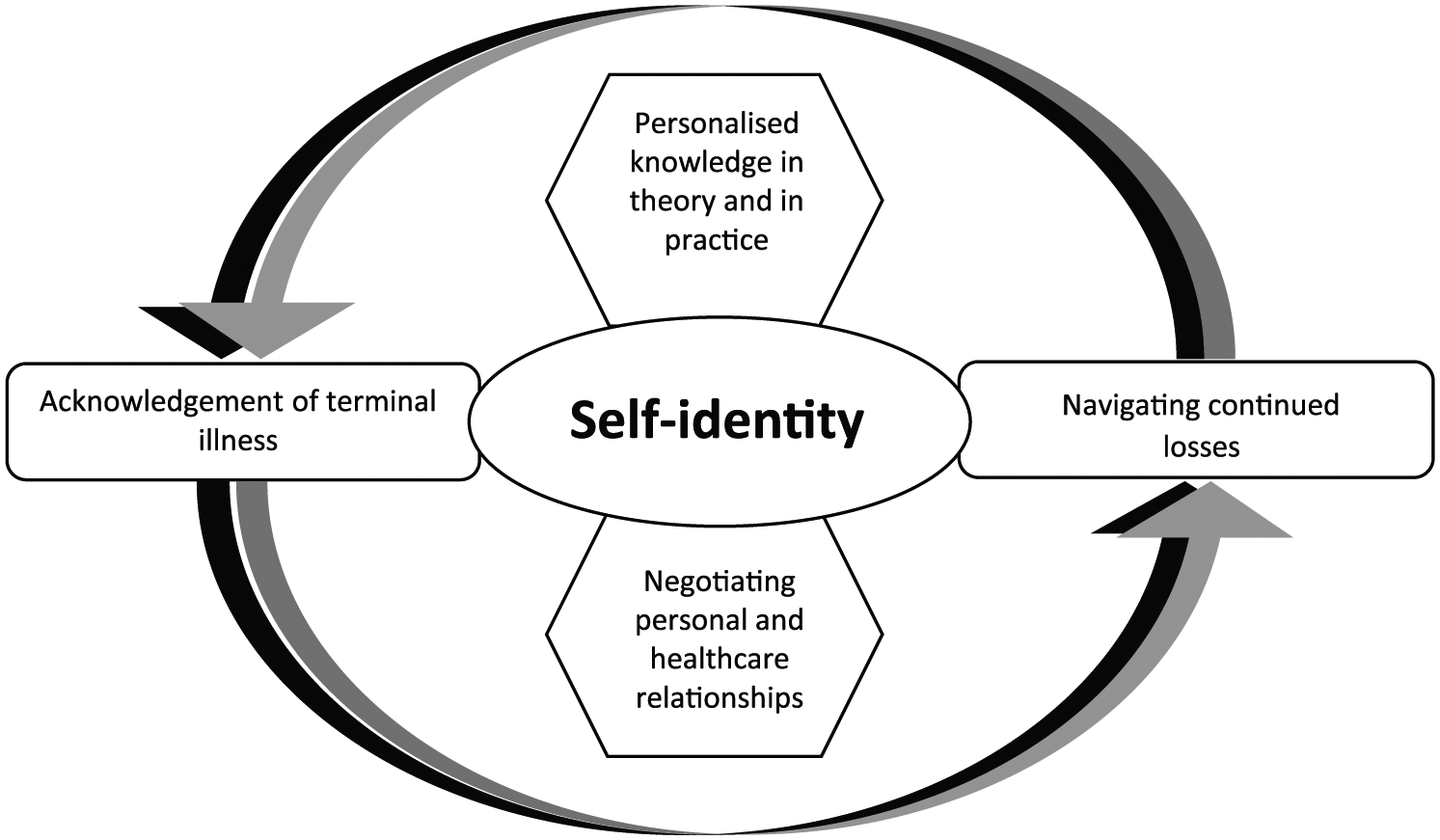
Proposed conceptual model of patient empowerment for adults with advanced life-limiting illness.
Self-identity
Eight papers described the importance of self-identity as both a process to becoming empowered and being empowered. Self-identity, in the context of empowerment, reflects the beliefs a patient has about themselves, expressed, although not exclusively, in terms of self-esteem, self-image and ideal-self.
