
Abstract
Background:
Volunteers fulfil several roles in supporting terminally ill people and their relatives and can positively influence quality of care. Healthcare in many countries faces resource constraints and some governments now expect communities to provide an increasing proportion of palliative care. However, systematic insights into volunteer presence, tasks and training and organisational challenges for volunteerism are lacking.
Aim:
Describe organised volunteerism in palliative direct patient care across the Flemish healthcare system (Belgium).
Design:
A cross-sectional postal survey using a self-developed questionnaire was conducted with 342 healthcare organisations.
Setting/participants:
The study included full population samples of palliative care units, palliative day-care centres, palliative home care teams, medical oncology departments, sitting services, community home care services and a random sample of nursing homes.
Results:
Responses were obtained for 254 (79%) organisations; 80% have volunteers providing direct patient care. Psychosocial, signalling and existential care tasks were the most prevalent volunteer tasks. The most cited organisational barriers were finding suitable (84%) and new (80%) volunteers; 33% of organisations offered obligatory training (75% dedicated palliative care, 12% nursing homes). Differences in volunteer use were associated with training needs and prevalence of organisational barriers.
Conclusion:
Results suggest potential for larger volunteer contingents. The necessity of volunteer support and training and organisational coordination of recruitment efforts is emphasised. Organisations are encouraged to invest in adequate volunteer support and training. The potential of shared frameworks for recruitment and training of volunteers is discussed. Future research should study volunteerism at the volunteer level to contrast with organisational data.
Keywords
Palliative care volunteers may reduce stress, offer practical and emotional support and provide a link to the community for people who are dying and those close to them.
Citing increasing resource constraints in professional healthcare, some governments, including that of Belgium, are proposing that a larger proportion of care at the end of life should be provided by informal caregivers.
While the literature has widely reported on volunteer tasks, no specific data regarding volunteer numbers, training and recruitment in palliative care are available on which to base this intended policy shift.
Psychosocial and existential care and fulfilling signalling functions are the most prevalent tasks undertaken by volunteers, but come with increased volunteer training provision.
Organisations employing volunteers in practical care for people who can no longer function independently more often cite legal and financial barriers.
The recruitment of suitable and new volunteers is the most cited organisational barrier to maintaining and increasing the numbers of volunteers.
Non-specialist palliative care organisations (not including community care) are advised to invest more strongly in volunteer support and training.
Governments turning to volunteering to combat pressures on professional healthcare are advised to provide shared frameworks expedite recruitment coordination and standard, context-sensitive volunteer training.
Tailored recruitment strategies that offer flexible, low-threshold volunteering roles should be devised to engage both younger and older volunteers.
Introduction
Volunteers played a major role in the early days of the palliative care movement. They continue to be involved in the provision of palliative care, both in the community and in institutional settings.1–3 Although family and professional caregivers provide the majority of end-of-life care, volunteers take up several roles,4,5 for example, assisting with recreational and social programmes, visiting patients, taking them out and providing companionship and support.6–9 These tasks are considered as core to providing quality palliative care. Previous studies show that volunteers can positively influence the quality of care for both the person who is dying and those close to them by reducing stress, offering practical and emotional support and providing a link to the community.2,10–12
There is a widespread move to reduce the amount of care provided by professionals, given the limitation in resources allocated to healthcare and the growing needs of ageing populations, and volunteers are expected to play an even more substantial role in future palliative care in several countries.13–16 Some governments are now pushing for a partial shift from formal healthcare services towards community care (e.g. through volunteerism).13,14
The feasibility of such a shift requires an understanding of current volunteer practices; however, data on the total volunteer workforce deployed in palliative care, whether they provide direct patient care and what tasks they perform, are scarce. The extent of relevant training and the barriers to maintaining a volunteer workforce are also unknown. In several countries, including Belgium, palliative care provision is divided into dedicated and generalist (i.e. palliative care provided by care providers other than those of dedicated palliative care services); 17 previous quantitative studies have focused mainly on dedicated palliative care services rather than looking at a broader approach to improving well-being near the end of life.5,18–21
To address these knowledge gaps, this study provides an extensive description of the current state of organised volunteerism in palliative direct patient care across the entire healthcare system in Flanders, Belgium. It thereby adds to the literature, following the lead of the European Association for Palliative Care (EAPC) Taskforce on Volunteering. 22 The research questions are as follows:
To what extent do various healthcare organisations that provide palliative care embed volunteers in patient care?
What types of palliative care activities do these organisations have their volunteers perform in patient care?
What organisational barriers to maintaining and expanding a volunteer force do these organisations encounter?
Which recruitment strategies do these organisations employ?
To what extent do these organisations offer training to their volunteers and which subjects are offered?
Method
We conducted a cross-sectional postal survey between June and October 2016 among healthcare organisations providing care for people with terminal illnesses – who are not necessarily in the terminal stage – in the Flemish healthcare system. The Belgian regions (Flanders, Wallonia and Brussels) have autonomy over various aspects of healthcare in the different language communities (Flemish, French and German speaking), including home care, hospital care and long-term care. The Flanders government is responsible for these aspects in Flanders and for the Flemish-speaking community in Brussels. We therefore included Flanders and Flemish-speaking Brussels for this study, and excluded Wallonia.
Definition of volunteerism
We define volunteerism in palliative care as the time freely given by individuals, with no expectation of financial gain, within
some form of organised structure other than the already existing social relations or
familial ties, with a palliative approach, i.e. the intention of improving the quality
of life of adults and children with terminal illnesses and those close to them (family
and others). (Adapted from Goossensen et al.
22
)
Volunteers do not have an employment contract or statutory appointment within the organisation in which they perform these tasks. This definition is in accordance with that provided by the Belgian federal law.23,24 We focus on community volunteers in direct patient care, that is, members of the local community that work in care-focused roles and are regularly involved with patients and those close to them, provided they are not merely performing their medical profession unpaid. 22 Finally, we focus on volunteers who fit this definition and provide care for people with terminal illnesses and their families. This definition was incorporated into our questionnaire.
Sample
Our unit of analysis is the individual organisation. We identified organisations and services through the up-to-date listings of healthcare organisations recognised by the Flemish ministry for Welfare, Public Health and Family. We considered hospital departments as organisations, as volunteerism is more directly coordinated at this level. Our inclusion criteria were that organisations:
Provide care for people with terminal illnesses;
Potentially work with volunteers;
Are active in Flanders or Brussels;
Are on the list of healthcare organisations of the Flemish ministry for Welfare, Public Health and Family.
