
Abstract
Background:
It is important to understand the costs of palliative and end-of-life care in order to inform decisions regarding cost allocation. However, economic research in palliative care is very limited and little is known about the range and extent of the costs that are involved in palliative care provision.
Aim:
To undertake a systematic review of the health and social care literature to determine the range of financial costs related to a palliative care approach and explore approaches used to measure these costs.
Design:
A systematic review of empirical literature with thematic synthesis. Study quality was evaluated using the Weight of Evidence Framework.
Data sources:
The databases CINAHL, Cochrane, PsycINFO and Medline were searched from 1995 to November 2015 for empirical studies which presented data on the financial costs associated with palliative care.
Results:
A total of 38 papers met our inclusion criteria. Components of palliative care costs were incurred within four broad domains: hospital care, community or home-based care, hospice care and informal care. These costs could be considered from the economic viewpoint of three providers: state or government, insurers/third-party/not-for-profit organisations and patient and family and/or society. A wide variety of costing approaches were used to derive costs.
Conclusion:
The evidence base regarding the economics of palliative care is sparse, particularly relating to the full economic costs of palliative care. Our review provides a framework for considering these costs from a variety of economic viewpoints; however, further research is required to develop and refine methodologies.
Keywords
Economic evidence in palliative care is important for making decisions regarding allocation of resources.
Economic research in palliative care is very limited.
Little is known about the range and extent of costs that are involved in palliative care provision and approaches used to capture these costs.
Components of palliative care costs are incurred within four broad domains: hospital care, community or home-based care, hospice care and informal care.
Palliative care costs can be considered from the economic perspective of three providers: state or government, insurers/third-party/not-for-profit organisations and patient and family and/or society.
A wide variety of costing approaches are used to derive costs; the majority are country specific.
Research should prioritise evaluations of the full economic costs of palliative care, rather than discrete elements of care.
A framework for considering the components of costs to include in economic evaluations is presented and can be adapted for use in future research.
Further research is required to develop and refine economic methodologies, particularly those which enable international comparisons to be made.
Introduction
Growing demands are being placed on palliative care services as a result of population ageing, extending palliative care to people with non-cancer diagnoses and increasing death rates. 1 As a result, palliative care must compete with other areas of care for finite resources, within a highly competitive funding environment, so that resources can be allocated effectively. It is therefore important to understand the costs of palliative and end-of-life care in order to inform decisions regarding cost allocation. 2 Health economic evaluations are widely used to aid decision-making with respect to healthcare services, including palliative care. The analysis of the comparative costs of alternative treatments or healthcare programmes is common to all forms of economic evaluation. Two of the most fundamental questions to be considered in such evaluations are as follows: (1) which costs should be considered and (2) what is the viewpoint for the analysis (i.e. from whose perspective are costs to be considered). 3
Within the context of palliative care, the first of these questions is complicated by the nature of palliative care interventions which commonly include multiple interacting elements, 4 meaning the type and extent of costs are often complex. The second question is complicated by the wide range of individuals and organisations who are involved in funding palliative care and the overlap between these different providers. 5 Palliative care is currently provided across three settings: hospital, community or home-based and hospice. Where palliative care is provided in hospices and specialist inpatient units, these are often co-funded through public healthcare systems or insurers and third-party not-for-profit organisations. This means the adoption of a single ‘viewpoint’ for economic evaluation is often not appropriate. In addition, the financial costs to patients and family caregivers in palliative care are also significant, although this viewpoint has been particularly neglected and under-researched. 6 Therefore, while well-evidenced and robust methods are available to guide economic evaluations in health care, 6 the most appropriate methods to undertake such evaluations in the context of palliative care are unknown, due in large part to the complexity inherent within the discipline. Perhaps as a consequence of these methodological challenges, economic research in palliative care is very limited. Indeed, a 2011 report from the UK Department of Health identified a ‘stunning lack of good data surrounding the costs for palliative care in England’ (p. 9). 5 The international evidence base regarding the economic dimensions of palliative and end-of-life care provision is similarly sparse. 7 A recent study from Canada noted the narrow viewpoint that the majority of economic analyses have taken, highlighting that these have been limited to the measurement of publicly financed care without consideration of the considerable costs faced by other stakeholders, including patients and their families. 8 These issues are further compounded by inconsistent definitions of palliative care internationally 9 which have hampered attempts to identify exactly what constitutes a palliative care cost.
