
Abstract
Background:
Spiritual distress is prevalent in advanced disease, but often neglected, resulting in unnecessary suffering. Evidence to inform spiritual care practices in palliative care is limited.
Aim:
To explore spiritual care needs, experiences, preferences and research priorities in an international sample of patients with life-limiting disease and family caregivers.
Design:
Focus group study.
Setting/participants:
Separate patient and caregiver focus groups were conducted at 11 sites in South Africa, Kenya, South Korea, the United States, Canada, the United Kingdom, Belgium, Finland and Poland. Discussions were transcribed, translated into English and analysed thematically.
Results:
A total of 74 patients participated: median age 62 years; 53 had cancer; 48 were women. In total, 71 caregivers participated: median age 61 years; 56 were women. Two-thirds of participants were Christian. Five themes are described: patients’ and caregivers’ spiritual concerns, understanding of spirituality and its role in illness, views and experiences of spiritual care, preferences regarding spiritual care, and research priorities. Participants reported wide-ranging spiritual concerns spanning existential, psychological, religious and social domains. Spirituality supported coping, but could also result in framing illness as punishment. Participants emphasised the need for staff competence in spiritual care. Spiritual care was reportedly lacking, primarily due to staff members’ de-prioritisation and lack of time. Patients’ research priorities included understanding the qualities of human connectedness and fostering these skills in staff. Caregivers’ priorities included staff training, assessment, studying impact, and caregiver’s spiritual care needs.
Conclusion:
To meet patient and caregiver preferences, healthcare providers should be able to address their spiritual concerns. Findings should inform patient- and caregiver-centred spiritual care provision, education and research.
Keywords
Spiritual distress is prevalent among patients with advanced disease and is associated with poor quality of life and increased healthcare costs.
An international survey of palliative care clinicians and researchers identified the need for research into the spiritual care needs, preferences and experiences of patients and their caregivers.
However, the survey did not include patients and caregivers, whose research priorities in spiritual care remain unknown.
Patients and caregivers in nine countries across four continents described many spiritual concerns, but reported spiritual care to be lacking.
Participants’ preferences highlighted the need for all interdisciplinary team members to address spiritual issues.
Patients’ and caregivers’ research priorities included understanding the qualities of human connectedness, communicating sensitively about spirituality, staff education, spiritual care assessment, making spiritual care appropriate for diverse populations, studying the impact of spiritual care, and caregivers’ spiritual care needs.
All staff caring for people with incurable, progressive disease should have a basic level of competency in spiritual care.
Clinical education aimed at improving spiritual care should draw on the findings from this study regarding patient and caregiver needs, experiences and preferences regarding how spiritual care is provided.
Identified research priorities can help ensure future spiritual care research is patient- and caregiver-centred.
Background
Through international consensus, spirituality has been defined as ‘a dynamic and intrinsic aspect of humanity through which persons seek ultimate meaning, purpose, and transcendence, and experience relationship to self, family, others, community, society, nature, and the significant or sacred’. 1 Spiritual distress is suffering related to this dimension of personhood and includes existential components (e.g. meaninglessness and hopelessness) as well as religious concerns. Spiritual distress is prevalent among patients with advanced disease2–4 and is associated with poor quality of life, 5 end-of-life despair, 6 requests for physician-assisted suicide 7 and dissatisfaction with care. 2 Family caregivers report high levels of spiritual distress and unmet needs,8,9 particularly in the context of a life-limiting illness.10–12
Spiritual care, that is, support from healthcare providers that aims to ameliorate spiritual distress, is neglected in clinical practice,2,13–18 with only 6%–28% of patients receiving spiritual care from their healthcare teams.2,5,19,20 This is contrary to patient wishes21,22 and policy guidance internationally.23–25 Evidence suggests that a lack of spiritual support by healthcare teams is associated with poor quality of life, dissatisfaction with care, less hospice utilisation, more aggressive treatment and increased costs, particularly among some ethnic minority groups and patients with high levels of religious coping.5,26–28 Spiritual care specialists such as chaplains (usually, and in the context of this study, a member of the clergy or religious leader) and pastoral care providers, who provide specialist spiritual support but may not be religious, possess advanced training in addressing spiritual concerns. However, it is increasingly recognised that all healthcare providers working with patients with serious illness are responsible for providing basic spiritual care, referring to specialists when needed. Despite this, evidence to inform spiritual care provision and training is limited.29–33 A Northern and Western hemispheric bias is also evident, with most research conducted in the United States and Western Europe. To redress this deficit, an international evidence base is required to guide clinicians in the provision of spiritual care, to ensure patients’ and family members’ support needs are met.
Selman et al. 34 conducted an online survey via the European Association for Palliative Care (EAPC) to identify spiritual care research priorities among palliative care clinicians and researchers (n = 971), and found that understanding spiritual care needs and preferences in multi-faith, multi-cultural populations was a priority area. However, the survey did not consult patients and caregivers regarding their own research priorities in this domain, which is essential if the international research agenda is to be centred on service users’ genuine needs. 1 The goal of this study was to explore patients’ and caregivers’ needs, experiences, preferences and research priorities in spiritual care internationally.
Methods
Study design
This is a qualitative focus group study, conducted in 2013–2014.
Participating sites
The study was conducted across 11 sites in nine countries: South Africa (Cape Town), Kenya (Nairobi), South Korea (Seoul), the United States (San Francisco, New York, Washington), Canada (Calgary), the United Kingdom (London), Belgium (Leuven), Finland (Tampere) and Poland (Poznan). All the sites provided care for patients with incurable, progressive disease, either through community or inpatient services, and had capacity to support the research. We aimed to recruit across a range of countries and regions to produce a broad, descriptive account of patients’ and caregivers’ needs, experiences, preferences and research priorities across diverse settings.
