
Abstract
Background:
Population ageing represents a global challenge for future end-of-life care. Given new trends in place of death, it is vital to examine where the rising number of deaths will occur in future years and implications for health and social care.
Aim:
To project where people will die from 2015 to 2040 across all care settings in England and Wales.
Design:
Population-based trend analysis and projections using simple linear modelling. Age- and gender-specific proportions of deaths in hospital, care home, home, hospice and ‘other’ were applied to numbers of expected future deaths.
Setting/population:
All deaths (2004–2014) from death registration data and predicted deaths (2015–2040) from official population forecasts in England and Wales.
Results:
Annual deaths are projected to increase from 501,424 in 2014 (38.8% aged 85 years and over) to 635,814 in 2040 (53.6% aged 85 years and over). Between 2004 and 2014, proportions of home and care home deaths increased (18.3%–22.9% and 16.7%– 21.2%) while hospital deaths declined (57.9%–48.1%). If current trends continue, numbers of deaths in care homes and homes will increase by 108.1% and 88.6%, with care home the most common place of death by 2040. If care home capacity does not expand and additional deaths occur in hospital, hospital deaths will start rising by 2023.
Conclusion:
To sustain current trends, end-of-life care provision in care homes and the community needs to double by 2040. An infrastructure across care settings that supports rising annual deaths is urgently needed; otherwise, hospital deaths will increase.
Population ageing is a global phenomenon with challenges for the future provision of health and social care.
The majority of people prefer to die in their usual place of care.
There has been a recent rise in the number of deaths at home and fall in deaths in hospital.
If the recent decline in hospital deaths is sustained, by 2040 the annual numbers of people dying at home and in care homes will almost double and care home will become the most common place of death.
If there is no expansion of capacity and end-of-life care training for staff in care homes and in home care services, the trend in declining hospital deaths will likely reverse by 2023.
We urgently need a policy response that strategically plans for the future increased need for end-of-life care across all care settings.
The development of new models of care to support increasing numbers of people at the end of life is imperative.
This study provides a clear analysis model for projecting place of death that can be replicated internationally.
Introduction
The numbers of deaths worldwide are set to rise from 57 million in 2015 to 70 million in the next 15 years. 1 People are living to older ages, and patterns of death and disease are changing. Non-communicable diseases accounted for over two-thirds of all global deaths in 2012 2 and their prevalence is expected to increase in the future. 3 As in other rapidly ageing nations, the impact of population ageing in England and Wales will become increasingly evident in the next few decades. There is an urgent need to plan ahead to ensure we meet the healthcare needs of our population in the future.
A robust understanding of where people die is vital to support health policies, resource allocation and service delivery, for example, to support the planning and commissioning of palliative care services. Place of death is considered a marker of quality, because it is related to quality of life and bereavement outcomes.4,5 It also indicates the extent to which care meets people’s preferences at the end of life, since most people prefer to die at home or in their usual place of living and care. 6 Knowledge of where people are likely to die is an important indicator of where pressures in the health system may occur in future years. It also points to priority areas for education and training to ensure our current and future workforce can provide care that enables people with advanced conditions to live well and die peacefully where they wish to be.
A previous study by Gomes and Higginson 7 projected future trends in home and institutional deaths from 2004 to 2030 in England and Wales, based on trends from 1999 to 2003. This study guided subsequent end-of-life care policies, such as the End of Life Care Strategy (2008), 8 which successfully raised the profile of end-of-life care and influenced practice. 9 The long-standing trend of declining home deaths described by Gomes and Higginson 7 has subsequently slowed and even reversed.10,11 Alongside these policy changes and new trends in place of death, population ageing has increased. 12 Thus, it is timely and vital to provide new projections of where people will die in the future to inform health and social care policy and planning. This study builds on the work by Gomes and Higginson by extending the projections by 10 years and examining settings that are important providers of end-of-life care but not previously explored, namely care homes and hospices. This study aims to project where people in England and Wales will die from 2015 to 2040 across all care settings and examine implications for end-of-life care provision.
