
Abstract
Background:
Researchers report difficulties in conducting research with children and young people with life-limiting conditions or life-threatening illnesses and their families. Recruitment is challenged by barriers including ethical, logistical and clinical considerations.
Aim:
To explore how children and young people (aged 0–25 years) with life-limiting conditions or life-threatening illnesses and their families were identified, invited and consented to research published in the last 5 years.
Design:
Systematic review.
Data sources:
MEDLINE, PsycINFO, Web of Science, Sciences Citation Index and SCOPUS were searched for original English language research published between 2009 and 2014, recruiting children and young people with life-limiting conditions or life-threatening illness and their families.
Results:
A total of 215 studies – 152 qualitative, 54 quantitative and 9 mixed methods – were included. Limited recruitment information but a range of strategies and difficulties were provided. The proportion of eligible participants from those screened could not be calculated in 80% of studies. Recruitment rates could not be calculated in 77%. A total of 31% of studies recruited less than 50% of eligible participants. Reasons given for non-invitation included missing clinical or contact data, or clinician judgements of participant unsuitability. Reasons for non-participation included lack of interest and participants’ perceptions of potential burdens.
Conclusion:
All stages of recruitment were under reported. Transparency in reporting of participant identification, invitation and consent is needed to enable researchers to understand research implications, bias risk and to whom results apply. Research is needed to explore why consenting participants decide to take part or not and their experiences of research recruitment.
What is already known about this topic?
Recruitment to research with children and young people with life-limiting conditions or life-limiting illnesses is challenged by factors including limited researcher access to participants, ethical considerations and characteristics of the population.
What this paper adds?
Recruitment strategies are not consistently reported in current research with this population.
Inadequate reporting of recruitment practices limits our capacity to judge study quality, risk of bias, representativeness of samples, generalizability of results and ultimately the applicability of findings.
Greater and clearer reporting of participant identification, invitation, screening, eligibility and consenting practices is needed for research recruiting children and young people (CYP) with life-limiting conditions (LLC)/life-threatening illnesses (LTI) and their families.
Implications for practice, theory or policy
Consistent use of reporting guidelines and online supplements should be encouraged by all journals.
Introduction
There is an international need for research of all types involving children and young people aged 0–25 years (CYP) with life-limiting conditions (LLC; conditions for which there is no reasonable hope of cure and from which children or young people will die 1 ) or life-threatening illnesses (LTI; conditions for which curative treatment may be feasible but can fail 2 ) and their families. 3 Research is required to explore pain and symptom management, decision making about care and treatment, illness experience, and service development and delivery.
A number of challenges to recruitment for research with this group have been reported in the literature. 4 These include clinical considerations such as the often unpredictable course of the illnesses, 5 limited access to potential participants as a result of both logistical factors and paternalistic attitudes, 6 the perceived potential burden on participants 7 and difficulties securing ethical approval. 8 As a result, recruitment to research may be slow and selective. 7 This may affect the quality of research, risk of bias and the generalizability of findings.9,10
There is debate about when and how, and even if, CYP with LLC/LTI and their families might be invited to take part in research. 11 At the same time, there is also growing evidence that CYP with LLC/LTI and their families value opportunities to participate in research and that this can be a positive experience for them.11–13
Internationally, the culture of research is changing14,15 as the importance of establishing robust evidence for care is increasingly understood. In the United Kingdom, the National Institute for Health Research (NIHR) has established a Clinical Research Network for Children, and CYP and their families are being encouraged to share their views and participate in the design, review and conduct of research to ensure that it is valid, feasible and acceptable to potential participants.16–19
CYP with LLC/LTI are likely to receive a palliative approach to care, often alongside active treatments. 20 Interest in research on both adult and children’s palliative care is gaining momentum and guidance has been developed for its design and conduct. The MORECare (Methods of Researching End of Life Care) statement 21 provides best practice solutions specifically for planning and conducting palliative care research, as well as the reporting of attrition data. However, it appears that such guidance is not routinely adhered to and a lack of reporting of methodological information has been identified in research with CYP with LLC/LTI and their families.14–16,22
In this systematic review, we explored the reported methods of participant identification, invitation and recruitment of CYP with LLC/LTI and their families to research, conducted internationally and published over the last 5 years (September 2009 to September 2014). We wished to understand the challenges to recruitment, how these differ between types of studies, identify areas of good practice and provide evidence for areas in which improvements might be made.
Aims and objectives
We aimed to explore methods of recruitment of CYP with LLC/LTI and their families to qualitative, quantitative and mixed-methods research reported in peer-reviewed journal articles.
Our objectives were as follows:
To document the procedures for identifying, inviting and consenting eligible CYP with LLC/LTI and their families to research;
To document recruitment rates;
To identify reasons given for non-enrolment, both reasons given by researchers and clinicians for not approaching eligible participants, and those given by potential participants for deciding not to take part;
To explore whether recruitment differs between types of studies;
To explore what barriers and facilitators to research recruitment were highlighted by the authors of reviewed studies.
Methods
Inclusion criteria
Primary studies of all methodologies (quantitative, qualitative and mixed-method design) were included. Eligible studies reported research recruiting CYP with LLC/LTI (and/or their family members), were written in English and published between September 2009 and September 2014. Conference abstracts were not included. We applied the United Nations definition of ‘young people’, extending from birth to 25 years. Studies recruiting parents, grandparents or siblings of CYP with LLC/LTI were also included. The Richard Hain Directory 23 of International Classification of Diseases, 10th Revision (ICD-10) diagnoses was used to ascertain whether diagnoses could be considered life-limiting or life-threatening; where definitions were unclear, the opinion of a clinical expert in paediatric palliative care (M.C.) was sought.