It was within this context that we identified a need to synthesise the existing literature in order to inform much needed consideration of which costs are potentially relevant in economic evaluations of palliative care. Related to this, we also identified a need to consider the methods used to collect, and accurately cost, palliative care data with a view to providing methodological guidance for future economic evaluations in palliative care. The aim of this article is therefore to undertake a systematic review of the health and social care literature to determine the range of financial costs related to a palliative care approach and explore approaches used to measure these costs.
Methods
In order to increase methodological rigour and transparency, and provide clarity around the research aim, the following definitions have been applied to the key concepts of the review. A palliative care approach is defined as a comprehensive package of palliative care incorporating specialist and/or generalist elements. For the purposes of this review, specialist palliative care is defined as care provided by professionals who have undergone recognised specialist palliative care training and generalist palliative care is defined as palliative care provided as part of standard clinical practice by any healthcare professional who is not part of a specialist palliative care team. The range of costs is defined as all elements or components of health and social care expenditure related to a palliative care approach, including costs to patients and/or family members and societal costs. Approaches to measuring costs are the methodological approaches used by researchers to capture and accurately cost economic data relating to a palliative care approach.
Four electronic databases (CINAHL, Cochrane, PsycINFO and Medline) were searched from 1995 to Nov 2015. A search strategy was devised by the authors in consultation with an information specialist (Table 1) and applied to title, keywords and abstracts. The search was limited to the last 20 years in recognition of the rapidly changing nature of funding and economic research and the limited relevance of research published pre-1995. The search comprised Medical Subject Headings (MeSH) and keywords related to the research question; an initial scoping search was undertaken in order to refine the search strategy. Appropriate wildcards were inserted to search for word ending truncations where necessary. Reference lists of included studies were hand-searched. We also undertook a comprehensive grey literature search of the following organisations: Marie Curie Cancer Care, Nuffield Trust, UK Department of Health, National Institute for Clinical Excellence (NICE), Kings Fund, World Health Organization (WHO), National Audit Office (NAO), Office for National Statistics, National Council for Palliative Care, National End of Life Care Intelligence Network, American Academy of Hospice and Palliative Medicine and US Department of Health and Human Services. All searches were undertaken in November 2015.
Search terms.
MeSH: Medical Subject Headings.
Title and abstracts of all articles were screened by C.G. to identify those which met the study inclusion criteria. Study inclusion criteria can be found in Table 2. The original intention had been to restrict inclusion to papers which reported the full economic cost of palliative care, that is, the costs incurred in all settings related to the receipt of a palliative care approach, from the viewpoint of all providers including state/government, third-party payer and society and patient/family. However, the scoping exercise identified very few papers that met this criterion so inclusion criteria were expanded to papers reporting costs in more than one setting or from the viewpoint of more than one provider.
Inclusion and exclusion criteria.
Full texts of all included articles were independently screened by two of the four authors (C.G., M.G., C.I. and T.R.). Studies were again assessed to identify those which met the inclusion criteria. Where there was lack of consensus, a third person acted as arbitrator. Details of included studies were extracted onto pre-defined forms.
The scoping search indicated that studies included in the full review would be likely to have diverse methodologies and significant heterogeneity; therefore, a thematic synthesis method was chosen in order to achieve translation between the results of the diverse studies. 10 The thematic approach guided data extraction and was based on pre-defined categories relating to the research aim. Data were extracted on the aim of the study, the design of the study, the components of costs, the data sources used and the methods used to collect cost data (Table 3).
