
Abstract
Background:
Parents of children with a life-limiting disease have to rely on themselves at home while adequate paediatric palliative care is lacking. In several countries, paediatric palliative care teams are introduced to ensure continuity and quality of care and to support the child and the family. Yet, little is known about how parents experience such multidisciplinary teams.
Aim:
To obtain insight into the support provided by a new paediatric palliative care team from the parents’ perspective.
Design:
An interpretative qualitative interview study using thematic analysis was performed.
Setting/participants:
A total of 47 single or repeated interviews were undertaken with 42 parents of 24 children supported by a multidisciplinary paediatric palliative care team located at a university children’s hospital. The children suffered from malignant or non-malignant diseases.
Results:
In advance, parents had limited expectations of the paediatric palliative care team. Some had difficulty accepting the need for palliative care for their child. Once parents experienced what the team achieved for their child and family, they valued the team’s involvement. Valuable elements were as follows: (1) process-related aspects such as continuity, coordination of care, and providing one reliable point of contact; (2) practical support; and (3) the team members’ sensitive and reliable attitude. As a point of improvement, parents suggested more concrete clarification upfront of the content of the team’s support.
Conclusion:
Parents feel supported by the paediatric palliative care team. The three elements valued by parents probably form the structure that underlies quality of paediatric palliative care. New teams should cover these three valuable elements.
Parents of children with a life-limiting disease have to rely on themselves at home while adequate paediatric palliative care is lacking.
Over the last decade, paediatric palliative care teams are introduced in several countries to ensure continuity and quality of care.
Parents feel supported by the paediatric palliative care team and increasingly valued the team over time.
Parents highly valued the process-related aspects such as providing one reliable point of contact, continuity throughout the palliative trajectory and coordination of care; practical support; and the team members’ sensitive and reliable attitude.
The parents’ understanding of the additional value of the paediatric palliative care team increases the likelihood of parents’ acceptance of the team in an early stage of the palliative trajectory.
New paediatric palliative care teams should cover all three valuable elements identified in this study.
Paediatric palliative care teams can develop further by using the combination of the three valuable elements to provide support on new developments in paediatric palliative care, such as advance care planning.
Introduction
Parents caring for a child with a life-limiting disease (LLD) at home often lack adequate paediatric palliative care (PPC). They have to rely on themselves, during stressful and burdensome circumstances as well.1–4 As children with a LLD are increasingly cared for at home,5–7 well-organised PPC covering hospital and homecare situations is needed.3,8,9 Over the last decade, paediatric palliative care teams (PPCT) and PPC programmes have been introduced in several countries to support the child and family and ensure continuity and quality of care.10,11 Such teams generally focus on a multidisciplinary setting, 24-hour availability, coordination of complex care processes, ensuring continuity of care at home, hospital and hospice and sufficient expertise to address the physical, psychosocial and spiritual needs of the child and family.3,8,9
Studying the outcomes of PPCTs is still in its infancy. Some studies showed improvement of the child’s quality of life, better management of the child’s symptoms and reduction of the child’s suffering.10,12–17 Children were also more likely to die at home. 12 Additionally, Groh et al. 14 indicated that the involvement of a PPCT improved the parents’ quality of life and decreased their burden of homecare. Other studies evaluating PPCTs showed parents’ satisfaction with the provided PPC by these teams.10,11,16,18 Furthermore, parents felt supported emotionally, with decision-making and with communication within the family and with healthcare professionals (HCP), and felt more prepared for their child’s end-of-life experience.10,15–17
Besides the above-mentioned outcomes of PPCTs, little is known what a PPCT means to parents in detail. Therefore, this study aims to gain insight into the parents’ experiences with a multidisciplinary PPCT, supporting children and families throughout complex palliative care processes.
Methods
To elucidate parents’ experiences with the PPCT (Box 1), an interpretative qualitative study using an inductive thematic analysis was conducted.20–22 The method and reporting follow the Consolidated Criteria for Reporting Qualitative Research (COREQ). 23 This study was part of a larger study aimed to evaluate a newly introduced PPCT and to explore parents’ experiences with caring for a child with a LLD.
Description of the Paediatric Palliative Care Team (PPCT).
In June 2012, the first Dutch hospital-based PPCT was initiated at a large children’s university hospital in Amsterdam. The PPCT is a multidisciplinary team consisting of five specialised nurses (i.e. case managers) trained and experienced in paediatric palliative care, two child life specialists, a social worker, a psychologist and a chaplain. In addition, two paediatricians and two paediatric oncologists were appointed to the PPCT for consultation and participation in the weekly multidisciplinary team meetings.