Methods
Design
Population-based trend analysis using simple linear modelling and explicit assumptions to project where people will die in England and Wales based on recent death registration data (2004–2014).
Data sources
We used publicly available datasets provided by the Office for National Statistics (ONS). First, the ONS supplied death registration data on all registered deaths by place of occurrence in England and Wales from 2004 to 2014.12,13 Second, mid-year forecasts for future population and deaths in England and Wales were obtained. 14
Place of death data
Our primary outcome was place of death. Death registration is a legal requirement and a widely recognised and accepted data source for measuring place of death.11,15 Death registration data in England and Wales is considered to be of high quality. 16 We were supplied with anonymous information for all deaths registered within each calendar year between 2004 and 2014. We used place of death categories defined according to a revised classification (2010; applied retrospectively to years 2004–2009 by the ONS on request): (1) home, (2) care home (local authority and non-local authority), (3) hospital (National Health Service (NHS) and non-NHS), (4) hospice, (5) other communal establishments and (6) elsewhere. Deaths at home were those at the usual residence of the deceased, where this was not a communal establishment. ‘Other communal establishments’ included schools, hotels and prisons, while ‘elsewhere’ referred to motorways, the street and other public spaces. We combined the categories ‘other communal establishments’ and ‘elsewhere’, referred to as ‘other’ hereafter. Place of death information was provided by the informant of death, who is usually a relative of the deceased. All data were stratified by age and gender, using the seven ONS standard age groups (up to 4, 5–14, 15–44, 45–64, 65–74, 75–84, 85 and over years). The first three categories were collapsed for presentation of findings.
Forecast population data
The ONS provides several population forecasts using estimates of mid-year population, according to a range of explicit assumptions about future fertility, life expectancy and migration patterns. Forecast deaths are provided for each age year and by gender. We used the ‘principal’ forecasts as it is widely used by local authorities and commissioners for resource allocation and planning. Methods for forecasts are provided elsewhere. 17
Data analysis
We projected place of death for all deaths forecast to occur in England and Wales up to 2040 using age- and gender-specific proportions in each place of death from 2004 to 2014 and applying these to the age- and gender-specific numbers of future deaths forecast by ONS. Where projected numbers became negative (for categories that had a small number of deaths), we fixed the value at zero. We produced three projection scenarios with explicit assumptions. For each scenario, the total number of projected deaths across all care settings was compared against the total number of forecast deaths provided by the ONS to examine the margin of error. All analyses were conducted in Excel.
Scenario 1 assumed that the proportions of deaths occurring in each care setting in 2014 will remain unchanged over time. The age- and gender-specific proportions in each place of death for 2014 were applied to the forecast numbers of deaths in each consecutive year until 2040 to obtain the projected number of deaths occurring in each care setting. Scenario 2 assumed that the average trend in place of death in the last 11 years (2004–2014) will continue linearly until 2040. For this scenario, we calculated annual percentage changes in age- and gender-specific proportions of deaths for each of the five care setting categories separately. Mean annual percentage changes in the 11 year period were assumed to continue for each subsequent year and these proportions were applied to the age and gender distribution of the forecast deaths in future years.
Scenario 3 followed the same assumptions as Scenario 2; however, it additionally assumed that the maximum capacity of care homes was reached in 2014. It was assumed that the absolute number of deaths that are to occur in care homes in the future could not exceed those observed in 2014. This scenario was explored as there have been a number of care home closures in recent years. 18 People admitted to care homes have complex needs with a combination of disability, frailty, multiple long-term conditions and cognitive impairment. 19 Therefore, any additional deaths were assumed to occur in hospital and so were subtracted from the care home category and added to the hospital category in each future year.
Ethics
This study uses routinely collected aggregated and anonymised data that are publicly available; therefore, no ethical approvals were necessary.