Details of included studies.
PCT: primary care trust; ER: emergency room; AHCR: Ambulatory and Home Care Record; WELCAN: Welsh/Canadian; GP: general practitioner; PC: palliative care; EOL: end of life; DIN: Doctors Independent Network; MIMS: Monthly Index of Medical Specialties; OT: occupational therapist; RIW: Resource Intensity Weight; MCBS: Medicare Current Beneficiary Survey; IV: intravenous; HF: heart failure; RF-HI: Republic Fund of Health Insurance; NHS: National Health Service; HSPCs: home-specialised palliative care services.
Study quality was evaluated using the ‘Weight of Evidence Framework’, a method which structures quality and relevance appraisal in terms of three dimensions which involve both generic standards and review-specific assessments. 48 This approach to quality appraisal is particularly recommended for reviews involving studies with diverse methodologies where traditional method–specific checklists are not appropriate. The first dimension is the quality of execution of the study according to generic and accepted standards associated with that type of study (methodological quality). The second dimension is the appropriateness of the study design for answering the review question (methodological relevance). The third dimension is how well matched the study is to the focus of the review (topic relevance). Studies were given a grading of 1–3 (low–high) for each dimension and scores totalled. Studies with a total score of <4 were excluded.
Results
Search results are summarised in the adapted Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart in Figure 1. A total of 39 papers met our inclusion criteria; however, one scored poorly on study quality (<4) and was subsequently excluded resulting in a final total of 38 papers (Table 3). All studies reported on a ‘palliative care approach’; however, the definition of palliative care differed across studies. The majority of studies were retrospective reviews of routine or claims’ data (n = 18) or prospective cohort studies (n = 10). Five studies were literature reviews, two were economic modelling studies, one a comparison group design, one a pilot study and one a methods development study. The majority of studies were from Canada (n = 11), the United States (n = 7) and the United Kingdom (n = 7). Quality scores of the included studies varied markedly, and only four received the top score of 9.13,14,18,47 In general, low scores reflected the lack of high-quality data with which to estimate costs, rather than poor methodological choices or poor topic relevance.
PRISMA diagram summarising search results.
Components of palliative care costs
Included studies reported a wide range of costs that were associated with providing a palliative care approach. However, only eight papers (based on data from five studies) collected data on the full economic cost of palliative care including costs incurred in all settings, from the viewpoint of all providers.8,13,14,18–20,29,47 While some studies may have been conducted for a specific purpose which did not require full costs to be collected, the lack of comprehensive data on economic costs is concerning. Analysis of data from all included studies indicated that components of palliative care costs were incurred within four broad domains or settings: acute hospital care, community or home-based care, hospice care and informal care. These costs could be considered from the viewpoint of three providers: state or government, insurers/third-party/not-for-profit organisations and patient and family and/or society. Viewpoint differed significantly depending on the healthcare funding system of the country in which the research took place. Table 4 provides a framework of the core cost components which are potentially relevant in economic evaluations of palliative care and the viewpoints from which these costs can be considered.
Framework outlining perspectives of economic evaluations in palliative care and components of their related costs.