Sampling and recruitment
We aimed to recruit 4–12 participants per focus group, utilising purposive sampling to ensure diversity in diagnoses, age, gender and religion/beliefs where possible. A group of 4–12 was felt to be optimum to generate discussion while remaining manageable. Separate focus groups for patients and caregivers were conducted so that participants had shared experiences of illness/caregiving and would feel able to speak freely. Inclusion criteria for patients were having an incurable, progressive disease and being an adult (18 years or older). Caregivers were adults with experience of caring for someone with incurable, progressive disease. Participants were recruited via one of the clinicians at the site introducing the study, with follow up by the researcher; via posters displayed in participating sites, which informed potential participants of the date of the focus group(s) and how to find out more about the study; and/or via letters of invitation sent to potential participants with a study information sheet. We aimed to achieve data saturation, that is, to collect data until analysis resulted in no new themes emerging. 35
Data collection
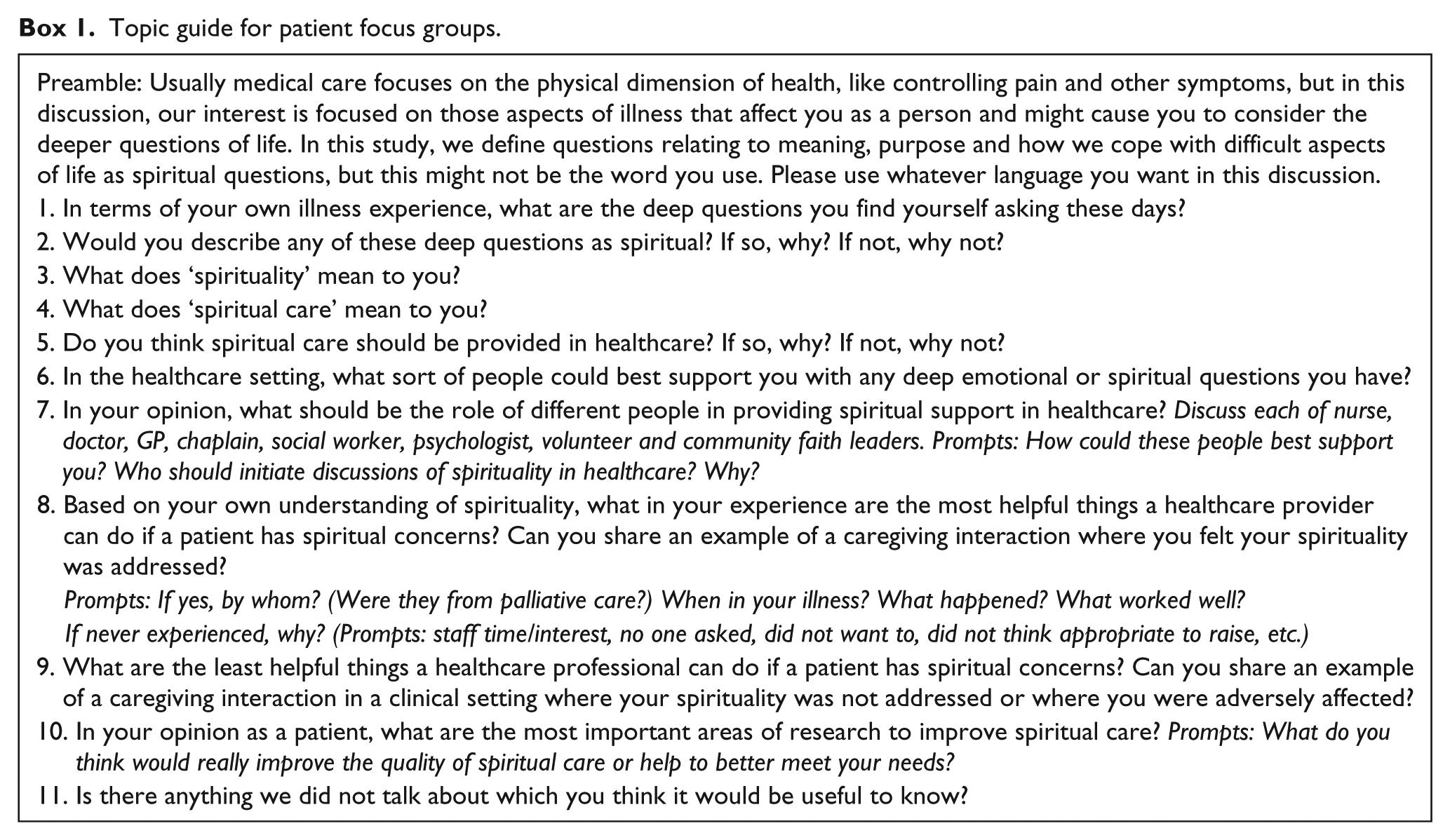
At each site, a researcher with qualitative experience (Appendix 1) conducted two focus groups (one with patients and one with caregivers), following a standardised protocol and training guidelines developed for the study (L.E.S.) based on the literature.36,37 The researchers were known to some participants, but were not involved in their care. An observer took field notes. The semi-structured focus groups followed a topic guide developed on the basis of literature and feedback from the project advisory group (Boxes 1 and 2).
Topic guide for patient focus groups.
Topic guide for caregiver focus groups.
