
Abstract
Background:
The new World Health Organization’s ‘End TB’ strategy specifies palliative care within its strategic pillars. Limited data on patient-reported problems are available to inform an effective care response.
Aim:
We aimed to (1) identify most burdensome problems, (2) compare intensity of problems for drug-susceptible and drug-resistant tuberculosis and (3) identify predictors of problem identifiers.
Design:
Cross-sectional self-report quantitative study.
Setting/participants:
Self-report palliative care problems (physical, psychological, social and spiritual) were collected among patients on admission to a general district hospital with tuberculosis and multidrug-resistant tuberculosis wards in South Africa.
Results:
Totally, 114 patients were recruited. The items with worst score responses were worry (60.5%), pain (42.1%), help and advice to plan for the future (35.1%), symptoms (29.0%) and ability to share feelings (25.1%). In ordinal logistic regression, age was predictive of a higher (worse) score for total Palliative Outcome Scale total score (0.058, 95% confidence interval = 0.0018–0.099, p = 0.005) and Factor 2 (interpersonal wellbeing: 0.038, 95% confidence interval = 0.003–0.073, p = 0.031). Interestingly, multidrug-resistant tuberculosis was predictive of lower (better) score for both total Palliative Outcome Scale score and Factor 1 (physical and psychological wellbeing). Weight, human immunodeficiency virus status and prior treatment were not significantly associated with any of the three.
Conclusion:
Currently, patients with drug-susceptible tuberculosis are only admitted to hospital with complications, explaining their worse scores. The high burden of physical and psychosocial problems experienced by our sample provides strong evidence of the need for palliative care alongside potentially curative options.
This original study was implemented to address the absence of evidence identified in our prior review. The evidence was systematically reviewed and updated on 28 November 2015. The search terms such as ‘tuberculosis’, ‘TB’, ‘palliative’, ‘hospice’, ‘terminal’ and ‘end-of-life’ were combined within PubMed and MedLine, and no new primary evidence was identified.
The new World Health Organization’s (WHO) STOP TB strategy names palliative care as a required component of care, but there is no current evidence of the nature or severity of palliative care needs.
This WHO strategy includes palliative care in two of its three pillars. However, to date, no data have been generated on patient-reported palliative care needs to inform an effective clinical response.
This study addresses the global health challenge of tuberculosis (TB). Given the dropout from treatment, the difficulties in managing drug-resistant TB and TB-related mortality, a recent evidence-based declaration and policy have called for improved access to palliative and end-of-life care.
It identifies the self-report problems of drug-resistant and drug-susceptible TB patients, and importantly shows that those admitted have a high burden of multidimensional problems.
Due to policy of forced admission of drug-resistant patients, they have a lower burden of problems than those with drug-susceptible TB.
The data reveal a high burden of worry, pain, need for help and advice to plan for the future, symptoms, and sharing feelings, each of which were scored as being highly burdensome by at least 25% of the sample.
Inpatient settings require training and skills to assess and manage multidimensional patient problems alongside attempts to treat the disease.
Introduction
In 2013, there were 9 million new tuberculosis (TB) cases, and 1.5 million deaths. 1 In total, 3.5% of new TB cases and 20.5% of previously treated cases have multidrug-resistant tuberculosis (MDR-TB), that is, resistance to at least isoniazid and rifampicin (the two most powerful anti-TB drugs). 1 In 2013, the World Health Organization (WHO) estimates that 480,000 people developed MDR-TB; 9% of these had extensive drug-resistant tuberculosis (XDR-TB which is defined as MDR-TB plus resistance to at least one fluoroquinolone and a second-line injectable). XDR-TB patients have lower successful treatment rates than MDR-TB. 2 MDR-TB has a treatment success rate of 48%, 22% not completing treatment and a 35% mortality rate. 1 South Africa has the highest TB incidence and prevalence, second highest number of diagnosed MDR-TB cases and the largest number of HIV-associated TB cases. 3
Palliative care is needed for those who may die from their TB infection,4,5 especially XDR-TB. 6 The new WHO End TB strategy calls for palliative care to achieve zero suffering, 7 advocating ‘access to palliative and end-of-life care’. 8 We aimed to measure palliative care-related problems among patients with both drug-susceptible and drug-resistant TB on admission to hospital. The objectives were as follows: (1) measure intensity of physical, psychological social and spiritual problems; (2) compare intensity by drug susceptibility and (3) determine predictors of problem intensity.