Maintaining routines, particularly with respect to personal-care activities, positively benefitted autonomy and self-esteem, reinforced by HCPs or families encouraging patient involvement in daily basic and important decisions. Maintaining a daily schedule was also described as a motivating element to ‘keep living in the face of death’. 33 However, the ability for patients to control or partake in daily basic care activities was challenged by the timetabling of care and imposition of non-negotiable health and social care both in community and hospital settings.27,33 This blanket caregiving created a ‘defy or comply’ response from patients, depending on their strength and/or confidence to challenge professionals. 33
Receiving the respect of others, reflected in being acknowledged, and being afforded privacy and inclusion despite disability were key features of empowerment.27,28,33,36 Experiencing overt changes to one’s physical appearance, described by one patient as ‘shrinking’, poses a significant threat to confidence and generates a fear that others will fail to recognise patients’ power, identity and capabilities as bodies transform. 33
Personalised knowledge in theory and in practice
The need for personalised illness education that emphasises the pathophysiology of symptoms to support understanding of symptom management emerged as a component of becoming empowered. Merely providing knowledge and skills around symptom management was highlighted as insufficient. 27 Personalised information provision, at the patient’s pace, that included the expected symptom trajectory and more generally ’what to expect’, was reportedly empowering.29,30
Mikkleson et al. 36 report on the benefits of a ‘healthy’ lifestyle educational intervention, emphasising the continued desire to be ‘healthy’ and make ‘healthy choices’ even in the advanced stages of illness, as a mechanism for regaining control, which promoted confidence and coping. The need to personalise and pace these approaches was also reported after patients expressed feelings of guilt when failing to achieve mutually designed ‘goals’. 36
In congruence with the findings from other patient populations, having knowledge and skills encouraged patient participation in self-management, enhancing confidence and renewing a sense of self-responsibility and motivation.26,29,34,36 In contrast, desire for self-management education was often tempered by the patient’s ‘ability’ to consider further, inevitable losses. In this patient group, self-management education should be delivered sensitively and in a personalised manner which respects changes in capacities, capabilities and priorities over time.
Negotiating personal and healthcare relationships
Eight studies explored features of personal and healthcare/professional relationships that enabled and sustained a sense of empowerment for patients. The qualities advocated applied to HCPs, families, informal carers, patients and services, with the synergy between these groups integral in the attainment of empowerment. Empowering partnerships were fostered by families and HCPs ‘being and listening’ rather than ‘doing’, reinforcing equality, respect and therein the patient’s self-identity.31–33,37 Central to these partnerships was engaging patients in their care rather than resigning them to a passive role in paternalistic, overly nurturing relationships. Owing to the deleterious effects of advancing disability, relationships and roles needed constant re-evaluation. In this context, empowered exchanges involved patients negotiating the offers of support from HCPs or families and protecting the proportion of the proposed activity that can be achieved independently.33,36
HCPs needed to communicate in an unrushed, empathic, honest and inclusive fashion,31,32 tailoring patient-centred decision-making to support the preferences and values of the patient over time. Clinicians over-emphasising patient choice/autonomy in efforts to empower patients (e.g. by ‘dumping’ information on them rather than collaborating in decision-making), conversely resulted in patients feeling abandoned and disenfranchised. 31 In addition, respecting the preference of some patients to pass on responsibility for decision-making can be an empowering demonstration of wishes for patients. 31
There is evidence that for some patients, desire for open and honest communication can be restricted by the fear of losing hope, based on either previous experience or an expectation of clinicians censoring hope when communicating with complete honesty in the context of life-limiting illness. This is reflected in the works of Richardson et al. 33 and Olsman et al. 35 where patients describe the desirable ability of HCPs to ‘protect hope’ to enable patients to retain a degree of positivity for the future in spite of their prognosis.
