
Abstract
Background:
Carer factors prevent patients achieving timely and appropriate hospital discharge. There is a lack of research into interventions to support carers at hospital discharge.
Aim:
To explore whether and how family carers are currently supported during patient discharge at end of life; to assess perceived benefits, acceptability and feasibility of using The Carer Support Needs Assessment Tool (CSNAT) Approach in the hospital setting to support carers.
Design:
Qualitative.
Setting/participants:
Three National Health Service Trusts in England: focus groups with 40 hospital and community-based practitioners and 22 carer interviews about experiences of carer support during hospital discharge and views of The CSNAT Approach. Two workshops brought together 14 practitioners and five carers to discuss implementation issues. Framework analysis was conducted.
Results:
Current barriers to supporting carers at hospital discharge were an organisational focus on patients’ needs, what practitioners perceived as carers’ often ‘unrealistic expectations’ of end-of-life caregiving at home and lack of awareness of patients’ end-of-life situation. The CSNAT Approach was viewed as enabling carer support and addressing difficulties of discussing the realities of supporting someone at home towards end of life. Implementation in hospital required organisational considerations of practitioner workload and training. To enhance carer support, a two-stage process of assessment and support (hospital with community follow-up) was suggested using the CSNAT as a carer-held record to manage the transition.
Conclusion:
This study identifies a novel intervention, which expands the focus of discharge planning to include assessment of carers’ support needs at transition, potentially preventing breakdown of care at home and patient readmissions to hospital.
Keywords
Family carers are essential in making it possible for patients to remain at home towards the end of life and play an important role in achieving hospital discharge.
The multiple impacts on carers of taking on this role and their need for support are well recognised in end-of-life care policy guidance.
Palliative-care patients are often re-admitted to hospital following discharge due to breakdown in carer support at home.
A novel intervention for hospital discharge: expanding the focus of discharge practice to include assessment of carers’ support needs at transition to help prevent breakdown of care at home and patient readmission to hospital.
Identification of carers’ lack of awareness of the realities of 24-h caregiving and of patients’ end-of-life situation as a major barrier for practitioners wishing to support carers during discharge.
The potential of The Carer Support Needs Assessment Tool (CSNAT) Approach to facilitate conversations about the realities of caregiving at home towards the end of life, thereby eliciting carer concerns and enabling the provision of support.
Enabling successful discharge of palliative-care patients to home and prevention of readmissions is a key issue for health services.
To date, the focus of interventions to achieve this outcome has been on patients, yet we know that carers are crucial in enabling palliative-care patients to remain at home.
This study identifies key issues to be considered in turning current policy ‘aspirations’ for person-centred care for carers into practice realities within a hospital context.
Background
Timely discharge from hospital and avoidance of readmissions are major concerns of health services. In the United Kingdom, there is guidance about hospital discharge in general from different sources1–5 and specifically about hospital care at end of life (EOL).6–10 In both contexts, guidance makes clear the need to involve carers in discharge where they are involved in supporting patients at home. However, guidance references to involving carers ‘with the patient’s permission’ suggest their involvement relates more to meeting patients’ rather than carers’ needs with regard to caregiving after discharge to home.
We know from research that the majority of patients wish to die at home 11 and that family carers are essential in making home-care possible.12,13 Carer factors are an important contributor to difficulties in achieving timely and appropriate hospital discharge.14,15 The odds of discharging patients from hospital to die at home are considerably reduced if carers are reluctant to support discharge. 16 However, such reluctance may stem from lack of preparation and information. 17
Discharge is not a single event, but a process that includes prevention of breakdown of home-care and readmission. 14 Likelihood of remaining at home until death is reduced by two-thirds if carers prefer otherwise, even if patients are supported by palliative home-care, 18 and a major reason for hospital admission is breakdown of informal care at home, even where carers willingly take on care. 19 Carers therefore form a crucial component in successful discharge: ensuring they are prepared for home-care is likely to increase likelihood of discharge and decrease that of readmission.
However, research reviews show that carers often feel uninvolved and unsupported in the discharge process and that staff do not routinely identify and support carers.20–22 The majority of carers report not being asked about their needs or whether they can cope after the patient is discharged.14,20–25 Often health professionals do not realise that what appears routine to them is challenging to carers. 14
There has been a lack of research into interventions to support carers at hospital discharge in general: a scoping review of service provision for carers around hospital discharge found only five studies involved an intervention, none of which focussed on the discharge process as directly related to carers. 22 A systematic review of randomised controlled trials (RCTs) of discharge planning interventions found only 14 separate studies conducted over a 19-year period. 26 The review concluded that integration of caregivers into discharge planning reduces risk of hospital readmission, but was unable to determine the most effective method of caregiver integration. An Australian trial has tested a specific carer intervention at discharge: the Further Enabling Care at Home (FECH) programme which involved telephone assessment and support delivered by a dedicated FECH nurse. 27 The trial showed significant improvements for carers enrolled in the programme in preparedness to care after discharge and reduction in caregiver strain.