Search strategy
A systematic search of the literature was performed in the following: MEDLINE, PsycINFO, Web of Science, Sciences Citation Index and SCOPUS in September 2014. A combination of indexed and free-text terms was used to reflect the three components forming the search strategy (CYP; LLC/LTI recruitment).
Descriptive terms that have been used previously by other systematic reviews24,25 relating to all stages of youth were used. Terms relating to palliative care, death, bereavement and recruitment practices were also included. The MEDLINE search strategy is shown in Appendix 1.
Data screening
Two reviewers (B.F.H. and L.J.M.O.) screened citations against the inclusion criteria. Disagreements regarding eligibility were resolved through reading full text articles and discussion.
Data extraction
The data extraction tool was piloted by B.F.H. and L.J.M.O., and minor adjustments were made. We sought to extract the following from each study: research design, recruitment location and setting, funding source and type of body providing ethical review, sample characteristics, and numbers of participants screened, identified as eligible, invited to participate and consented. We also extracted reasons for the non-invitation of eligible participants and reasons given by eligible participants for non-participation. Data were extracted independently by one of four reviewers (B.F.H., L.J.M.O., V.V. or B.C.). A sample of data extracted by each reviewer was checked for accuracy and consistency by another reviewer.
Where data that we wished to extract could not be found in the article, we categorized this as ‘not reported’. No attempts were made to obtain this information by contacting the authors. We did not assess, alongside data extraction, the overall quality of each study using recommended checklists as we wished to explore the quality of reporting of recruitment information, rather than quality of the research itself.
If provided, descriptions of researchers’ experiences of recruiting participants were also extracted. We were interested in strategies employed by authors that aimed to facilitate recruitment and any issues encountered which hindered the recruitment processes. This information was usually found in the discussion section of the included papers. These data were not available in all reviewed studies.
Data analysis