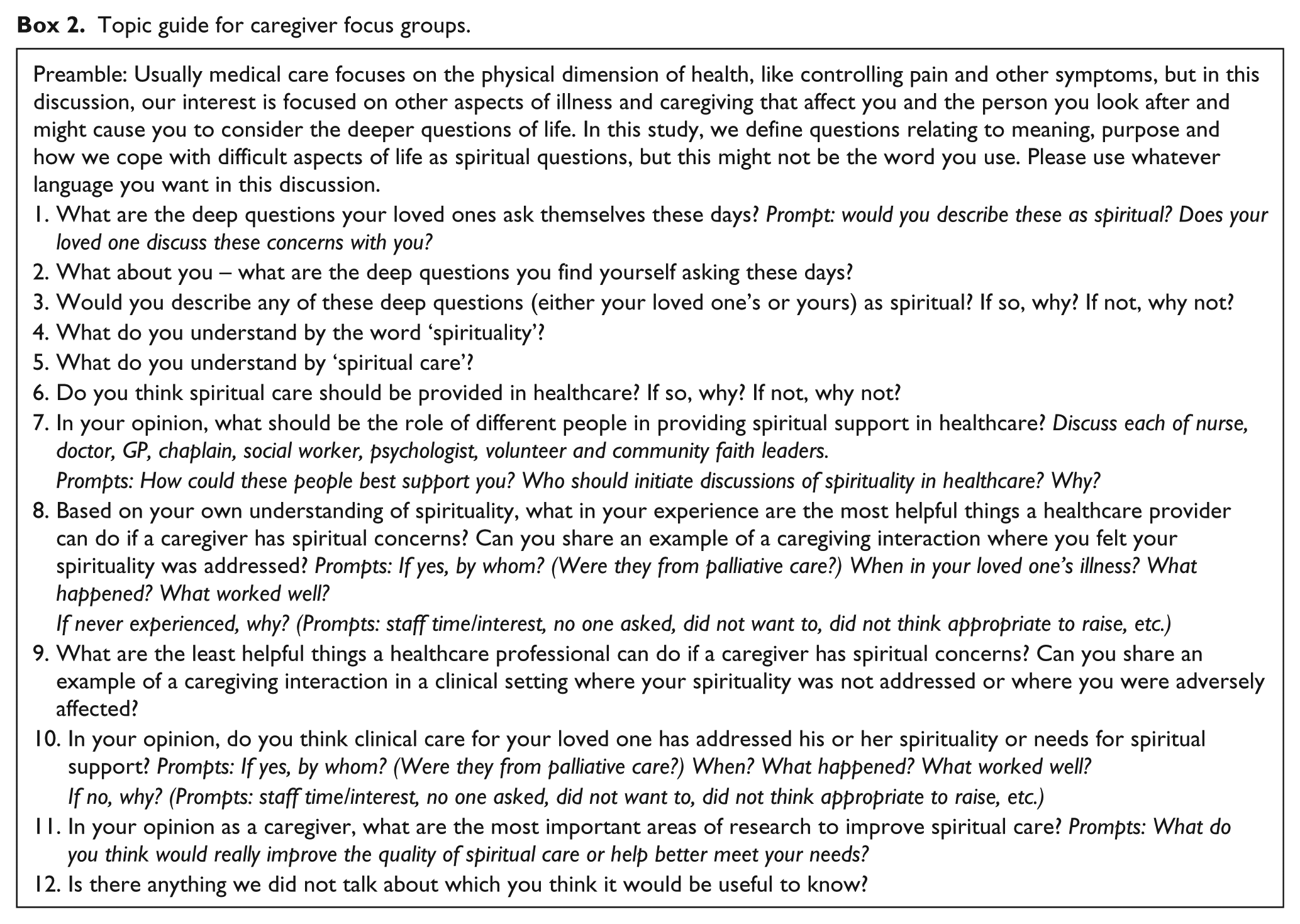
Our research was in the subtle realist paradigm, in which reality is conceptualised as existing objectively, but known only from each individual’s own perspective. 38 This approach, which posits a reality that can be separate from our knowledge of it, is appropriate in qualitative research which aims to accurately describe patient and caregiver experiences and views to inform health service delivery. Data collection was informed by an inclusive definition of spirituality 1 and sought to understand patients’ and caregivers’ own perspectives. We described the research as focusing on ‘those aspects of illness that affect you as a person and might cause you to consider the deeper questions of life’. We defined questions relating to meaning, purpose and how we cope with difficult aspects of life as ‘spiritual’ questions, but encouraged participants to use whatever language resonated with them.
The data collection documents, information sheets and consent forms were translated from English by the research team at each site where necessary. Focus groups were conducted in the most appropriate language for the location and audio-recorded. Prior to analysis, recordings were transcribed and translated into English by professional translators. The research teams at each site verified the translated transcripts against the recordings.
Analysis
Data were analysed thematically 39 in NVivo v10, by qualitative researchers from the United Kingdom, Finland, Canada and New Zealand (L.E.S., L.J.B., S.S., I.K., R.E.). This descriptive methodology was appropriate given the cross-cultural, exploratory nature of the research. 40 Analysis occurred in stages: after familiarisation with the data, two researchers (L.E.S. and S.S. for patient data; L.E.S. and R.E. for caregiver data) independently developed coding frames based on two focus group transcripts each, generating themes and sub-themes inductively from the data as well as deductively from the topic guide. Coding frames were compared and integrated to produce two overall coding frames (for patients and for caregivers), including definitions of themes and sub-themes. The coding frames were applied to the remaining transcripts using line-by-line coding (L.E.S., S.S., R.E., L.J.B., I.K.) and findings aggregated in a narrative, paying attention to non-confirmatory cases and differences between patient and caregiver views and experiences (L.E.S.). Field notes were used to contextualise the data and inform interpretation.
Anonymised data extracts are used in presenting findings (Tables 2–4). These are tagged with a unique ID code and location of the focus group.
Ethical approval
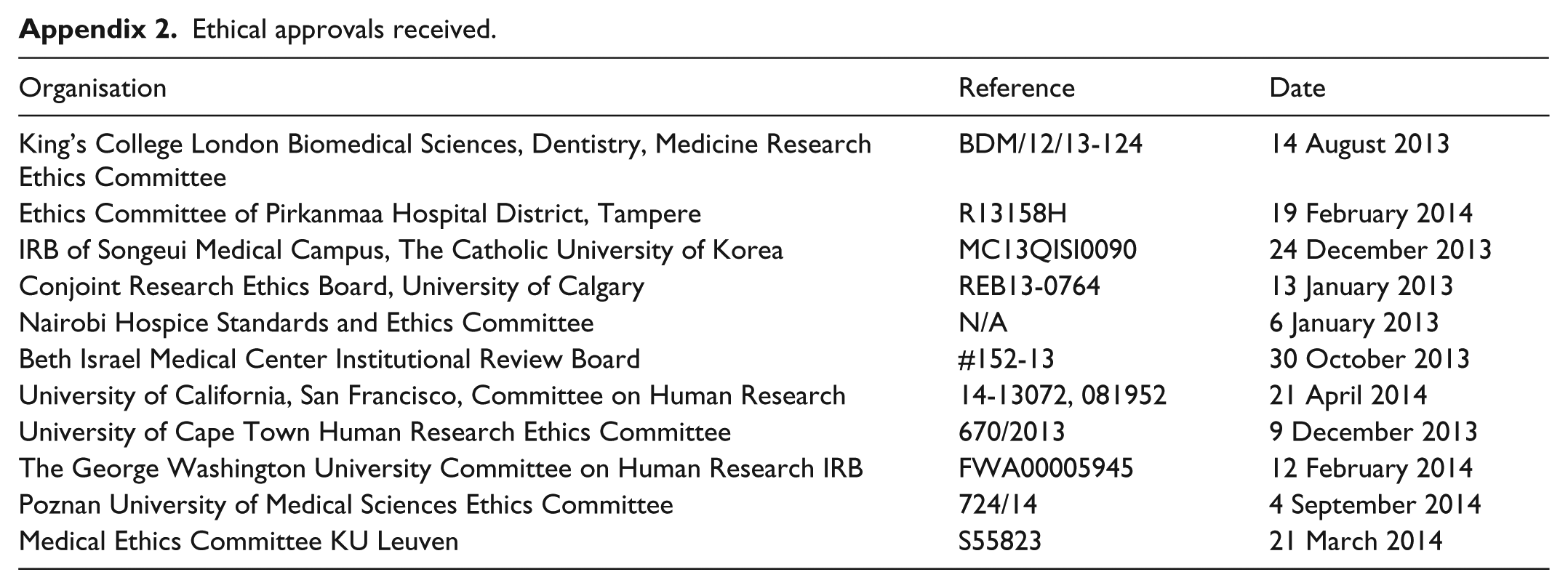
Approval to collect data was obtained from all sites’ local research ethics committees and for the overall study (Appendix 2). All participants gave written, informed consent.