The Carer Support Needs Assessment Tool (CSNAT) Approach, which formed part of the FECH programme, is an intervention developed, tested and implemented in hospice home-care as a comprehensive, person-centred approach for assessing and supporting carers.28–33 The aim of this study is to focus on carers in the discharge process: (1) to explore whether and how carers of palliative-care patients are currently supported at discharge from hospital at EOL and (2) to assess perceived benefits, acceptability and feasibility of using The CSNAT Approach in the hospital setting to support carers during discharge. This is the first development stage of the Medical Research Council (MRC) Framework for Evaluation of Complex Interventions 34 to develop an intervention to facilitate discharge. Figure 1 provides an overview of The CSNAT Approach.
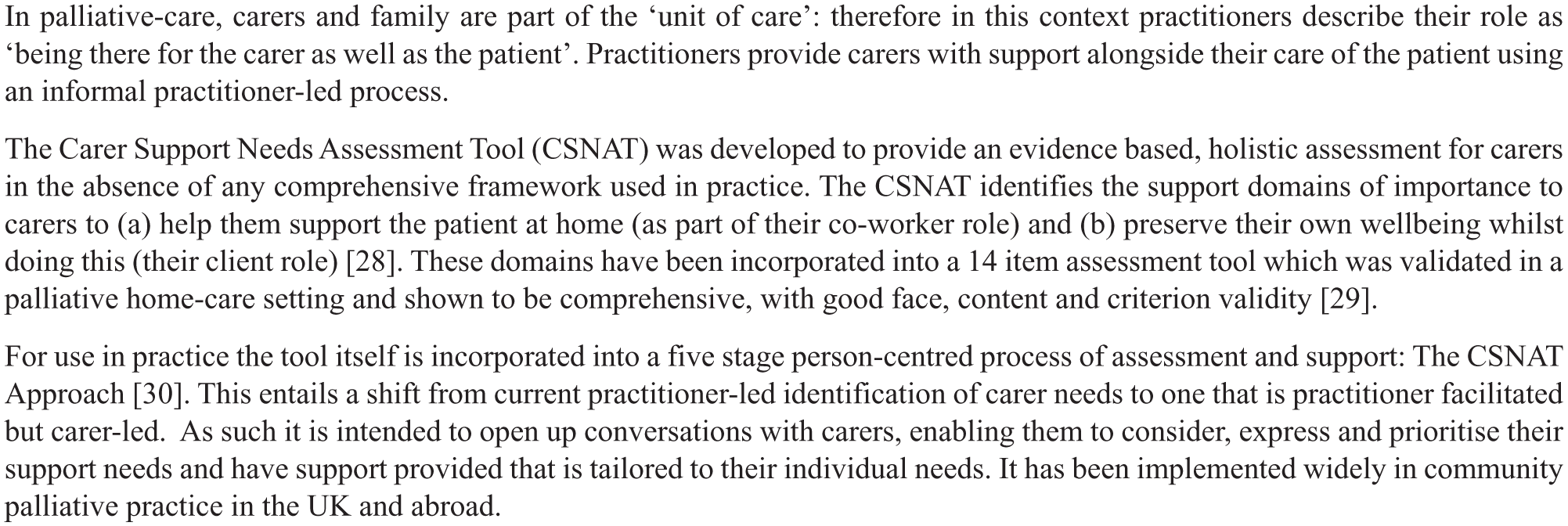
The CSNAT Approach.
Methods
Qualitative design: focus groups, interviews and workshops
Ethical approval was received from NRES Committee Northwest–Greater Manchester West on 9/10/14 (REC reference no. 14/NW/1311). All participants provided written consent.
Setting and scope
The study was conducted between December 2014 and November 2015 across three National Health Service (NHS) Trusts in England serving a diverse population in terms of social deprivation, ethnicity and urban/rural areas. The primary NHS site recruited practitioners and carers. The other sites recruited practitioners.
The study focussed on discharges to home of patients with a palliative condition who had a carer (see Figure 2 for criteria of discharges). ‘Family carer’ or ‘carer’ may not always be a conventional family member, but denotes a lay person who provides a close, supportive role.
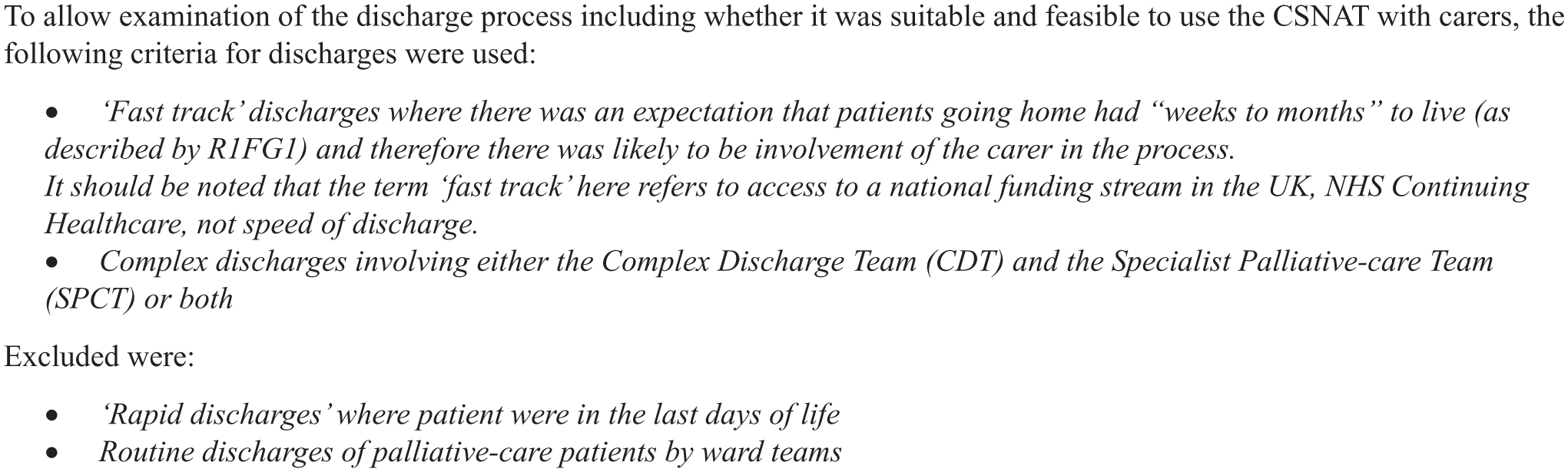
Scope of palliative-care discharges.
