
Abstract
Background:
Morphine can cause central nervous system side effects which impair driving skills. The legal blood morphine concentration limit for driving is 20 µg/L in France/Poland/Netherlands and 80 µg/L in England/Wales. There is no guidance as to the morphine dose leading to this concentration.
Aim:
The in silico (computed) relationship of oral morphine dose and plasma concentration was modelled to provide dose estimates for a morphine plasma concentration above 20 and 80 µg/L in different patient groups.
Design:
A dose–concentration model for different genders, ages and oral morphine formulations, validated against clinical pharmacokinetic data, was generated using Simcyp®, a population-based pharmacokinetic simulator.
Setting/participants:
Healthy Northern European population parameters were used with age, gender and renal function being varied in the different simulation groups. In total, 36,000 simulated human subjects (100 per modelled group of different ages and gender) received repeated simulated morphine dosing with modified-release or immediate-release formulations.
Results:
Older age, women, modified-release formulation and worse renal function were associated with higher plasma concentrations. Across all groups, morphine doses below 20 mg/day were unlikely to result in a morphine plasma concentration above 20 µg/L; this was 80 mg/day with the 80 µg/L limit.
Conclusion:
This novel study provides predictions of the in silico (computed) dose–concentration relationship for international application. Individualised morphine prescribing decisions by clinicians must be informed by clinical judgement considering the individual patient’s level of impairment and insight irrespective of the blood morphine concentration as people who have impaired driving will be breaking the law. Taking into account expected morphine concentrations enables improved individualised decision making.
Morphine can cause central nervous system side effects which impair driving.
The blood morphine concentration driving legal limit is 20 µg/L in France/Poland/Netherlands and 80 µg/L in England/Wales.
There is no dose–concentration guidance as to what morphine dose would lead to these concentrations.
For the same oral morphine dose, older age, women, modified-release formulation and worse renal function are associated with higher morphine plasma concentrations.
With normal renal function,<20 mg/day morphine is unlikely to result in a morphine plasma concentration above 20 µg/L; this is <80 mg/day morphine for the 20 µg/L limit.
The morphine dose–concentration relationship helps inform individualised prescribing decisions by clinicians for people needing morphine.
Clinical judgement considering the individual patient’s level of impairment and insight for any plasma concentration is needed.
Introduction
Morphine is commonly prescribed for pain management and can cause central nervous system harms such as cognitive and psychomotor impairment which can have a negative impact on driving skills.1,2 An offence of driving with certain controlled drugs above specified blood limits came into force in England and Wales in March 2015.3,4 This includes a 80-µg/L morphine limit at the time of testing.3,4 It gives police powers to arrest and test people suspected of driving with higher than specified blood levels of certain controlled drugs. The 80 µg/L limit was established after taking into account epidemiological and experimental data of blood morphine concentrations of individuals and impaired driving. 5 However, the legal blood concentration of morphine varies across European countries from 9 µg/L (Norway), to 20 µg/L (France, Poland, Netherlands) to 80 µg/L (England/Wales).5,6 In the United States, driving on therapeutic opioids varies between states. 7 Arizona, Indiana, Iowa, Minnesota and North Carolina have statuary defences for drivers taking prescription opioids. In Maine, South Dakota and Wyoming, driving while taking prescription drugs known to impair driving is prohibited, even if driving is not affected. 7 In Australia, people taking opioids are not allowed to drive if their driving is impaired, irrespective of blood levels. For unimpaired drivers, in Australia and New Zealand, no blood concentration cut-off applies.8,9 This heterogeneity in laws within and between countries illustrates that a concentration–impairment relationship is not established. National and international medical recommendations also reflect this uncertainty. In a UK National Health Service document, oral morphine equivalent doses above 220 mg/day were considered probably not safe to drive. 10 The Royal College of Anaesthetists states that doses around 200 mg/day could be as dangerous as having borderline illegal driving blood alcohol levels. 11 The American College of Occupational and Environmental Medicine states that acute and chronic opioid use is not recommended for patients who operate motor vehicles. 12
Anyone driving in England and Wales with blood concentrations above 80 µg/L will be breaking the law, whether their driving was impaired or not. However, people taking morphine for medical reasons may have a statutory ‘medical defence’ if they have blood concentrations greater than the legal limit.3,4 For this defence to be valid, their driving must be unimpaired, the drug must be prescribed, supplied/sold to treat a medical problem and taken in accordance with prescriber instructions (or the medicine information leaflet). Written evidence may be required. Despite the clear guidance on blood concentrations, there is no guidance relating to the dose which would equate to being over the specified limits. 3 A Swedish study of 2029 apprehended drivers showed that those individuals who had morphine detected in their blood had a mean morphine concentration of 46 µg/L (2.5 and 97.5 percentiles: 6 and 210 µg/L). 13 This indicates that a proportion of apprehended drivers had morphine concentrations above 80 µg/L and most above 20 µg/L. Furthermore, drug-impaired driving does not necessarily relate to plasma concentration of morphine. 13
In clinical practice, the dose of morphine which approximates to morphine blood concentrations of 20 and 80 µg/L is not known. This study aimed to model the relationship between oral morphine daily dose and plasma concentration for which the driving laws apply to help inform personalised patient decisions. In silico (computed) pharmacokinetic modelling was used to account for inter-individual variables across different ages and genders, and to detect differences between oral morphine preparations.