Results
Participant characteristics
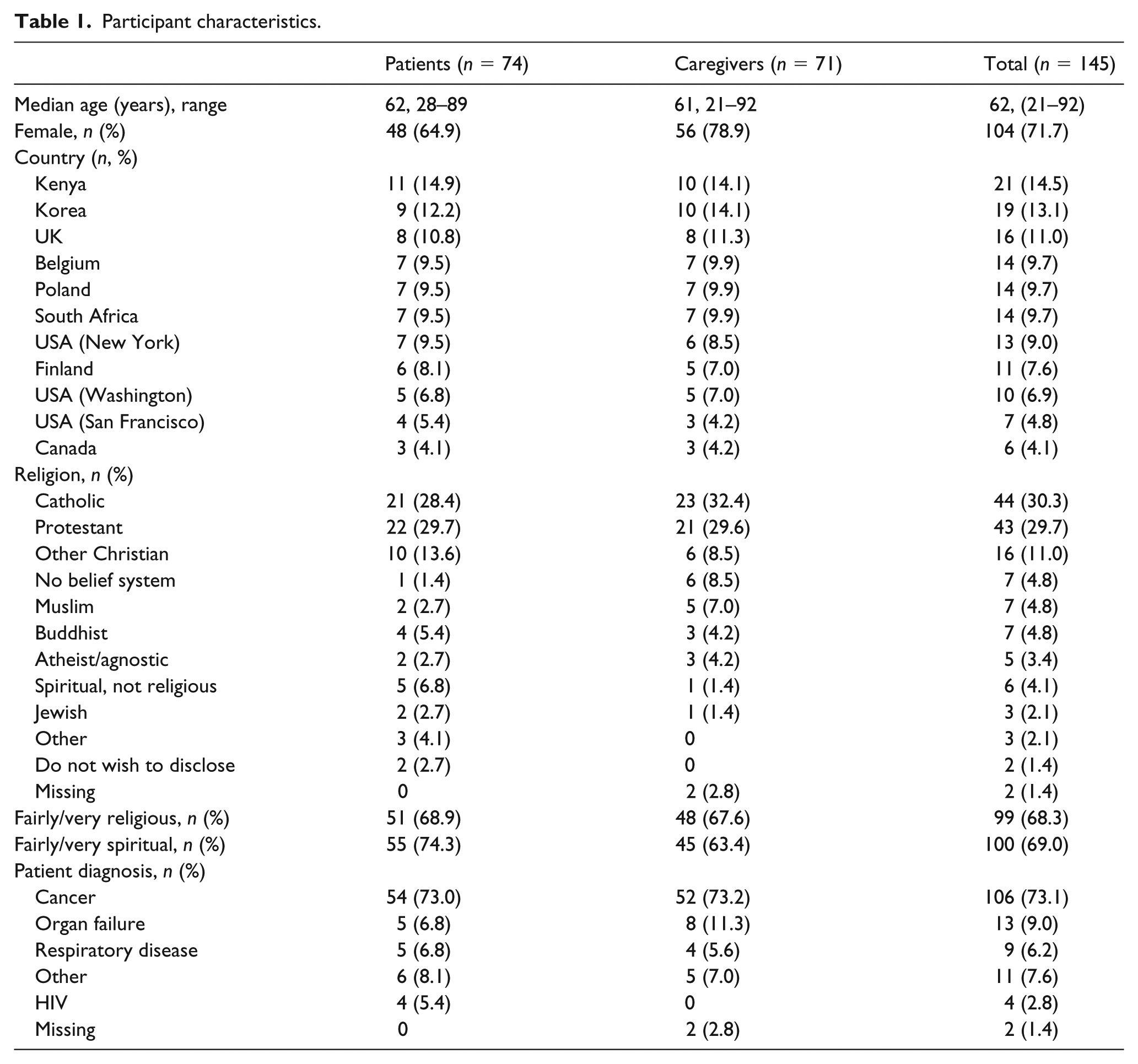
A total of 74 patients and 71 caregivers participated in 22 focus groups ranging 1–2 h (Table 1). Among patients, the median age was 62 years, 48 were women, and 53 had cancer. Caregivers’ median age was 61 years and 56 were women. Two-thirds of participants in both groups identified themselves as Christian, with 68% identifying themselves as fairly to very religious and 69% as fairly to very spiritual. Each focus group lasted approximately 90 min.
Participant characteristics.
Findings
Five themes were identified: patients’ and caregivers’ spiritual concerns, understanding of spirituality and its role in illness, views and experiences of spiritual care, preferences regarding spiritual care, and research priorities. Data saturation was achieved, that is, coding the later transcripts did not result in the identification of new themes in the data.