The PPCT is responsible for the coordination, continuity and provision of good quality of paediatric palliative care, irrespective of the child’s place of residence. In addition, the PPCT strengthens regular care by providing support and education to healthcare professionals involved in paediatric palliative care. If regular care fails, the PPCT is competent and qualified to provide temporary nursing care when needed, also at home.
The PPCT is open to all children diagnosed within any of the four categories of a life-limiting or a life-threatening disease, 19 preferably in an early stage of the child’s disease. The support provided by the PPCT is continuous throughout the disease trajectory, including a 24-hour availability of the case managers and bereavement care after the child’s death. Out-of-hours the case managers have access to the paediatric specialists on call of the children’s university hospital.
The PPCT aims not to replace existing care but to navigate parents and involved healthcare professionals through the complex care processes and to gap the bridge between the homecare situation and hospital through contact with the parents by phone, email and personal visits at home and during hospitalisations. When indicated, also the treating physician visits the family at home.
Sample
A purposeful sample of Dutch-speaking parents of children with a LLD primarily residing at home who were referred to the PPCT was recruited from an university children’s hospital (the Emma Children’s Hospital AMC, Amsterdam). To capture a wide range of perspectives and facilitate a broad understanding and validation of our findings, variation in selected children was sought with respect to the duration of PPCT’s involvement, malignant and non-malignant diagnoses and the phase of the palliative trajectory. 24 Based on the literature, the palliative trajectory was distinguished in four phases: diagnostic phase, phase of losing normality, phase of decline and the dying phase.19,25 Some parents were approached shortly after the child’s death to increase insight into the dying phase. Parents of 35 cases were identified as eligible. A member of the PPCT or the clinician introduced this study to parents and asked permission for the researchers to contact them. In six eligible cases, the introducing HCP considered the parents’ situation too vulnerable to inform them about this study. Parents of 29 children were invited by telephone to participate by the researchers. In five cases, parents refused participation. Reasons for refusal were as follows: no time (n = 2), too burdensome (n = 2) and unknown (n = 1).
Data collection
Individual open interviews were conducted at home between August 2013 and November 2015 and lasted from 30 min to 2 h. The interviewers (L.V.: trained in qualitative research; M.K.: experienced qualitative researcher) were independent researchers from another university than where the PPCT was established. To check whether all topics were discussed, a topic list (Online Appendix) based on the literature and experts’ knowledge was used to guide the interview. Topics relevant for this study were as follows: who introduced the PPCT, timing of introduction of the PPCT, content of support by the PPCT, missing aspects and recommendations for the PPCT. Field notes were made after each interview. Interviews were audio recorded and transcribed verbatim. Descriptive background variables were gathered from parents and the medical records. The study was approved by the research ethics committee of the Academic Medical Centre Amsterdam (12 June 2013; Reference number: W13_120 # 13.17.0153). Written informed consent was obtained from all participating parents.
Data analysis
In accordance with methods that optimise validity and rigour, 26 an inductive thematic analysis was used.20–22 Three researchers (L.V., M.K., J.v.D.) were involved during the entire process. They used joint meetings to reach agreement on interpretation of the data and findings and work towards consensus. Therefore, researcher triangulation was ensured to improve reliability of the analysis.
The thematic analysis consisted of two phases. First, the researchers (re)read the transcripts of eight interviews individually to become familiar with common aspects and phrases in the context of the interview.20–22 At least two researchers analysed and open coded these eight transcripts individually with paper and pencil and compared interpretations together. The meaning of the separate fragments was determined by the meaning of the interview as a whole. 27 The open codes were recoded, resulting in an adapted code list with concepts at a more abstract and conceptual level. 20
During the second phase, every new interview was read and discussed by at least two researchers. Supported by the software program NVivo10, 28 one researcher (L.V.) coded all transcripts. After coding each transcript, the code tree was evaluated and, if indicated, revised. The different codes were sorted into themes, which were defined and refined. 21 To guide the constant comparative method, the research team went back and forth between the different steps and the entire data set to capture the main aspects of the themes in the raw transcripts. To ensure validity and provide transparency of the results, an audit trail was used to record methodological choices and substantive ideas and concepts related to the interpretation of the data. Saturation was reached on a conceptual level.