Recruitment and data collection
Focus groups with healthcare professionals
Practitioners were purposively sampled from teams involved in discharge of patients with a palliative condition to home (specialist palliative care, complex discharge, community Macmillan and district nursing teams) aiming for broad representation of different healthcare professionals (HCPs). A lead contact in each Trust facilitated recruitment by distributing study recruitment packs to teams containing an invitation letter, study information leaflet, reply form and freepost envelope for its return. Interested HCPs responded directly to study researchers.
In total, 40 practitioners took part, 29 from hospital, 11 from community. Participants are described in Table 1.
Healthcare professional participants.
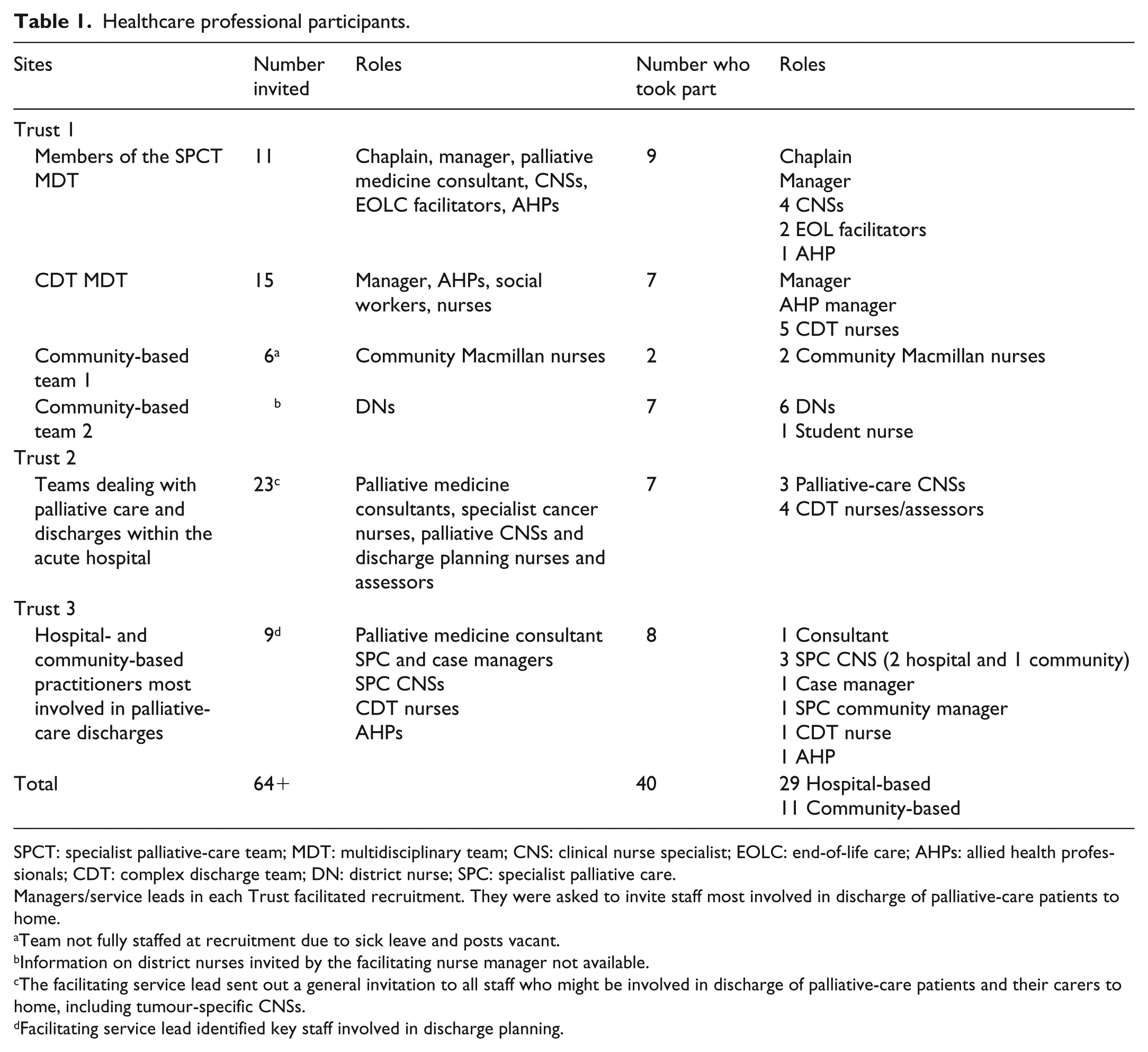
SPCT: specialist palliative-care team; MDT: multidisciplinary team; CNS: clinical nurse specialist; EOLC: end-of-life care; AHPs: allied health professionals; CDT: complex discharge team; DN: district nurse; SPC: specialist palliative care.