Quantitative analysis
We used descriptive statistics to summarize the type of studies included, the recruitment strategies employed and the recruitment rates achieved. If we had found sufficient levels of reporting of items of interest, we planned to conduct comparative statistical analyses to assess differences in recruitment rates between (1) studies with different types of aims, such as intervention studies and psychosocial studies and (2) studies using different participant invitation methods, for example, an invitation letter in comparison to inviting participants in person.
Qualitative analysis
Any text specifically on researchers’ experiences of recruiting their sample was identified and analysed. We applied thematic synthesis as outlined by Thomas and Harden 26 and described in Langford et al. 27 to these informal data. Thematic synthesis is an adaptation of thematic analysis and can be used to pool qualitative data across different studies. Three stages of the recruitment process were used as a coding (grouping) framework: (1) identifying or screening participants, (2) inviting or approaching them to participate and (3) obtaining consent. Codes relating to the barriers and facilitators experienced in relation to each of these stages emerged from the data. Coding was completed in NVivo 10 by one reviewer (B.F.H.) and reviewed by two further reviewers (B.C. and L.J.M.O.), disagreements were resolved through discussion.
Results
Literature search
Figure 1 presents a Preferred Reporting items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the inclusion process. Our initial search yielded 6419 citations, 215 of these met all criteria and were included in this review. Appendix 2 lists references for all included studies.
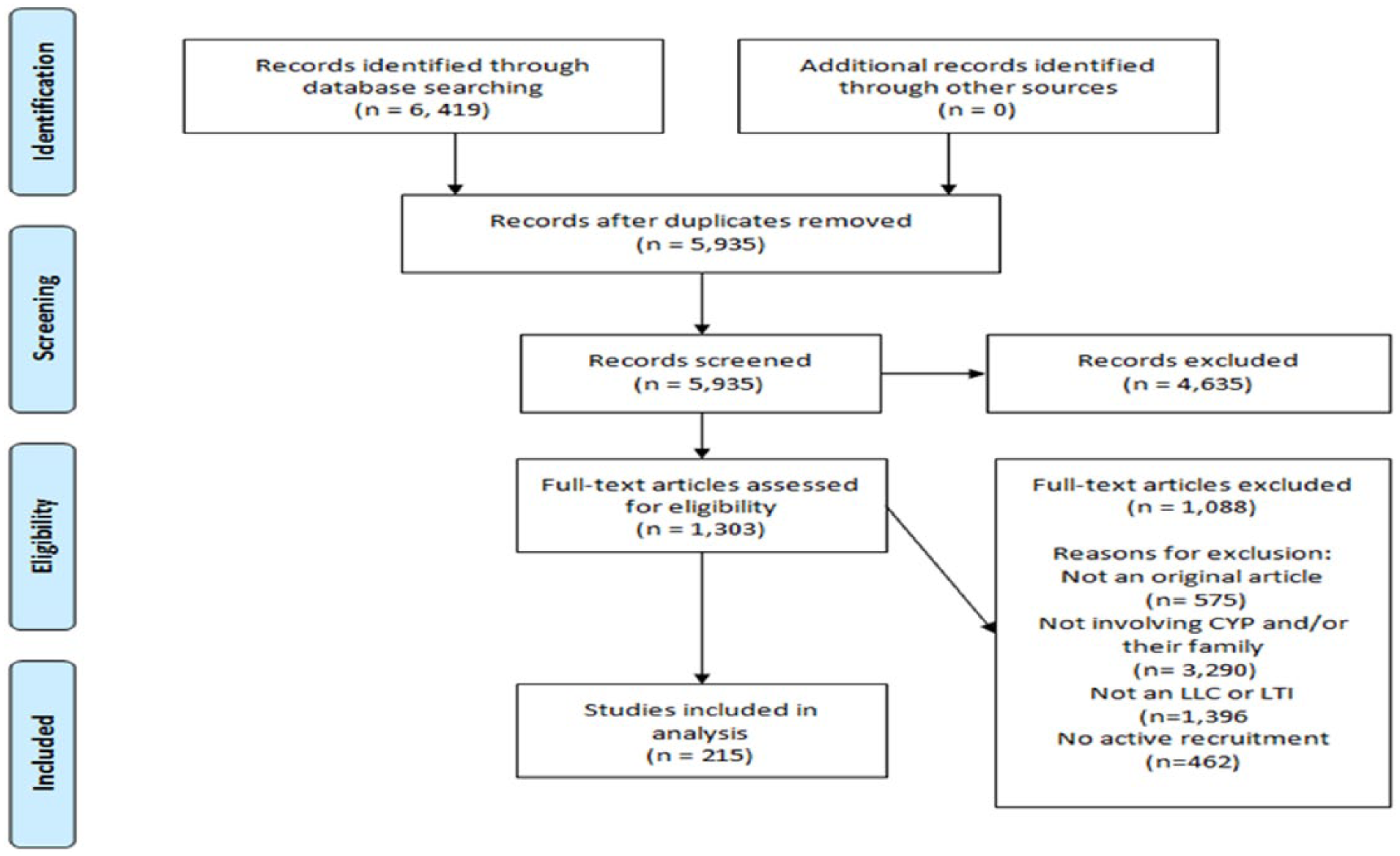
PRISMA flow diagram.
Study types
Table 1 summarizes the research aims of reviewed studies.
Research aims of reviewed studies.
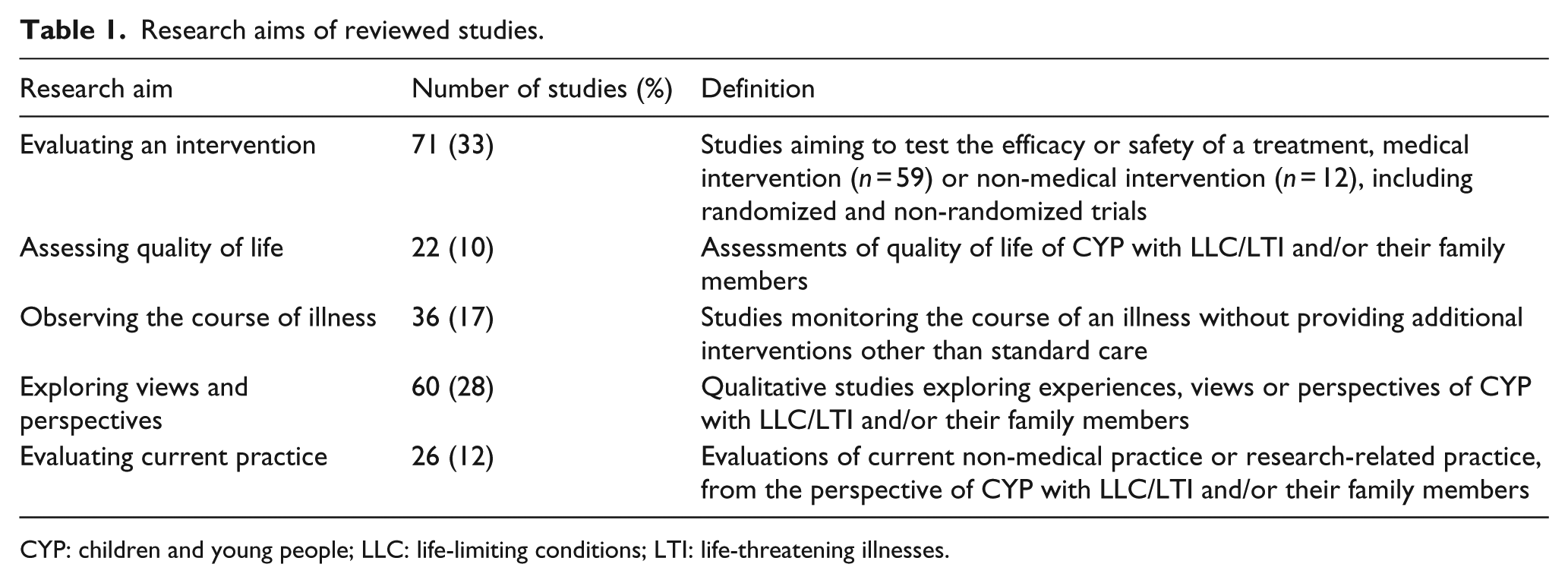
CYP: children and young people; LLC: life-limiting conditions; LTI: life-threatening illnesses.
Context and setting
Nearly half of reviewed studies were conducted in North America (46%), a quarter in Europe (26%), 10% in Asia, 7% in Australia and New Zealand, 6% in Africa, 1% in South America and a minority across multiple countries (4%). The majority of research was conducted within hospitals (83%).