Results
Recent trends in place of death
The previously reported trends in place of death in England and Wales from 2004 to 2010 have since continued in the same direction (Table 1 and Figure A in supplementary material). Between 2004 and 2014, there have been increases in the proportion of deaths occurring at home and in care homes (18.3%–22.9% and 16.7%–21.2%, respectively). Hospice deaths also increased slightly but remained the place of death for a small minority (4.6% in 2004 to 5.5% in 2014). In contrast to community-based deaths, the proportion of hospital deaths declined during the 11-year period (57.9%–48.1%) and fell below 50% in 2012, meaning that the majority of people no longer die in hospital. Deaths elsewhere declined from 2.5% to 2.3% between 2004 and 2014.
Number and proportion of deaths occurring in each setting 2004–2014.
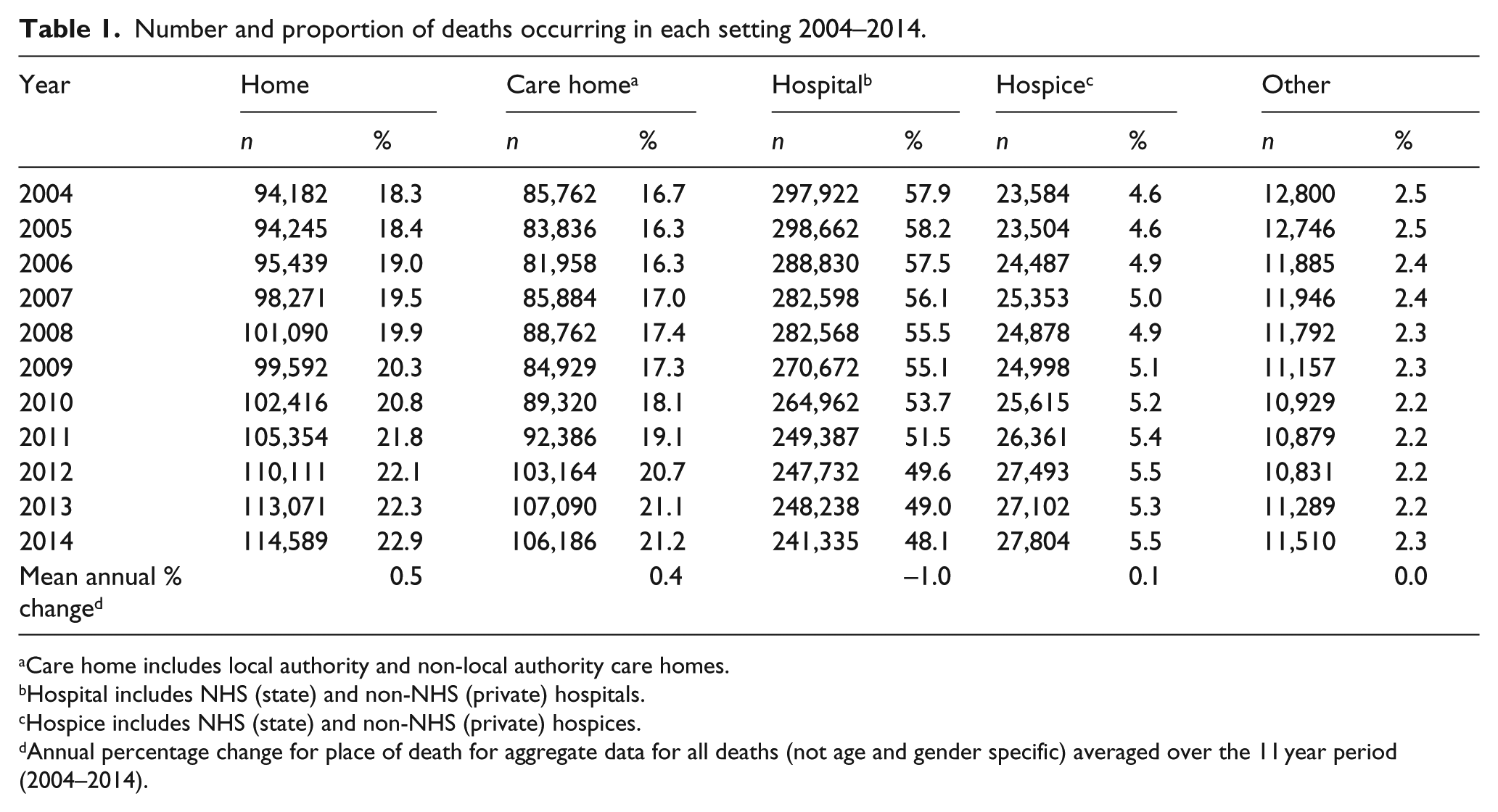
Care home includes local authority and non-local authority care homes.