Managers/service leads in each Trust facilitated recruitment. They were asked to invite staff most involved in discharge of palliative-care patients to home.
Team not fully staffed at recruitment due to sick leave and posts vacant.
Information on district nurses invited by the facilitating nurse manager not available.
The facilitating service lead sent out a general invitation to all staff who might be involved in discharge of palliative-care patients and their carers to home, including tumour-specific CNSs.
Facilitating service lead identified key staff involved in discharge planning.
Eight focus groups (FGs) were conducted, lasting 35–105 min, facilitated by two researchers (L.A./G.E., L.A./D.J. or G.E./D.J.). Discussions were recorded with participants’ permission. The topic guide covered four broad areas: (1) current assessment processes leading up to patient discharge including involvement of carers, (2) exploration of carer-related concerns surrounding discharge, (3) initial views of the CSNAT and its person-centred approach and (4) when/how The CSNAT Approach may be used at discharge to improve carer support.
Interviews with carers/next of kin
Bereaved and current carers/next of kin (hereafter called carers) were invited to participate. Carers of patients discharged from the Trust shortly before death and who were 6–18 months post-bereavement were eligible and were identified by the Trust’s Information Team together with the specialist palliative-care team (SPCT) and complex discharge team (CDT). Current carers were identified at weekly hospital multidisciplinary teams (MDTs). The SPCT highlighted any instances of concern about carers’ ability to participate in an interview. All invitation packs to carers were sent by the SPCT: interested carers responded directly to the study researcher (L.A.) who provided further information, arranged an interview with them at home and took informed consent prior to interview. Table 2 summarises recruitment and characteristics of 22 carer participants.
Characteristics of carer participants.
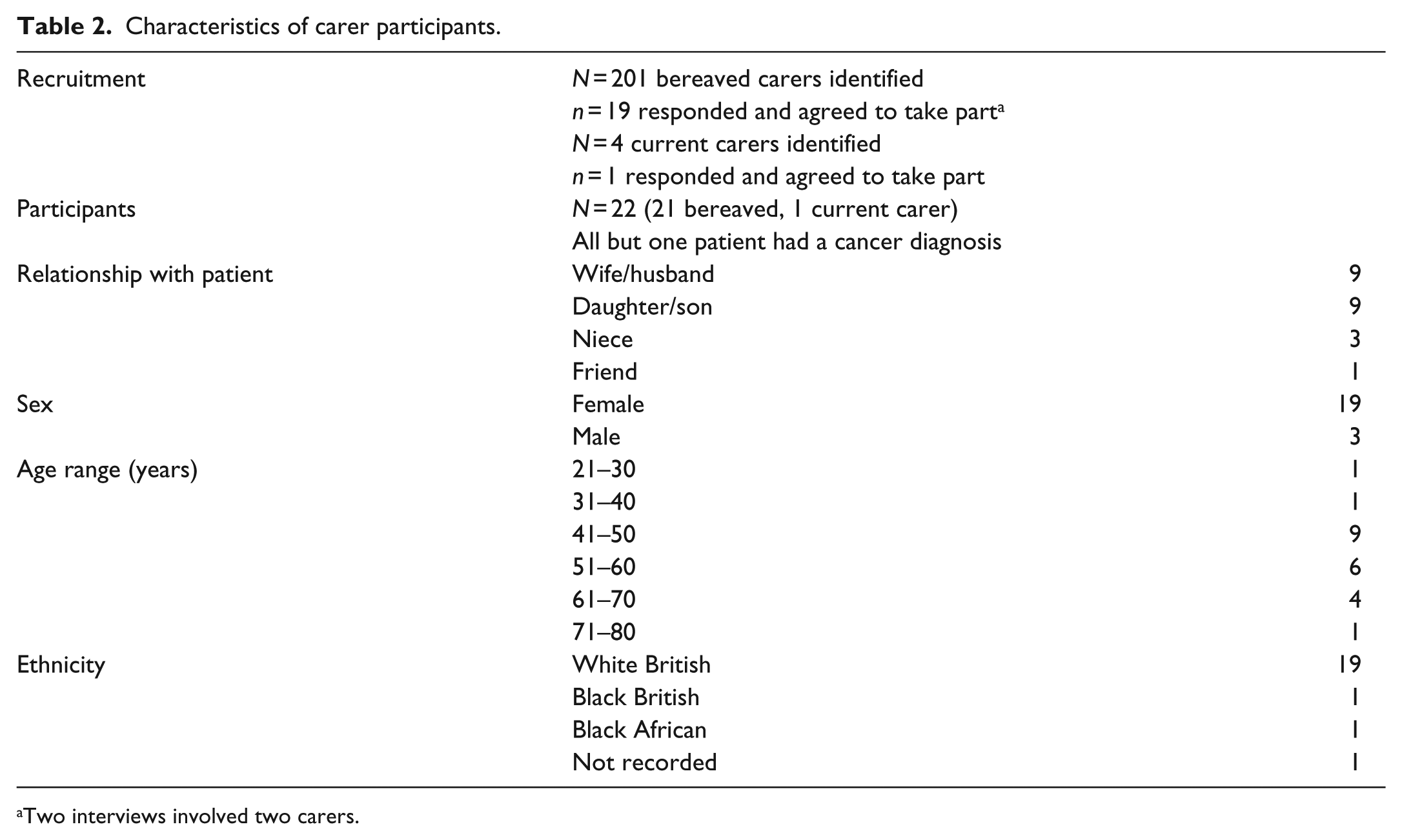
Two interviews involved two carers.