Possessing the confidence to seek help from others, both family and HCPs, was also a feature of empowerment.28,31,34,36,37 Obtaining permission to seek the help was intrinsic to this process, three of the included studies described interventions that supported patients’ interaction and discussions with HCPs.31,34,37
Acknowledgement of terminal illness
Studies described a point where by patients acknowledged their impending death, inclusive of the stark realities of what that might mean for their physical and mental capacities, in order to regain a sense of control. In this context, control was signified through sorting affairs and making decisions in response to the limitations placed on their life expectancy. 25 Control was also manifested through patient-led ‘handing over’ of physical tasks to family or HCPs to facilitate the reassignment of energy to alternative tasks/focuses. 33 While one study stated that empowerment could not truly be achieved without people acknowledging their mortality and the consequences of progressive disability, 30 others provided examples of patients feeling empowered, having stated their wish to avoid discussions around their mortality and future losses. 33
Navigating continued losses
Adaptation to, and coping with, continuous physical and social losses was cited as a key feature of becoming and being empowered in five papers. Adaptation was achieved through changing priorities, sorting personal affairs and planning for further deteriorations.25,27,30 Coping involved refocusing on small daily tasks. 33
Having hope was central to the patient’s capacity for adaptation and coping, with hope a motivating element to ‘go on’ as losses continued to manifest. 33 The fragility of hope and therein one’s ability to cope and continue was recognised as being under continuous threat. 30
Possessing the skills and capacity to continually adapt, and remain resilient to, loss provided opportunity to achieve or regain a sense of feeling ‘in control’. 30 The presence or absence of control thus emerged as a key moderator to being or becoming empowered.
Themes within the conceptual model
‘Self-identity’, as a central feature of patient empowerment, includes preserving, enhancing and communicating self-identity. It reflects the importance placed on identity for self (the patient), relationships and society. In the theoretical model, each theme has a potentially mutually influential relationship with self-identity.
An example of this is demonstrated by Richardson et al. in their qualitative interview study exploring issues surrounding empowerment and daily decision-making with 11 terminally ill hospice in-patients. Patients associated negotiating offers of care and inclusion in therapeutic relationships with strengthened self-identity; this mitigated the challenges to self-image and self-identity produced by the negative appearance-altering manifestations of their illness. 33
Olsman et al. investigated the relationship between hope and empowerment through interviews with 29 patients receiving specialist palliative care support. Patients needed HCPs to convey hope of what still can be done. Patients ‘having hope’ were protective against the reality of terminal illness, including potential functional losses. Retaining hope consequently enhanced capacities to acknowledge and manage transitions in their illness and made patients feel more powerful. This resulted in HCPs ‘recognising patients own power, in spite of severe illness’. 35
‘Acknowledgement of terminal illness’ and ‘Navigating continued losses’ themes within the model represents features felt by patients to be inescapable in the advanced stages of life-limiting illness. These, like all the themes identified, were expressed to different degrees within the literature. An example is provided by Olsman et al. 35 when a patient, not wishing to acknowledge her terminal diagnosis with HCPs, communicated this preference to help negotiate these relationships and felt empowered as a result.
‘Personalised knowledge in theory and in practice’ and ‘Negotiating personal and healthcare relationships’ include features of empowerment conceptualised as being optional for patients to engage with and, when engaged, open to influence by patients themselves.
Discussion
Summary of main findings
To our knowledge, this is the first review to explore the concept of patient empowerment for adults living with advanced, life-limiting illness. Principally, we have identified that while there is a paucity of research in this area, the evidence available demonstrates the differences in the factors/themes associated with patient empowerment for adults in the advanced stages of a life-limiting illness in comparison to other patient groups. Key differences relate to the continued physical and psychosocial challenges this group encounter, producing contrasting patient empowerment foci and outcomes.
Distinct for our population of interest is the experience of continued insults and resultant losses that occur within short periods of time. Empowerment, when you are dying, includes the capacity to withstand insults and losses which may compromise, in particular, a patient’s self-identity. Protecting self-identity is central to empowerment for this group and represents a key motivator to ‘continue living’, 33 in comparison to other patient groups, where enhanced or sustained health states are seen as both a motivator and outcome of empowerment.4,38,39
From the literature focused on patients with long-term conditions (the group that empowerment strategies have largely evolved to target), a key empowerment outcome is aimed towards enhancing patients ‘feelings of control over their illness’.5,13,15 In contrast, an outcome or focus for empowered patients with terminal illness appears to centre around self-identity, as opposed to control of their illness or health state(s). For example, this review found that patients placed stronger emphasis on the benefits of equitable therapeutic relationships with HCP with respect to self-identity (feeling respected and valued),27,33,35 rather than focusing on the product of that relationship being to enhance their ‘feelings of control over their illness’.