We consulted 12 experts from different types of healthcare organisation where people may come to die and where people with terminal illnesses may be treated to find out where volunteers may regularly be active in patient care (see Appendix 1). Box 1 provides a list and descriptions of all organisation types included in our sample framework based on this expert consultation.
Sample framework of Flemish and Brussels healthcare services potentially involving volunteers in direct patient care, Belgium, 2016. a
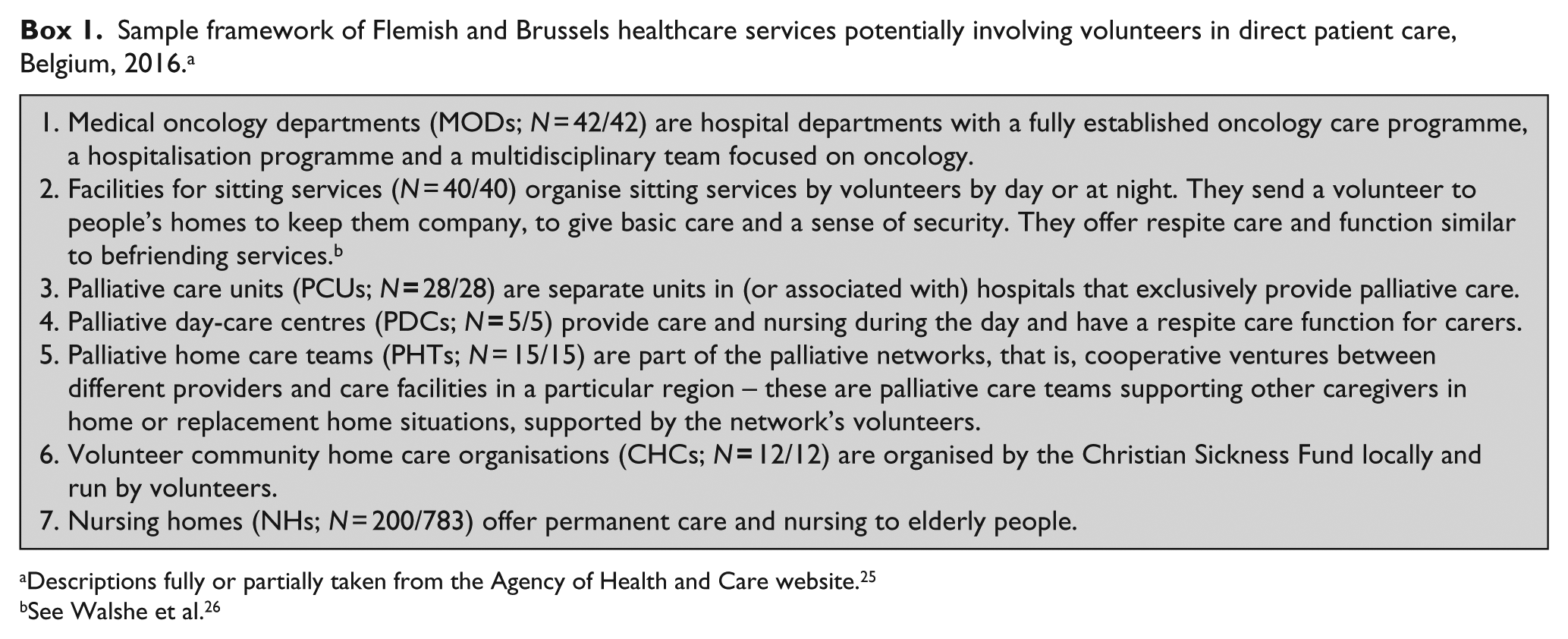
Descriptions fully or partially taken from the Agency of Health and Care website. 25
See Walshe et al. 26
Ethical approval
The proposal for this study was submitted for approval to the commission of medical ethics of the university hospital of Brussels (ref. B.U.N. 143201627927). Approval was granted on 23 March 2016.
Samples and procedure
We surveyed a full population sample of all organisation types except for NHs where a random sample of 200 from a total of 783 was taken (25.5%). Our total N for this survey was 342.
All questionnaires were sent out simultaneously by post, pre-numbered to track response. A thank-you note and reminder were sent out 1 week later; 3 weeks post mail-out a replacement questionnaire and new cover letter were sent to all non-respondents. Five weeks post mail-out the remaining non-respondents were contacted by telephone. New questionnaires were supplied by email when necessary. Seven weeks post mail-out a non-response survey consisting of four questions was sent by post to gauge whether respondents had received the questionnaire, had sent it back and if not why. Questionnaires were addressed to representatives of the organisation. Informed consent was assumed upon participation. Data input did not include the questionnaire numbering, thereby ensuring anonymity of the data set.
Questionnaire
The self-developed questionnaire consisted of 26 questions covering (a) volunteer presence, (b) volunteer tasks, (c) organisational barriers to volunteerism, (d) volunteer recruitment, selection and evaluation, (e) volunteer training, (f) volunteer involvement, (g) the respondent’s evaluation of volunteer involvement, (h) the organisation’s volunteerism policy, (i) the organisation’s care capacity and (j) the respondent’s demographic information. The questionnaire was developed based on the literature on volunteerism in palliative care and input from representatives of each organisation type in our sample framework. The questionnaire was tested cognitively in two rounds, each with different representatives. Representatives were asked to complete the questionnaire in the presence of the executive researcher in order to identify conceptual clarity or difficulties of the questions. These questions were then reworked between rounds. The questionnaire used items from two validated measures, activities of daily living (ADL), 27 commonly used to measure people’s ability to function independently, and instrumental ADL (iADL), 28 commonly used to measure people’s ability to live at home independently. All other measures were self-constructed. For details including the specific items used for ADL, iADL and psychosocial, signalling and existential (PSE) care tasks, see the questionnaire in Appendix 2 in Supplementary Material.