Methods
Design
Cross-sectional self-report.
Setting
TB ward and the MDR-TB ward of a rural South African District Hospital, a decentralised TB and MDR-TB Treatment Centre. This setting enabled us to us to (1) determine the care needs of patients within institutions; 9 at the time of this study, people in South Africa with MDR-TB had treatment initiated in hospital 6 and those with drug-susceptible TB admitted when serious complications arise; (2) meet our goal of data implementation for improved patient care and outcomes in a defined place of care; a novel hospital-based palliative care service in South Africa achieved lower admission rates, lower length of stay and higher home-death rates; 10 and (3) South Africa has one of the highest rates of TB/MDR-TB globally, and public hospitals urgently require evidence to manage admissions.
Inclusion/exclusion criteria
Inclusion criteria are as follows: aged 18 years and older, confirmed diagnosis of TB, admitted to the hospital during preceding week and could voluntarily give informed consent. Exclusion criteria are as follows: professional nurse identified patient as not being cognitively able/too ill to respond to the study questions (using clinical judgement).
Data collection
Consecutive patients were approached. The African Palliative Care Association African Palliative Outcome Scale (APCA POS) is a brief multidimensional outcome measure of patient problems, 11 has sound psychometric properties, 12 is well reported across conditions and settings13–20 and has a stable factor structure. 18 Answers are scored using Likert scales 0–5, and patients may respond verbally or using a hand scoring system. 21 In order to standardise data collection methods among a population with varying levels of literacy, a researcher read the questions aloud in isiZulu or English and recorded responses. Self-report items are as follows: age, gender, has partner/spouse and number of children being cared for. The following data were extracted from file: weight, history of previous TB diagnoses, response to TB treatment, HIV status and whether patient was currently on antiretroviral (ART) treatment. We attempted to extract CD4 count, but as with previous research 22 we found a large amount of missing data (49.1%).
Sample size
The sample size of 114 was based on routine data on TB admissions and enabled measurement of prevalence for any single POS item with a 50% response distribution, and for comparison between TB and MDR-TB participants (using prior data of African POS data on the physical and psychological symptom factor, to detect a difference of 2.5 between MDR and XDR groups with a standard deviation of 4.13, 90% power and 5% significance, n = 114) 17 This also meets the minimum recommended ratio of 10 cases:variable 23 for the planned analysis.
Analysis
POS items were reversed as necessary, 0 = best and 5 = worst score. For Objective 1, descriptive analysis was undertaken for patient characteristics and APCA POS item and factor scores, reporting medians and interquartile ranges (IQRs). Response rate and completeness of data were also calculated. For Objectives 2 and 3, associations with APCA POS factors were identified using ordinal logistic regression. Three models were constructed, each with the dependent variable of an APCA POS factor (rather than using a total score, which could potentially mask variations between domains). First, univariable analyses were conducted with POS factor scores entered as tertiles. As ordinal logistic regression provides a cumulative odds ratio, the independent variables’ relationship to the dependent variable were first explored in contingency tables to determine a uni-directional association with ordinal/continuous independent variables, then entered as follows: age (continuous covariate), gender (factor, two levels of male/female), drug resistance (factor, two levels of drug resistant/drug susceptible), weight (continuous covariate), HIV status (factor, two levels of positive/negative), whether patient has a partner (factor, two levels of yes/no), whether patient has children (factor, two levels of yes/no) and prior TB treatment (factor, two levels of yes/no). ART current use was not entered due to collinearity with HIV status (84.5% of HIV + patients were on ART). Following each univariate analysis, multivariable models were constructed (independent variables entered into the multivariable model if significant at the 25% level). 24 Model fit was evaluated using likelihood ratio χ2 test, estimate (log odds regression coefficient) and 95% confidence interval, Nagelkerke pseudo-r2 as a measure of variance and score test of parallel lines to determine assumption of proportional odds held. Cases with missing data were excluded. Ethical approval was granted by University of Cape Town’s Faculty of Health Sciences Human Research Ethics Committee (220/2012) and provincial KwaZulu-Natal Research Committee (HRKM69/12).