Interviews with carers were recorded with their permission. Discussions began with an exploration of carer’s experience of the discharge process and any concerns they had about the planned discharge. Carers’ views about the CSNAT were sought: asking them to reflect back on their caring experiences and say whether they felt it would have helped them discuss any concerns.
Workshops with HCPs and carers
Workshops were mentioned to participants at the end of FGs and interviews. Carers who expressed an interest in further participation were invited to the workshops. All practitioner participants were also invited. Two workshops took place with 14 HCPs (7 SPCT, 4 CDT, 2 district nurses and 1 community nurse team leader) plus five carers (all bereaved). Attendance was dependent on availability on days scheduled for workshops.
Workshops lasted 2.5 h (including lunch/refreshments) and were recorded with participants’ permission. Each workshop began with a brief overview of the study, key findings and a reminder of The CSNAT Approach. This was followed by (1) whole group discussion of the tool itself and then (2) small group discussions of how this new approach might be used with carers at hospital discharge towards EOL.
Data analysis
All recordings were fully transcribed, checked and anonymised. A thematic analysis was conducted, based on the framework approach. 35 The analysis process involved two researchers (D.J./G.E.). Initial transcripts were read and re-read by the researchers to gain familiarity with the data. Then each researcher, independently, developed an indexing framework of key issues arising from both data and topic guides. Key issues identified were compared and discussed, and a coding framework agreed to organise the data. Atlas/ti was used to facilitate data management. The coding framework was applied to all transcripts by D.J., checked by G.E. and minor additional codings were added. Both researchers wrote notes/memos throughout the process of data collection and analysis. Broad themes derived from the data were identified and interpretations discussed and agreed.
Findings
Findings are organised into three sections, representing practitioners’ and carers’ perspectives: (1) current barriers to supporting carers at hospital discharge, (2) utility of The CSNAT Approach for hospital discharge and (3) fit of The CSNAT Approach within a hospital context. Italics indicate verbatim quotations. ID numbers beginning with P indicate responses from practitioners and those with C are from carers. We have also indicated which FG (e.g. FG1) or workshop (e.g. W1a) the quotation came from.
Current barriers to supporting carers at hospital discharge
Organisational focus on patients’ needs, not carers’
Needs assessments on discharge naturally focussed on patients: ‘… because the patient and the duty of care that we have to the patient is uppermost in our mind’ (P2FG3). Emphasis was placed on practical aspects of discharge (e.g. equipment needs and services for patients) often driven by getting NHS Community Healthcare (CHC) funding in place: ‘so the care is planned and I think it’s a very physical approach, a practical approach, I don’t think the emotional element sits in with it really’ (P2FG2). Services had no procedures for identifying carers’ support needs at patient discharge as unlike hospice contexts, services were not formally ‘there for the carer as well as the patient’. While carers participated in discharge conversations, this often depended on them being present when the patient was assessed. The assessment therefore focussed on patients’ needs: any carer concerns were picked up informally. The following quotation exemplifies the lack of a carer remit ‘Honestly, the carers are my second thought and they’re only my thought if there becomes a difficulty, so as long as they’re happy with everything and everything is going along, I don’t consider their [needs]’ (P5FG7). Carers’ experiences reflected this: none of those interviewed described any formal assessment of their needs. However, carers had very a strong sense that they needed support at this time: ‘I think that’s what they need, people need support when they come out. The carer needs the support as much as the patient, because without the carer where does the patient go?’ (C5).
Carers’ ‘unrealistic expectations’ of caregiving at EOL and support at home
Further problems could occur if carers had what practitioners described as ‘unrealistic expectations’ about caregiving at home. Practitioners found that carers often just wanted the patient to go home, but they did not necessarily have a clear idea of the reality of 24-h caregiving: You try and make them aware of the sort of responsibility as well that they’re going to have at home and how they’re going to deal with the situation and get their thoughts about how they feel they’ll cope when they get home. (P4FG7) This was echoed by district nurses who cared for patients post-discharge: ‘[carers] don’t realise until they get home the physical and emotional demands that that then brings, and quite often within 24 or 48 hours of being home, you get a bit of a crisis going on’ (P2FG5). Others recognised that as the process itself was designed to help facilitate discharge, the level of detail carers needed got missed.