Statistical analysis
We performed univariate and bivariate analysis using IBM SPSS 24. Cross-tabs were run to calculate proportions for each variable for each organisation type. Percentages were rounded. Chi-square tests were performed to check for statistical differences in proportions across types (significance at p = 0.05 or lower was indicated with a (*)). Agreement was calculated for the item batteries regarding ADL-tasks (six items), iADL-tasks (eight items) and PSE tasks (five items) using Cronbach’s alpha to evaluate how closely related these sets of items were as a group. Analysis of variances (ANOVAs) were conducted to test for associations between mean scores of different variables. All categorical variables for volunteer tasks, training and training subjects, recruitment strategies and organisational barriers were recoded into dummy variables for all analyses.
Results
Out of 342 organisations, a response was received from 258. Out of 84 non-response surveys sent, 27 were returned (25%). Seven organisations (28%) indicated that they had not received a questionnaire. Of those that had received one, 7 (27%) had replied but the reply had not reached us; 37% of those that received a questionnaire but did not return it cited lack of time. Six returned non-response surveys were considered as partial responses, because they either indicated having no volunteers or provided limited data. These were added to the total response, bringing the N up to 264. Non-eligible respondents (e.g. the organisation no longer exists) were subtracted from the sample denominator, bringing it down to 334. In accordance with American Association for Public Opinion Research (AAPOR) guidelines, 29 we reached a valid response rate of 79% (264/334; Table 1).
Survey response.
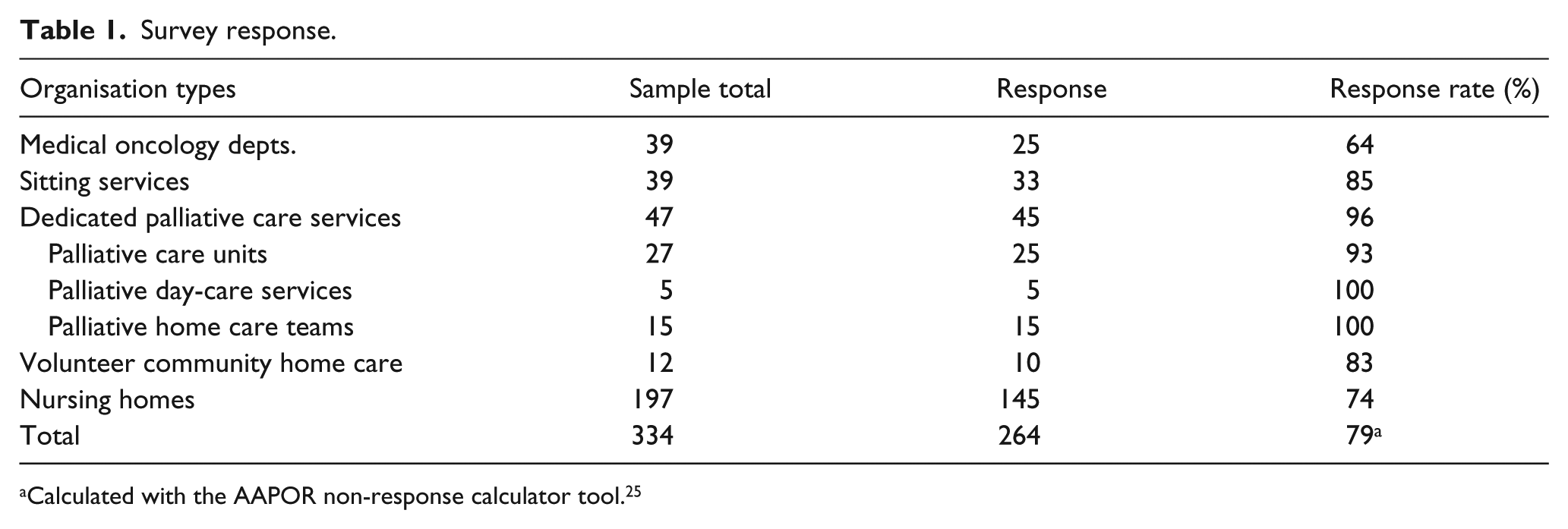
Calculated with the AAPOR non-response calculator tool. 25
Volunteer presence
A total of 94% of organisations had volunteers and 80% had volunteers in direct patient care (Table 2). Dedicated palliative care services were most likely to have direct patient care volunteers (98%) and MODs least likely (64%). In most cases, volunteers were registered with the organisation surveyed (90%). Those with direct patient volunteers had 57 volunteers (standard deviation (SD) = 7) per 100 patients on average, PCUs had the highest average (256 per 100 patients (SD = 28)) and NHs had the lowest (33 per 100 patients (SD = 3; data not shown in tables).
Healthcare organisations with palliative care volunteers, Flanders, 2016 a .
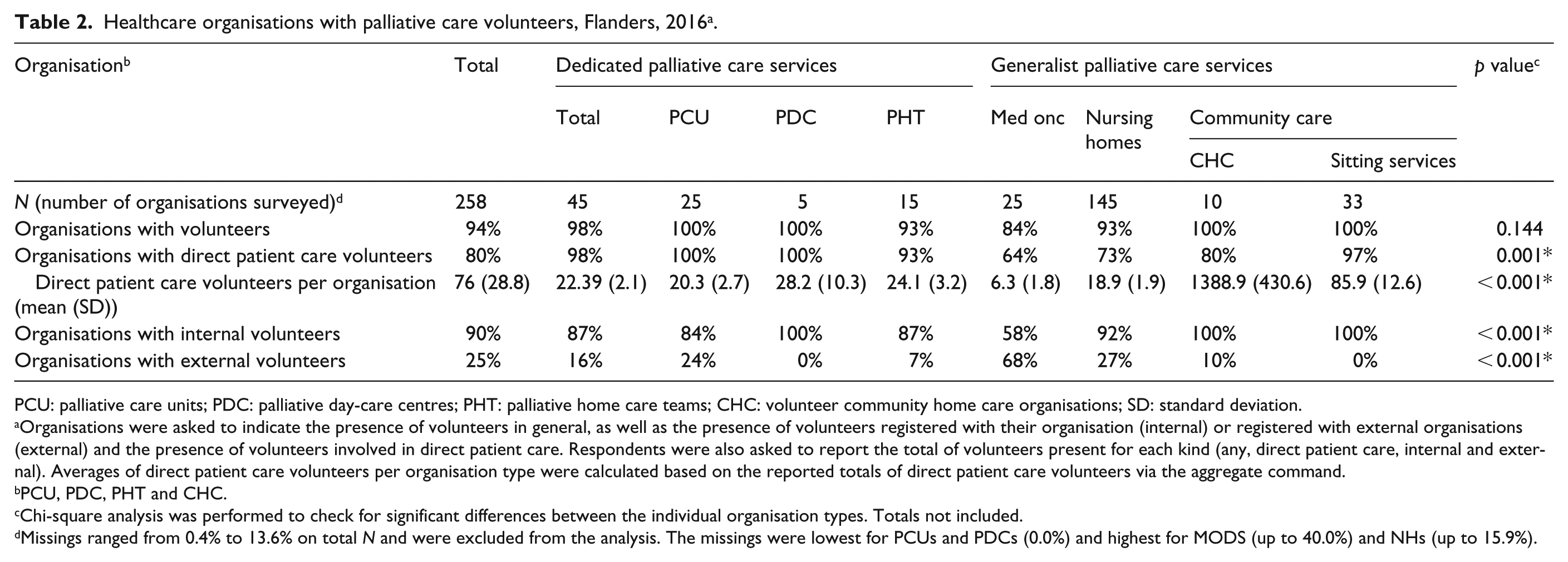
PCU: palliative care units; PDC: palliative day-care centres; PHT: palliative home care teams; CHC: volunteer community home care organisations; SD: standard deviation.