Furthermore, relationships with HCP and families, for this group, evolve more readily owing to persistent losses and often inevitable physical or cognitive dependency. There is a delicate need for shifting responsibilities over time, with points at which the patient ‘hands over’ increasingly to others. Recognising evolving physical limitations and letting others ‘do’ can instil a sense of control so long as it is balanced and paced to the patients preference and is not restricted by timetabled, non-personalised care. This is in contrast to the focus on persistently equal relations and responsibilities for HCP/families and patients in other groups.4,7,15
Our review identified just two papers that sought to explore empowerment as a study objective.27,33 Richardson et al. explored the meaning of empowerment and decision-making from the perspectives of 11 patients in receipt of specialist palliative care support, while Selman et al. studied the challenges to and facilitators of empowerment in an ethnographic study interviewing 26 patients aged ⩾65 years receiving specialist palliative care. Both papers communicate the emphasis placed, by patients, on relationships and services that enable them to attain and retain respect, acknowledgement and inclusion.
We did not identify any papers evaluating interventions designed to empower patients with advanced disease. The five mixed method studies that evaluated interventions referenced empowerment as an incidental outcome. In contrast, Bravo et al. 4 identified 67 studies with published definitions of patient empowerment for patients with long-term conditions. Barr et al. 5 identified 30 studies on 19 measures of empowerment for a range of patient groups, although none designed specifically for patients with advanced, life-limiting conditions.
Limitations
The terms ‘patient empowerment’ and ‘patient activation’ largely occur within research and policy in developed, high-income countries and might not translate across all countries and cultures. We retained studies that exclusively included and defined patients as being in the advanced stages of life-limiting illness. Not all papers report the phase/stage of illness of participants, so we might have missed papers that might have contributed to the aims of this study.
Implications for policy, research and practice
Our review found no evidence of attempts to incorporate patient empowerment into the design or evaluation of services that support people with advanced life-limiting illness. In contrast, there is a significant body of work in this area for patients with long-term conditions and as part of population health-promotion strategies.12,13,40,41
We suggest, based on the findings from this review, that current programmes and measures of patient empowerment may not be wholly applicable to patients with advanced, life-limiting disease. First, many of these existing approaches assume a role for prevention of negative health states or promotion of lifestyle measures to benefit health states. 15 Second, there is little research addressing and/or managing the irreversible aspects of health states. 40 Third, there may be additional dimensions and aspects of empowerment in advanced illness, as described in the opening of our discussion. On this basis, we would argue that presently there is no reliable and valid way to assess whether existing services and structures are or are not empowering to patients with advanced, life-limiting disease.
The findings of this review highlight the desire of many patients to remain actively involved in decisions about, and in the practice of, their care. To this effect, we suggest that services should aim to support and promote empowerment. The emerging use of discrete choice experiments in service assessment and design42,43 may offer a method to maintain patient inclusion and support the generation of services that will benefit patient empowerment in tandem. In addition, interventions shown to empower patients should be incorporated into routine practice; these include interventions that support patient and HCP dialogue28,31 and involve personalised lifestyle and self-management advice.29,36,37
Conclusion
This review provides an evidence base and conceptual model to inform future research into patient empowerment for patients with advanced life-limiting illness. Being an ‘empowered patient’, when living with advanced life-limiting illness is different to the experience and meaning of empowerment for other patient groups. ‘Patient empowerment’ emerges as a metaphor for all that enables people to maintain their self-identity until the very end of life.
Considering the benefits of services and programmes designed to empower patients in other groups, further research is needed to ensure end-of-life care is optimally empowering. We would propose that the themes of this review may provide a useful starting point to guide the assessment of existing services and development of a new dialogue surrounding patient participation in the design of services and interventions.