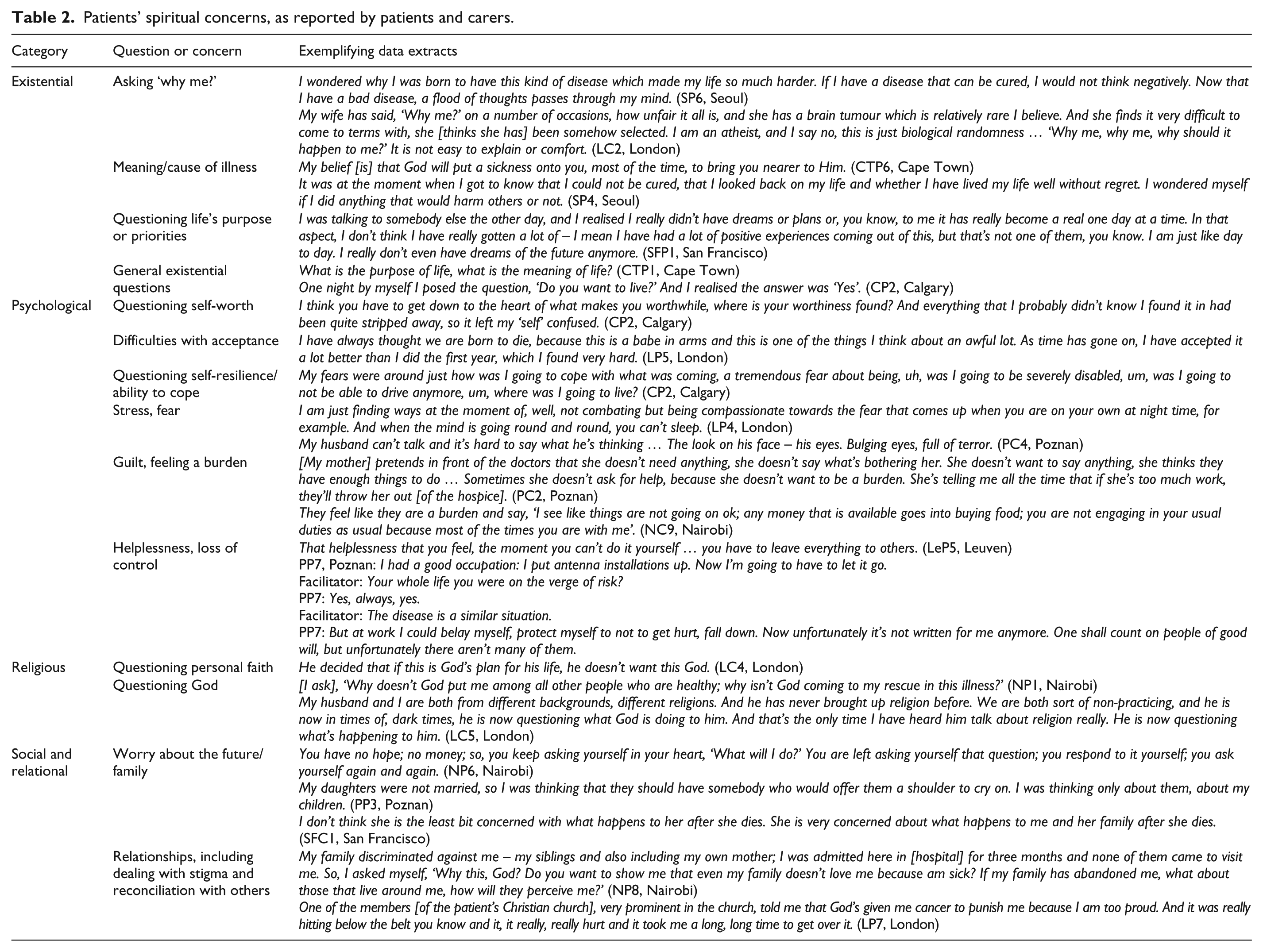
Patients’ and caregivers’ spiritual concerns
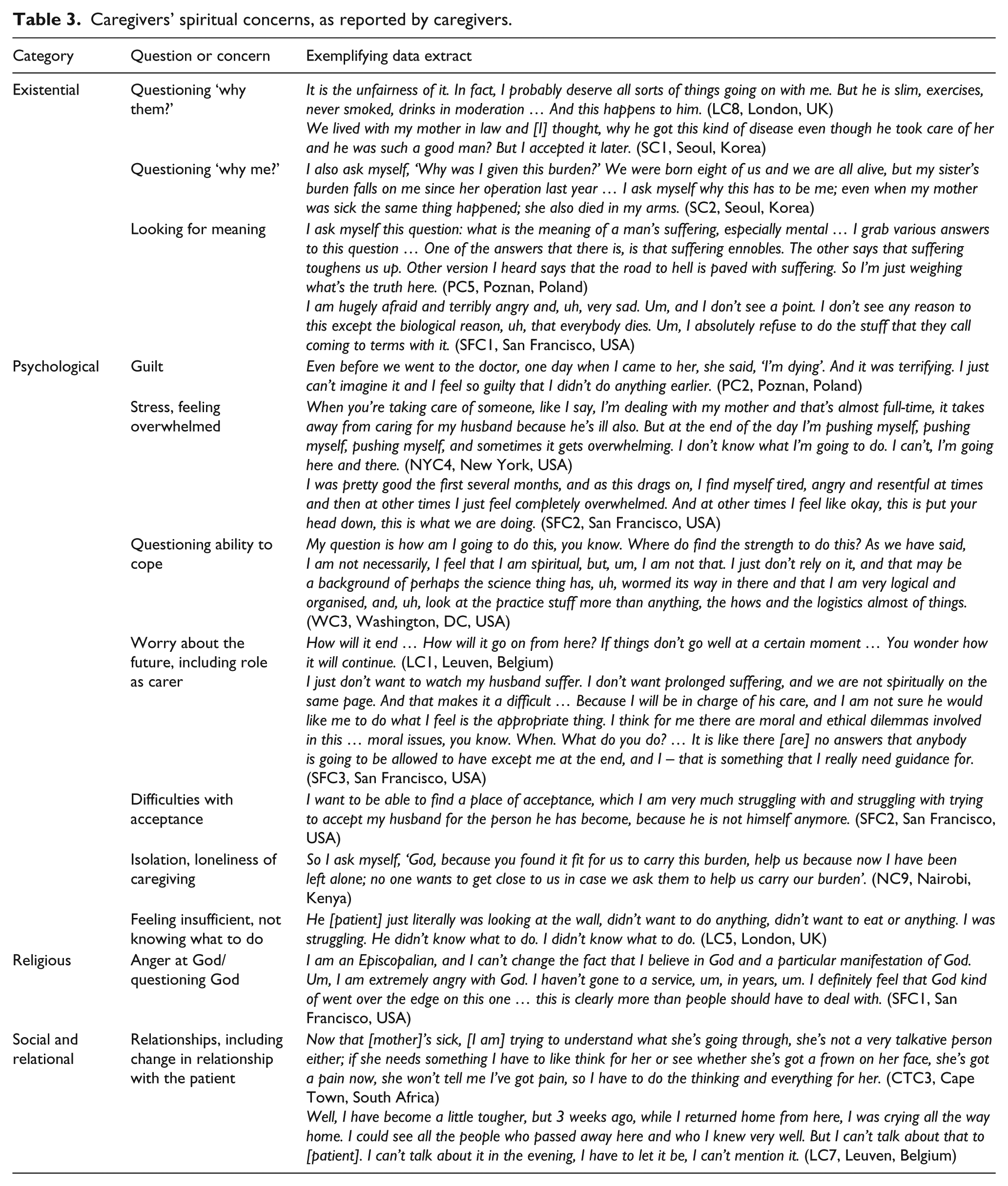
Patients and caregivers were asked to describe and discuss the ‘deeper questions of life’ which arose for patients with advanced disease (Table 2). Caregivers were also asked to describe their own deeper questions (Table 3). A wide range of spiritual questions, problems and concerns were reported, arising in four categories: existential, psychological, religious and social/relational. There was striking similarity across sites in the concerns and problems reported, as demonstrated in the data extracts (Tables 2 and 3), although these were framed differently in different contexts; for example, worry about the future for one’s family was often compounded by economic concerns in Kenya. Four caregivers (from Poznan, Tampere, London and San Francisco) reported that the patient they cared for did not have, or had not expressed, any ‘deeper’ questions (Table 4, Q1).