Methods
In silico physiology-based pharmacokinetic modelling was used to assess the plasma concentrations which relate to oral doses of immediate and modified-release morphine (MST Continus®) in order to estimate the daily dose of morphine which is likely to produce a plasma concentration of 20 and 80 µg/L. This was modelled in men and women across a range of ages. A number of software and models are available, offering different focal strengths.14–17
Calculations were undertaken using Simcyp® Population-Based Simulator software (version 14; Certara™, New Jersey, USA). This software simulates absorption and metabolism in a physiology-based modelling platform, delivering a range of dose–plasma concentrations across a diverse population. 18 In silico characterises biological experiments carried out entirely on a computer, applying algorithms or computer simulations to model biological processes. These in silico techniques are widely used in such a way to model representative data from a large number of potential subjects.18,19 To adequately predict in vivo behaviours from in vitro data, the models use information on the human body for each ‘test’ subject, the physical chemistry of the drug molecule and the conditions of its use (dose and dosing schedule). Physical chemistry of the drug and dosing schedule were implemented based on information from the Royal Society of Chemistry’s ChemSpider, Drug Bank and dosing through the British National Formulary.20,21 Distribution was calculated using the minimal physiologically based pharmacokinetic (PBPK) model option with volume of distribution included as a user input of 2.9 L/kg with a 27% coefficient of variance. 22 To enable calculation of individual patient variability factors, multivariate models are used to ensure valid predictions of the key processes such as absorption and metabolism.23–25 The covariates for these processes have been previously described.18,26–28 In the gastrointestinal tract, Simcyp’s Advanced Dissolution Adsorption and Metabolism (ADAM) multi-compartmental models are used to represent the physiological state.29,30 These models use multiple mathematical ‘compartments’ (from stomach to anus) which contain a volume and flow rate, representing the physiological state. Within each of these compartments, release of the drug, interaction with the gut wall (degradation and metabolism), absorption (passive and active) and first-pass liver metabolism are considered. The model accounts for changes in liver function associated with ageing, based on the microsomal protein per gram of liver in ageing samples. 31 Average renal function for each age group is calculated using the Cockcroft and Gault equation. 32
