
Abstract
Background:
Children and infants with impaired swallow or compromised enteral absorption require alternative routes for administration of analgesia. Recent clinical guidance and practice for paediatric palliative care teams, who often treat such children, supports buccal morphine sulphate as a fast acting, effective and easily administered agent for pain relief. However, a consideration of the physicochemical properties and potency of morphine would suggest that it is not a suitable candidate for delivery via the transmucosal route, raising questions about its use in children and infants.
Aim:
To explore the permeability of buccal morphine sulphate in an established ex vivo porcine buccal mucosa as a necessary step in examining efficacy for use in children with life-limiting conditions and life-threatening illnesses.
Design:
A permeation study conducted with morphine sulphate in an ex vivo porcine buccal tissue model. Flux values and pharmacokinetic data were used to calculate the plasma values of morphine that would result following buccal administration in a 20kg child.
Results:
Results show that the estimated steady state plasma values of morphine sulphate following buccal administration in this model do not achieve minimum therapeutic concentration.
Conclusion:
These data strongly suggest that morphine sulphate is not suitable for buccal administration and that further research is needed to establish its efficacy in relief of pain in children with life-limiting conditions and life-threatening illnesses.
Palliative care teams often treat children with impaired swallow or reduced enteral absorption.
Recent surveys of clinicians working in paediatric palliative care have identified the prescribing of buccal morphine sulphate (MS) as a fast acting and easily administered agent for pain relief.
Prior consideration of the physicochemical properties and potency of morphine indicate it is not a suitable candidate for delivery via the transmucosal route.
A permeation study conducted with MS in an established ex vivo porcine buccal tissue model generating buccal absorption data which are extrapolated to plasma values based on the pharmacokinetics of morphine in children.
Results confirm that the estimated steady state plasma values of MS following buccal administration in this model do not achieve minimum therapeutic values.
These findings as well as those in the literature suggest careful consideration before using buccal morphine to treat pain in children with life-limiting and life-threatening conditions.
Introduction
Managing pain in children in the palliative care setting can be challenging due to limitations in routes of administration and lack of appropriate formulations. The oral transmucosal route of administration is favoured by children’s palliative care clinicians for symptom management when pain is sudden in onset, consciousness level reduced, swallow impaired, and there is no intravenous or subcutaneous access.
In buccal administration, drugs avoid first-pass metabolism, appearing in the circulatory system within 1 min, with peak plasma concentrations achieved within 15 min1–3 – considerably faster than the enteral route. The advantage of the buccal mucosa as a route of administration is its relatively large, immobile, smooth surface, with a rich blood supply, enabling rapid absorption into the systemic circulation. As such, the oral cavity provides a simple and accessible ‘no needles’ alternative, often preferable to parents and children. 4
A recent online questionnaire of 100 physician members of the Association of Paediatric Palliative Medicine (APPM) UK showed that 53% of respondents prescribe buccal morphine to infants and children 5 as part of routine practice. It is also recommended for use in current guidelines 6 and publications. 7 Yet there is considerable evidence from the adult literature that does not support buccal administration of morphine sulphate (MS).8–11 Moreover, there is no clear evidence of efficacy in the paediatric population. Reports of efficacy may reflect actual ingestion of the drug rather than buccal absorption.
Aim
To evaluate the transport properties of MS in an established ex vivo buccal mucosa model, as part of consideration of the efficacy of buccal morphine for the relief of pain in children with life-limiting conditions (LLC) and life-threatening illnesses (LTI).
Design
The ex vivo porcine model is a well-established and scientifically respected model for evaluating drug absorption across buccal tissue.12–14 The pig is the closest model to humans with respect to buccal or sublingual permeation properties.12,15 The knowledge of a drug’s buccal permeation properties, along with reported pharmacokinetic data, allows for calculation of plasma values following buccal administration in vivo. 12
Effective oral transmucosal delivery is usually associated with those molecules which are also administered via the transdermal route because of the inherent physicochemical properties of drugs required for absorption via both routes. Compounds, such as fentanyl, typically have a low molecular weight (<500), balanced lipophilic/hydrophilic properties and are potent (typical daily dose by any route should not exceed 20 mg because of the barrier properties of the tissue). Drugs that ionise (such as MS) will be present in saliva in both ionised and unionised forms. The log D, which indicates the distribution coefficient of the drug between lipid and water phases, is much more favourable for fentanyl than morphine with reference to buccal permeation. Notably, the minimum starting dose for oral morphine in adults is 10–20 mg and, taken together with the negative log D value (see Table 1), it strongly suggests that morphine is not efficacious when administered via the buccal route.
Physicochemical properties of fentanyl versus morphine.