Results
Sample characteristics
In all, 46 patients were excluded, n = 136 were invited to participate (response rate: 83.8%), the planned sample of n = 114 consented (see Table 1).
Sample characteristics (n = 114).
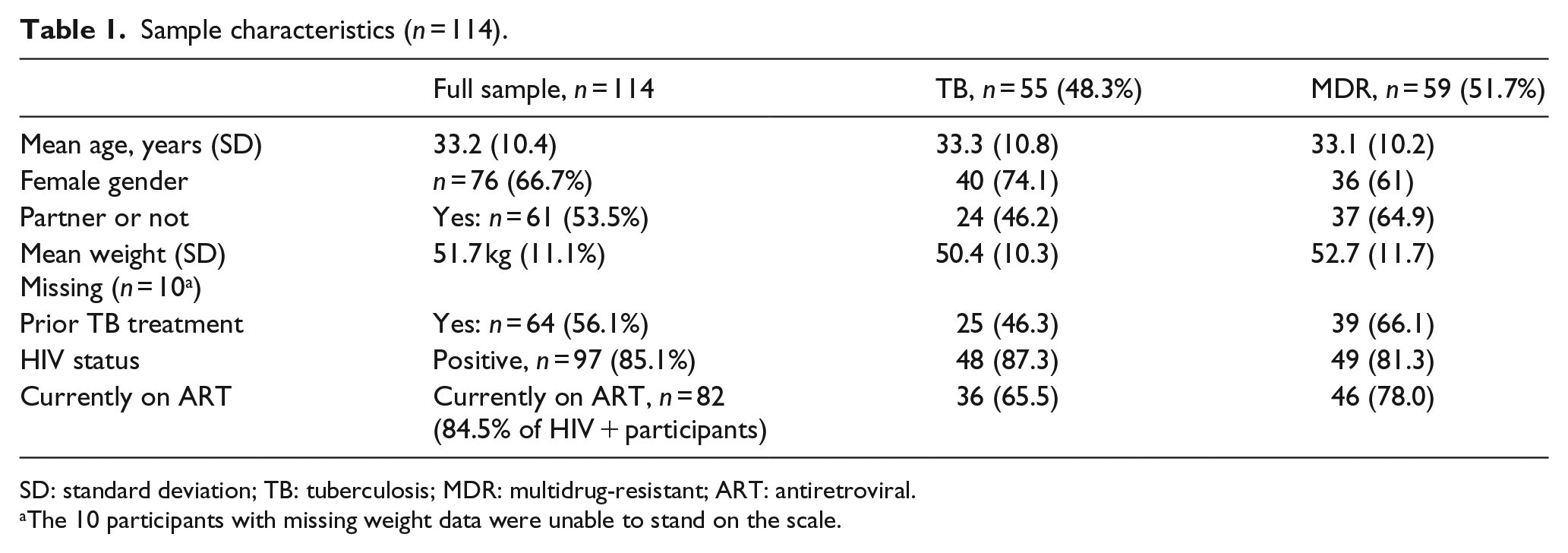
SD: standard deviation; TB: tuberculosis; MDR: multidrug-resistant; ART: antiretroviral.