Sample
Over half of studies recruited only CYP (56%), over a third recruited only family members (35%) and the remaining 11% recruited both CYP and family members. Young people aged 12–25 years were the least represented with 7% of studies recruiting this age group exclusively. The ages of CYP were not reported in a consistent manner, making descriptions of the ages of participants difficult. Ages of CYP with LLC/LTI were reported in 76% of all studies. Mean ages reported ranged from 19 min of life to 21.1 years.
CYP with malignant and non-malignant conditions were roughly equally represented (malignant: 45%; non-malignant: 44%; and both conditions: 11%). The majority of studies recruited families whose child was alive at the start of the study (79%). In almost half of the 45 studies (47%), recruiting bereaved families, recruitment occurred more than 1 year after bereavement (Table 2).
Summary of characteristics of reviewed studies, n (%).
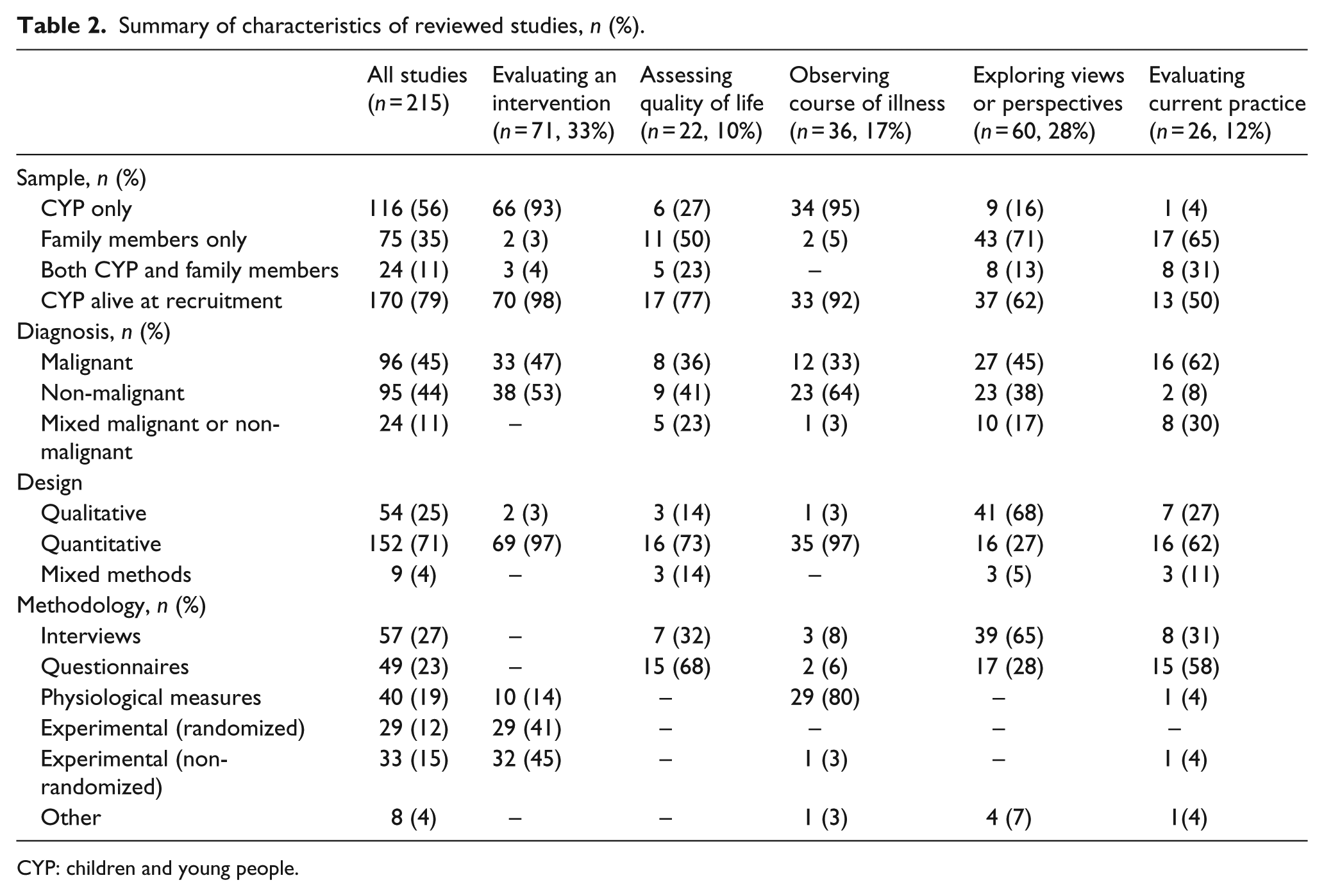
CYP: children and young people.
Study design
Most studies were quantitative (71%), 25% were qualitative, while mixed-methods studies were uncommon (4%). Over a quarter of studies (27%) used interviews, 27% used experimental methods, 23% used questionnaires, 19% recorded physiological measures and 4% of studies used other methods.
Recruitment strategies – procedures used for identifying, inviting and consenting eligible patients and their families to research
Information concerning the methods of participant recruitment was not often reported (Table 3).
Methods used for the identification and invitation of participants and details of who provided consent for participation.