Patients’ spiritual concerns, as reported by patients and carers.
Caregivers’ spiritual concerns, as reported by caregivers.
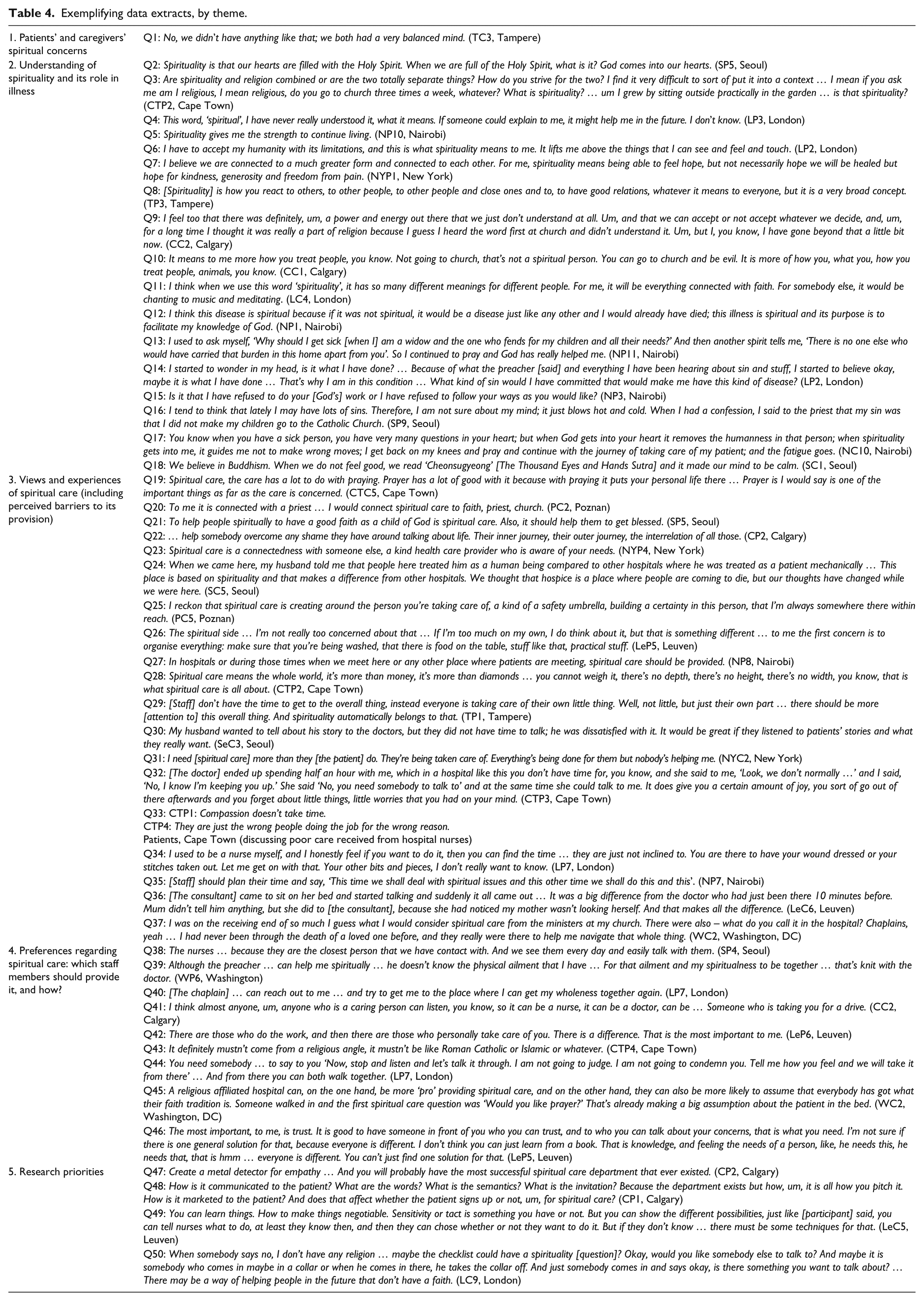
Exemplifying data extracts, by theme.
Understanding of spirituality and its role in illness
Many patients either described a religious conception of spirituality as related to belief in God (Table 4, Q2) or found the concept difficult to understand or define (Q3 and Q4). Others talked about a deeper dimension of life that was a source of transcendence and meaning, and a coping resource (Q5–Q7), or described spirituality in relational terms (Q8). Caregivers largely understood spirituality to be a religious concept, but many also stressed that spirituality was distinct from religion (Q9). Relational conceptions of spirituality were common (Q9 and Q10), as well as the view that spirituality means different things to different people (Q11).
For some patients, illness was inherently spiritual (Q12). Some patients drew upon their spiritual beliefs and were supported by spiritual leaders and faith communities to help them cope with and accept their illness (Q13). Conversely, framing their illness in relation to their beliefs led other patients to blame themselves or their imperfect past behaviour for their current situation (Q14–Q16). Caregivers described how their beliefs, spiritual practices (e.g. meditation, prayer) and support from their faith community helped them cope with their role (Q17 and Q18).