The 10 participants with missing weight data were unable to stand on the scale.
Patient problems
The problems with worst median scores were worry, pain and other symptoms (see Table 2). In terms of clinical importance, items with worst score responses (i.e. at least a quarter of the sample scored 4 or 5 in the possible range of 0–5) were worry (60.5%), pain (42.1%), help and advice (35.1%), symptoms (29.0%) and sharing feelings (25.1%).
Baseline APCA African POS scores for full sample of patients with drug responsive and drug-resistant TB, reporting previous 3 days (n = 114).
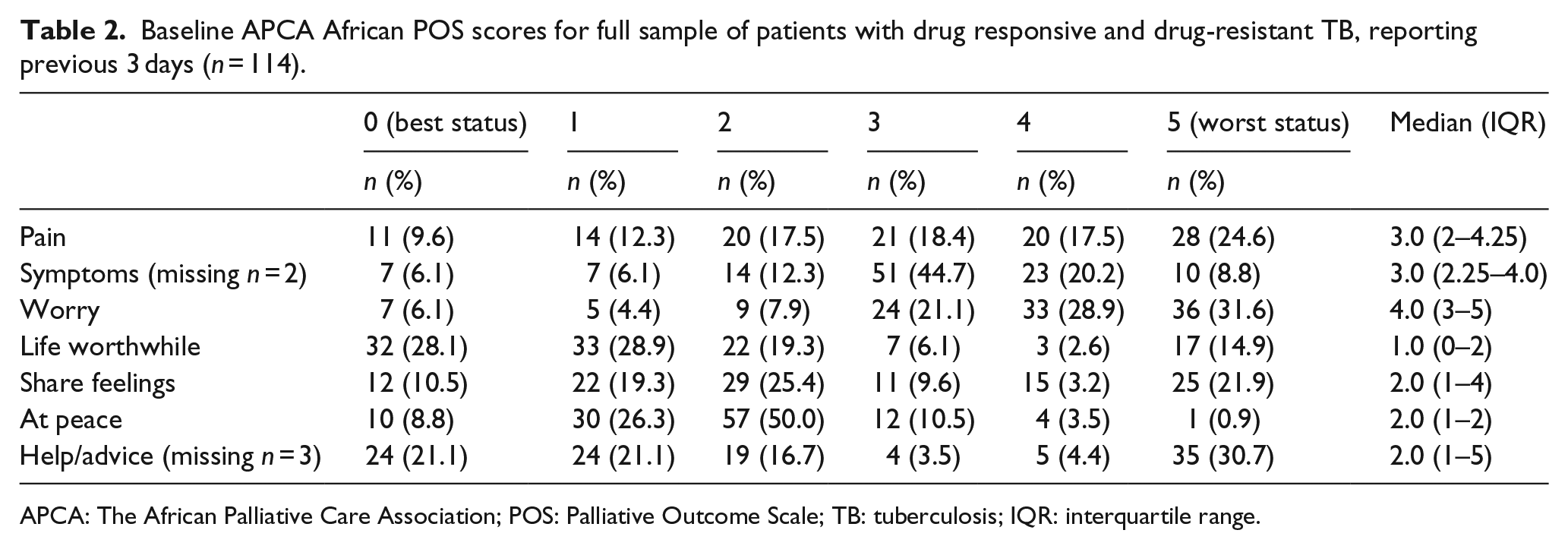
APCA: The African Palliative Care Association; POS: Palliative Outcome Scale; TB: tuberculosis; IQR: interquartile range.
Following univariate analysis (Table 3), in multivariable models (Table 4), age was predictive of a higher (worse) score for total POS score and Factor 2 (interpersonal wellbeing). Interestingly, a diagnosis of drug-resistant TB was predictive of lower (better) score for both total POS score and Factor 1 (physical and psychological wellbeing). In contrast, weight, HIV status and prior treatment were not significantly associated with any outcome.