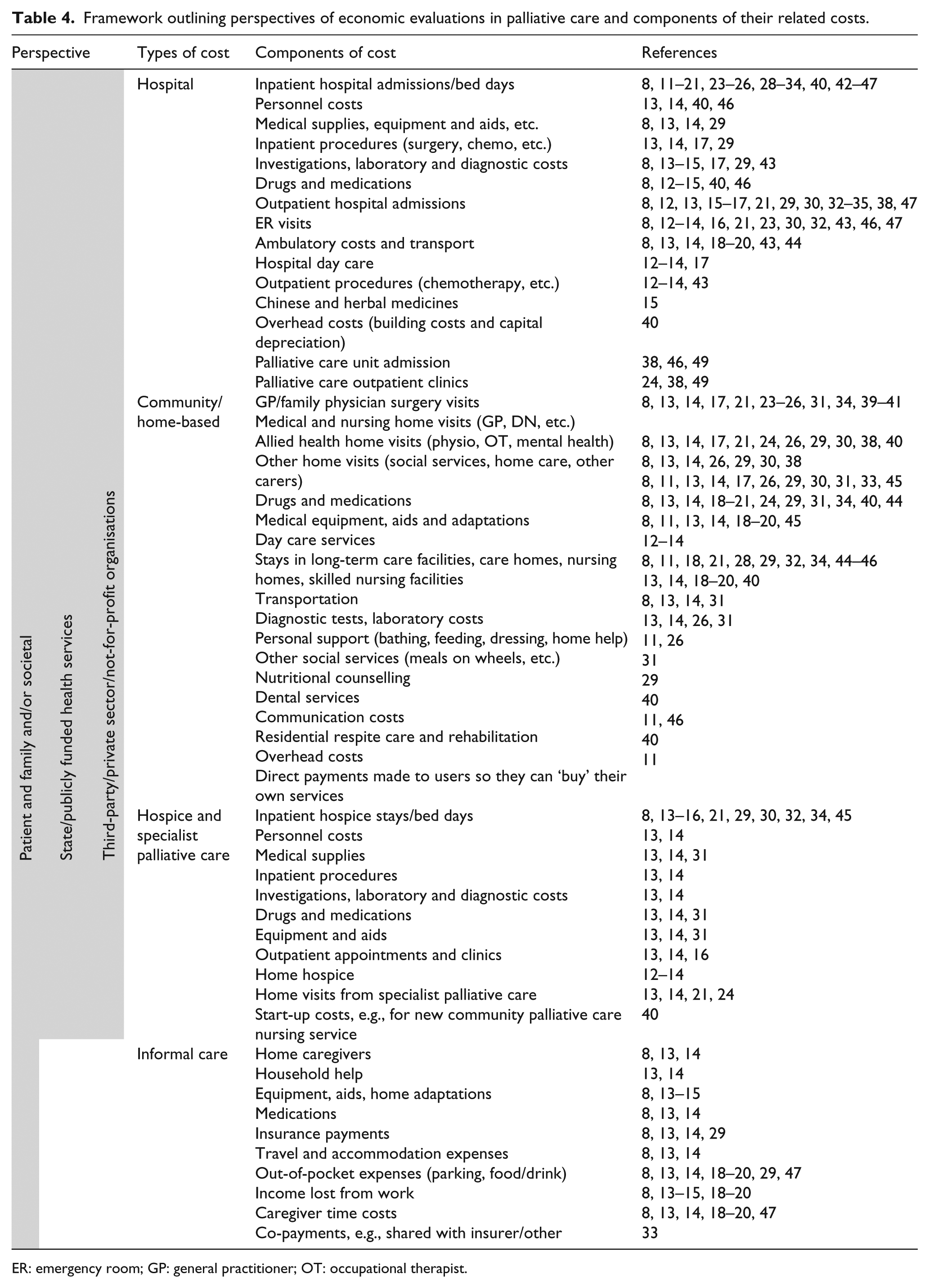
ER: emergency room; GP: general practitioner; OT: occupational therapist.