Results
In total, 42 parents (24 mothers, 18 fathers) of 9 children diagnosed with a malignant disease and 15 children diagnosed with a non-malignant disease were included. A total of 11 parents were interviewed after the child’s death, of which five were second interviews. In total, 47 interviews were conducted. For patient characteristics, see Tables 1 and 2. Cases varied in time between diagnosis and start of the PPCT, the duration of the PPCT’s involvement and the amount of provided support by the PPCT (Table 3). Analysis of the interviews revealed that parents highly valued three main elements of the PPCT’s support: (1) process-related aspects, (2) practical support and (3) the PPCT members’ attitude. Additionally, suggestions for improvement of the PPCT are presented below.
Characteristics of the parents (N = 42) and their ill child (N = 24).
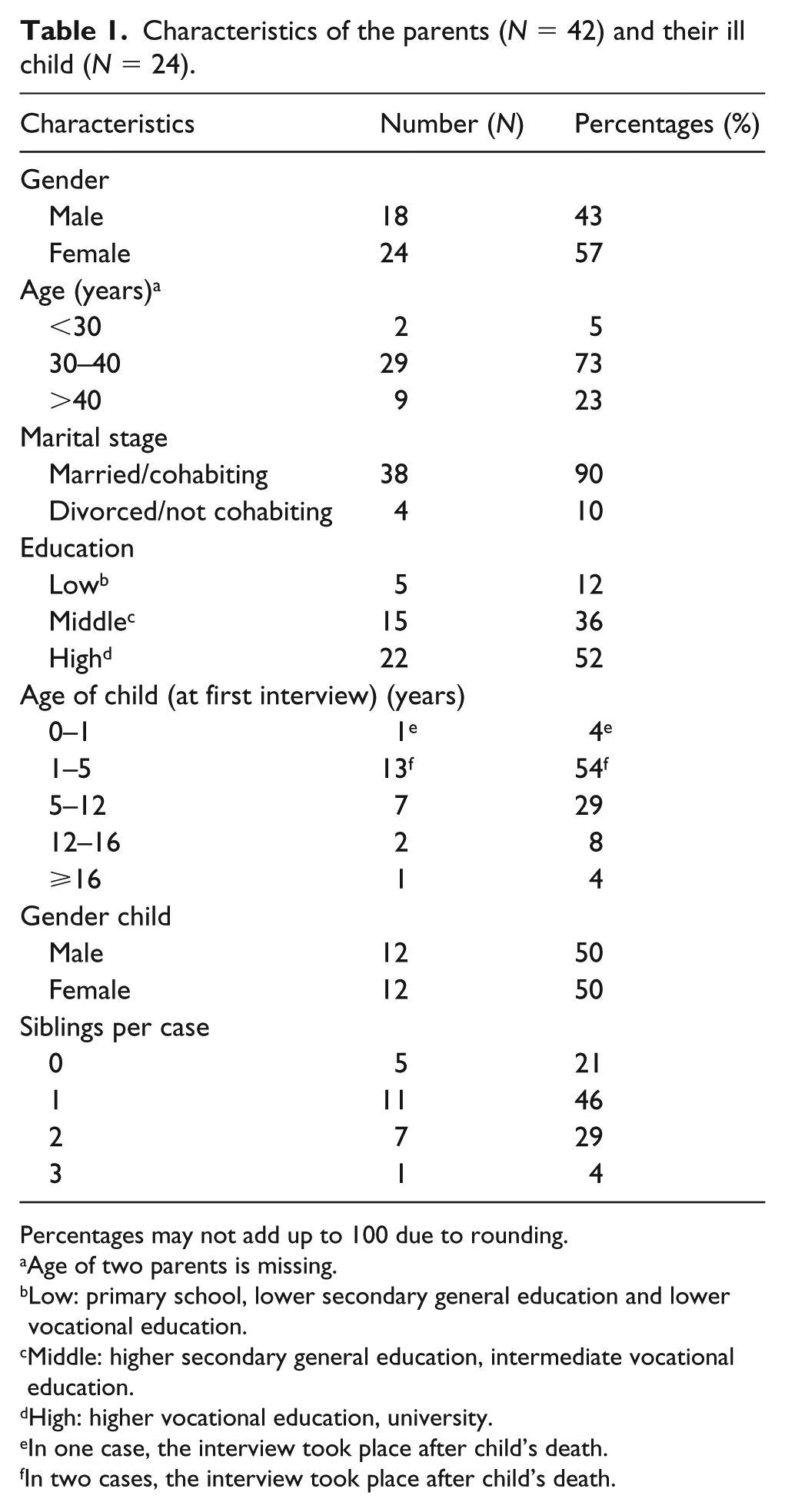
Percentages may not add up to 100 due to rounding.