Views and experiences of spiritual care, including perceived barriers
Just as participants’ conceptions of spirituality varied, so did their understandings of spiritual care. Some participants understood it to be essentially religious; for example, in Cape Town and Nairobi, caregivers talked about spiritual care as prayer, while in Poland, caregivers related spiritual care to seeing a priest (Q19 and Q20). Some religious patients saw the primary purpose of spiritual care to be helping them integrate their personal faith into the illness experience (Q21). However, many participants across the sites did not consider spiritual care to be religious care, instead describing it as providing a safe space, listening and counselling. These patients emphasised the role of spiritual care in providing existential support and human connection at a difficult time (Q22 and Q23). Some caregivers understood spiritual care broadly to encompass all care that goes beyond consideration of physical needs. In this sense, they saw palliative care staff as providing spiritual care and their own caregiving as essentially spiritual (Q24 and Q25).
There was some variation across sites regarding the importance patients and caregivers placed on spiritual care; for example, patients and caregivers in Belgium were less likely to see it as a fundamental component of healthcare compared to those in Africa (Q26 and Q27). However, most patients and caregivers across sites agreed that spiritual care was an essential facet of whole person care that should be addressed in healthcare when approaching the end of life (Q28).
Both patients and caregivers reported that spiritual care for patients was lacking (Q29 and Q30). Inadequate spiritual support for caregivers was also noted (Q31). Participants perceived insufficient staff time (Q32) as a barrier to the provision of good spiritual care. However, others suggested that its neglect might have more to do with lack of motivation, prioritisation and/or interest on the parts of healthcare providers (Q33–Q35). Participants generally reported good experiences of spiritual care when received (Q36 and Q37).
Preferences regarding spiritual care: which staff members should provide it, and how?
Patients’ preferences regarding who provides spiritual care varied widely and included doctors, nurses and healthcare assistants, as well as trained spiritual care specialists. Nurses and healthcare assistants were preferred by many, as patients tended to have most contact and familiarity with them (Q38). Physicians were identified as essential in providing spiritual care, due to their relationship with patients and their important role in treating the patient’s illness (Q39). The role of spiritual care specialists was also recognised and valued (Q40). Caregivers emphasised that spiritual care was a responsibility of all staff and appreciated volunteers and peer support (Q41).
Human connection was perceived as a prerequisite to providing effective spiritual care. Patients and caregivers described essential approaches to care that engendered this human connection: putting the patient first, making an extra effort, being reliable and present, and seeing spiritual care as an integral part of care. Additionally, patients felt there were intrapersonal factors or attitudes that predicated a human connection: openness, respect, genuineness, non-judgement, hopefulness, honesty, empathy, kindness and being spiritually aware (Q42–44). Proselytisation and other prescriptive approaches to spiritual care were highlighted as insensitive and inappropriate (Q45). Participants emphasised that spiritual care needed to be individualised and that staff should avoid categorising or stereotyping (Q46).
Research priorities
When asked to consider spiritual care research priorities, patients identified a need to understand the qualities, nature and practice of human connectedness (e.g. compassion, empathy) (Q47). Patients’ other priorities included communicating sensitively about spirituality, particularly in initiating conversations about spiritual care needs (Q48); raising patient awareness of the availability of spiritual care and self-care practices; improving public discussion of death and dying; and how to provide spiritual care within the time constraints of contemporary healthcare. Research that was multi-professional and informed by patients was recommended.
Caregivers emphasised the need to develop educational interventions for staff (Q49); investigate ways to make spiritual care suitable for diverse populations, including those of no religious faith (Q50); improve the assessment of spiritual care needs; study the impact of spiritual care and consider carers’ spiritual care needs, including during bereavement.
Discussion
Main findings
This study provides, for the first time, a picture of patients’ and caregivers’ spiritual concerns, spiritual care experiences and preferences, and priorities in spiritual care research in an international sample. Participants described a wide range of ‘deeper’ concerns that were remarkably common across countries. These concerns were spiritual in the sense of relating to ultimate meaning, purpose, transcendence and relationships to self, others and the significant/sacred. 1 Many concerns were existential, psychological and social/relational in nature rather than overtly religious, although religious distress (related to the content of beliefs and questioning one’s faith) was also evident.
The rich descriptions of spiritual concerns in this study highlight the importance of attending to these in palliative care. However, participants reported a wide-spread neglect of spiritual care needs in practice: spiritual care was needed and felt to be important, but was frequently not addressed by healthcare providers. Participants suggested that the neglect of spiritual care was a matter of prioritisation and staff attitude as much as lack of time. Participants had wide-ranging preferences regarding who provides spiritual care, valuing both specialist and non-specialist spiritual care providers. This suggests that the most appropriate person to provide spiritual support depends on the individual patient or caregiver, as well as the type and severity of distress and the skills of the healthcare professional. Across sites, there were commonalities in the attitudes and approaches perceived as necessary to spiritual care, regardless of who provided it.
Patients emphasised the need for patient-informed multi-disciplinary research into the innate and relational qualities of spiritual care and how to foster them among staff. Their other priorities included communicating sensitively, raising patient awareness of spiritual care and self-care practices, improving public discussion of death and dying and how to provide spiritual care given time limitations. Caregivers highlighted the need to develop educational interventions for staff, make spiritual care suitable for diverse populations, improve assessment, study the impact of spiritual care and consider caregivers’ spiritual care needs, including during bereavement.
Strengths and weaknesses of the study
A strength of the study is that it was informed by an inclusive conceptualisation of spirituality, and participants were encouraged to speak about their deepest concerns and needs in their own language. There is much debate about definitions of spirituality, and adopting an inclusive definition means we captured social and psychological concerns as well as those narrowly conceived of as ‘spiritual’. We believe this reflects the complexity of human experience, which is not easily compartmentalised into ‘spiritual’, ‘social’ and ‘psychological’, and in which relationships are key. 41 Recruiting from nine countries provides an overall picture of patients’ and caregivers’ views, experiences, preferences and priorities internationally, and we achieved data saturation. However, the study was not designed to explore differences in experiences by site or within each country: just two focus groups were conducted at each site, and we did not aim for data saturation at each site. Data should not be taken as representative of the views and experiences of patients and caregivers in that country and cannot result in site- or country-specific recommendations for improving spiritual care. Findings should also not be extrapolated beyond the nine countries involved, as patients and caregivers in other countries might have different experiences and views. A limitation of this study is that we did not have the resources to conduct back translation to check the validity of the translations. However, the local researchers at the sites (who were fluent in English as well as the local language) checked the transcripts for accuracy. Despite our intention to recruit a diverse sample, most participants had cancer and identified as at least fairly religious and Christian, although, as the data extracts show, there was a continuum of secular and religious views. These factors could limit the transferability of findings.