The ‘healthy Northern European population’ was used for this study, with all model values retained except for age, gender and renal function. These values were altered to ascertain the dose–pharmacokinetic relationships for different groups.
The pharmacokinetic model for morphine was validated in two stages. First, parameters were developed to match maximum concentration (Cmax), time to achieve maximum concentration (Tmax), area under the curve (AUC) and plasma/time shape parameters, with clearance and volume of distribution used from the mean of reported data.22,33–36 Second, the predicted and measured plasma concentrations across the dose range at steady state were compared.35–37 This represented the best available population data for the dosing of morphine with slight over prediction being built into the model to ensure conservative clinical application (Figure 1).
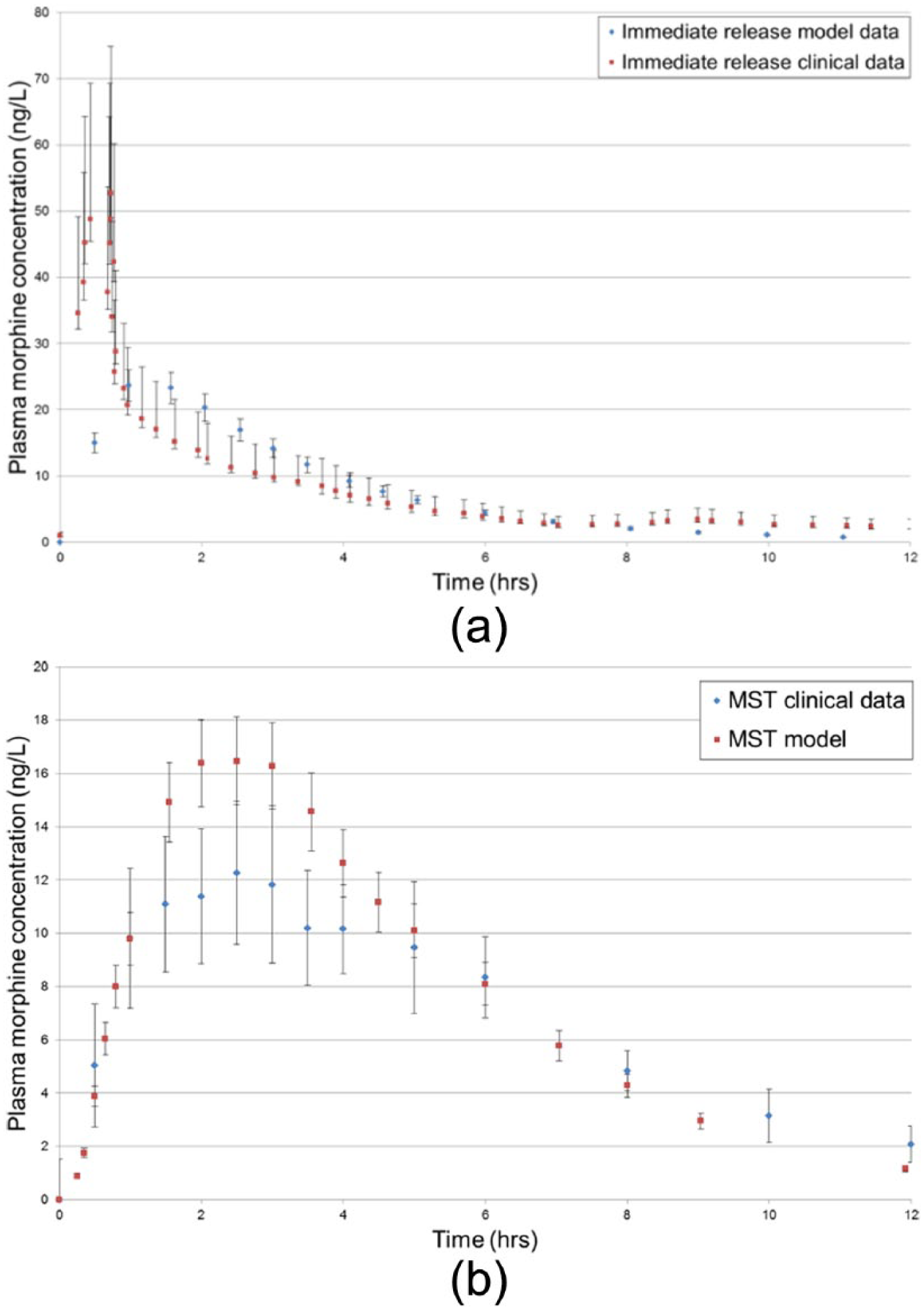
Model validation via comparison of mean data from clinical trials35–37 of (a) 20 mg immediate-release oral formulation and the in silico model in healthy diverse individuals and (b) 30 mg modified-release morphine tablets and the in silico model in healthy diverse individuals. Error bars show 10% standard error in the model and studied variance within clinical subjects in the trial data.
Dosing intervals were selected due to clinical relevance, with a 12-h interval used for modified-release dosing and a 6-h interval for immediate-release dosing. Although immediate-release dosing can occur at 4-hourly intervals, often the dose is taken less than six times a day. Furthermore, the same dose at 4- and 6-hourly dosing intervals resulted in comparable mean maximum plasma concentrations at steady state, with the 6-hourly dose leading to an increased chance of being above 80 µg/L and thus would provide the more conservative guidance (Figure 2).
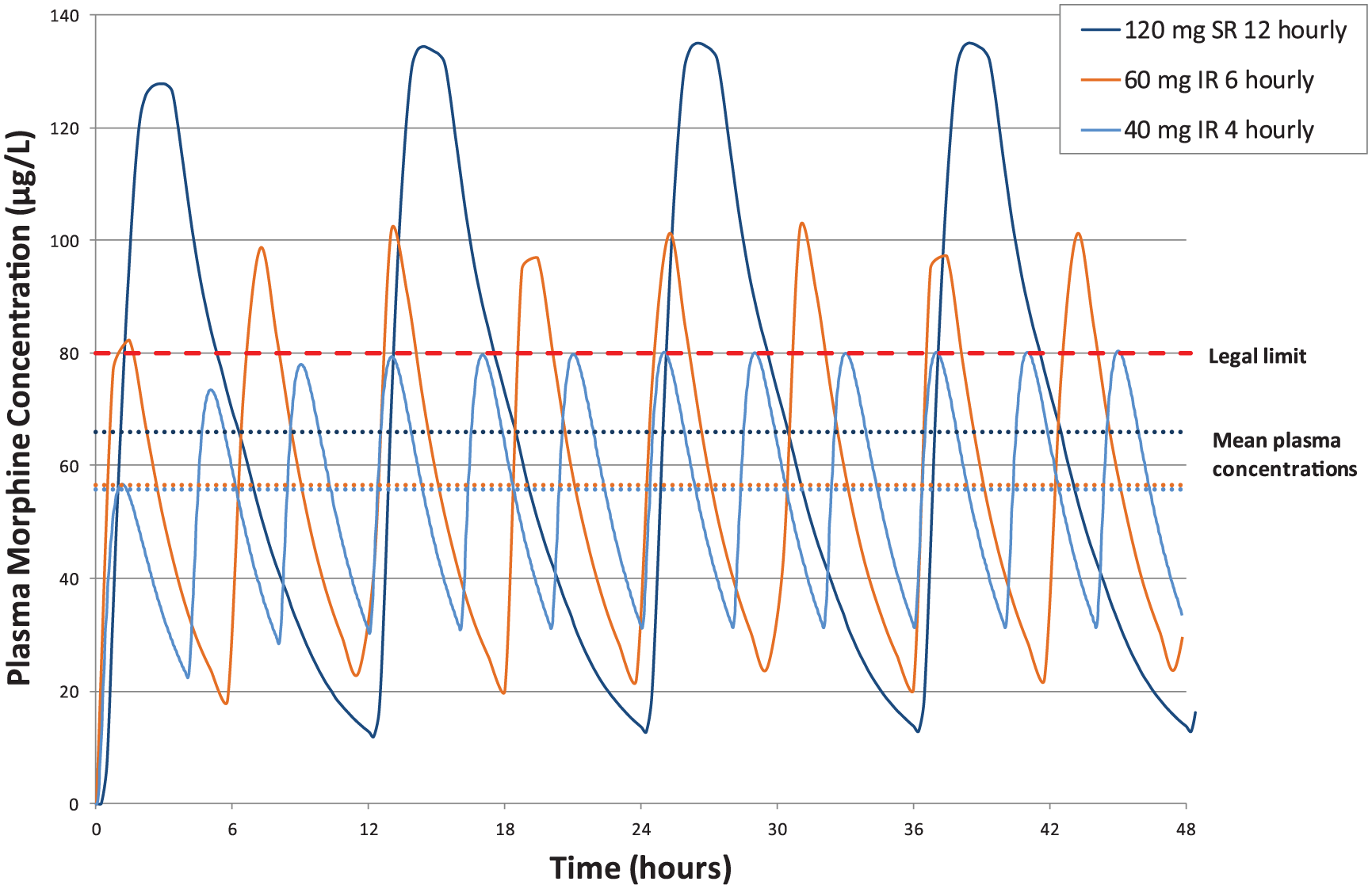