Hospital costs comprised all costs relating to inpatient, outpatient and ambulatory care in hospital. Hospital costs were the most commonly captured, reflecting the fact that hospital care tends to form the largest financial component of end-of-life care. Hospital costs included those relating to inpatient admissions, outpatient admissions, emergency room (ER) visits and ambulatory care. Some studies included country or culturally specific costs, for example, Chan et al. 15 evaluated palliative care costs in hepatocellular carcinoma in Hong Kong and included costs of Chinese medicines and herbal remedies. Only one study explicitly identified hospital overheads (building costs and capital depreciation, etc.) as a component of care costs, despite overheads accounting for a substantial 20% of the cost per patient per day in this study. 40 Community or home-based care costs comprised all costs generated through care based in the community or in the patients’ own home. These costs were numerous and there was significant heterogeneity across studies in the nature of these costs, most notably between different countries. These costs included visits and associated costs from general practitioners (GP’s)/family physicians and community nurses, and also a wide range of additional ancillary costs such as those incurred from social services, support from allied health professionals and care provided in a range of day care and residential settings. Only one study specifically included costs of mental health care. 26 Hospice care costs comprised all costs relating to inpatient and outpatient hospice care. They were broadly similar to those related to hospital care, but were usually recorded less comprehensively, perhaps as a consequence of the range and complexity of providers involved in funding hospice care and the differential definitions of hospice across the world. Costs incurred by patients and their families were included in only a small number of studies.8,13–15,18–20,29,47 Some of these costs represented direct costs to patients and family (i.e. direct outlays of money or out-of-pocket costs); however, others were assumed or indirect costs (i.e. income lost through illness or caregiving, or caregiver time costs). None of the included studies attempted to capture costs relating to lost productivity from the perspective of employers.
Description of costing approaches used to derive costs
A wide variety of costing approaches were used to derive costs. These approaches varied significantly between different countries, largely dependent on the differing funding mechanisms for health care. For example, studies from the United States commonly utilised Medicare and Medicaid insurance claims’ data to calculate costs relating to palliative care.29,16,27,34,44,45 Medicare and Medicaid are national social insurance programmes which provide health coverage in the United States. Using Medicare or Medicaid data to calculate costs has the advantage that claims’ data represent the true cost to the insurer, and not a proxy or derived cost. However, it should be acknowledged that while claims’ data provides an accurate cost estimate, this only represents a narrow viewpoint for analysis as it fails to capture costs to third-party providers, patients/families or society. The apparent complexity of capturing truly comprehensive cost data is reflected in the fact that only one study from the United States attempted to describe costs that included both Medicare and non-Medicare expenditure. 29
In contrast, studies from the United Kingdom calculated costs using more diverse methodologies, due to the complex arrangement of commissioned publicly funded health services. For example, UK studies generally calculated hospital costs on the basis of national ‘tariffs’.11,15,17,24,38 A tariff is the cost attached to a grouping of healthcare units of similar resource need (a currency) and represents the cost paid by the commissioner not the actual cost to the healthcare provider. 50 Approaches to deriving community and hospice costs were based on data which are generally considered to be even less accurate. UK community costs were commonly derived from nationally available ‘Unit Costs of Health and Social Care’. These unit cost estimates are calculated by the Personal Social Services Research Unit drawing together a range of routine data and research to provide estimates of national unit costs. 51 Estimates of the cost of hospice care in the United Kingdom are perhaps the most difficult to determine, with National Health Service (NHS) and voluntary sector providers funded in a variety of different ways. Georghiou and Bardsley 22 attempted to calculate hospice costs based on national data but acknowledged ‘our estimate of the costs of hospice care at the end of life was based on crude aggregated measures of national hospice care use’ (p. 29). In addition to significant national differences in the way costs were calculated, differences were sometimes noted at a regional level. In Canada, for instance, unit costs for hospitalisation are agreed regionally by federal health authorities and differ, for example, between Ontario 47 and Alberta 18 meaning different costing approaches are required even within a single country.
Approaches to capturing costs incurred by patients and their families were particularly complex as these costs are split between direct outlays of money (out-of-pocket costs) and indirect or assumed costs related to lost income from work or caregiver time. The collection of data on direct costs usually relied on patient or caregiver self-report of actual costs,8,13–15,18–20,29,47 an approach that provides a ‘true’ cost but is susceptible to error and recall bias. In cases where participants were unable to recall an actual cost, Dumont et al. 18 obtained an estimate by taking the average cost of the same item as provided by other participants. Approaches to capturing assumed or indirect costs were more complex. Chai et al.,13,14 Yu et al. 47 and Guerriere and Coyte 8 used the human capital approach which assigns a monetary value to caregiver time using costs estimated from census data on average earnings. Dumont et al. 18 used a similar approach whereby caregiver time costs were obtained based on an average monetary value attributed to household work in Canada for men and women.