Footnotes
Appendix 1
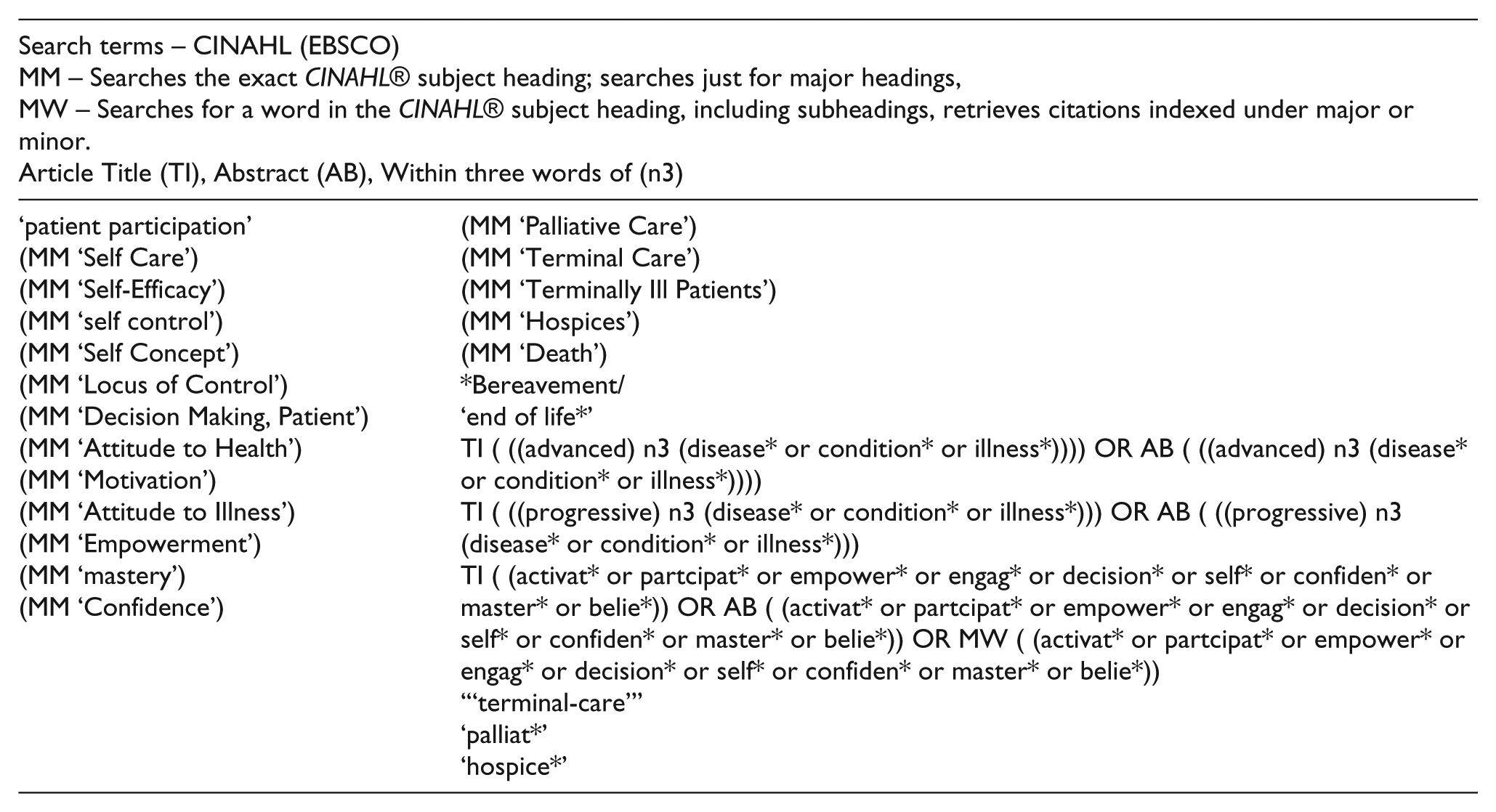
| Search terms – CINAHL (EBSCO) MM – Searches the exact CINAHL® subject heading; searches just for major headings, MW – Searches for a word in the CINAHL® subject heading, including subheadings, retrieves citations indexed under major or minor. Article Title (TI), Abstract (AB), Within three words of (n3) |
|
| ‘patient participation’ (MM ‘Self Care’) (MM ‘Self-Efficacy’) (MM ‘self control’) (MM ‘Self Concept’) (MM ‘Locus of Control’) (MM ‘Decision Making, Patient’) (MM ‘Attitude to Health’) (MM ‘Motivation’) (MM ‘Attitude to Illness’) (MM ‘Empowerment’) (MM ‘mastery’) (MM ‘Confidence’) |
(MM ‘Palliative Care’) (MM ‘Terminal Care’) (MM ‘Terminally Ill Patients’) (MM ‘Hospices’) (MM ‘Death’) *Bereavement/ ‘end of life*’ TI ( ((advanced) n3 (disease* or condition* or illness*)))) OR AB ( ((advanced) n3 (disease* or condition* or illness*)))) TI ( ((progressive) n3 (disease* or condition* or illness*))) OR AB ( ((progressive) n3 (disease* or condition* or illness*))) TI ( (activat* or partcipat* or empower* or engag* or decision* or self* or confiden* or master* or belie*)) OR AB ( (activat* or partcipat* or empower* or engag* or decision* or self* or confiden* or master* or belie*)) OR MW ( (activat* or partcipat* or empower* or engag* or decision* or self* or confiden* or master* or belie*)) ‘“terminal-care”’ ‘palliat*’ ‘hospice*’ |
Appendix 2
Study findings related to empowerment mapped to themes.