Comparison of 240 mg daily dosing and its effect on time spent over the legal limit for 40 mg 4-hourly, 60 mg 6-hourly, immediate-release and 120 mg 12-hourly modified-release oral morphine in the 70- to 80-year-old female group, also displayed is the 80 µg/L England and Wales legal limit and mean plasma concentration.
Age, gender and renal function parameters were altered in the model to explore the dose–pharmacokinetic relationships for different groups of people. For both men and women, age ranges of 18–90 years were used, divided into 18–40 and then in 10-year intervals. The effect of renal failure on dose–concentration relationship was evaluated by adjusting renal function parameters in line with the National Kidney Foundation classification of glomerular filtration rate (GFR) for mild (70 mL/min/1.73 m2), moderate (50 mL/min/1.73 m2) and severe (20 mL/min/1.73 m2) renal failure. 38
Sampling intervals were 15 min for the immediate-release preparation model and 40 min for the modified-release model, for at least 7 days. Prediction of the amount of time a person is likely to be over the limit is based on the number of sampled points within a simulated 24-h period that were over 80 µg/L (Figure 2). All data points above 80 µg/L (Figure 2) would be considered as time over the legal limit. Such data would not be captured from the mean plasma concentrations (Figure 2), which are below the legal limit and if used alone would wrongly classify the patient as under the legal limit at this dose.
Plasma concentration over time was modelled for morphine doses between 5–200 mg twice-daily in 5 mg increments to 100 mg, 25 mg intervals thereafter; and 10–200 mg four-times daily in 10 mg intervals, for modified and immediate-release oral preparations, respectively. Each dose of each formulation was simulated on 100 individuals for at least 7 days to ensure steady state was reached. Mean data from the 100 individuals were used to determine the dose to plasma concentration relationship. Individual datasets can be found in the online supplement. These data were then analysed to determine the number of hours which those individuals with the highest Cmax response were over the legal limit (20 or 80 µg/L) for a given dose. This was achieved by use of the 95th percentile data from each sub-population, with these data reported in Figures 3, 4 and Supplementary Figures 1 and 2 – as the aim of this work was to determine doses conveying the highest risk of a patient being above the legal limit.