Hospital includes NHS (state) and non-NHS (private) hospitals.
Hospice includes NHS (state) and non-NHS (private) hospices.
Annual percentage change for place of death for aggregate data for all deaths (not age and gender specific) averaged over the 11 year period (2004–2014).
Projections of deaths by age and gender
The ONS projects that the population of England and Wales will increase from over 57 million in 2014 to over 66 million in 2040 (16.4% increase). Figure 1 shows the projected numbers of deaths by age and gender. Overall, the number of deaths is projected to increase by 27.0% from 501,424 in 2014 to 635,814 in 2040. In 2014, 83.9% of all deaths occurred in people aged 65 years and over, and this is projected to increase to 90.9% in 2040. Most striking is the 75.3% increase in deaths for the 85 and over age group, with a higher increase for men within this age group (111.8% increase compared to 53.4% for women). In 2014, 38.8 % of all deaths occurred in people aged 85 years and over, and this percentage is projected to increase to 53.6% in 2040.
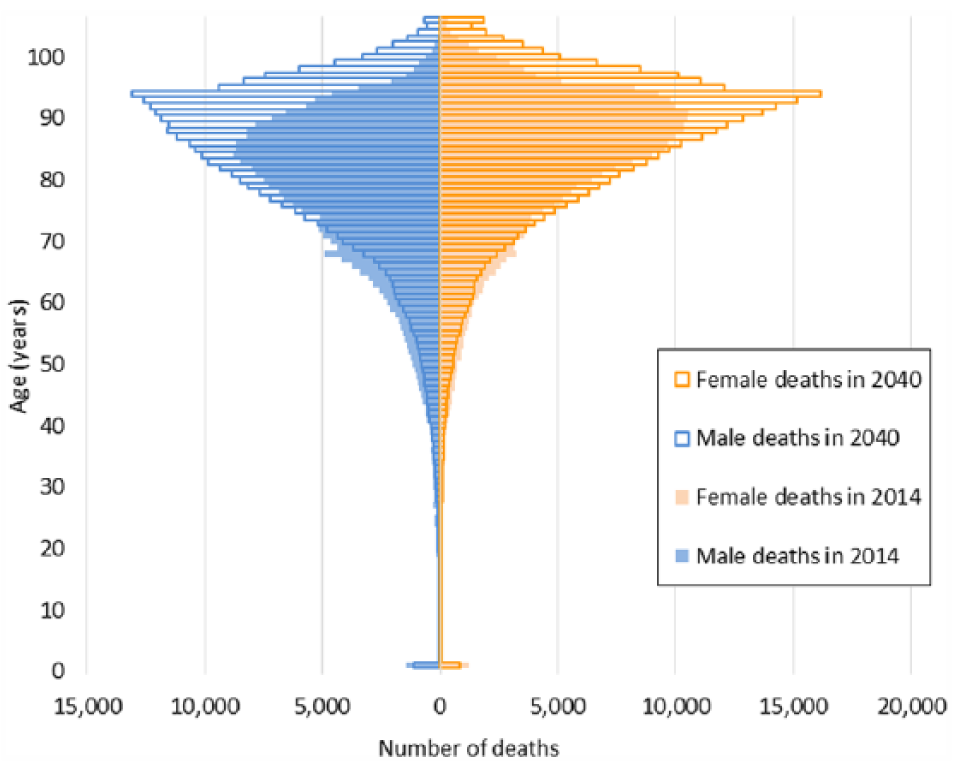
Actual and projected deaths in 2014 and 2040 by age and gender.