Univariate association with the POS total score, and POS factors as dependent variables.
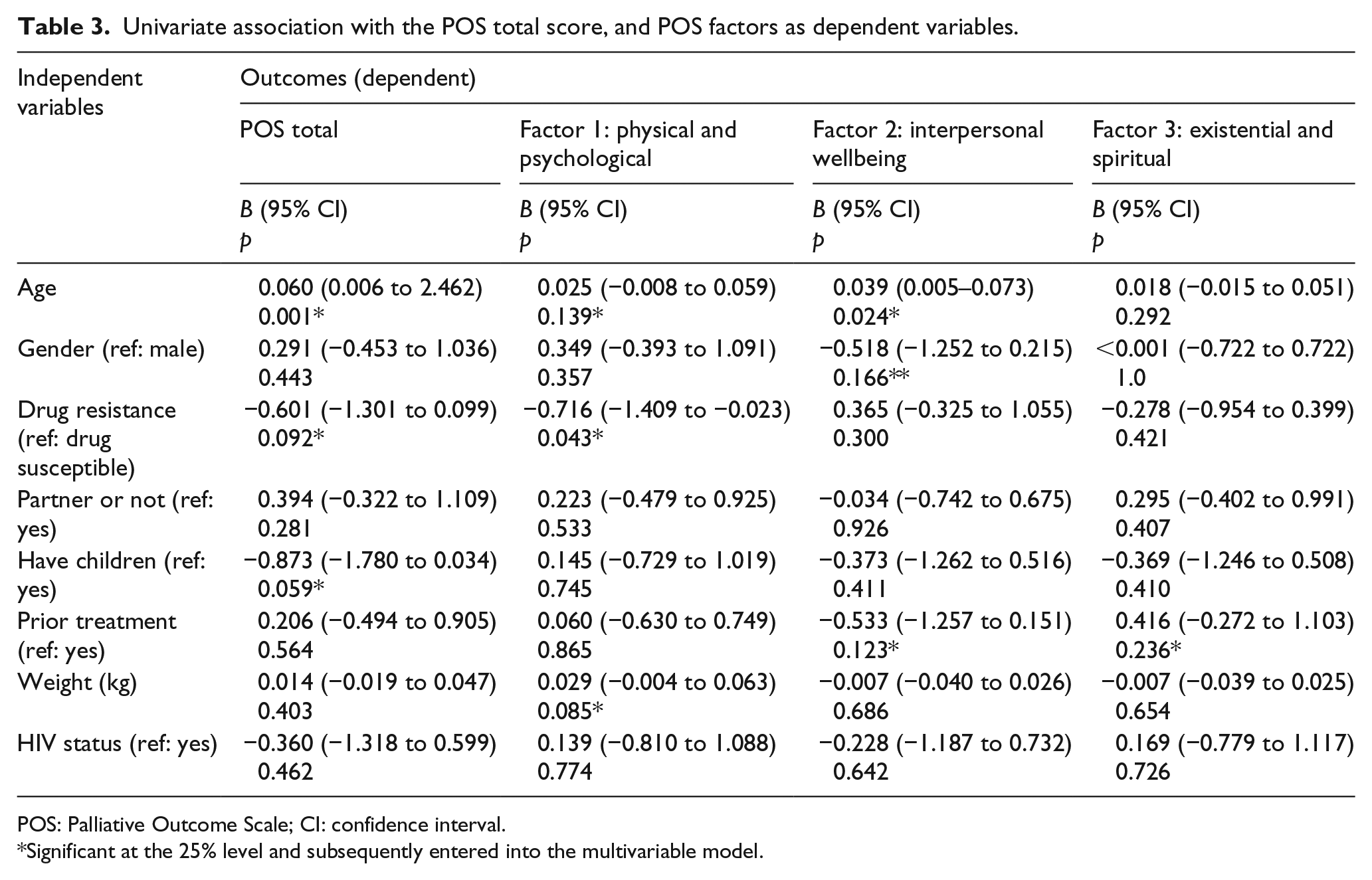
POS: Palliative Outcome Scale; CI: confidence interval.