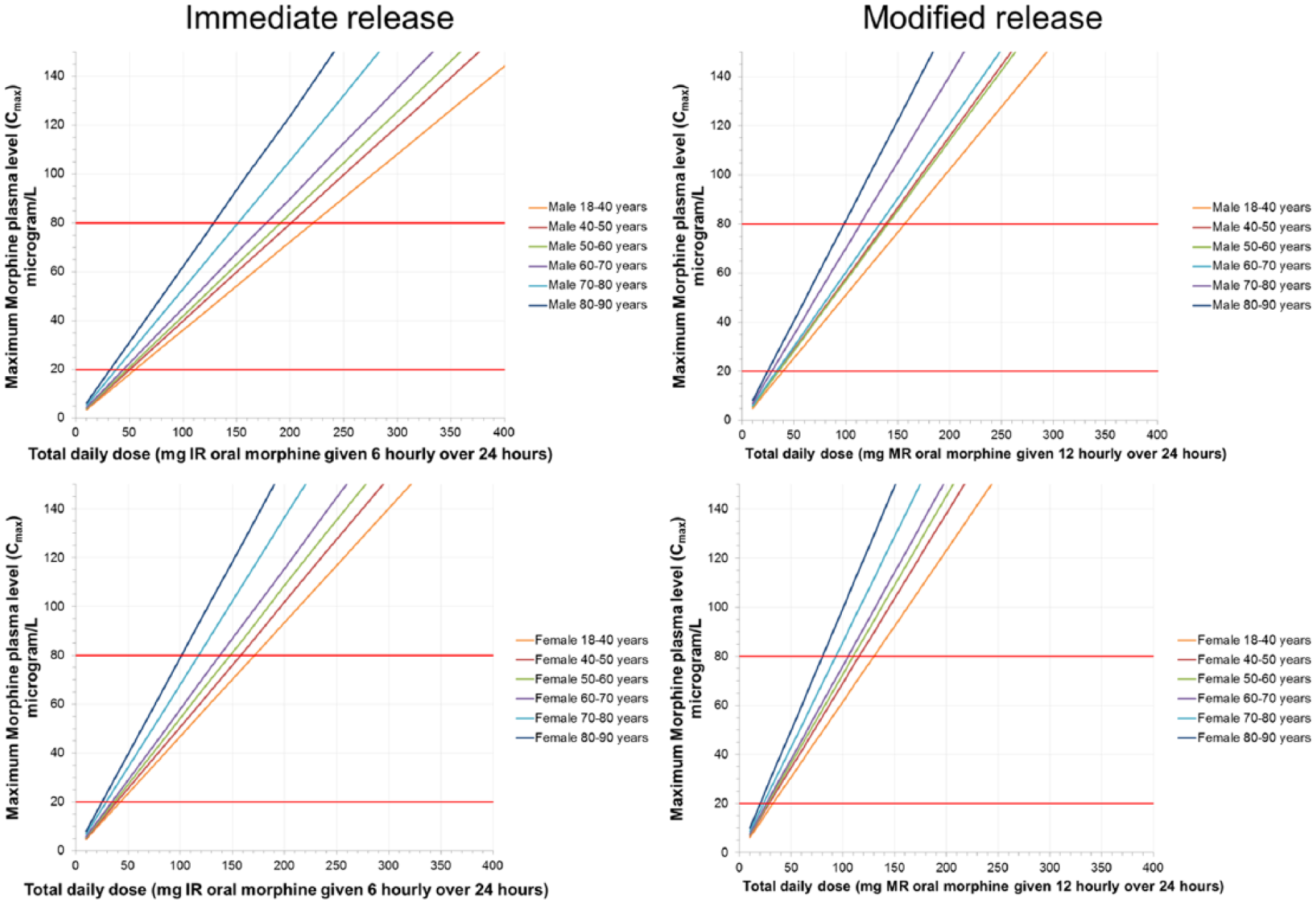
The maximum morphine concentration (Cmax) is related to the daily morphine dose, in men (top) and women (bottom) divided into ages, taking different doses of immediate-release (left) and modified-release (right) morphine. The red lines represent the legal plasma levels in France, Poland, Netherlands (20 µg/L) and England/Wales (80 µg/L). Due to population variance, accuracy is only within the 10–20 mg dosage range presented on the scale bars; the 95th percentile data are presented here as a worst case scenario.
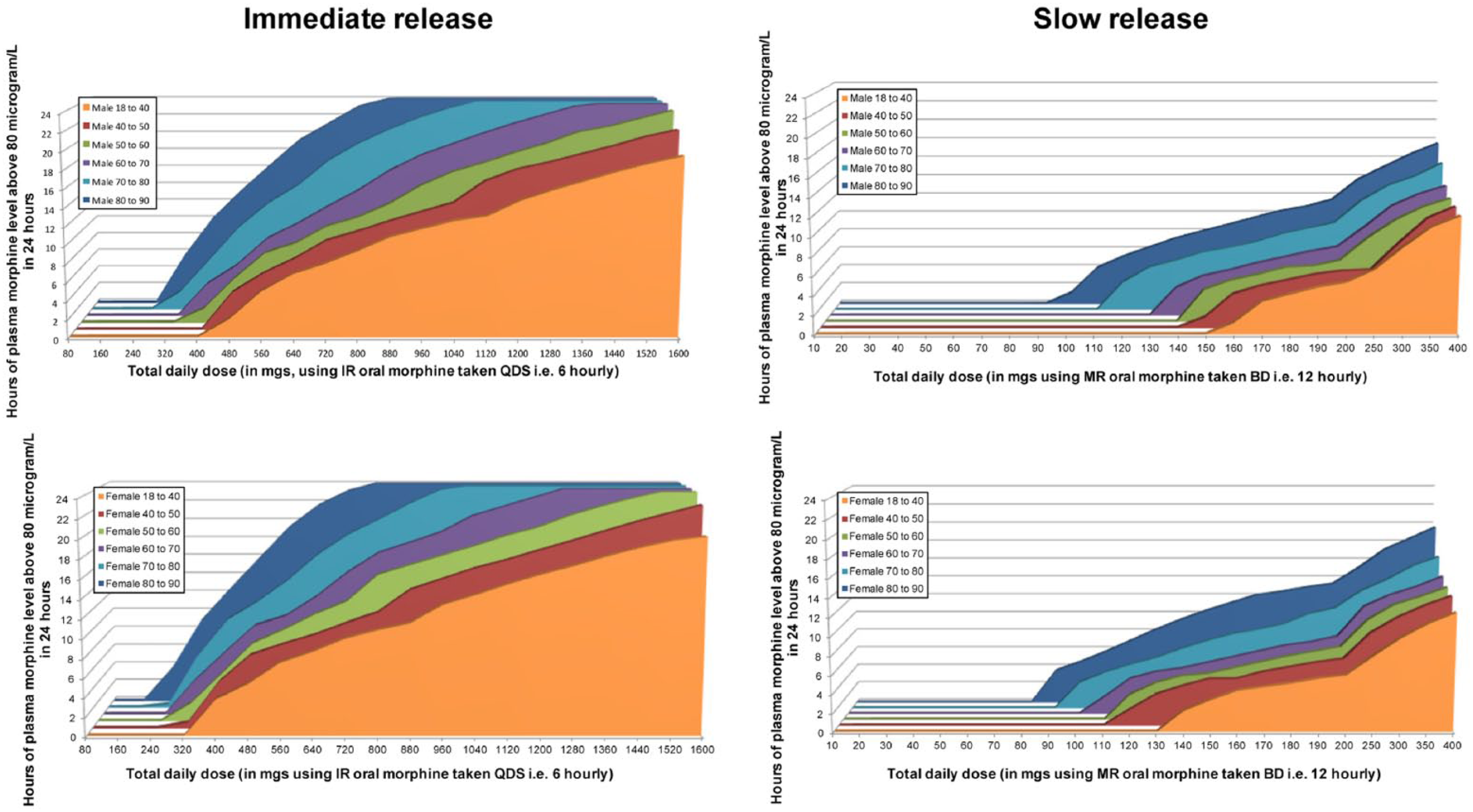
The number of hours per day plasma levels will be above 80 µg/L in men (top) and women (bottom) divided into ages, taking different doses of immediate-release (left) and modified-release (right) morphine. The 95th percentile data are presented here as a worst case scenario. The increments of immediate-release and modified-release dosing are not the same and are non-linear.
The law states the legal morphine concentration in blood. Morphine levels between whole blood and plasma have previously been reported to correlate in a linear fashion with a relationship close to 1.02. 39
Results
In silico modelling for 100 ‘men’ and 100 ‘women’ for each age range and dose gives a mean of the oral morphine dose concentration relationship. The dose precision within the data is limited to the order of 10–20 mg dosing intervals, as per the axis of the charts. From this, it is possible to determine, in each population, the dose which equates to a morphine plasma concentration (Figure 3 and Supplementary Figure 1).
The dose which equates to the legal morphine plasma concentration in France, Poland, Netherlands (20 µg/L) and England/Wales (80 µg/L) can be determined (Figure 3 and Supplementary Figure 1). The morphine plasma concentration has also been represented by the time a person is likely to be over 80 µg/L (Figure 4 and Supplementary Figure 2). This is shown at steady state for people of different ages, genders, morphine formulations (assuming normal renal and hepatic function for that age/gender) and renal failure (Figure 4 and Supplementary Figure 2).