Organisations were asked to indicate the presence of volunteers in general, as well as the presence of volunteers registered with their organisation (internal) or registered with external organisations (external) and the presence of volunteers involved in direct patient care. Respondents were also asked to report the total of volunteers present for each kind (any, direct patient care, internal and external). Averages of direct patient care volunteers per organisation type were calculated based on the reported totals of direct patient care volunteers via the aggregate command.
PCU, PDC, PHT and CHC.
Chi-square analysis was performed to check for significant differences between the individual organisation types. Totals not included.
Missings ranged from 0.4% to 13.6% on total N and were excluded from the analysis. The missings were lowest for PCUs and PDCs (0.0%) and highest for MODS (up to 40.0%) and NHs (up to 15.9%).
Volunteer tasks
ADL and iADL tasks: 86% of organisations had volunteers helping with eating and 78% with lifting and moving (Table 3). Significant differences were found between organisation types for all ADL tasks, with sitting services on average having their volunteers perform the most ADL tasks (4.69) and NHs (1.80) (p < 0.001) and MODs (1.33) (p < 0.001) the least. Transporting patients was the most prevalent iADL task across organisations (69%), particularly in NHs (83%). Sitting services often have volunteers helping patients take medication (72%); this was rare in other organisation types. PCUs (4.26) and sitting services (3.69) on average had volunteers performing the most iADL tasks; MODs (1.40) and PHTs; (1.36) the least. (PCUs-MODs (p < 0.001); PCUs-PHTs (p < 0.001); sitting services-MODs (p < 0.001); sitting services-PHTs (p < 0.001).) PHTs had volunteers perform significantly less iADL tasks than PCUs (p < 0.001).
Tasks performed by direct patient care volunteers in healthcare organisations providing palliative care, Flanders, 2016 a .
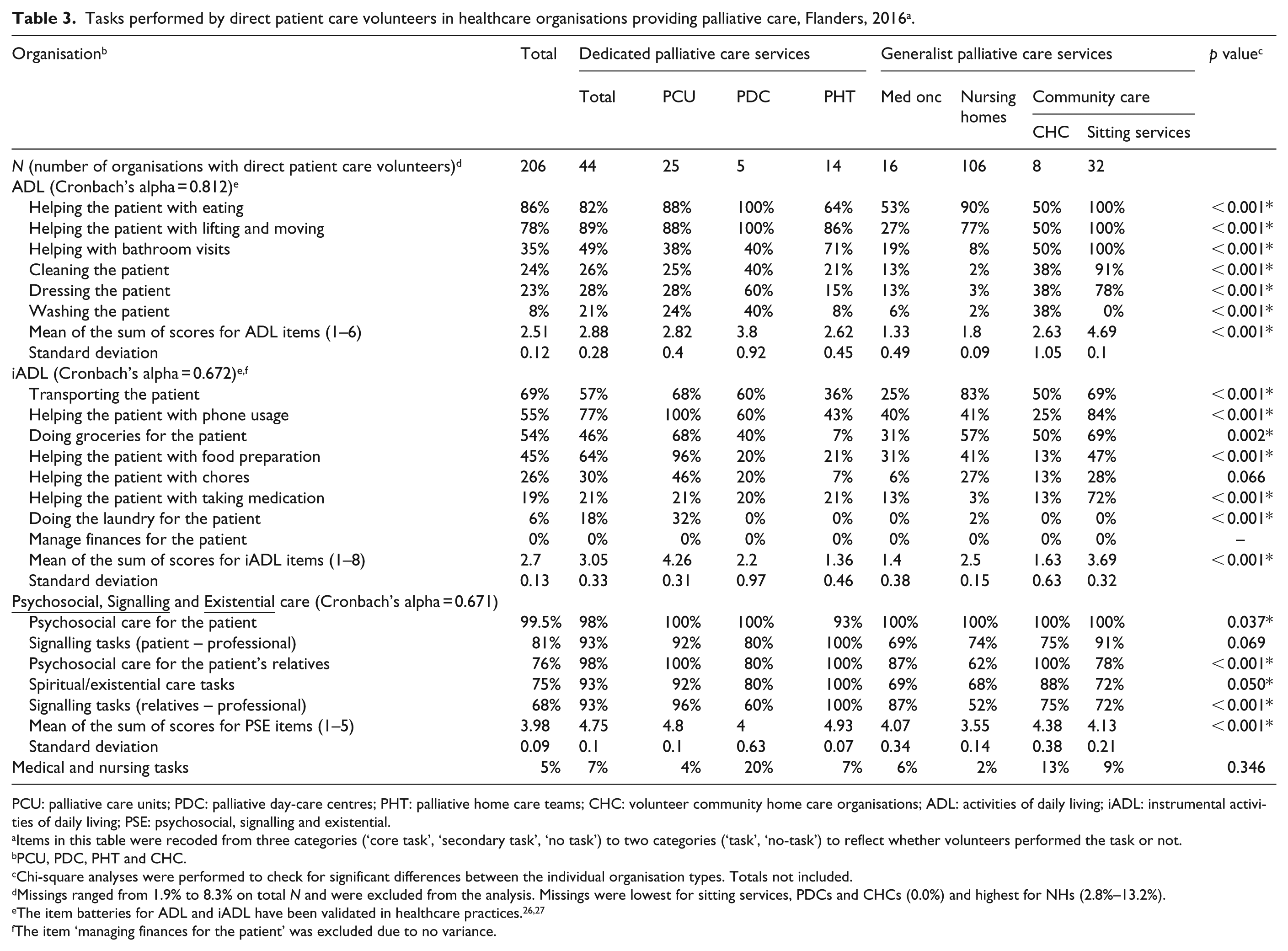
PCU: palliative care units; PDC: palliative day-care centres; PHT: palliative home care teams; CHC: volunteer community home care organisations; ADL: activities of daily living; iADL: instrumental activities of daily living; PSE: psychosocial, signalling and existential.