Significant at the 25% level and subsequently entered into the multivariable model.
Multivariate analyses for total POS score, and POS factors as dependent variables.
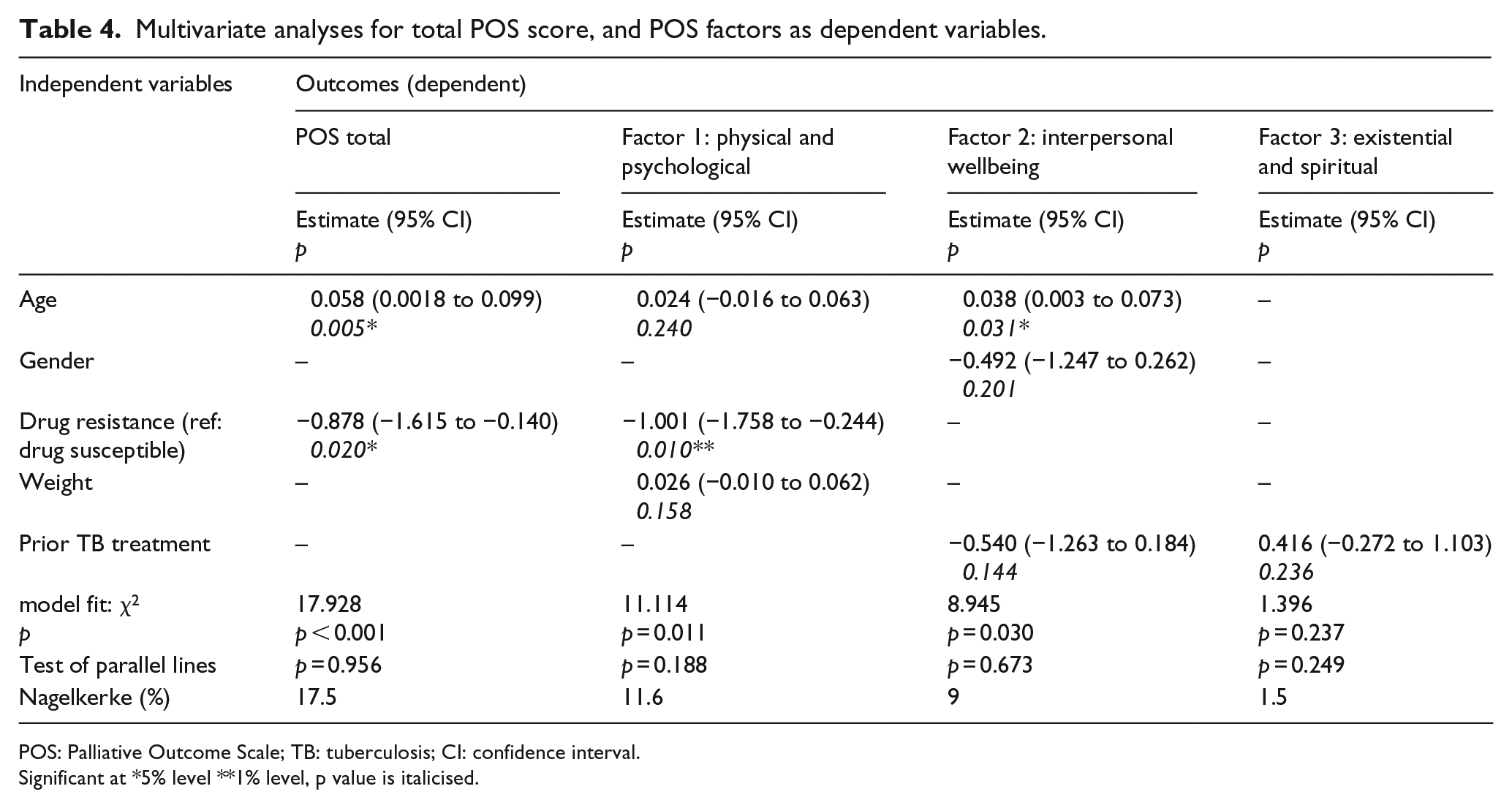
POS: Palliative Outcome Scale; TB: tuberculosis; CI: confidence interval.