Mistaken impressions had also to be managed regarding level of nursing support likely to be available at home: ‘that a Macmillan nurse will be in that house 24 hours a day. They will order all the care, they will order all the medications, they will sort all the financial stuff out’ (P3FG1) or that district nurses could be expected to respond instantly if symptoms change. Expectations of availability of support at night were a particular difficulty because ‘nights are often the thing that tip people over the edge’ (P5FG5). Practitioners felt that conversations about expectations needed to happen earlier in the process: ‘someone explaining the actual nitty-gritty of things to people might be a bit more realistic for them to make that informed choice rather than get home and have the shock of it’ (P6FG5).
Lack of awareness of EOL situations
A significant barrier to preparing carers for patients’ discharge expressed by all practitioner groups was when carers had limited awareness that patients were approaching EOL. This posed difficulties for practitioners with eliciting carer concerns: they described not having skills for EOL conversations and for some this resulted in them ‘trying to backtrack’ (P4FG4) or ‘backpedalling’ (P5FG7) to avoid these discussions altogether. Furthermore, lack of carer awareness meant practitioners were unable to put in place certain supports on discharge: ‘… denying them, for example, Hospice at Home, you know, and Macmillan, denying them all sorts of services’ (P1FG2).
Utility of the CSNAT for comprehensive, carer-centred assessment in hospital
Given absence of any assessment process for carers at discharge and problems associated with this, initial practitioner responses to using the CSNAT were very positive: ‘I think it looks good’ (P2FG1). They said it covered everything they would expect to see: ‘Yes, definitely the right questions’ (group agreement FG8), with one group reflecting on its usefulness: ‘because we’ve got nothing at all in place and also I am aware that there are quite a few things on here that we don’t do very well’ (P3FG5). Carers too were entirely positive: ‘it’s a good tool’ (C21); ‘I think that would be very useful’ (C22). They reflected: ‘They should be asking all these questions, you know, to the carers’ (C11); ‘I think all those are something that need dealing with, don’t they’ (C6). Potential benefits were also identified, outlined below.
Legitimising support for carers themselves
Carers identified their own reluctance to consider support for themselves at this time: ‘because I think you put yourself on the back burner, you do, all carers put themselves on the back burner’ (C21). The CSNAT was therefore seen as valuable: ‘[it] gives the carer permission to think about themselves’ (C21W2a). Practitioners concurred, ‘relatives feel that they need the permission to say, do you know what, I can’t do this and I need help’ (P2W1b). Furthermore, practitioners felt that using the CSNAT would clearly indicate their interest in supporting carers: … with the best will in the world, they’re also very focused on that individual, and then a ‘How are you?’, it’s polite and it’s respectful and it’s cursory, but it’s not like this. It actually says we actually care about how you are feeling. (P4FG5)
Visibility of support needs
Carers found actually being able to see the CSNAT questions useful in enabling them to consider support needed as most had no idea what caregiving towards EOL involved. One carer explained, because you’re completely at sea, you’ve no idea, you’re going home with your family member with their bag of drugs and if somebody said, ‘what kind of help do you need?’ you wouldn’t know, you need to have … in a situation like that you’ve got to have prompts and suggestions, would you need help with this, would you need … and that’s perfect. (C20)
This contrasted with the current situation where ‘the ball’s put in your court to think of what you need to ask’ (C3), which was unhelpful when carers felt they did not know what to ask. Giving carers the opportunity to see the CSNAT domains made a few practitioners worry that carers might be upset: ‘I worry as well is whether the main people absolutely panic and think what’s going to happen. They’ve given me this, I haven’t even thought of half of this one’ (P2FG6). However, this view was not expressed by carers.
Assisting communication of support needs
The CSNAT Approach was seen as enabling carers to communicate their needs: ‘And I think because it does give people the opportunity to say, “No I don’t need that, I don’t need that, actually I really do need this”’ (C20). Having a copy of the tool itself further enabled this: ‘… sometimes you don’t know what to ask and you can’t remember. Whereas if you’ve got something written down that you can go back to, you can make notes or you can gather your thoughts’ (C7). This was particularly pertinent when carers were becoming overwhelmed or feeling emotional. This view was shared by practitioners: ‘when it’s on paper’. ‘You can put down your thoughts and feelings on a piece of paper when you’re on your own’ (P1W2a).
Facilitating discussion with carers of caregiving at EOL and support at home
Importantly, practitioners felt that The CSNAT Approach would help address carers’ lack of awareness about caregiving at home which was a significant barrier to providing support, for instance: You could actually hand it to them and say, ‘I want you to look at this, and the next time we come back, we’re going to talk about it’. Because sometimes you haven’t got, like, time to spend going slowly through something. But if they’ve had a chance to just have a quick look, to look at it when they were quiet, and think, right, I just need that. And then the next time the nurse comes, you can say, ‘Have you had a look at that, and what did you think?’ And then it just, sort of, like, opens things up. (P6W1d) Having a ‘way in’ to these types of conversations was valuable: You know, sometimes that [the CSNAT] could perhaps be a really good prompt for that scenario. And I have to say, as a practitioner, those scenarios where you have someone saying no, I’m going to take them home, I’m doing it all myself, are the hardest ones to work through. (P5W2a) The ‘way in’ to opening up discussions was also made easier by the questions: ‘none of [the questions] say that you’re dying, do they?’ (P2W1b) but ‘a lot of them are what they should be discussing on discharge anyway’ (P3W1b).
Fit of The CSNAT Approach within a hospital context
Practitioners and carers identified organisational issues to be addressed to implement this approach.