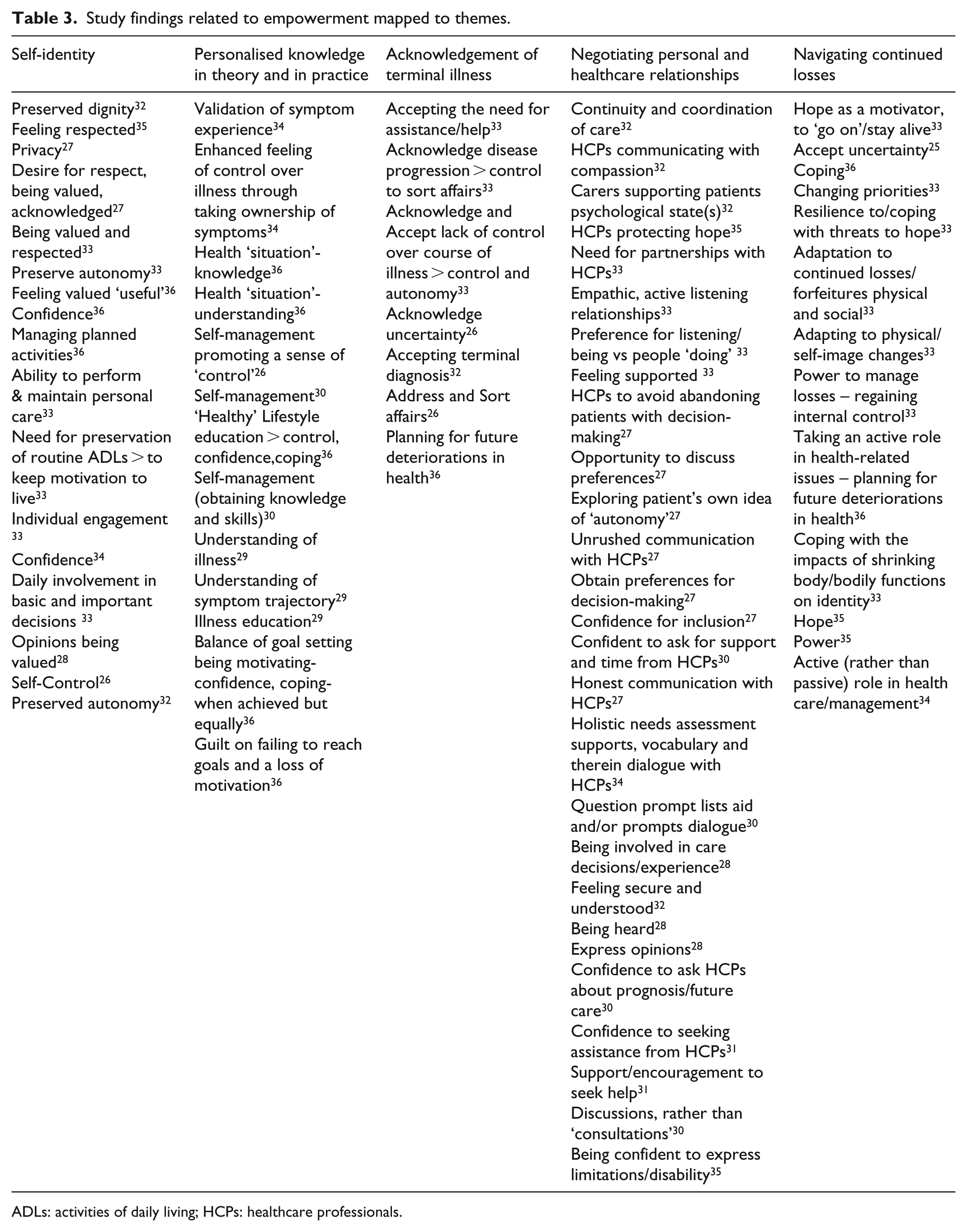
| Self-identity | Personalised knowledge in theory and in practice | Acknowledgement of terminal illness | Negotiating personal and healthcare relationships | Navigating continued losses |
|---|---|---|---|---|
| Preserved dignity
32
Feeling respected 35 Privacy 27 Desire for respect, being valued, acknowledged 27 Being valued and respected 33 Preserve autonomy 33 Feeling valued ‘useful’ 36 Confidence 36 Managing planned activities 36 Ability to perform & maintain personal care 33 Need for preservation of routine ADLs > to keep motivation to live 33 Individual engagement 33 Confidence 34 Daily involvement in basic and important decisions 33 Opinions being valued 28 Self-Control 26 Preserved autonomy 32 |
Validation of symptom experience
34
Enhanced feeling of control over illness through taking ownership of symptoms 34 Health ‘situation’-knowledge 36 Health ‘situation’-understanding 36 Self-management promoting a sense of ‘control’ 26 Self-management 30 ‘Healthy’ Lifestyle education > control, confidence,coping 36 Self-management (obtaining knowledge and skills) 30 Understanding of illness 29 Understanding of symptom trajectory 29 Illness education 29 Balance of goal setting being motivating-confidence, coping-when achieved but equally 36 Guilt on failing to reach goals and a loss of motivation 36 |
Accepting the need for assistance/help
33
Acknowledge disease progression > control to sort affairs 33 Acknowledge and Accept lack of control over course of illness > control and autonomy 33 Acknowledge uncertainty 26 Accepting terminal diagnosis 32 Address and Sort affairs 26 Planning for future deteriorations in health 36 |
Continuity and coordination of care
32
HCPs communicating with compassion 32 Carers supporting patients psychological state(s) 32 HCPs protecting hope 35 Need for partnerships with HCPs 33 Empathic, active listening relationships 33 Preference for listening/being vs people ‘doing’ 33 Feeling supported 33 HCPs to avoid abandoning patients with decision-making 27 Opportunity to discuss preferences 27 Exploring patient’s own idea of ‘autonomy’ 27 Unrushed communication with HCPs 27 Obtain preferences for decision-making 27 Confidence for inclusion 27 Confident to ask for support and time from HCPs 30 Honest communication with HCPs 27 Holistic needs assessment supports, vocabulary and therein dialogue with HCPs 34 Question prompt lists