Mild renal failure did not significantly affect morphine concentrations, with reduced hepatocyte concentrations showing a greater impact – included within modelling of the older age groups. As morphine is renally excreted, increasing severity of renal failure increased the duration of the morphine plasma concentration being above 20 or 80 µg/L; this was especially so for immediate-release morphine (Supplementary Figures 1 and 2).
Older age, women and poor renal function were associated with higher plasma concentrations (Figures 3 and 4; Table 1).
Estimated daily morphine doses below the legal driving limits.
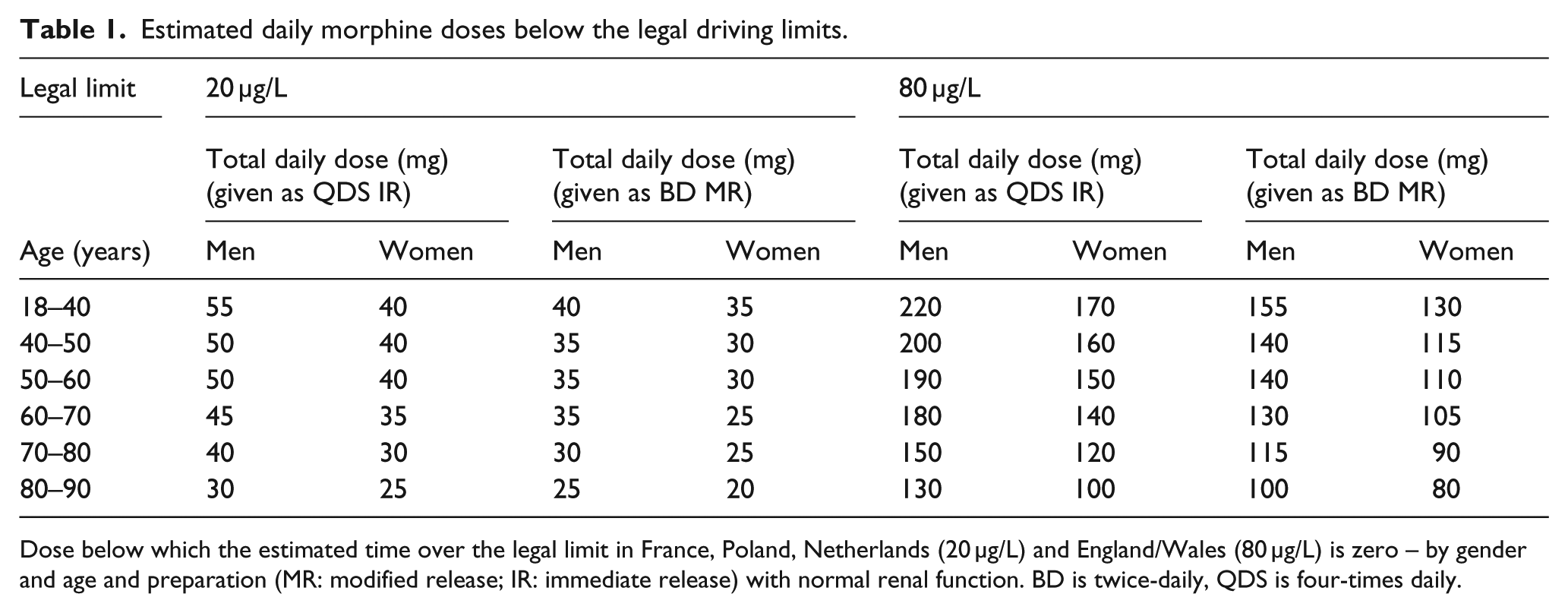
Dose below which the estimated time over the legal limit in France, Poland, Netherlands (20 µg/L) and England/Wales (80 µg/L) is zero – by gender and age and preparation (MR: modified release; IR: immediate release) with normal renal function. BD is twice-daily, QDS is four-times daily.
Discussion
Using in silico modelling, this study estimates a dose–plasma concentration relationship in the context of the legal morphine limit, taking into account gender, age, renal function and morphine preparation. Table 1 presents a clinical guide to estimate the dose–plasma concentration likelihood in terms of exceeding the England/Wales legal blood morphine driving limit of 80 and 20 µg/L in France, Poland and Netherlands. Older age (especially above 70 years of age), women, modified-release morphine formulation and worsening renal function were associated with higher plasma concentrations. These modelling data give an approximation of the morphine dose, across a range of situations, which would likely lead to a morphine plasma concentration of ⩾20 or 80 µg/L. The model does not consider specific diseases, how other factors and other drugs affect metabolism and cognition and how cognition itself relates to safe driving. This must be determined by the clinician and patient, including assessment of the patient’s own perspective of their cognitive performance and ability to drive at that instance. 40
In patients with cancer pain, daily morphine doses in studies were mostly between 100 and 250 mg but ranged from 25 to 2000 mg. 41 This indicates that many patients will be on morphine doses that, according to our model, could lead to a morphine plasma concentration above 20 and even 80 µg/L. This is also the case for patients on opioids for non-cancer pain, where 19% (n = 455) were on over 200 mg morphine equivalent/day, 42 and opioid-dependent patients being treated with morphine (n = 211), mean daily dose 791 ± 233 mg/day. 43