Description of data collection tools
In general, the tools used to collect cost data were developed on an ad hoc basis for individual studies and were not standardised or validated tools. For example, Dumont et al. 18 developed their study questionnaire through the Delphi procedure and generated questions in line with the validated Canadian Community Health Survey performed by Statistics Canada. Other authors extracted administrative or claims’ data directly into study-specific protocols.12,29,27,34,44,45 The study by Guerriere and Coyte 8 proposed the use of a standardised framework for capturing costs in Canada: the Ambulatory and Home Care Record (AHCR). This tool was designed to capture comprehensive costs and was subsequently validated and used in the studies by Chai et al.13,14 and Yu et al. 47 The study by Mosoiu et al. 40 also proposed a standardised costing framework for Romania;, however this was restricted to cost elements to the public healthcare system and did not include any costs from the viewpoint of third party or patient/family and society.
Discussion
This systematic review explored which costs are potentially relevant in economic evaluations of palliative care and identified approaches to collecting, and accurately costing, palliative care data. The findings suggest that a wide range of costs can be incurred during the palliative phase, costs that can be considered in four key domains: hospital care, community or home-based care, hospice care and informal care. Findings also suggest three key provider viewpoints to consider in economic analyses: state or government, insurers/third-party/not-for-profit organisations and patient and family and/or society. However, few studies in this review attempted to capture the full economic cost of palliative care with only eight papers collecting comprehensive cost data.8,13,14,18–20,29,47 Various reasons may account for this. Studies undertaken for specific organisations such as Regulatory Authorities may be required to conform to a specific perspective. This will vary on a national basis. For instance, in England, the National Institute for Health and Care Excellence (NICE) 52 states that ‘productivity costs and costs borne by people using services and carers that are not reimbursed by the NHS or social services should not usually be included in any analyses. That is, a societal perspective will not normally be used’. It may also be reasonable to exclude certain costs if they are known to have little impact on the overall results. However, economic evaluations should be explicit about what has been included and excluded and provide justification for this.
The collection of data which captures the full economic cost of palliative care is an urgent priority. This has been highlighted in a recent report from the UK National End of Life Care Programme 53 which noted that despite the existence of a range of costing information, ‘there are no robust, agreed costs of end of life care’. A necessary prerequisite to calculating the full economic cost of palliative care is an understanding of the potential range of costs to be included in any economic analysis. Our review provides an overview of the core cost components that are potentially relevant within each of four key domains and a framework for considering these costs from a variety of economic viewpoints. The framework identifies core cost components as identified by this review but is unlikely to be comprehensive and therefore should be considered a basic framework from which to build on. The range of cost components and the viewpoint from which analyses are undertaken are also necessarily context- and country specific. For example, in countries with comprehensive health coverage, the majority of hospital costs will be covered by state or third-party providers, while in low-income countries without comprehensive health coverage these costs will often be covered by patients and their families. Our framework is designed to be wide in scope and adaptable, with the intention that researchers from countries with differing funding mechanisms for palliative care can select the most appropriate cost components and viewpoints for their needs. All the studies in this review were from upper-middle or high-income countries, 54 and there is a notable absence of data from lower income economies. Therefore, our proposed framework is likely to require further refinement to be suitable for research in low-income countries. In countries where multiple providers (agencies) are involved in the delivery of palliative care, there is likely to be a range of cost, resource and other outcomes which are potentially relevant to any evaluation. In these situations, multi-agency cost consequence analysis in which all the impacts of an intervention across different sectors (e.g. hospital care, community care, social care) are reported in a disaggregated form may be helpful. 55 This type of analysis highlights the distribution of effects across the system and allows potential economic barriers and perverse incentives to be managed.