Projections of deaths by place of occurrence
Figure 2 (and Table A in supplementary material) displays where people might die in future years according to the three scenarios. The margin of error for the total deaths in 2040 projected using recent trends (Scenarios 2 and 3) compared with the ONS forecast total deaths was minimal at 0.17%. There was no margin of error for Scenario 1 due to the application of fixed proportions.
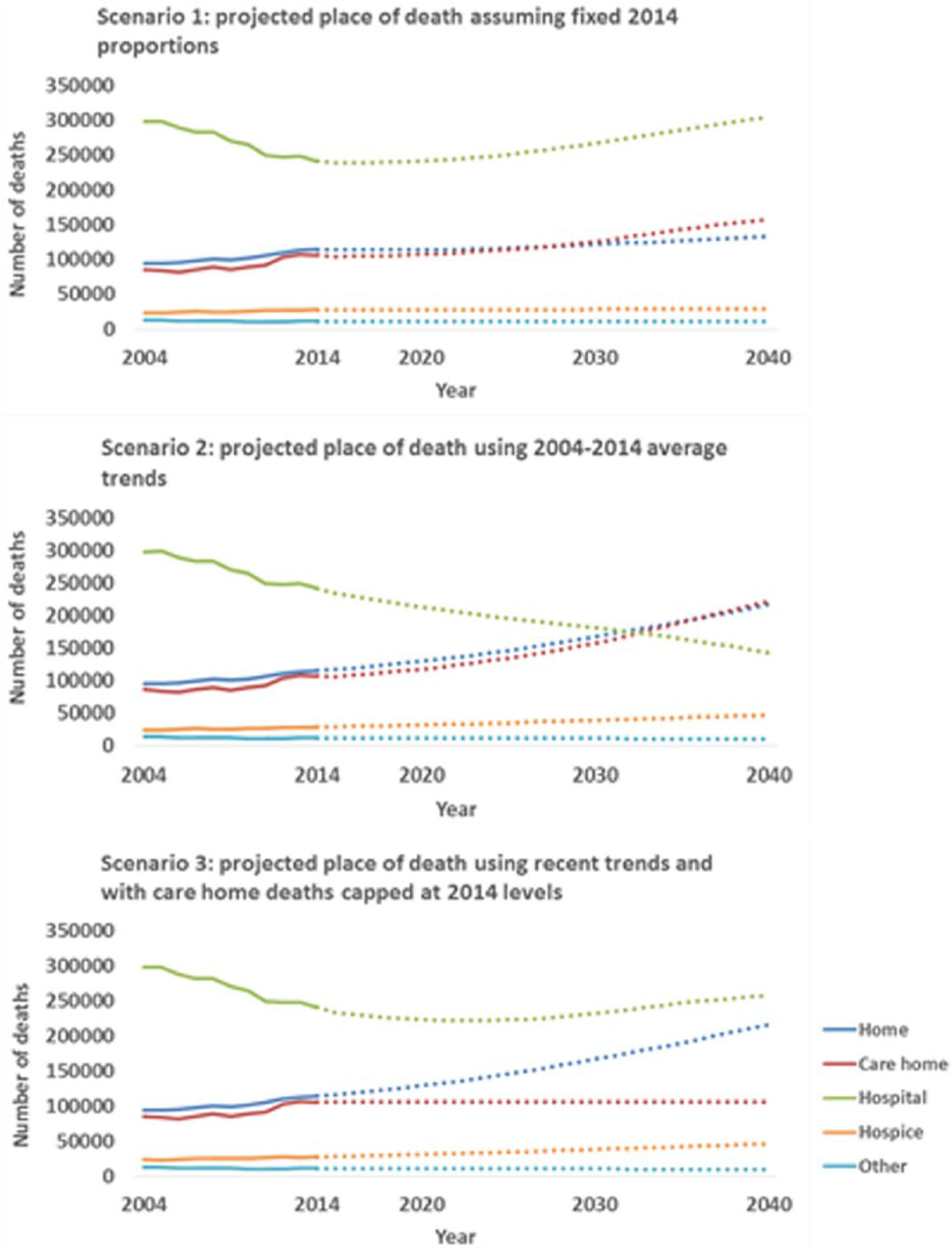
Actual (2004–2014) and projected (2015–2040) numbers of deaths in each setting in England and Wales.