Items in this table were recoded from three categories (‘core task’, ‘secondary task’, ‘no task’) to two categories (‘task’, ‘no-task’) to reflect whether volunteers performed the task or not.
PCU, PDC, PHT and CHC.
Chi-square analyses were performed to check for significant differences between the individual organisation types. Totals not included.
Missings ranged from 1.9% to 8.3% on total N and were excluded from the analysis. Missings were lowest for sitting services, PDCs and CHCs (0.0%) and highest for NHs (2.8%–13.2%).
The item ‘managing finances for the patient’ was excluded due to no variance.
PSE: Almost all organisations had volunteers providing psychosocial care for the person who was dying (99.5%), 76% for their relatives. In 81% of organisations volunteers fulfilled a signalling function as a go-between for patients and professional caregivers and in 68% for relatives. Volunteers undertook spiritual and existential care tasks in 75% of cases; whether volunteers provide psychosocial care and signalling tasks for relatives differed significantly across organisation types, dedicated palliative care services on average undertaking the most PSE tasks (3.98) and NHs the fewest (3.55; p < 0.001). In 5% of organisations, volunteers performed medical and nursing tasks.
Barriers
The most cited barriers to maintaining and expanding a volunteering force were finding suitable (84%) and new (80%) volunteers, and the time investment a volunteering force requires (51%; Table 4). For sitting services, legal proscriptions regarding volunteer tasks (84%) were often cited. Financial costs were rarely cited except by sitting services (65%) and PHTs (57%). None of the PDCs cited financial costs as a barrier. Finally, the integration of volunteers into the organisation was identified as a barrier in 29% of organisations.
Organisational barriers to volunteerism and volunteer recruitment strategies for healthcare organisations providing palliative care, Flanders, 2016 a .
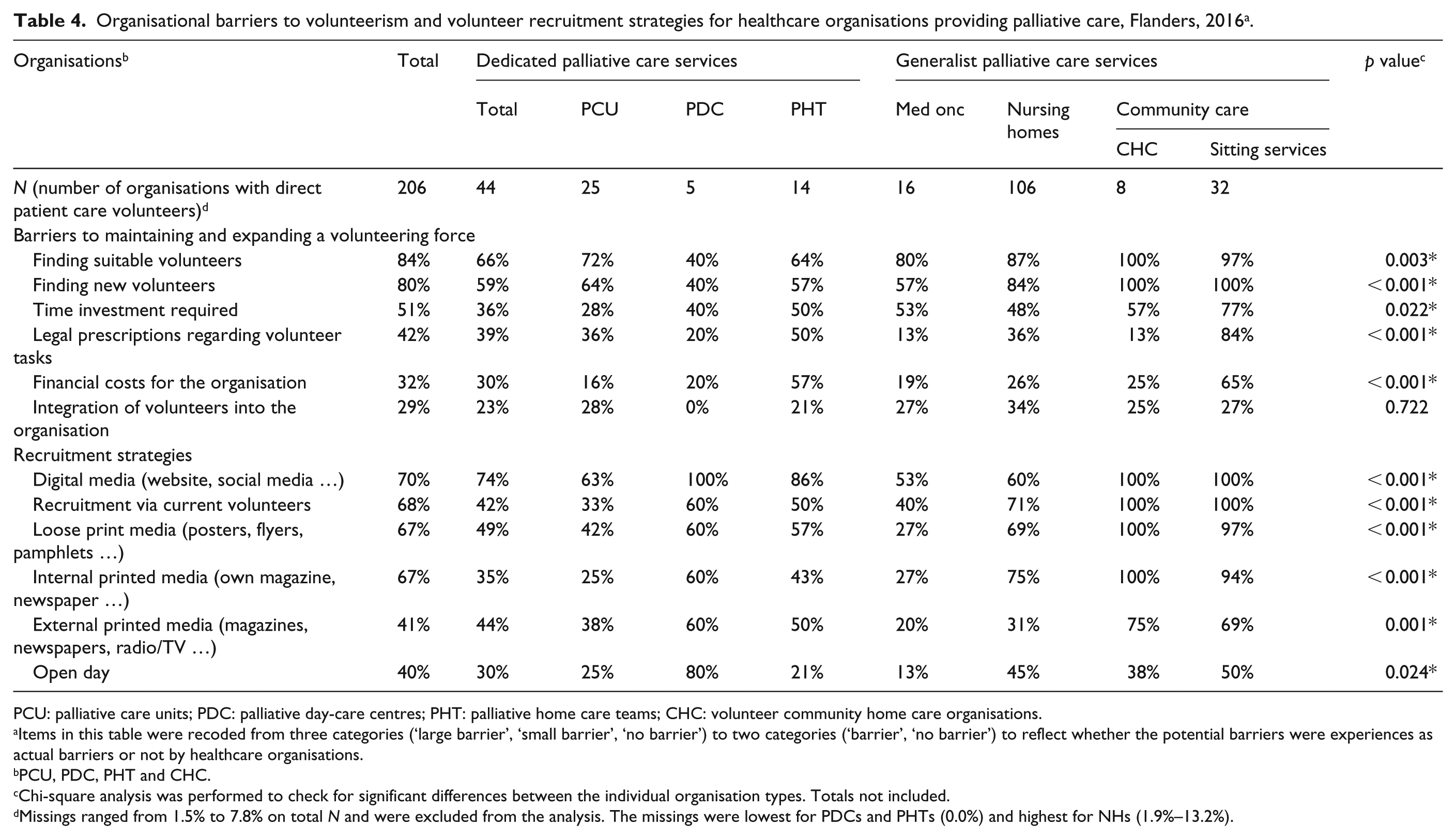
PCU: palliative care units; PDC: palliative day-care centres; PHT: palliative home care teams; CHC: volunteer community home care organisations.