Of particular note was the lack of studies in this review which explored costs from the viewpoint of patient and family, related to informal care. This is despite mounting evidence which highlights both the magnitude of these costs and the significant impact of the costs in terms of health and wel-lbeing.6,56,57 In a context of limited resources and growing demand for services, family caregivers are expected to shoulder an increasing burden of responsibility for palliative care provision. 58 The associated financial costs to patient and family are significant, and it is imperative that these costs are accounted for as part of any full economic costing in palliative care. Our review findings support a recent UK report on the costs of dying at home which noted ‘economic analyses should reflect the cost to family members of caring, and should consider how savings to the state can be harnessed to support carers to continue to care at home’. 58 The approaches used to capture cost data from patient and families are complex and may deter researchers from attempting to estimate these costs. Evidence suggests that these costs include both direct (out-of-pocket) and indirect costs (carer time costs, lost income, etc.). 57 While estimates of direct costs to patient and family are relatively easy to capture using self-report measures such as those employed by Dumont et al.18–20 and Chai et al.,13,14 the collection of indirect cost data is more complex. The human capital approach is often used for estimating time lost from employment; 59 this approach applies the current average wages by age and sex categories to lost labour market time. Caregiver time lost from other household or leisure activities can be valued using replacement costs based on the average hourly wage of a homemaker.13,14 The use of methods such as these enables a consistent approach to the collection of patient and family data which are easily adapted by country and/or region. However, it should be acknowledged that these approaches are subject to limitations. The human capital approach is subject to market imperfections such as gender, race and other types of discrimination. 60 In addition, both approaches generate crude population estimates of cost rather than the true cost to an individual. Finally, it should be noted that none of the studies in this review attempted to capture productivity costs, that is, productivity losses to employers. These costs should be acknowledged as an additional potential component of cost that could be considered under the societal perspective.
A wide range of approaches to capturing and deriving costs were identified in the included studies. Most approaches focused on hospital costs, which is not surprising given that inpatient hospital care is consistently identified as the most costly component of palliative care.16,18,24,29 Whatever approach is used, it is important that both unit quantities and costs/prices should be defined to ensure transparency. Approaches to capturing costs were generally specific to the country and healthcare funding system in which the study took place. The majority of the approaches are derived from North American literature; this presents a challenge to researchers from other countries as economic evidence does not transfer easily between countries or between different healthcare systems. 49 For example, it is difficult to envisage how an approach solely utilising insurance claims’ data could be usefully adapted to a country with a largely state-funded healthcare system. Despite this, international comparisons on the economics of health provision clearly have value for gaining insight into the cost-effectiveness of various health systems and models of health care. Indeed, in recent years, the emergence of high quality and comparable international health and economic data in the field of ageing has allowed economic modelling through an international comparative lens. 49 Therefore, while significant challenges still exist with the translation of health data between countries and health systems, there is clear potential for benefit if these challenges can be overcome.
Limitations
Searches were limited to English language articles so we cannot be completely confident that our searches were comprehensive. The majority of grey literature searches were from UK and North American sources; therefore, data from other countries may have been missed. Studies included in the review had variable rigour and relevance and generalisations should be considered with caution. The majority of studies in the review only included cancer patients, and findings may not be generalisable across other conditions.
Conclusion
Our review findings point to an urgent need for further research on the economic costs of palliative care. Research which captures the full economic cost should be prioritised in order to gain insight into the inter-relationships between different cost domains and different provider viewpoints and could build on the cost framework proposed here. Methodological developments are also required to generate novel approaches to data collection which provide more accurate cost estimates. These may include economic modelling approaches such as those which have recently been used to estimate costs of care in cancer. 61 While some approaches will be country- or region specific, the value of internationally comparative economic data is significant and should drive further methodological developments in this area.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical review
No ethical review was required for this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This review was funded by a Vice Chancellor’s Fellowship at The University of Sheffield.