Scenario 1
As the age- and gender-specific proportions of deaths in each care setting are assumed to be static in Scenario 1, the trends observed are driven by the projected demographic changes. In this scenario, the numbers of deaths in hospital are projected to increase over future years, even though the proportions remain the same. By 2027, the number of people dying in care homes is projected to exceed the number of people dying at home. Unlike in other care settings, the number of people dying in hospices is projected to remain stable over time until 2040.
Scenario 2
Projections using the past 11-year average change (Scenario 2) show increasing home, care home and hospice deaths and decreasing hospital deaths (Tables B and C in supplementary material show findings by age and gender). According to this scenario, by 2040 68.6% of all deaths will occur in a care home or at home (220,952 and 216,110 deaths, respectively), with about a third in each care setting (34.7% in care homes and 34.0% at home). Hospice deaths are projected to increase from 27,804 (5.5%) in 2014 to 46,690 (7.3%) in 2040. While hospice would remain the place of death for a minority, care homes and home would both become more common settings for death than hospital by 2040, which is projected to decline from 241,335 deaths (48.1% of all deaths) in 2014 to 142,543 deaths in 2040 (22.4% of all deaths).
Scenario 3
The third scenario illustrates the possible impact of care homes reaching capacity if additional care home deaths occur instead in hospital settings. In this scenario, the number of deaths at home, in hospices and in other settings are the same as for Scenario 2. However, the pattern for hospital deaths looks markedly different if care home capacity does not increase beyond the level observed in 2014 (106,186 deaths). In this scenario, hospital deaths will continue to decline until 2023 when the trend reverses. By 2040, hospital deaths would have increased to 257,308 (40.5%).
Discussion
Our projections show that if current trends continue, the need for end-of-life care will rise substantially over the next 25 years, particularly at home and in care homes. The recent trends of increasing deaths in usual place of care are in line with the population’s preferences,6,20,21 indicating an improvement in end-of-life care provision. If current trends continue, deaths in care homes, homes and hospices will almost double by 2040, which will account for 76.0% of all deaths. Care home deaths are projected to become the most common place of death by 2040. However, if care home capacity does not increase and these additional deaths instead occur in hospital, the decline in hospital deaths will reverse by 2023, rising to 40.5% of all deaths by 2040. New approaches to caring for people at the end of life will need to be considered. If people are to be supported to die outside hospital, input from the NHS, social care and the voluntary sector as well as families and friends will be required. While these results relate to the population of England and Wales, there are clear parallels with other nations experiencing similar patterns of population ageing in future decades. 22
Our projections suggest that care homes will become increasingly important settings for end-of-life care, corroborating findings from similar studies in Belgium and France.23,24 Therefore, new approaches to care homes must be considered and can be informed by alternative models seen elsewhere. For example, ‘nursing home medicine’, which is recognised as a medical speciality in the Netherlands, 25 and the ‘teaching nursing home’ model developed in Australia. 26 However, if care home capacity declines, it is likely that hospital deaths will rise, as has been observed in Portugal. 27 It is concerning that there are many examples of care homes closing for economic reasons. If the trend of declining hospital deaths reverses, there will also be a greater imperative to examine alternative models of hospital care, such as hospice wards and units within the hospital, which have been implemented in the United States 28 and elsewhere. 29
The rise in numbers of people dying in community settings with complex care needs, such as those associated with multi-morbidity and frailty,30,31 present additional challenges for care provision. For example, palliative care need is projected to increase by 42% by 2040, increasing out of proportion to deaths. 32 Palliative care delivered by specialists has been shown to improve outcomes for patients and family carers. 33 However, only a minority of people receive specialist palliative care at the end of life, 34 and access is more common for people with cancer compared to non-cancer conditions, despite similar needs.35,36 How to identify people who could benefit from palliative care 37 and improve its coverage to an increasing target population in community settings is a key challenge of the next few decades. This requires improved integration of palliative care into primary care in future years. 38 These are areas of research and clinical care that require urgent attention.