Age of two parents is missing.
Low: primary school, lower secondary general education and lower vocational education.
Middle: higher secondary general education, intermediate vocational education.
High: higher vocational education, university.
In one case, the interview took place after child’s death.
In two cases, the interview took place after child’s death.
Diagnosis and stage of the palliative phase of the disease.
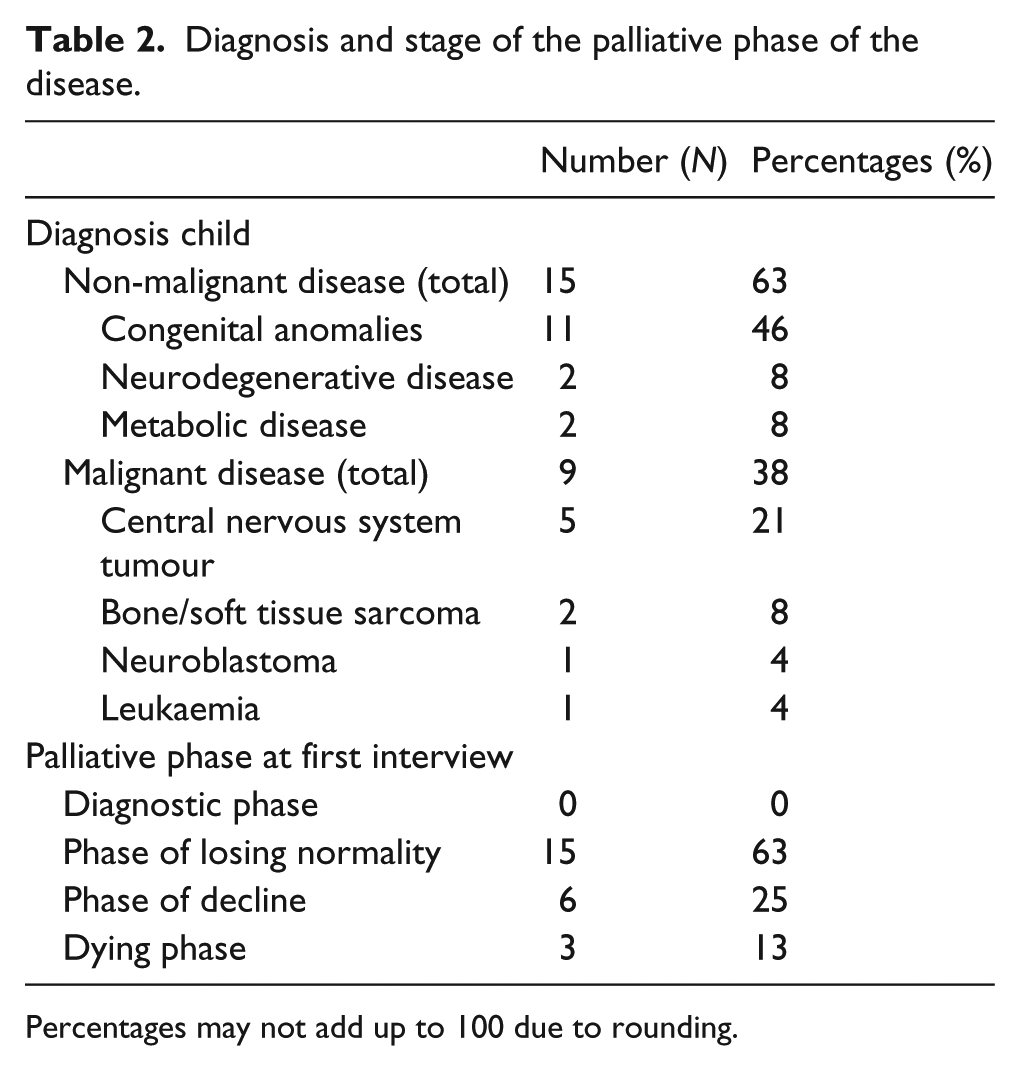
Percentages may not add up to 100 due to rounding.
Involvement of the paediatric palliative care team.