Items in this table were recoded from three categories (‘large barrier’, ‘small barrier’, ‘no barrier’) to two categories (‘barrier’, ‘no barrier’) to reflect whether the potential barriers were experiences as actual barriers or not by healthcare organisations.
PCU, PDC, PHT and CHC.
Chi-square analysis was performed to check for significant differences between the individual organisation types. Totals not included.
Missings ranged from 1.5% to 7.8% on total N and were excluded from the analysis. The missings were lowest for PDCs and PHTs (0.0%) and highest for NHs (1.9%–13.2%).
Recruitment
Digital media (70%), current volunteers (68%) and internal printed media (e.g. monthly magazine) (67%) were the most prevalent recruitment strategies (Table 4). PDCs were the only organisation type of which the majority (80%) uses open days to recruit volunteers.
Volunteer training
Of all organisations, 91% indicated that training in some form was offered in direct patient care; 33% provided obligatory training (Table 5), dedicated palliative care services most often (75%) and NHs least often (12%) (p < 0.001). PHTs all provided obligatory training (100%). Overall, the most frequent training subjects were ‘themes regarding specific patient groups (e.g. dementia, cancer)’ (71%), ‘the organisation’s visions and values’ (61%), ‘volunteers’ positions and roles within care’ (56%) and ‘ethics (discretion)’ (54%). ‘Basic knowledge and skills in palliative care’ were only offered by 43%, mainly PDCs and PHTs (100%). ‘Advance care planning’ was only taught in 16%, mainly PHTs (86%).
Healthcare organisations offering training to their direct patient care volunteers in palliative care, Flanders, 2016 a .
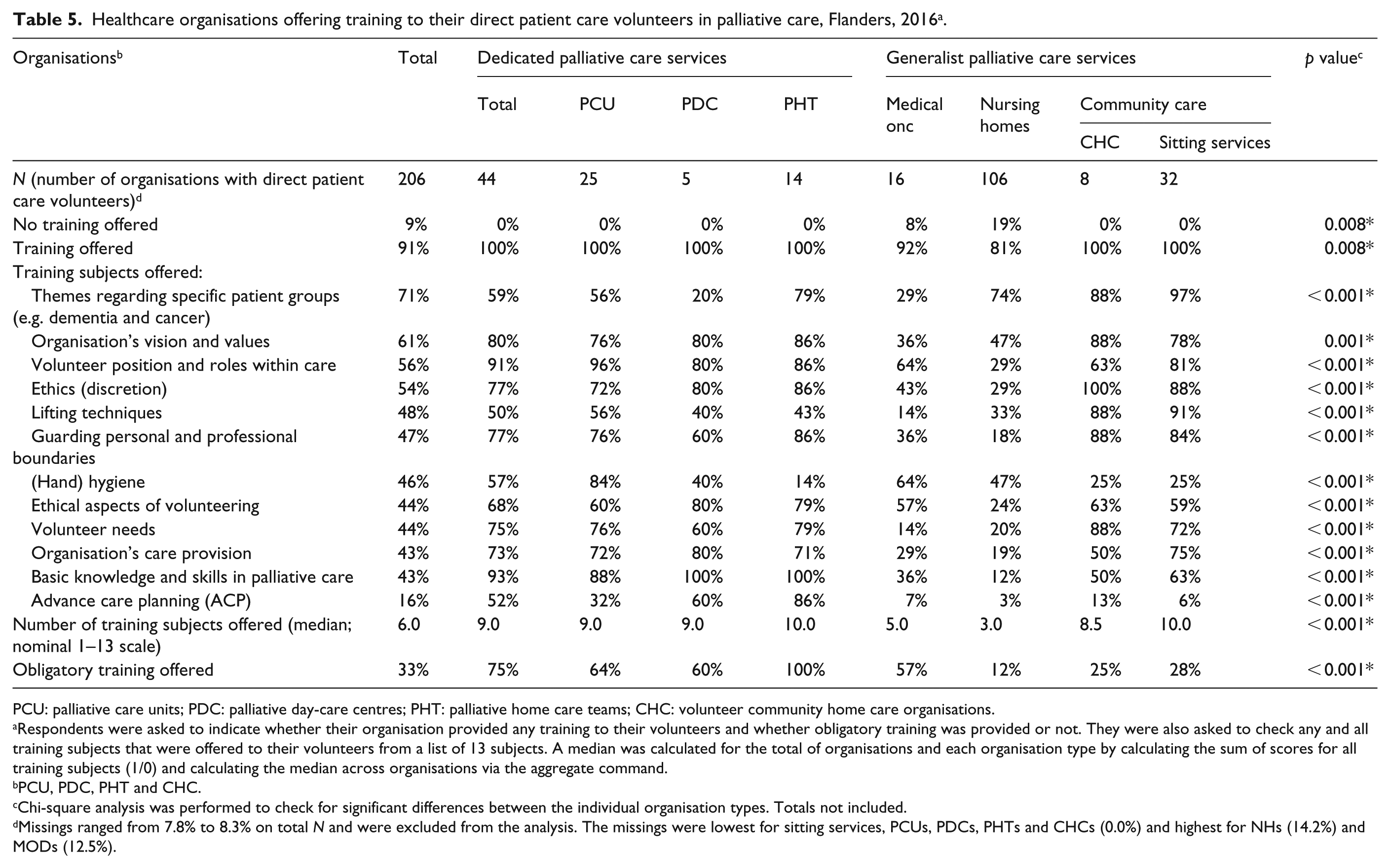
PCU: palliative care units; PDC: palliative day-care centres; PHT: palliative home care teams; CHC: volunteer community home care organisations.
Respondents were asked to indicate whether their organisation provided any training to their volunteers and whether obligatory training was provided or not. They were also asked to check any and all training subjects that were offered to their volunteers from a list of 13 subjects. A median was calculated for the total of organisations and each organisation type by calculating the sum of scores for all training subjects (1/0) and calculating the median across organisations via the aggregate command.
PCU, PDC, PHT and CHC.
Chi-square analysis was performed to check for significant differences between the individual organisation types. Totals not included.