What this study adds
Our findings contribute to the understanding of patients’ and caregivers’ spiritual care needs, preferences and experiences towards the end of life provided by qualitative studies from New Zealand, 3 Australia, 42 Norway, 43 the United Kingdom, 44 the United States,45,46 Taiwan,47,48 Japan 49 and India. 50 We found that patients and caregivers experience a range of existential, psychological, religious and social concerns; these reflect both the existential concerns (e.g. threats to self-identity) emphasised in Henoch and Danielson’s review 51 and the relational concerns that emerged as central in Edwards et al’s 41 review of qualitative literature on understandings of spirituality.
The finding that spiritual care is needed but neglected supports other evidence of a lack of attention to spiritual care needs.2,5,13–20 Participants’ view that lack of time was not the main reason for this neglect echoes Balboni et al.’s study, which found that neither lack of time nor space was associated with spiritual care provision in oncology. Rather, the barriers were inadequate training, clinicians not viewing it as their professional role, and worry that spiritual care is inappropriate due to power inequity between patient and clinician. 52 Other studies have identified additional barriers: lack of expertise and the sense that others could do a better job. 53 Among nurses, higher perceived competence in spiritual care is associated with viewing spirituality/spiritual care broadly, not just in religious terms.54,55 Taken together, these studies suggest specific areas of education to improve spiritual care; for example, deepening practitioner’s self-awareness and self-understanding to help promote human connectedness, and ensuring that spiritual care is understood not purely as religious care. However, changes to organisational culture are also needed to shift practice,56,57 for example, incentivising good spiritual care provision via quality indicators and paying staff for time spent on spiritual care. Our findings support models of palliative care which emphasise that all staff should be comfortable with, and competent to provide, a basic level of spiritual care, with more advanced psycho-spiritual and religious support provided by specialists.58,59 The virtues of openness, authenticity, non-judgement and kindness which patients described have been identified as essential motivators in compassionate care 60 and appear in a conceptual analysis of spiritual care in nursing. 61
Researchers and clinicians in the EAPC survey 34 prioritised research into spiritual care interventions and their effectiveness, overcoming barriers in spiritual care due to staff attitudes, helping staff talk about spiritual issues (e.g. via conversation models), screening and assessment and understanding needs and preferences in multi-faith, multi-cultural populations. These priorities overlap with patients’ prioritisation of communication and how to provide spiritual care, and caregiver’s prioritisation of assessment and impact. However, patients were more focused on understanding the qualities or attributes of spiritual care providers than caregivers and survey respondents. This echoes findings from other studies62–65 and suggests that for patients, the quality of spiritual care depends on the quality of human connection rather than the nature of the intervention itself. Clinicians’ and researchers’ prioritisation of spiritual care interventions rather than attitudes might reflect a professional emphasis on ‘doing’, rather than the ‘being’ 66 often emphasised in spiritual care practice. 65
We found that while individuals are unique in expressions of spirituality, there are commonalities that can serve as pillars for ongoing international collaboration to improve spiritual care (e.g. The Global Network for Spirituality & Health 67 ). Findings suggest that training staff and volunteers in spiritual care provision in palliative care must become an international priority. They also provide a framework for future research, providing the service user counterpart to the research priorities previously identified. 34 Further research is needed to explore cultural differences in service users’ experiences and preferences and identify models of spiritual care that are culturally sensitive and locally appropriate.
Conclusion
Our findings provide evidence that spiritual care is an essential but neglected component of care, according to patients and their caregivers across a range of countries. Participants described human connection, person-centredness and integration in healthcare as fundamental to spiritual care. While spiritual care specialists play important roles, including staff support, participants emphasised the importance of spiritual care competency across disciplines. The priorities identified here should be used to guide future spiritual care research and clinical and educational initiatives.
Footnotes
Appendix
Ethical approvals received.
| Organisation | Reference | Date |
|---|---|---|
| King’s College London Biomedical Sciences, Dentistry, Medicine Research Ethics Committee | BDM/12/13-124 | 14 August 2013 |
| Ethics Committee of Pirkanmaa Hospital District, Tampere | R13158H | 19 February 2014 |
| IRB of Songeui Medical Campus, The Catholic University of Korea | MC13QISI0090 | 24 December 2013 |
| Conjoint Research Ethics Board, University of Calgary | REB13-0764 | 13 January 2013 |
| Nairobi Hospice Standards and Ethics Committee | N/A | 6 January 2013 |
| Beth Israel Medical Center Institutional Review Board | #152-13 | 30 October 2013 |
| University of California, San Francisco, Committee on Human Research | 14-13072, 081952 | 21 April 2014 |
| University of Cape Town Human Research Ethics Committee | 670/2013 | 9 December 2013 |
| The George Washington University Committee on Human Research IRB | FWA00005945 | 12 February 2014 |
| Poznan University of Medical Sciences Ethics Committee | 724/14 | 4 September 2014 |
| Medical Ethics Committee KU Leuven | S55823 | 21 March 2014 |
Acknowledgements
The authors would like to thank all the patients and caregivers who participated, the staff at the participating sites, Suzanne O’Brien for data entry and analysis and members of the Project Advisory Group. The InSpirit collaborative includes the co-authors and the following collaborators: Mieke Vermandere, Liz Gwyther, Clint Cupido, George Handzo, Andrew Goodhead, Aquinas Nyakundi, Julianna (Jinsun) Yong, Imsun Seo, Katarzyna Stachnik, Yvette Coulter and Najmeh Jafari. L.E.S. obtained funding, designed and coordinated the study, led data analysis, drafted the manuscript and takes responsibility for the content. L.J.B. assisted with data analysis, administration and drafting of the paper. S.S., I.K. and R.E. contributed to the design of the study and assisted with data analysis. S.S., I.K., P.S., R.A.P., E.D.-S., M.G., S.A., C.P., J.H. and N.G. contributed to data collection. P.S. also obtained funding. J.H. was a patient representative on the Project Advisory Group. All authors contributed to the intellectual content of the manuscript and have approved the final version.
Data sharing
Requests to access anonymised transcripts should be directed to the corresponding author (L.S.).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics and consent
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: They thank the Sir Halley Stewart Trust and the University of Cape Town for contributing to the research costs.