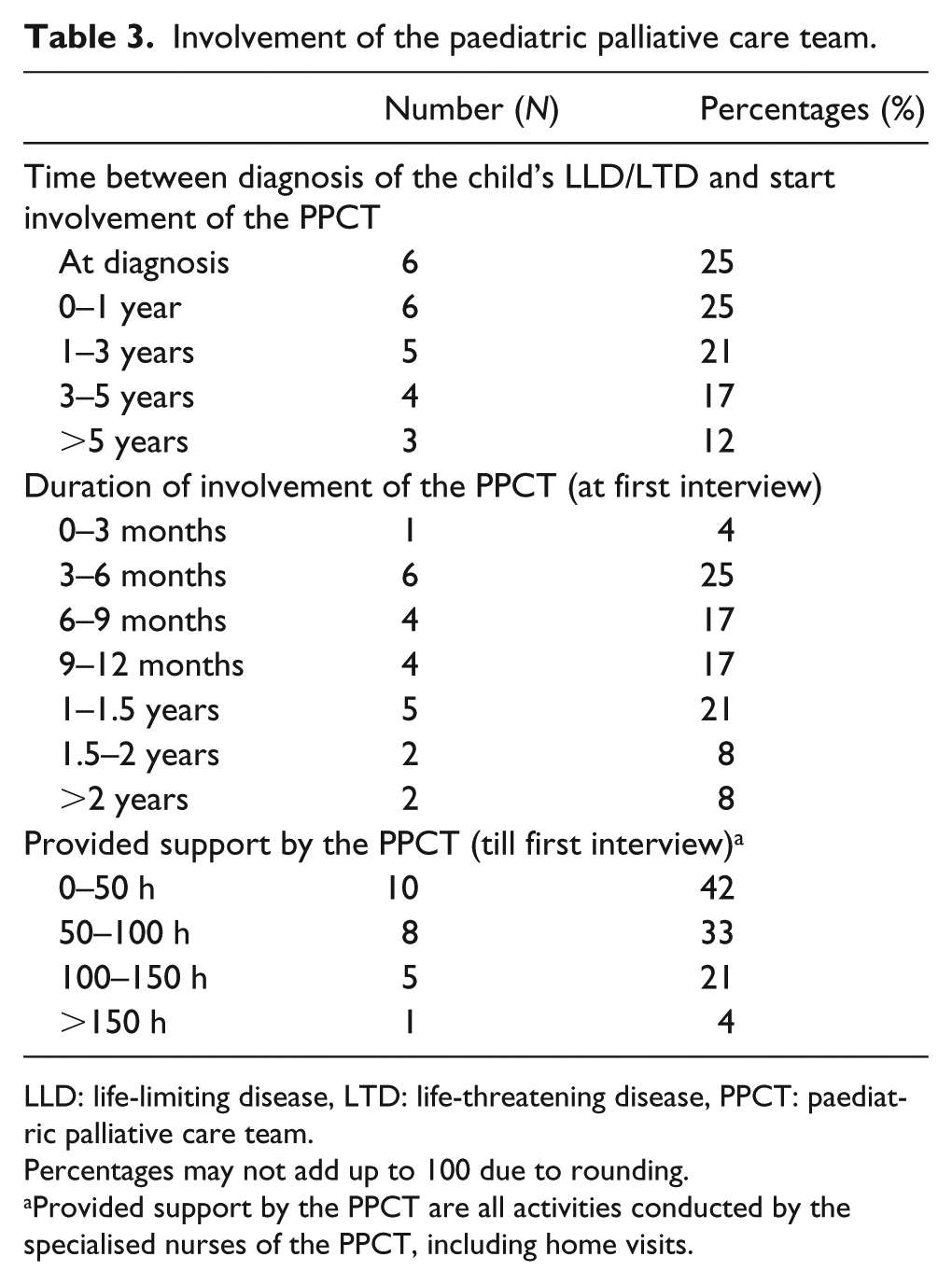
LLD: life-limiting disease, LTD: life-threatening disease, PPCT: paediatric palliative care team.
Percentages may not add up to 100 due to rounding.
Provided support by the PPCT are all activities conducted by the specialised nurses of the PPCT, including home visits.