Missings ranged from 7.8% to 8.3% on total N and were excluded from the analysis. The missings were lowest for sitting services, PCUs, PDCs, PHTs and CHCs (0.0%) and highest for NHs (14.2%) and MODs (12.5%).
Associations with volunteer use
Organisations that had their volunteers help with more ADL (p < 0.001), iADL (p < 0.05) and PSE (p < 0.001) tasks than the average organisation provided significantly more training subjects to volunteers (Table 6). They also more often provided training regarding basic knowledge and skills in palliative care and lifting techniques. Higher-than-average volunteer deployment in ADL and PSE care were both associated with higher provision of most, and in the case of PSE care all training subjects surveyed. Higher-than-average volunteer use in ADL care was associated with higher indication of organisational barriers such as finding new volunteers (p < 0.05), time investment required (p < 0.05), legal prescriptions regarding volunteer tasks (p < 0.001) and financial costs (p < 0.001).
Association of volunteer use with volunteer training, organisational barriers and organisation types.
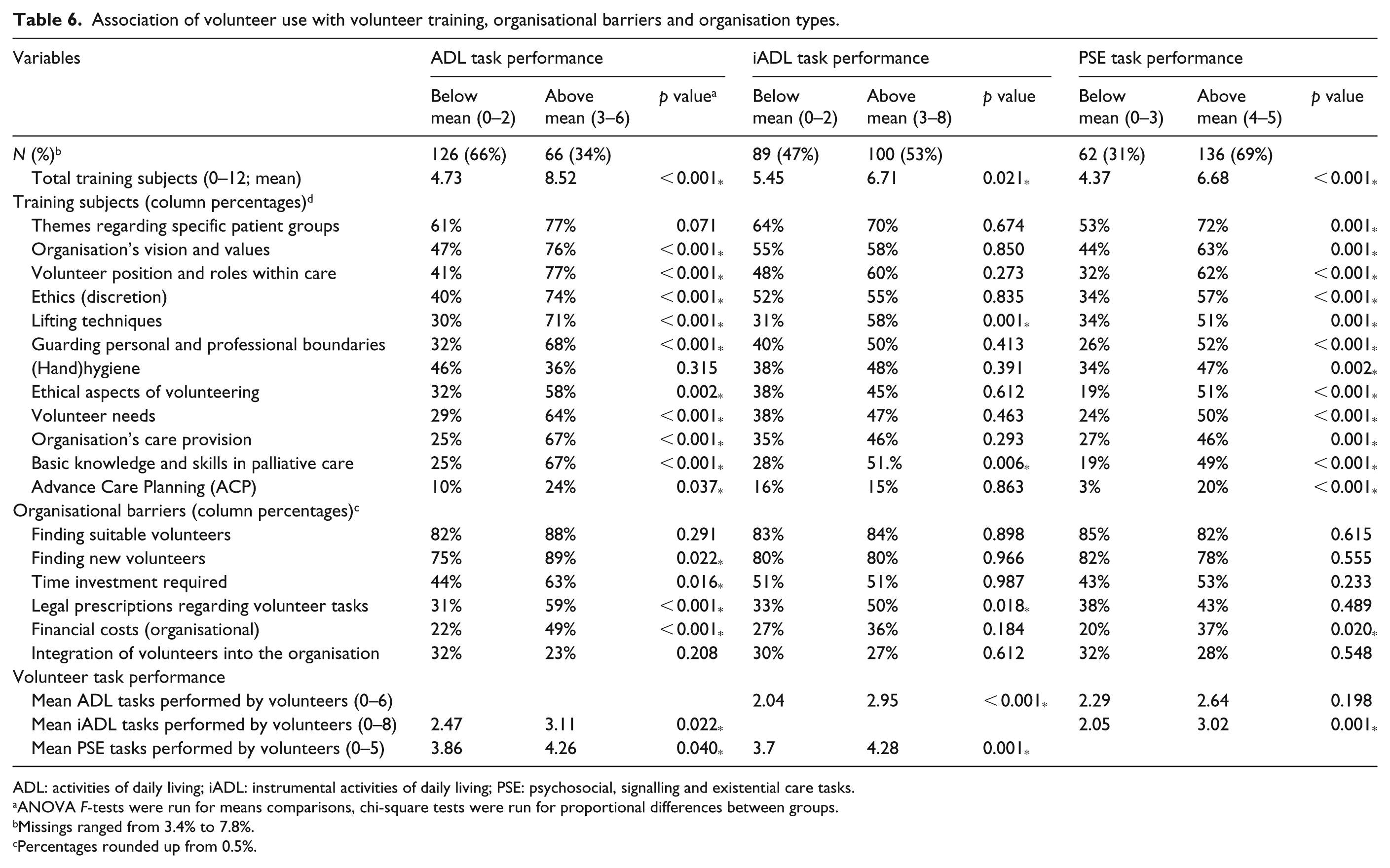
ADL: activities of daily living; iADL: instrumental activities of daily living; PSE: psychosocial, signalling and existential care tasks.
ANOVA F-tests were run for means comparisons, chi-square tests were run for proportional differences between groups.
Missings ranged from 3.4% to 7.8%.
Percentages rounded up from 0.5%.
Discussion
Main results
Direct patient care volunteers were present in both dedicated and generalist palliative care, most often in dedicated palliative care (97%–100%) and community care services (80%–97%) but also in a majority of NHs (73%) and MODs (64%). Volunteers across all organisation types perform various palliative care tasks including practical ADL and iADL tasks, the most prominent being PSE care tasks. Dedicated palliative care and community care services stood out regarding volunteer training and training subjects provided; NHs and MODs rarely provided palliative care skills or advance care planning training. Results showed that the most important barriers to having a volunteering force were acquiring new and suitable volunteers. Organisational emphasis on volunteer PSE care was related to higher volunteer training provision, while emphasis on volunteer ADL care was related to both higher volunteer training provision and higher indication of financial and legal barriers.
Strengths and limitations
This study is, to our knowledge, the first to map registered direct patient palliative care volunteering across a whole healthcare system in both dedicated and generalist palliative care. Its scope and sample frame allow observations to be generalised to the Flemish and Flemish-speaking Brussels context. While non-response was low, some bias is possible; some non-respondents may not have volunteers. In some cases, respondents may be remote from their volunteers, affecting the reliability of their responses. Although we followed a robust expert-consultation-based method to determine the sample of organisations potentially providing palliative care volunteers, there may be others with direct patient care volunteers. By focusing on registered volunteers, we potentially missed less frequent, unregistered forms of volunteering. Finally, because of our focus on the Flemish healthcare system, we did not include Wallonia and the French-speaking community in Brussels. As healthcare is differently organised in the French speaking part of Belgium, our results do not apply for palliative care volunteerism in these communities.