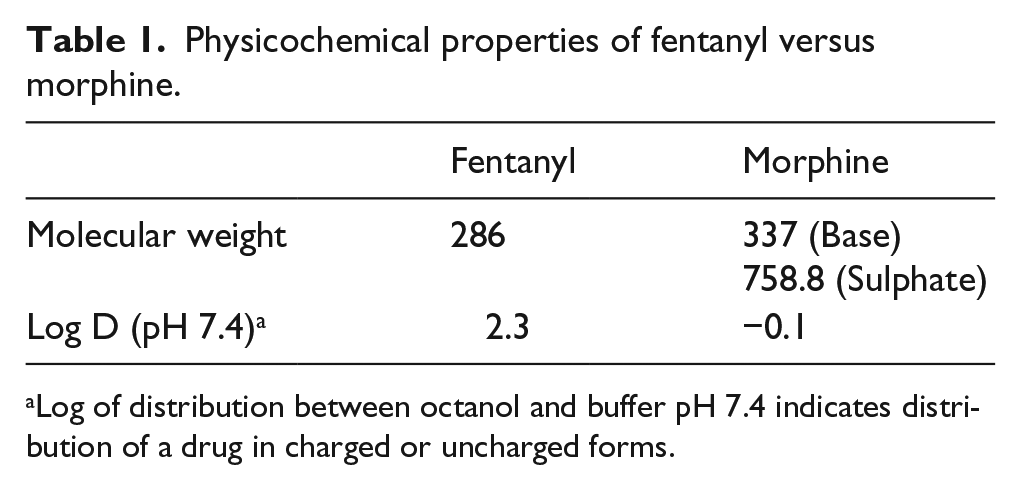
Log of distribution between octanol and buffer pH 7.4 indicates distribution of a drug in charged or uncharged forms.
Methods
All materials were obtained from Sigma-Aldrich and Fisher Scientific (UK). The high-pressure liquid chromatography (HPLC) analytical method including buccal model permeation and mass balance studies were done as previously described.16,17
In paediatric clinical practice, the buccal dose of morphine in an opioid naive child is generally calculated using an approximation to an equivalent intravenous dose of 50–100 µg/kg (due to theoretical consideration of first-pass metabolism) or, in children established on opioids, as 1/10th to 1/6th of the background opioid dose. Therefore, based on the weight of a 20-kg opioid naive child and a morphine dose of 100 µg/kg, in this permeation study, 200 µL of MS (1 mg/mL) in NaCl (0.9% w/v) was applied per cm2 in essence to replicate a total dose of 2000 µg of MS being administered to 10 cm2 of buccal tissue.
Results
Amounts of MS which permeated over 4 h are shown in Figure 1. Cumulative amounts permeated were 2.9 ± 1.2 µg/cm2.
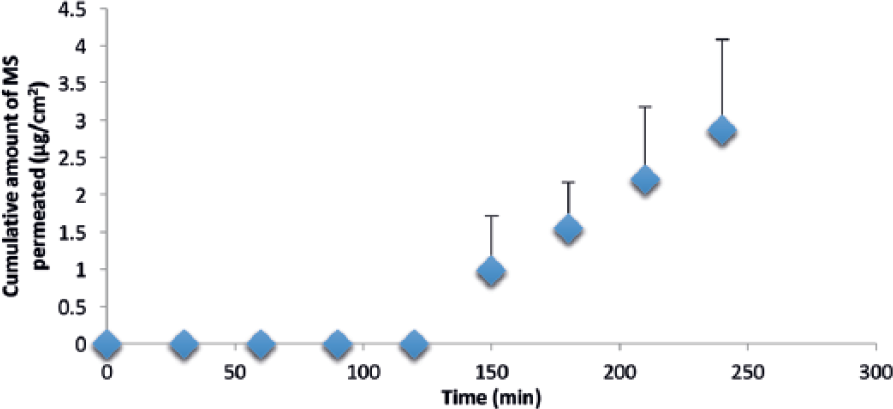
Permeation of MS in porcine buccal tissue over time (mean ± SD; n = 5).
From the linear portion of the profiles, steady state flux values were calculated as 1.32 ± 0.60 µg/cm2/h; the corresponding lag time before drug appears in the receptor phase was determined to be 1.8 ± 0.1 h.
Results of mass balance studies, presented in Figure 2, demonstrated a total recovery of >90% of MS. Most of the drug remained on the surface of the tissue after 4 h, with approximately 1.8% of the applied dose permeating to the receptor fluid and 7% being retained in the tissue.