Valuable elements of the PPCT
Process-related aspects
Parents appreciated the following process-related aspects of the PPCT: one reliable point of contact, continuity and coordination. All parents emphasised that they now had one easy accessible and reliable point of contact. When calling the PPCT, parents knew that they would be directly in touch with the right person, who was well-informed about their child and family. For parents this meant saving valuable time because they did not have to repeatedly tell their story. Moreover, parents knew that the PPCT could answer their question(s) or directly undertake some kind of action to support them:
It was a big relief to know that I absolutely could call her (case manager) any time. That is one of the most important things, you want to have that reassurance that if you are in a blind panic in the middle of the night with a child who is dying, that you immediately can get the right person on the line. And that you will be heard. And that was always the case, the team was accessible 24 hours a day, and she did have that back door entrance to the oncology department, so she knew whom she needed to call. (Mother, case 19, boy, malignant disease, interview took place after the child’s death)
Most parents considered the continuity of the PPCT itself during the palliative trajectory to be of major importance. Once parents realised the PPCT was available throughout the whole palliative trajectory, including bereavement, parents felt they could trust and rely on the PPCT knowing they would not leave them alone at some point:
Also important, that the team would be there for always, not like … We had a medical day care, of course she (daughter) could go there, but only until age 4. Then you have to look further again. And with the home care it was also like we will come, but only to take care of the PEG tube, until you can do it yourself. While with the team it was as long as she (daughter) is here and as long as you need it, we are here for you. Then you think, I can be open with you, you may know everything about me, because you will stay with me. (Mother, case 11, girl, non-malignant disease, interview took place after the child’s death)
Additionally, parents valued the out-of-hours accessibility of the PPCT. Although they rarely contacted the PPCT out-of-hours, knowing that the PPCT was accessible anytime, and thus someone who could always adequately help them, made parents feel less abandoned and more reassured to care for their child at home.
Most parents told that the case managers of the PPCT served as the central professional caregiver who had relations with all HCPs from all care settings involved in their child’s care. Furthermore, parents appreciated the home visits performed by the PPCT because parents noticed that this provided the PPCT with valuable insight into the situation at home and the support needed. Parents mentioned that the PPCT functioned as a bridge between them and the hospital because the PPCT knew all HCPs involved and knew the child and family both in the hospital and home setting. They appreciated that the PPCT could navigate through the hospital, making it possible to coordinate combined appointments or procedures or to urge an HCP to call parents back in time. Moreover, the PPCT could speed up the process of organising appropriate care:
What she (case manager) also does, look, she doesn’t have to know the answer, what she does is that she speeds up the process, so she says I think doctor Kortens (paediatrician) should call you now and then we had doctor Kortens on the line that same afternoon. It means that you directly are connected with the right people. (Father, case 12, 4-year-old boy, non-malignant disease)
One couple expressed this had been crucial in enabling them to go home with their child for their child’s end-of-life phase. Some parents mentioned that the PPCT tried to align all involved HCPs with each other and with the child’s and family’s needs by regularly informing them or by organising multidisciplinary conferences with them and parents. Due to the coordination of care by the PPCT, most parents no longer had to navigate uncharted territory themselves because they found the support they needed.
Practical support
All parents mentioned that the PPCT adequately and quickly arranged all kinds of practical matters relevant to the child and family, such as equipment, reimbursements or medical prescriptions. Parents experienced organising the practical matters themselves as complex tasks. When the PPCT provided practical support, parents saved energy and valuable time, which they now could spend on being there for their child. To get practical matters arranged, parents discovered they only once had to call the PPCT. This made parents feel that they could trust and rely on the PPCT when asking for help because the PPCT did what they promised. Consequently, parents felt greatly helped and relieved:
Then the paediatric palliative care team came into the picture and everything that I turned over to her (case manager), that was solved. You can arrange everything as parents but that takes so much energy, energy you totally don’t have any more and energy that you need for the last part leading to the death of your child. Then it is good that I can say to her, I’m coming up against this, we don’t have that and we have a question here. And she calls me back the same day to say this is arranged and this is the answer and that is the answer and tomorrow that person will be coming by. (Mother, case 19, boy, malignant disease, interview took place after the child’s death)
The PPCT members’ attitude
Parents appreciated various aspects of the team members’ attitude: sensitivity, experience and expertise, close involvement and awareness of the whole family. Parents valued that the PPCT members were sensitive to their needs and readiness to deal with necessary steps in PPC that are experienced as difficult to accept:
She (case manager) sensed very well what we wanted. And then it is pleasant, then it is comfortable. (Mother, case 4, 10-year-old boy, malignant disease)
Consequently, parents felt rarely disrupted or forced by the PPCT. Some parents appreciated that members of the PPCT were closely involved with their family without losing their ability to adequately support parents:
They (members of paediatric palliative care team) are affected, but not amongst those saying how horrible it is. No, just this is what we have to deal with, we have to deal with this situation and we are going to handle it. (Mother, case 12, 4-year-old boy, non-malignant disease)
Many parents indicated not knowing what the new world of their ill child would entail and what to expect throughout the palliative process. Therefore, parents appreciated the PPCT members’ (practical) experience and expertise in PPC because the members could address signalled issues to parents and provide insight into possible future situations, the range of care facilities and tailored advice towards parents:
My experience with her (case manager) is very positive. I think it’s really great, someone who knows the process, who knows what is happening, what the mechanics are, how it affects the situation at home, someone who really understands and says very sensible things. (Father, case 7, 7-year-old boy, non-malignant disease)
Additionally, parents mentioned that the PPCT not only cared for their ill child but also signalled the needs of the parents and, if present, the siblings. The ideas and strategies of the PPCT available to organise and coordinate the needed support for the whole family made parents feel relieved and assisted:
What I really like about the PPCT is that they have resources. And what’s so good is that they have the whole family in their scope, so that if Sem (sibling, 11 years), is not doing well at school, or if questions come from school, then I can ask the child life specialist or social worker to help come up with solutions. And that the psychologist can be consulted, for us as a family or the two of us as a couple. (Mother, case 7, 9-year-old boy, non-malignant disease)
Due to the PPCT’s attitude, parents described the PPCT as easy accessible and experienced a low-threshold to contact them. Parents emphasised they could tell their story or ask the PPCT anything and were respectfully treated without feeling judged, such as questions they could not or dared not ask anyone else because they felt as inappropriate or ignorant. For instance, ‘what will happen after my child dies and where is his/her body going to’. Most parents experienced that the PPCT really listened and was an adequate sounding board:
This week we were at the outpatient clinic and I was talking alone with our case manager about various things and you just see that she is really a listening ear. You can see that it isn’t fake, it’s really sincere. (Father, case 17, 9-year-old girl, malignant disease)
Consequently, parents felt taken seriously, emotionally supported, and they felt they could share their responsibilities to ensure the best support for their child and family. For instance, parents could discuss with the PPCT whether or not to consult a doctor when new symptoms suddenly appeared:
So I try to assess whether a physician needs to look at something or that it is more my searching, looking for a sounding board. If I just need someone else to state an opinion, for example about that low temperature, which she has had now for a month, yeah then I prefer to call the PPCT to ask whether they think I have to do something or not. Or can I just wait and see? (Mother, case 14, 1-year-old girl, non-malignant disease)
Parents received tailored advice from the PPCT and felt empowered in making, both minor and major, decisions without feeling forced by the PPCT. As such, parents experienced themselves as being in control of directing the process, which was highly valued.
Suggestions for improvement of the PPCT
Many parents had difficulty answering the question to formulate missing aspects or suggestions for improvement of the PPCT. One father missed adequate coordination of care between the PPCT and the homecare and had to direct more strongly to arrange care how he wanted it. Some parents felt disappointed that the PPCT did not regularly provide nursing care at home, as some of them had initially expected.
The most mentioned topic for improvement of the PPCT was to enhance parents’ understanding of the PPCT’s value in advance. Most parents described that they had limited expectations about what support the PPCT could provide them:
If we had known in advance, in hindsight we now know of course, because then you know what the paediatric palliative care team is and what palliative care involves, which supported us very well through that period (end-of-life phase of his son). So if we had known that in advance then we more easily could have changed our thinking (toward accepting the paediatric palliative care team). What the value of the team is and how much they can do for you and how much they can take care of, so you get more space to really be with your child and not just perform the medical procedures. Yes, that is really very valuable. (Father, case 19, boy, malignant disease, interview took place after the child’s death)
Nonetheless, they assumed that the PPCT could be useful in the future and accepted their involvement. Once they experienced the PPCT’s support in daily life, they became more aware of the content of the PPCT’s role and gradually valued this. Therefore, parents suggested that improved understanding of the PPCT’s value by parents of future patients might lead to greater reliance on the PPCT from the start:
The paediatric palliative care team is invaluable. And I think that they really should emphasise this more, apart from the 24 hours and 7 days a week, but people have to experience that their help really is a relief. That a group of people stand ready 24 hours a day, 7 days a week, who are the key to the university hospital, for all questions and issues … because they will come. And, in my opinion, if you make this clear to parents, that that is their role, well, then perhaps parents can see in advance that it … that it doesn’t feel as threatening. (Father, case 12, 4-year-old boy, non-malignant disease)
A booklet about the PPCT, including examples about the support the PPCT can provide and the variety of questions parents can ask, was suggested to clarify when and for what reasons parents can contact the PPCT and what support they can expect. The PPCT’s involvement sometimes confronted parents with their own extraordinary situation. Therefore, one parent suggested that parents might need time to accept that their child needs PPC, including the involvement of a PPCT.