aid and/or prompts dialogue 30 Being involved in care decisions/experience 28 Feeling secure and understood 32 Being heard 28 Express opinions 28 Confidence to ask HCPs about prognosis/future care 30 Confidence to seeking assistance from HCPs 31 Support/encouragement to seek help 31 Discussions, rather than ‘consultations’ 30 Being confident to express limitations/disability 35 |
Hope as a motivator, to ‘go on’/stay alive
33
Accept uncertainty 25 Coping 36 Changing priorities 33 Resilience to/coping with threats to hope 33 Adaptation to continued losses/forfeitures physical and social 33 Adapting to physical/self-image changes 33 Power to manage losses – regaining internal control 33 Taking an active role in health-related issues – planning for future deteriorations in health 36 Coping with the impacts of shrinking body/bodily functions on identity 33 Hope 35 Power 35 Active (rather than passive) role in health care/management 34 |
ADLs: activities of daily living; HCPs: healthcare professionals.
Acknowledgements
D.W. is the lead of the design and development of the study to include the acquisition, analysis and interpretation of data. Lead author involved in drafting and revising the article and approved the version to be published. F.E.M.M. contributed to the study design, analysis and interpretation of data and critical revision of the article and approved the version to be published. J.B. contributed to analysis and interpretation of data and critical revision of the article and approved the version to be published. L.S., A.M.F. and I.J.H. critically revised the article and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This paper presents independent research part-funded through a National Institute for Health Research (NIHR) Integrated Academic Training Fellowship (DW is an NIHR-funded Academic Clincial Fellow). The views and opinions expressed are those of the authors and do not necessarily reflect those of the National Health Service, the National Institute of Health Research, Medical Research Council, Central Commissioning Facility, NIHR Evaluation, Trials and Studies Coordinating Centre, the National Institute of Health Research Programme Grants for Applied Research, or the Department of Health.
Research ethics and patient consent
This study uses routinely collected, aggregated and anonymised data that are publicly available, and therefore, no ethical approvals were necessary.