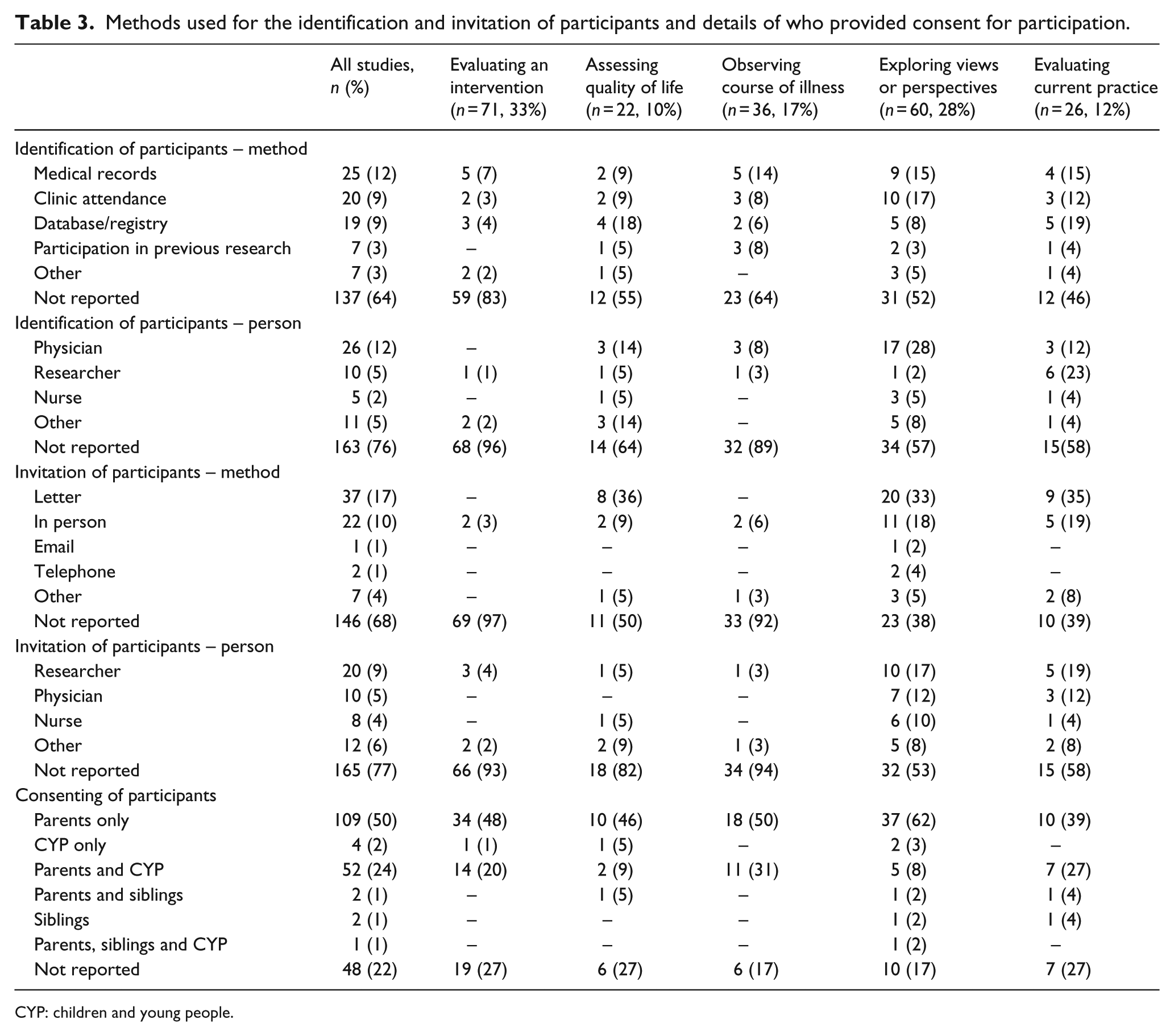
CYP: children and young people.
Identification of potential participants
Over half of the studies did not report how potential participants were identified (64%). In the 78 studies reporting this, nearly one-third identified potential participants using medical records (29%) and a quarter used clinic attendance (26%).
Less than a quarter of studies reported the person responsible for identifying potential participants (24%). Physicians identified potential participants in nearly half of the studies providing this information (48%). Studies evaluating an intervention or observing the course of an illness were least likely to report how potential participants were identified, whereas those evaluating current practice were most likely to report their methods for participant identification.
Invitation of participants
Over three quarters of studies did not report who invited potential participants (76%). In research evaluating an intervention, including treatment for disease, 96% of studies did not provide this information. In studies reporting this, it was most often a researcher (40%) or a physician (20%). Across all studies, 68% did not report the methods used for participant invitation, over half of those reporting this invited participants by letter (54%) and around a third invited participants in person (32%).
Consenting of participants
All studies required informed consent prior to participation; however, specifically who provided consent was not reported in 22% of studies. The majority of studies recruiting both CYP and their family (that provided this information) obtained CYP consent/assent in additional to parental consent (78%).
Recruitment rates and completeness of reporting
Numbers of potential participants screened and the proportion found to be eligible
The numbers of participants screened for eligibility were not consistently reported; over three quarters of studies did not report this (77%) (Table 4).
Recruitment rates, numbers of participants screened, found to be eligible, approached and consented in all studies.