As the number of people needing end-of-life care rises, consideration of the resilience, capacity 39 and training of the health and social care workforce is of growing importance, particularly in the community. If current trends continue and care homes become the most common place of death, it is vital that care home staff are adequately trained to deliver good quality care towards the end of life. While training in palliative care and end-of-life care is improving across health professions, 40 it is variable and often inadequate. 41 Palliative care and end-of-life care should be embedded into training curricula for all health professionals. New innovative partnership methods of delivering palliative care training, particularly in community settings, are required. The ECHO (Extension for Community Healthcare Outcomes) model of teleconferencing medical education and care management developed in the United States has been piloted in the palliative care setting in Northern Ireland, with positive early findings. 42 Research to evaluate education and training programmes in palliative care and end-of-life care is needed to support best practice.
Strengths and limitations
This study provides new national projections for where people will die, using simple methods to provide clear and interpretable projections, not deterministic forecasts. Previous projections guided policy changes by warning about what would happen in the future, which in turn effected significant change in place of death. New projections are therefore timely. We expanded the analysis to include deaths in care homes and hospices, which are important settings for end-of-life care provision. This is a strength of this study, as there is interdependence between settings. 43 There are however limitations relating to the assumptions made in the modelling. For Scenarios 2 and 3, we assumed linear change over time, which is an oversimplification, although recent trends do show approximately linear change over time. The assumption for Scenario 3 that care homes reach capacity in 2014, and care home deaths cannot therefore increase, is also an oversimplification. If length of stay prior to death reduces, then care home deaths could increase at constant bed capacity, as has been observed in Sweden. 44 However, the expected growth in the older population living with long-term functional dependence 45 means that it is reasonable to assume that care home duration is not likely to decrease in the future.
Despite trends of decreasing number of hospital deaths, hospital admission at the end of life is high and increases markedly at the end of life.46,47 Understanding the concurrent trends of planned and unplanned hospital use prior to the end of life is important in terms of resource use, and quality of end-of-life care, but was beyond the scope of this study. Evidence on the comparative quality of care between care settings is sparse, particularly for older people with non-cancer conditions, 48 and this work does not shed light on this aspect. These are important considerations for planning the future delivery of end-of-life care for growing numbers and require further investigation. However, this study provides a clear population-based analysis model to be replicated in nations in which death registration data are routinely collected and forecasts of future mortality are available.
Conclusion
These projections show that there will be substantial increases in deaths at home and in care homes over the next 25 years, if current trends continue, putting significant pressure on community services. If the reduction of deaths in hospital is to be sustained, there is an urgent need to expand the number of care home places and invest in community services and social care. If care home capacity does not increase or alternative approaches developed, the projected reduction of deaths in hospital will reverse, and demands on hospitals to provide end-of-life care will escalate. An urgent policy decision and strategic response to these imminent challenges is required to ensure that there is adequate infrastructure across settings to provide high quality care to people reaching the end of their life in future years.
Footnotes
Acknowledgements
The authors thank the Office for National Statistics (ONS) for supplying the data. Special thanks to Laura Todd from the ONS for assistance and advice in preparing the data for analysis. I.J.H. and B.G. conceived of the study concept. A.E.B. initiated the study, led the statistical analysis and drafted the paper. I.J.H., C.J.E., F.E.M., B.G., J.V., S.N.E. and A.E.B. developed the study design and participated in interpretation of data. All authors critically revised the paper for important intellectual content and approved the final version to be published. I.J.H. and C.J.E. supervised the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work is independent research funded by Cicely Saunders International and The Atlantic Philanthropies (grant number 24610). This research was supported by the Collaboration for Leadership in Applied Health Research and Care (CLAHRC) South London, which is part of the National Institute for Health Research (NIHR), and is a partnership between King’s Health Partners, St. George’s, University London and St George’s Healthcare NHS Trust. I.J.H. is an NIHR Senior Investigator. C.J.E. is funded by a Health Education England (HEE)/NIHR Senior Clinical Lectureship. B.G. is funded by the Calouste Gulbenkian Foundation. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.