Interpretation
This study yields useful insights into the current state of affairs as well as challenges and opportunities for expanding volunteerism in view of the move towards greater informal care provision. However, direct patient care volunteerism imposes challenges and requirements that should be met. Our results indicate that direct patient care volunteers are an important part of palliative care provision, existing in each organisation type surveyed. In line with the existing literature, volunteers help with daily activities and provide PSE care, 30 making them complementary to professional care provision, particularly in generalist palliative care services.
Dedicated palliative care services differ internally in a few notable ways. Because palliative home care service volunteers visit patients living at home (with help from family, friends and home nursing services) they perform fewer of the iADL tasks than full live-in facilities such as PCUs, where staff and volunteers are required to perform them. These volunteers, furthermore, often visit patients alone. This may explain the higher provision of obligatory volunteer training compared with PCUs and day-care centres, as direct supervision is less frequent than in live-in facilities where paid staff and volunteers are in close contact. PDCs were the only group from which not a single organisation indicated financial costs as a barrier. This may be because it is a semi-live-in facility where many patients still spend much time at home and where volunteers only work in the facility. Finally, PHTs provided more training in advance care planning than PCUs. This difference may be explained by the rapid turnover in units and that patients may have already gone through the advance care planning steps prior to admittance to the unit. Regardless, the high percentage of home care teams that provides this training to volunteers is striking.
Financial costs and legal prescriptions regarding volunteer tasks were overall rarely perceived as organisational barriers for volunteer care provision in Flanders and Brussels. However, indication of these barriers was higher for organisations deploying volunteers in ADL care. Furthermore, organisations report difficulties recruiting, suggesting a key challenge is developing tailored strategies to engage potential volunteers. Given that palliative care volunteers31,32 and volunteers in general 33 tend to be older, digital media may not be ideal for them but younger generations may be more time-constrained. It is therefore worthwhile offering flexible, well-defined volunteering roles to suit all age groups.
Aside from recruitment, appropriate support and training are crucial. Stronger emphasis on volunteer ADL care and stronger emphasis on volunteer PSE care were both associated with higher training provision. In addition to the higher indication of barriers mentioned above, this suggests that some forms of volunteer use are more resource-heavy than others. Despite increased training requirements, NHs and MODs consistently scored the lowest on 9 of the 12 surveyed training subjects, including ‘basic knowledge and skills in palliative care’, ‘volunteer needs’ and ‘advance care planning’, while their volunteers still perform many of the same care tasks as dedicated palliative care services.
Despite the historical dependence of NHs on informal caregivers in Belgium and problems of understaffing,34,35 NH volunteers receive little training and perform relatively fewer ADL and PSE tasks. NHs may therefore not provide their volunteers with the required support for their tasks and may not employ volunteers efficiently with regard to quality of care. Investing in proper support frameworks in coordination with palliative professionals to train and support volunteers in their provision of direct patient care is therefore recommended. Employing volunteers does not remedy underlying problems of understaffing and lack of funding; however, their presence, when appropriately supported, may relieve stress on staff and increase quality of care and well-being for patients. The development of tension between professional caregivers and volunteers is not yet fully understood, however, and warrants further research into this subject.
To address recruitment and training issues, policy makers may consider a shared framework – a network connecting organisations providing palliative care, coordinated by a regional, national or perhaps even European 36 umbrella organisation – through which volunteers may be recruited and introduced to different healthcare organisations according to individual profiles. The palliative networks in Belgium function regionally and recruitment efforts between organisations are not well coordinated. Frameworks should therefore be designed to expedite coordination and could incorporate standard, context-sensitive training in palliative direct patient care. This could also stimulate locally led community development programmes organised around local NHs, PDCs or regional palliative network. 37 The Compassionate Neighbours project in London, UK, is an example of such a programme. 38
However, the underlying causes for the problems with volunteer recruitment may differ according to the care setting. Future research should investigate these causes within different organisational settings. Future research should also study the characteristics of palliative care volunteerism at the volunteer level as a contrast with organisational data. International comparative data could indicate whether findings are generalisable to different countries and provide benchmarking opportunities for countries and communities with regard to their palliative care volunteer potential and challenges.
Conclusion
Volunteers provide palliative direct patient care in both dedicated and generalist palliative care services. Volunteers are extensively used in dedicated palliative care settings and community care settings, providing PSE care as well as more supportive tasks, and provided with a wide range of training. A narrower approach, with fewer tasks, less training and less focus on interactions with residents, health professionals and relatives, is taken in other settings, such as NHs and MODs. Differences in volunteer use may explain reported organisational barriers and training provision. Given the partial shift from professional to community care provision at the end of life in some countries, policy makers may draw on the insights in this paper in developing policy for healthcare organisations providing palliative care.
Supplemental Material
772263_supp_mat_Questionnaire_general_version_(English) – Supplemental material for Palliative care volunteerism across the healthcare system: A survey study
Supplemental material, 772263_supp_mat_Questionnaire_general_version_(English) for Palliative care volunteerism across the healthcare system: A survey study by Steven Vanderstichelen, Dirk Houttekier, Joachim Cohen, Yanna Van Wesemael, Luc Deliens and Kenneth Chambaere in Palliative Medicine
Footnotes
Appendix 1
Acknowledgements
The authors thank Thijs Reyniers, who provided the Excel template to track questionnaire mail-out and response, Jane Ruthven, who performed language editing of the manuscript, all volunteer coordinators and organisational representatives of Flemish and Brussels healthcare organisations, who provided data on their organisation or coordinated data gathering in the organisations under their jurisdiction, and all experts from different healthcare organisations in Flanders and Brussels, who participated in our expert consultation.
Data management and sharing
The data of this study are with the first author and are available upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Innovation by Science and Technology (IWT) as part of the INTEGRATE-project (SBO-IWT 140009).
Research ethics and patient consent
The proposal for this study was submitted for approval to the commission of medical ethics of the university hospital of Brussels (ref. B.U.N. 143201627927). Approval was granted on 23 March 2016.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.