Organisational factors
Responsibility for the process of carer assessment
The many practitioners potentially involved in hospital discharge towards EOL may diffuse responsibility for supporting carers. There was no consensus on who would be best placed to assess and support carers, each role having advantages and disadvantages. For example, it was considered well suited to SPCT members, but they may see only a small percentage of hospital palliative-care patients. Thus, responsibility for carer support would need to be determined within each hospital setting.
Time and workload capacity
Consideration of workload implications for assessment was required, as carer assessment is not usual hospital practice: ‘I don’t think it’s the time to do that. I honestly don’t. They don’t have time to do the drug rounds let alone anything else’ (P2W1a). Carers’ experiences reflected this: Nurses are running round like blue-arsed what’s-its, so you don’t want to ask them either. So you end up with this, ‘It’ll be alright, It’ll be alright’. And you don’t ask because you know everyone’s so busy. So you need to have something built in. (C21W2a)
Skills and training
Implementation of a new way of working had implications for training. Most hospital staff are generalists unlikely to have skills in EOL communication or awareness of carers’ situation, so training was seen as essential. In addition, hospital practitioners are not necessarily familiar with community resources, particularly around carer support: ‘it’s about the information, it’s about what’s out there. And if you don’t know what’s happening, you can be talking about home, and people have this lovely rosy view, but the practicalities are very different’ (P9W2b). There was also recognition of the need for more education of staff in person-centred care ‘actually identifying what is important to that person and then supporting [them]’ (P2W1b), given this underpins the CSNAT approach.
Incorporating The CSNAT Approach into routine practice
In addition, consideration of how carers could be included in the discharge process was required, including when the process was initiated, and how it could follow patients and carers through to the home-care setting.
Earlier engagement with carers
A clear message was that the CSNAT needed to be introduced early in the patient’s hospital stay, not when preparing for discharge as this was ‘a bit too late […] I think it’s great that it’s there for discharge but I think it needs to be more thought about earlier on’ (C17). Practitioners agreed, reflecting that carers are too focussed on getting patients home at this stage; this reality summed up as ‘Just get him home, stop giving me forms’ (P5aW2d). Instead, it was felt that the CSNAT could be used even before discharge was discussed: … to actually pick up any carer concerns, and then if discharge was then an option I think and kind of refer back to that. So it’s almost like a two part thing, it’s assessing the concerns but then checking out those concerns in relation to proposed discharge. (P1W1a) Advantages of its earlier use included making more time available for discussions, rather than rushing conversations immediately prior to discharge. Importantly, it would also provide an opportunity to ‘manage carers’ expectations’.
A two-stage process of assessment
To ensure meaningful support for carers at discharge, a hospital-based assessment alone was viewed as insufficient. Rather, a two-stage process linking hospital carer assessment with follow-up by community staff was viewed as essential as the full impact of caregiving was only realised once at home. One carer explained, ‘because until she was home we hadn’t realised we’d have a problem at night. […] we thought she’d go to bed and she’d be able to go to the toilet like she always could before and she couldn’t’ (C4). Thus, a further review was seen as crucial: P3: ‘… maybe even a couple of days later, because until they’re actually at home they don’t’. P2: ‘They don’t know what they don’t know’. P1: ‘A lot of people just have no idea what it’s like’ (W1a). Incorporation of the CSNAT into referrals to community nursing would enable the two stages of the process to be linked to alert community staff to the carer’s situation and act as prompt for completing a home-based assessment: ‘So if that [the CSNAT] […] came through with the initial discharge and then we would have a copy of the notes with maybe something on it, redo on such and such a date’ (P3W1a).
CSNAT as a carer-held record
To manage transition between hospital and home, workshops discussed the CSNAT as a carer held-record: ‘if the carer was to take ownership of this document, then it would be their continuity of care wouldn’t it, for them to take from the hospital to the community, to get the answers along the way’ (P1W2a). Others agreed: ‘I think ideally it would go with the carer’ (P4W1b), but were sceptical about how this might work ‘in the real world’, identifying that ‘it would work in a percentage of cases and then in other cases it wouldn’t work because people have different lives and lifestyles’ (P1W1b). Carers themselves felt it was a realistic option: I think it starts there with a normal mini meeting in the hospital, things are discussed, the person [patient] moves out, the carer takes the CSNAT […] home with them and the link happens where the practitioners say, right, okay, district nurses or community need to come in and help but then it starts again. (C4W1c)
Discussion
This article examines carer support during hospital discharge of palliative-care patients. Within current hospital practice, barriers to supporting carers were an organisational focus on patients’ needs, carers’ ‘unrealistic expectations’ of EOL caregiving at home and lack of awareness of patients’ EOL situation. Given absence of any routine process for identifying carers’ support needs at patient discharge, The CSNAT Approach was viewed positively by both practitioners and carers. Anticipated benefits included legitimising carer support, providing visibility of support needs and assisting their communication. Importantly, practitioners felt The CSNAT Approach could facilitate conversations about the realities of supporting someone at home towards EOL. In order to achieve its implementation within discharge planning, organisational factors were highlighted: which practitioners would undertake the assessment and workload and training implications. Incorporation into practice required engaging carers earlier in the hospital stay and managing transition between hospital and home through a two-stage process of assessment of carers’ support needs using CSNAT as a carer-held record.