Significant at *5% level **1% level, p value is italicised.
Discussion
This study is the first to report palliative care–related problems of TB patients. The most burdensome problems were worry, pain and symptoms. Help and advice to plan and ability to share feelings were scored in the worst response categories by 31% and 22%, respectively. The significant physical and psychological problems experienced by patients with both TB and MDR-TB confirm the need for person-centred, holistic palliative care currently proposed for MDR-TB.4,5 The worst score related to ‘worry’, requiring assessment and management of psychological wellbeing. In all, 79.8% had childcare responsibility. These children become extremely vulnerable when orphaned, and traditional African models of surrogacy may no longer be feasible. 25 Psychosocial support is also important for management of adverse events related to TB treatment,26,27 and education, counselling and encouragement support treatment adherence. 27 Optimal psychosocial care for those with HIV disease continues to be a priority alongside prevention and treatment; 28 the provision of TB medical care focused solely on the technical elements of treatment would be suboptimal.29–31
Admitted patients with drug-susceptible TB had more severe pain, symptoms and worry than those with drug-resistant TB. Therefore, those admitted with anticipated positive treatment outcomes also require access to palliation. A community-based assessment of palliative care-related problems experienced by people with drug-susceptible TB is required to ensure problems are assessed and managed prior to admission, and to ensure continuity for those discharged. Existing community palliative care teams and hospices are well placed to provide education, training and clinical support to hospital teams. 6 Training should include treatment side effects and effective communication while implementing infection control measures. 26 Palliative care and infection control for TB patients in hospital and community have both been successfully provided in South Africa.26,32
There are a number of limitations to our data: (1) sampling bias through exclusion of those too ill participate may have led to underestimation of problems; (2) exclusion of children due to lack of a validated measure although this is in final stages of validation; 33 (3) no data on potentially confounding variables of functional performance or time since admission/treatment; (4) interviews were within 7 days of admission and improvement may have already taken place although prior study suggests a slower response to these complex problems; 34 (5) relative contribution of comorbidities is not known although palliative care should be delivered according to needs, not diagnosis.
The suffering experienced by TB patients should be relieved26,35 This study responds to requests for evidence of palliative care problems.4,5 Prior evidence of effectiveness of HIV palliative care (for whom TB is common) demonstrated significant improvements for the problems reported by our sample. 29 Recent trial evidence also found effectiveness for quality of life, psychiatric morbidity and psychosocial problems among HIV patients on treatment. 28 Therefore, effectiveness of palliative care for TB patients is plausible. Our novel data should inform care delivery to support the guidelines for providing palliative care to patients with TB 26 and the specification of palliative care within the WHO TB Strategy.
Footnotes
Acknowledgements
The authors thank the Wolfson Foundation for providing KD with a bursary. They also thank South Coast Hospice (SCH) for providing professional back-up in terms of the distress protocol and for the professional time of Francisca Dladla (FD) an experienced Zulu-speaking palliative care nurse who fulfilled the role of research assistant. Thanks also to the Hospice Palliative Care Association of S Africa for reimbursing SCH for FD’s time. They are especially grateful to the participants who gave their time and data freely and to the staff in the busy TB wards.
Author contribution
K.D. conceived, designed and conducted this study. R.H. provided academic supervision and input at all stages of design and reporting, and conducted the analyses. D.C. provided clinical academic mentorship during the study and contributed to the design and interpretation. All authors contributed to the drafting and approval of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.