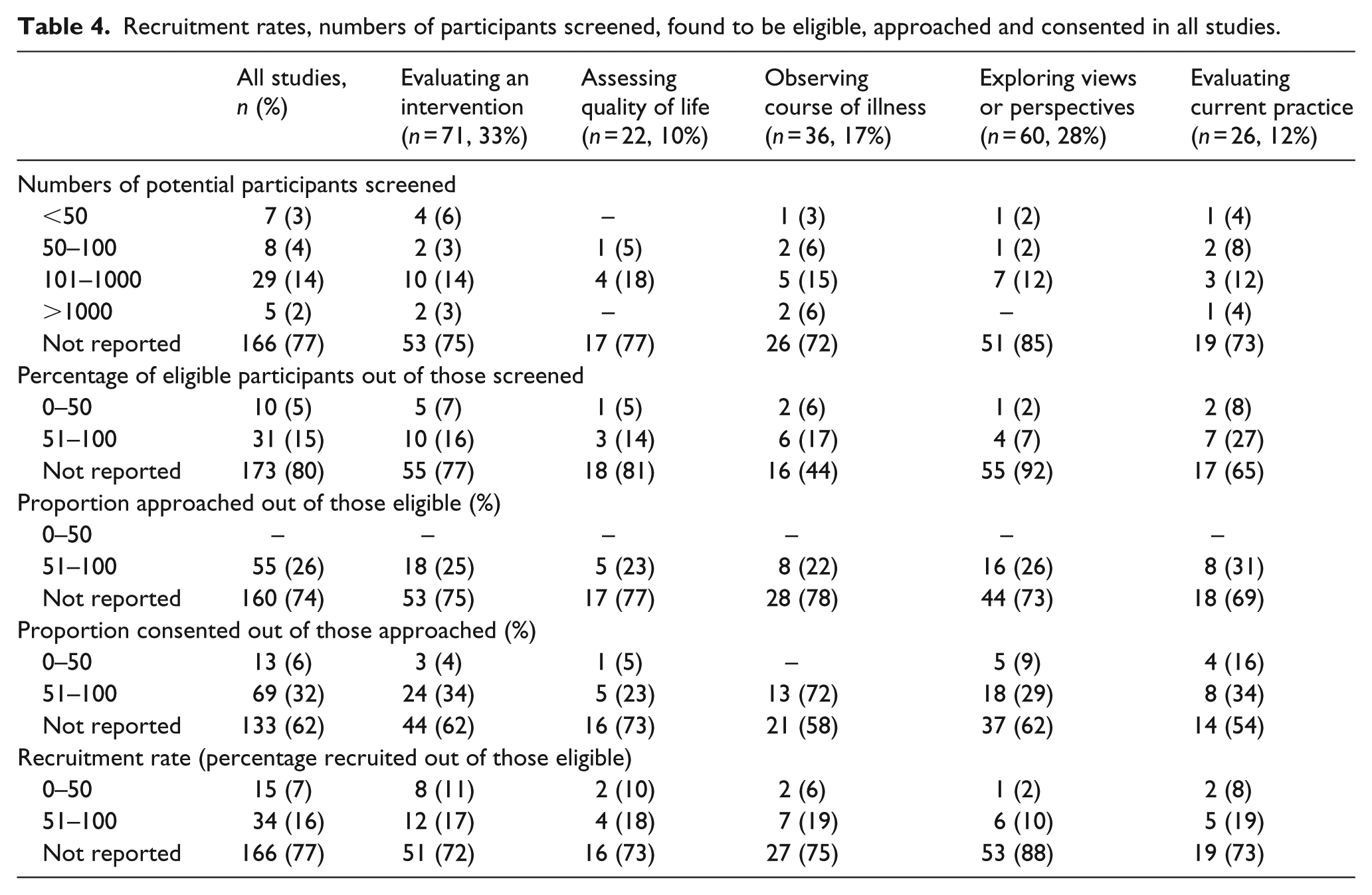
It was not possible to calculate the proportion of eligible participants out of those screened in 80% of studies. Where this proportion could be calculated, 24% found less than half of those screened to be eligible and 76% found over half of screened to be eligible for participation.
Proportion approached out of those eligible
The proportion of eligible participants approached was not reported in nearly three quarters of studies (74%). Of the minority of studies providing this information (n = 55), all approached over 50% and the majority approached between 75% and 100% of individuals eligible for participation (93%).
Proportion consented out of those approached
The proportion of eligible participants consented out of those approached could not be calculated in over half of the studies (62%). Of the 82 studies providing this information, the majority consented more than half of approached participants (84%), while 16% recruited less than half those approached.
Recruitment rate (proportion recruited out of those eligible)
Just over 10% of studies reported recruitment targets; of these, 71% met their target. Over three quarters (77%) of studies did not provide the necessary information to calculate recruitment rates. In the 49 studies where this was possible, around a third recruited less than 50% of eligible participants (31%).
Reasons for non-enrolment
A total of 19% of studies approached all eligible participants. In 7% of studies, all invited participants decided to take part. Despite the majority of studies not approaching all eligible participants, 66% did not report reasons for this and 80% did not report reasons given by potential participants for deciding not to participate.
Reasons for not approaching eligible participants (non-invitation)
Of the 20% of studies reporting reasons for not contacting eligible participants, the most commonly cited were missing participant data (either clinical or contact, n = 25), judgements from clinicians of participant unsuitability (n = 14), unanticipated death (n = 13) or caregivers denying approach (n = 9). Other reasons included logistical considerations (e.g. distance participants lived from hospital, n = 7), researchers’ perception of participant unsuitability (n = 2) and communication difficulties (n = 2).