The model shows that compared with 12-hourly modified-release morphine, higher daily doses of 6-hourly immediate-release morphine are needed to achieve a morphine plasma concentration above 20 or 80 µg/L. This is because time over 20 and 80 µg/L is the main outcome, rather than the mean plasma concentration (which would not detect people at risk of being above 20 or 80 µg/L; Figure 2). Due to absorption differences, immediate-release morphine formulations produce a higher Cmax, for a shorter period compared to equivalent doses of modified release. Although equivalent doses of modified-release morphine were associated with higher plasma concentrations, the concentration oscillations associated with repeated immediate-release administration might have a detrimental effect on skills required for driving.44–46 The modified-release model was for MST Continus.
In the model, older people, particularly above 70 years old, have a higher morphine plasma concentration for a given morphine dose. This is because as age increases, renal and hepatic function deteriorates (although this may remain within the normal range for the age group) and muscle mass reduces. In the renal failure model, estimated GFR is decreased, increasing the plasma concentration of morphine. Although mild renal failure did not affect morphine concentrations, which is expected when considering morphine concentrations alone (i.e. not the metabolites due to its high water solubility. 47 Due to the higher Cmax in modified-release preparations, the time above 80 µg/L is differently affected in modified-release versus immediate-release preparations, although the proportional change is comparable for both preparation types. Women have a higher plasma concentration from a given dose compared to men due to proportionally smaller bodies and associated organs used for metabolism and clearance of morphine (liver and kidneys). 48
As pain might have a detrimental effect on driving,49,50 it is important this is well managed and appropriate analgesics are not stopped.