We found little evidence from carers or practitioners that carers’ needs were identified and supported within the discharge process. On one hand, this is perhaps unsurprising in the hospital setting where the majority of practitioners would identify their role as caring for patients, unlike in hospice care where the ethos also includes supporting carers. However, the End of Life Care Strategy 36 has long recognised the impact on carers of caregiving, and National Institute for Health and Care Excellence (NICE) has Quality Standards for end-of-life care 37 and transitions between hospital and home 9 which include comprehensive assessment and holistic support for carers and family according to their needs and preferences. Failure to implement these standards would appear to be a missed opportunity to better prepare carers for caregiving at home and so reduce the likelihood of readmissions.
A common difficulty for practitioners was preparing carers for the realities of EOL caregiving. Consequently, when introduced to The CSNAT Approach, practitioners’ reactions were very positive. As in previous CSNAT studies, 32 anticipated benefits included giving carers permission to consider their own needs, opening up conversations, assisting communication about support needs and offering a ‘way in’ to difficult discussions. As such, The CSNAT Approach may enable practitioners to achieve the ‘honest, informed and timely conversations’ which are one of the building blocks identified for achieving the Ambitions for Palliative and EOL Care for carers as well as patients. 38
While recognising the utility of the CSNAT, participants were clear about practicalities to be addressed including who should undertake the assessment and the implications for workload. In addition, training reinforcing person-centred approaches to assessment and support would be required. The current vision for EOL care 38 is based on the House of Care model which puts person-centred care at its core. Implementation of person-centred-care with patients is not without difficulty, requiring re-consideration of professional roles. 39 The challenge of this approach for carers is even greater, particularly in acute hospitals where carers are not within the remit of the majority of services. A value of this study is that it identifies what is required to turn current policy ‘aspirations’ for carers into practice realities within acute hospitals and provides a foundation for further work on implementation in this context.
Carers and practitioners identified how carer assessment and support could be facilitated through the transition between hospital and home. This involved a two-stage process: (1) starting assessment early in the hospital stay, in keeping with the principles of effective discharge planning 40 and (2) follow-up review by community practitioners at home, using the CSNAT as a carer-held record to manage the transition. This is a novel intervention, focussed on supporting carers, to enhance the discharge process. There is existing evidence that both transition-care planning and coordination 41 and integration of informal carers in discharge planning 29 are factors affecting hospital readmissions. In addition, we know that interventions which assist transition from hospital to home are effective in reducing hospital readmissions and that those starting during the hospital stay and continuing after discharge are more effective than those starting after discharge. 42 This potential intervention puts these factors into practice, underpinning further work on intervention implementation.
Limitations of the study
This was an initial exploratory study; however, it was conducted within three large hospitals with key staff involved in discharge planning. Due to the difficult and sensitive subject area, many carers did not respond to the invitation to take part. Those who did take part provided highly valuable insights into current practice and potential use of The CSNAT Approach. The study was limited to perceptions of acceptability and feasibility of The CSNAT Approach as an intervention: the real test comes when it is implemented in practice. Nevertheless, the consistency and agreement between both practitioners and carers provides a strong underpinning for a future implementation study.
Implications for practice
Enabling successful discharge of palliative-care patients to home and prevention of readmissions is a key issue for health services. To date, the focus of interventions to achieve this outcome has been on patients. Yet we know that carers are crucial in enabling palliative-care patients to remain at home. This study shifts the focus of current practice of discharge planning to include whether and in what way the support needs of carers might be assessed and addressed during the transition to home-care. In so doing, it offers a new direction for intervention development for hospital discharge with the potential to improve support for carers over the transition to home and prevent breakdown of care at home which is often a cause of readmission of patients to hospital.
Footnotes
Acknowledgements
The authors are extremely grateful for the time and contribution of carers and practitioners who took part in this study. Special thanks are due to Mary Ledwick, our PPI advisor, who provided guidance and support throughout the study and who along with Dr Janet Diffin helped facilitate study workshops. The authors also wish to thank Dusia Romaniuk for facilitating participant recruitment. All authors have made a substantial contribution to the work of this paper and approved the final version of the manuscript. G.E.: substantial contribution to the study design, acquisition of funding, data collection, analysis and interpretation of data and drafted the article; L.A.: data collection, interpretation of data and revised article critically for important intellectual content; D.J.: data collection, analysis and interpretation of data and revised article critically for important intellectual content; G.G.: project lead, designed the study, acquisition of funding, data collection, analysis and interpretation of data and revised article critically for important intellectual content.
Accessing the CSNAT
The CSNAT is a copyright tool available free of charge to the NHS and not-for-profit organisations. Registration and a licence are required for its use. For further details about obtaining an inspection copy, please contact Dr Gail Ewing at the University of Cambridge (
Data management and sharing
The primary data for the study consist of a corpus of audio-recorded focus groups, interviews and workshops. The authors do not have participants’ consent to share these data with third parties. This includes person-identifiable data within interview transcripts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by a Marie Curie Project Award – reference no. MCCC-RP-14-A17071. The work was supported by NIHR CLAHRC Greater Manchester. The views expressed in this article are those of the author(s) and not necessarily those of the NHS, NIHR or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.