Reasons given by participants for non-enrolment (non-participation)
For studies in which not all eligible participants were recruited, 14% reported reasons given by potential participants for non-participation. Lack of interest was the most commonly reported reason (n = 10), followed by participants’ perception of practical (n = 9) and psychological burdens associated with research participation (n = 6). Personal reasons (n = 5), the child’s condition (n = 3), caregivers’ perceptions that their child needed their attention (n = 3) and refusal to consent to medical/surgical protocols (n = 1) or to randomization (n = 1) were also reported.
Researchers’ experiences of recruitment
Text regarding researchers’ experiences of recruitment were extracted from 58 studies (26%). This was coded thematically in relation to stages of participant recruitment.
Identification of potential participants
The unpredictable course and nature of illnesses and differing institutional policies and practices across research sites were reported as barriers to the identification of potentially eligible participants in four studies. Strategies used to facilitate the identification of eligible participants included widening inclusion criteria (e.g. changing the number of years since bereavement 28 ) or seeking support from lay steering groups (‘The parent advisors had particular interest in improving palliative care services and programs and volunteered to assist’ 29 ).
Invitation of participants
Perceived barriers to the invitation of potential participants included gatekeeping from both professionals (‘staff … often chose not to approach families where the child was at the end of life’) and parents (‘In most cases the mother received the initial telephone call … This evolved as another layer of gatekeeping’ 9 ). Logistical factors such as being unable to contact potential participants were also reported as barriers (‘Many young people were not consistently engaging with medical services and hence did not have the opportunity to be invited to take part in research’).
Strategies used to facilitate invitation and recruitment processes included considerations of the method and timing of invitations (‘6-24 months after bereavement was chosen to facilitate recall whilst being sensitive to the emotional requirements of parents’), outlining participants’ options during the invitation period (‘Providing opportunities for parents or formal carers to be present during meetings was welcomed by both the young people and parents/formal carers’ 30 ) or providing monetary incentives.
Consenting of participants
Barriers to obtaining consent included overcoming participants’ attitudes or preconceptions towards research (‘Some parents felt that their son/daughter would be unable to participate as they were either non-verbal or had severe learning disabilities’ 30 ), logistical factors and CYP characteristics (‘Symptoms such as fatigue can keep children in critical condition from participating in research’ 31 )
Methods found to facilitate the consenting process included incorporating a degree of flexibility (‘Rather than press for a decision on participation, they [participants] were advised they would be contacted after a week or so to discuss the study further’ 32 ), the attributes of the research team (‘Recruitment to the study depended on the appointment of an appropriately qualified and experienced research officer’ 9 ) and attitudes of potential participants (‘The majority of families treated in other hospitals … approached the physician themselves to discuss the possibility of an autopsy for research aims’ 33 ).
Discussion
This review explored systematically how CYP with LLC/LTI and their families have been identified, invited and consented to research, internationally, in the last 5 years.
Statement of principle findings
The majority of reviewed studies did not describe the methods employed in the identification, invitation or consenting of participants or the numbers considered or approached at each stage of the recruitment process. The lack of reporting observed that the proportion of eligible participants recruited (recruitment rates) could not be calculated in over three quarters of studies. This hindered our exploration of differences in recruitment practices between different types of research and to identify areas of good practice.
Where such information was available, we found that the documented reasons for non-invitation included missing clinical or contact data, or clinician judgements of participant unsuitability. The documented reasons for eligible patients deciding not to take part included lack of interest and participants’ perceptions of potential burdens.
The observed lack of reporting practices has implications for the interpretation and generalizability of the current evidence base underpinning the care and treatment of CYP with LLC/LTI and their families. Research with this population is open to the potential for bias for a number of reasons, whether this is due to characteristics of the population, the environment in which it is conducted or the different parties involved in their care. Without knowing who was considered and ultimately included or excluded from research, we cannot be sure that the results obtained are valid, generalizable and relevant for the populations that we are interested in. Moving forward research needs to be reported transparently in order for readers to be able to draw their own conclusions about how to use the information available.
Relationship with previous research and current reporting standards
Clinicians were most often reported to be responsible for the identification of potentially eligible participants and there is potential for this process to be influenced by clinician gatekeeping. As 80% of reviewed studies did not report how many screened participants were identified as eligible, we cannot expand further on this based on the findings of this review.
Strategies to overcome barriers to the invitation of participants reported included obtaining advice from steering groups and parent advisory committees. This is in line with current guidance advocating for the involvement of patients and the public in research design and conduct. 16
Guidance and standards are in place for the conduct and reporting of research 34 including the CONSORT (Consolidated Standards of Reporting Trials) statement, 35 the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) guidelines, 36 STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines 37 and for research with palliative populations, the MORECare Statement.21,38
While the CONSORT statement asks authors to provide information about the numbers of participants screened, identified as eligible and to provide reasons for excluding participants, not all journals require authors to follow reporting guidelines. Indeed information required by the CONSORT is not consistently reported in paediatric randomized controlled trials.39,40 This lack of adherence to guidelines could go some way to explaining the inconsistencies and inadequacies of reporting evidenced in this review.
The impact of inadequate reporting in research
Much research conducted with CYP with LLC/LTI and their families acknowledges its limited generalizability, but fails to report precisely to whom the research is generalizable to. Without the provision of more transparent information about the recruitment of CYP with LLC/LTI, it will be difficult to develop a sound understanding of the nature of barriers to research and for solutions to be generated and shared.