Discussion
Once parents experienced the support of the PPCT in daily life, they became more aware of the PPCT’s role and the content of their support and increasingly valued the PPCT. Three valuable elements of the PPCT were identified: process-related aspects, practical support and the PPCT members’ sensitive and reliable attitude. Parents suggested to clarify the content of the support provided by the PPCT more concrete upfront to increase the likelihood of an early parental acceptance of the PPCT.
PPCTs are primarily initiated to ensure quality and continuity of PPC.3,8,9 Parents in this study did not explicitly mention (improved) quality of PPC or continuity of PPC, instead, what they explicitly valued was the continuity of the PPCT itself. Whereas studies on PPCTs focus on outcomes of PPCTs,10–18 we tried to open the black box of what may have contributed to reach these outcomes. The combination of the valuable elements of the PPCT as identified in this study might be the reason that a PPCT is able to achieve these positive outcomes. As such, the valuable elements, including the home visits, are a main strategy of the PPCT to empower parents in performing all tasks that have to be done, particularly at home. Additionally, the PPCT members’ attitude, their practical approach and guidance throughout the palliative trajectory form a fundament on which parents can accept the PPCT and feel supported, without being forced to do so. Therefore, initiating PPCTs that cover these three elements is a good starting point for improving PPC. However, PPC should also include actively guiding parents for the next step in the palliative trajectory of their child and supporting parents in giving their child his or her voice.29,30 In this study, these aspects were not mentioned by parents.
Parents described that the PPCT helped them to open their eyes to other family members besides their ill child and, when needed, to arrange appropriate support for the siblings or themselves. Earlier studies indicated that it is important to support every family member because the death of a child has a devastating effect on the survivors.31–35 Contro et al. 36 described that PPC was not able to meet the needs of siblings before PPC programmes were established. Our study adds that parents perceived the PPCT’s awareness for all family members and their knowledge about the care possibilities as valuable because parents missed the energy or had no ideas how to support the siblings or themselves. Moreover, because of the availability of multidisciplinary professional support within the PPCT, adequate support was guaranteed when this was not available in the family’s neighbourhood.
Parents had limited expectations of the PPCT’s role. Apparently, it is challenging for parents to imagine what they might need now or in the future to feel supported. We hypothesise that this phenomenon complicates parents’ ability to express their needs in advance. This supports the strategy of coaching parents on the job and providing active direction to improve PPC.
This study has some strengths and limitations. It is the first Dutch study evaluating parents’ experiences with a PPCT. However, it is a one-centre study, limiting the generalizability of our results. Nevertheless, our sample showed a wide variation in diseases, phase of the palliative trajectory and duration of the PPCT’s involvement, and we included both fathers and mothers who were currently caring or had recently cared for a child with a LLD. These aspects enabled us to give a realistic overview of parental experiences with a PPCT. Well-educated parents were overrepresented in our study; however, we do not have the impression that this influenced the parental experiences of the PPCT. A few HCPs delayed or protected participation of eligible parents because they considered them as too vulnerable or burdened, a practice that is known as gatekeeping and often seen in palliative care research. 37 This might have resulted in an underestimation of the experienced support by parents of the PPCT. Differences between cultural and ethnic backgrounds were not captured. Future research should focus hereon because there might be cultural differences in parents’ acceptance of professional care, including a PPCT, and parents’ perceptions of end-of-life processes.
Conclusion
This study showed that parents feel supported by the PPCT and increasingly valued the PPCT. Parents highly appreciated the process-related aspects, the practical support and the PPCT’s members sensitive and reliable attitude. These three elements probably underlie the achievement of reported outcomes, such as improved quality of life of the child and family and qualified PPC. Therefore, new PPCTs preferably incorporate these elements in their approach. Additionally, PPCTs can develop further by using these elements to provide support on new developments in PPC, such as advance care planning.
Footnotes
Acknowledgements
We thank all the parents who participated in this study. We also thank Madelief Buijs for conducting the first interviews.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was sponsored by the Netherlands Organization for Health Research and Development (ZonMw), Grant Number 82-82100-98-208.