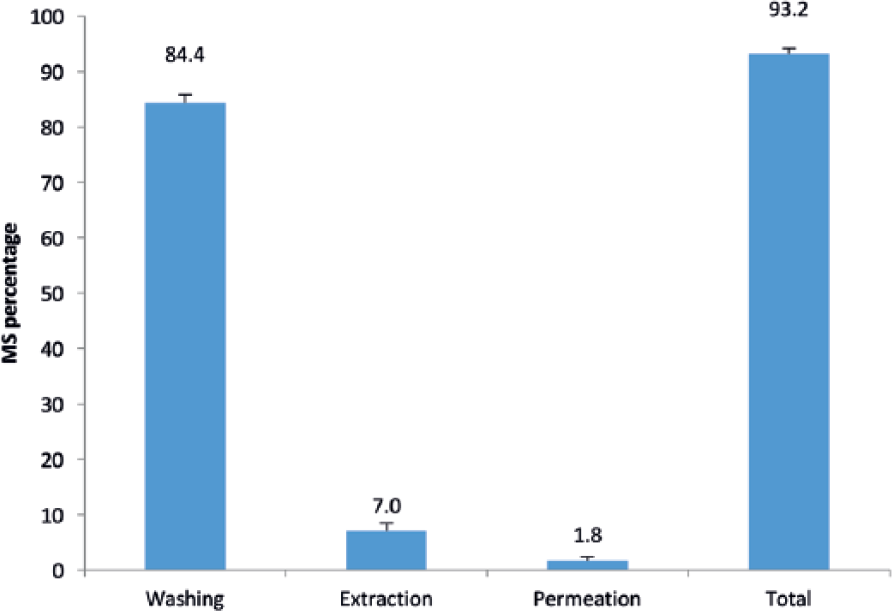
Amounts of MS recovered from surface of tissue, extracted from tissue and permeated to receptor phase in porcine buccal mucosa after 4 h (mean ± SD; n = 5).
Results show that less than 2% of the total MS quantity administered was actually absorbed through the porcine buccal mucosa. Results also indicate a considerable time lag – over 2 h – between application of the drug to the buccal tissue and any absorption occurring through the buccal tissue. With over 84% of MS found on the surface of the cells after 4 h, the results evidence that MS does not rapidly permeate porcine buccal mucosa.
Discussion
This study clearly demonstrates a poor absorption of MS in an ex vivo porcine buccal model. These findings support the existing knowledge base regarding the physicochemical properties of MS8–11,18–20 and its lack of suitability for transmucosal absorption.
For successful transmucosal delivery, drugs must have specific physicochemical properties. Drug absorption occurs through a passive diffusion process where solubility and lipophilicity are both necessary. More specifically, the epithelial membrane consists of a lipid (transcellular) pathway and an aqueous pore (paracellular) pathway, the latter being determined by molecular size, diffusion coefficient and partition coefficient.
The products available on the market today for buccal administration confirm that suitable drug candidates for administration via this route must have balanced hydrophilic and lipophilic properties and must be potent molecules, that is, total dose not greater than 20 mg daily. Thickness of tissue, the alkaline pH of saliva, available surface area and small fluid volume for absorption are also important factors.1,21,22
As morphine has a negative value for its distribution between lipid and water (Table 1), it is less suitable for buccal administration compared with fentanyl. It is also 80 times less potent than fentanyl.
There are several limitations to the hypothesis that the ex vivo porcine model reflects the in vivo environment in the child or infant. As yet, the permeation of paediatric human buccal mucosa has not been characterised in the literature. However, previous studies have confirmed ex vivo buccal porcine tissue is the closest model to human tissue and serves as an excellent model to assess feasibility of buccal drug delivery.12,15 That said, the degree of keratinisation, cell wall thickness and intercellular spacing may well be different in the neonatal epithelium as compared to the young child or adult, which may explain some of the anecdotal reports of efficacy in the use of buccal MS in infants and young children.
Additional factors such as rate of salivary production and flow were also not considered in this experiment. A higher flow rate of saliva is likely to increase the ‘wash-out’ effect and reduce absorption, hence having an important effect on drug pharmacokinetics. Increased salivary production and trouble managing these secretions are often cited as a common problem for children and infants managed by palliative care teams.23–25
Notwithstanding the molecule’s lack of suitability for buccal and/or sublingual delivery, attempts have been made by clinicians and pharmaceutical scientists to make available a buccal formulation of morphine.5–9,18–20,26 Early reported studies have lacked experimental rigour, with no oral morphine formulation as control. 26 Hoskin et al. 11 demonstrated that peak plasma drug levels occurred 6 hours after buccal administration of morphine with similar amounts of morphine-6-glucuronide; one of the major morphine metabolites measured for both oral and buccal administration. This suggests that the buccal absorption reported, in fact, reflects delayed oral absorption. These findings in human volunteers correlate with the results from this feasibility study. It is therefore possible that the analgesic effect thought to be due to buccal administration of morphine is actually due to absorption of the drug from the more distal gastrointestinal tract.
Despite not being wholly analogous to the living child, the porcine buccal model described above provides valuable information relating to buccal administration of analgesia in infants and children. Other opioids with favourable pharmacokinetic properties for buccal administration should also be investigated. Ideally, future research should include examination of the physiological properties of immature porcine buccal tissue compared to the adult model. This would also support further feasibility testing using permeation enhancers which may improve mucosal permeability and offer temporary enhancement of drug permeation via the paracellular route. 27
Conclusion
The laboratory study demonstrates that morphine is not well absorbed across the porcine buccal mucosa. It suggests that morphine does not cross the buccal mucosa in high enough quantities to be an effective analgesic and as such its use requires careful consideration when prescribing and also warrants further study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: E.M.H.’s post is funded by the Louis Dundas Centre for Children’s Palliative Care Programme Grant. M.B.-L.’s post is funded by the True Colours Trust.