Strengths and limitations
This study used in silico techniques to correlate morphine dose to plasma concentration. Age, gender, renal function and morphine formulation have been modelled for. The strength of PBPK modelling is that 36,000 simulated subjects at different ages and gender were simulated to receive repeated morphine dosing with both modified-release and immediate-release morphine formulations. The model has been shown to correlate with dose–concentration responses to in vivo study data.34,35,51–54 However, our model predicts higher plasma concentrations for a given morphine dose compared to in vivo data due to cautious model preparation to ensure that doses were not under predicting; this can be seen in the comparative data (Figure 1).35–37
Our model used one immediate-release and one modified-release formulation, based on collated published pharmacokinetic data.22,33–36 Clinically differing formulations and circumstances will lead to differing absorption kinetics between formulations, potentially leading to differing dose–concentration relationships in individuals. These findings offer an insight into the changing pharmacokinetic relationship with age and the effect an average dose will have and will help guide the clinician. People taking as required immediate-release morphine might do so at different dosing intervals. Some individuals might take 4 hourly doses instead. In practice, most patients do not take a dose overnight (e.g. 2:00 a.m.), and thus, the average dose interval is nearer 6 h than 4 h. We modelled morphine 6 hourly to clinical applicability within the confines of the software (as a dose gap cannot be added, for sleep/dose omission, etc.). Furthermore, during repeated administration, the individual morphine dose leading to a plasma concentration over 20 or 80 µg/L was effectively the same for 4 and 6 hourly dosing.
This study cannot account for all the variabilities between individuals. With 100 ‘people’ per modelled pharmacokinetic trial group, the results should be representative for northern European populations. A degree of variability around the ‘normal’ state has been included within the model, but this does not account for extreme variability. Extremes of body mass index (BMI), eating, drinking, drug interactions, and effects from the underlying disease/other co-morbidities have not been included in this model. These individual variables could potentially alter the pharmacokinetics and metabolism of morphine.3,55 The models suggest that cytochrome P450 enzyme inhibitors (inhibitors of hepatic clearance) would have a profound effect. As the active metabolites of morphine (e.g. morphine-6-glucuronide) are not included in the new law, they have not been modelled for, although morphine-6-glucuronide can have an impact on driving performance. 56 Multiple drugs have not been accounted for in the current study, although morphine is often used with other medications.6,57–59 The clinician must take all these factors into account. 5
Future research
Data using driving simulators and on-the-road assessments of the effects of stable morphine at different dose ranges, as well as opioid initiation and titration are needed. Although the law does not include morphine metabolites, they might influence cognition and driving. Future work should ascertain the concentrations of morphine metabolites and their relationship with cognitive, psychomotor function and driving impairment in different patient groups. The effects of immediate-release morphine taken ‘as-required’ in addition to regular modified-release morphine on morphine plasma concentrations are needed.
Clinical implications
This in silico modelling study evaluated the relationship between morphine dose and plasma concentration. This will help guide clinicians to know whether a patient is likely to have a plasma concentration above 20 or 80 µg/L (the legal driving limit), but this does not inform the risk of impaired driving for any individual for any plasma concentration. As there will be inter-individual variability, it is important that these data are used to guide personalised patient decisions, not make them.
Older age, women, modified-release formulation and worse renal function were associated with higher plasma concentrations. In general, across all studied groups, morphine doses below 120 mg/day were unlikely to result in a morphine plasma concentration above 80 µg/L. This was much lower at 30 mg/day for the 20 µg/L limit in France, Poland and Netherlands. An immediate-release morphine dose taken alongside modified-release morphine would lead to a higher plasma concentration.
The prescribing clinician must retain clinical judgement for each patient and advise to restrict driving until they know the effect of morphine on their driving ability. Both the legal limit and the actual effect on driving as well as patients’ own perspective of their cognitive performance need to be taken into consideration as people with impaired driving will be breaking the law irrespective of blood concentration.
Conclusion
In silico modelling of the dose–concentration relationship helps inform which patients are likely to have higher plasma concentrations after taking oral morphine. This information can help clinicians to make individualised prescribing decisions and provide advice on driving. Clinical judgement taking into account the individual patient’s level of impairment and insight is needed alongside understanding the dose–concentration relationship, as people who have impaired driving will be breaking the law irrespective of their morphine plasma concentration.
Supplemental Material
Supplementary_Figure_1 – Supplemental material for In silico (computed) modelling of doses and dosing regimens associated with morphine levels above international legal driving limits
Supplemental material, Supplementary_Figure_1 for In silico (computed) modelling of doses and dosing regimens associated with morphine levels above international legal driving limits by Jason W Boland, Miriam Johnson, Diana Ferreira and David J Berry in Palliative Medicine
Supplemental Material
Supplementary_Figure_2 – Supplemental material for In silico (computed) modelling of doses and dosing regimens associated with morphine levels above international legal driving limits
Supplemental material, Supplementary_Figure_2 for In silico (computed) modelling of doses and dosing regimens associated with morphine levels above international legal driving limits by Jason W Boland, Miriam Johnson, Diana Ferreira and David J Berry in Palliative Medicine
Footnotes
Acknowledgements
J.W.B. and D.J.B. developed the concept and design of this work. D.J.B. performed the in silico analysis, and all authors helped with the interpretation of the data. J.W.B. and D.J.B. wrote the first draft. All authors contributed to subsequent drafts and approved the final version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. J.W.B. and D.J.B. contributed equally to this article. J.W.B. is the guarantor.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: D.F. is funded by Fundação para a Ciência e Tecnologia (FCT) from the Portuguese Government (PhD grant SFRH/BD/109920/2015).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.