Our objective to explore what could be learnt from current research regarding recruitment practices was limited by a lack of reporting. Such learning is important to enhance success of future projects, thereby reducing waste and unnecessary exposure of CYP to suboptimal practices. Inadequate reporting of recruitment practices limits our capacity to judge study quality, risk of bias, representativeness of samples, generalizability of results and ultimately the applicability of findings. This has worrying implications for the policies which are underpinned by the current evidence base.
Strengths and limitations
The lack of reporting about recruitment processes meant that while we were able to conduct a narrative synthesis of the data, and a thematic synthesis of text from the discussion section of included papers provided, it was not possible to conduct an analysis of the association between research aim, recruitment strategies and recruitment rates.
We recognize that one potential explanation for the lack of information about recruitment processes may be related to journal constraints and word limits. In addition, for some variables, such as reasons for non-participation, researchers may not have access to this information, or may not have had the ethical approvals to collect and record data on non-participation. Nonetheless, the rate of recruitment reporting is lower than we had anticipated.
Our review was limited to studies published in English over the last 5 years, which may have introduced the potential for a language or publishing bias; however, studies from a range of countries were included. We restricted ourselves to the last 5 years for both practical reasons (limited resources) and in order to focus on the most current reporting practices. We did not include studies with mixed populations (studies recruiting CYP with LLC/LTI plus healthy controls or professionals involved in their care). Given the uniqueness of this population, we wanted to focus exclusively on CYP with LLC/LTI and their families. We are unable to comment on the reporting of recruitment practices in studies recruiting more heterogeneous populations.
The inclusion and analysis of informal data in systematic reviews are not common but have been successfully implemented in a few pioneering studies.27,41 Informal evidence provided a richer, fuller picture of recruitment than formal evidence alone. However, as relevant text was extracted from just over a quarter of reviewed studies (26%), the potential for biases within the data reviewed exists.
A potential criticism of this review could be the grouping of both medical (e.g. drug trials) and psychosocial studies under the research aim ‘evaluating an intervention’. We acknowledge that requirements and methodologies of studies within this category vary, yet these are the only studies for which there is the potential for direct physical participant benefit. The majority of studies within this category evaluated a medical intervention and from the data reported, there appears to be minimal differences between research with different aims in terms of recruitment methodologies used and recruitment rates achieved.
Recommendations for reporting of recruitment
In order to strengthen the evidence base and inform the development of future research and policies to improve the care and treatment of CYP with LLC/LTI and their families, greater clarity is needed in the reporting of research conducted with this population.
Future research should endeavour to provide transparent accounts of participant recruitment. In order to achieve this goal, we would urge authors to report recruitment methods and practices and we would encourage journals to make this part of the manuscript submission requirements. The use of online supplementary material facilities should be used where authors are constrained by word limits.
Implications for future research
Based on the content of recently published papers, we cannot judge the impact of different recruitment strategies or the extent of impact of the barriers reported due to the inadequacies of current reporting practices. Explorations of the effectiveness of different identification, invitation and recruitment strategies and the impact of flexibility in recruitment may serve to strengthen the evidence base and advance the care and treatment of CYP with LLC/LTI and their families. Further reviews of existing literature, including studies with mixed populations (those recruiting CYP with LLC/LTI plus healthy controls or professionals involved in their care), could prove illuminating.
This review has pooled the experiences of researchers’ recruiting CYP with LLC/LTI and their families to research in an attempt to explore recruitment practices employed, barriers encountered and steps taken to overcome them. Expanding this approach and further drawing upon both researchers’ and participants’ experiences and expertise could enable solutions to be generated, developed, implemented and shared among the research community. Researchers’ recommendations for facilitating the recruitment of this population spoke to the importance of listening to the views and preferences of potential participants with regard to research participation, and accommodating these preferences where possible.
We cannot presume to know what constitutes an unacceptable burden to research participation from the perspective of CYP with LLC/LTI and/or their families. Providing consenting participants, in research of all designs, with the opportunity to share their reasons for deciding to participate, and their views on what constitutes a burden or barrier to research could provide meaningful and useful insights into the research experience of this population and could inform the development of future research design and recruitment.
Footnotes
Appendix 1
Appendix 2
Acknowledgements
The authors acknowledge Margaret Comac (advice regarding whether diagnoses could be considered life-limiting or life-threatening), Lizzie Chambers (advice on interests and concerns of organizations using data about CYP with LLC/LTI and/or their families), Doug Hall (PPI), Kate Hall (PPI), Thines Ganeshamoorthy (PPI) and Grazia Manzotti (assistance with search strategy).
Author contribution
B.F.H. designed and ran the search strategy, screened the articles, extracted data, analysed the results, drafted and approved the final manuscript as submitted. L.J.M.O and B.C. designed the search strategy, screened the articles, extracted data, analysed the results, reviewed the manuscript and approved the final manuscript as submitted. V.V. designed the search strategy, extracted data and approved the final manuscript as submitted. L.J., M.L., M.B-L. and P.S. conceptualized the study, reviewed the manuscript and approved the final manuscript as submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: B.F.H.’s post is supported by The Health Foundation (grant code G25 512881 2LAAB), L.J.M.O.’s post is supported by Great Ormond Street Children’s Charity (G25 513947 2LGC), M.B.-L.’s post is supported by funding from The True Colors Trust (grant code G25 511830 2LGA), M.L. was supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRCs) North Thames at Bart’s Health NHS Trust. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. B.C., V.V., L.J. and P.S.’ posts are supported by Marie Curie core funding to the Marie Curie Palliative Care Research Department, UCL, grant MCCC-FCO-11-U.