
Abstract
Background:
Residents living in long-term care facilities are a vulnerable population. For many residents, a nursing home is their place of death. Palliative care and end-of-life decisions are important components of their care provision.
Aim:
To study the views of cognitively able residents and relatives on advance care planning, end-of-life care, and decision-making in nursing homes.
Design:
A qualitative study with in-depth interviews with nursing home residents and focus group interviews with relatives of nursing home residents. Analysis is based on interpretive description.
Setting/participants:
In total, 43 informants from nine nursing homes participated in the study (25 nursing home residents and 18 relatives). All included residents had capacity to provide informed consent and lived in long-term care.
Results:
The main findings of this study were the differing views about decision-making and advance care planning of residents and relatives. Residents do trust relatives and staff to make important decisions for them. The relatives are in contrast insecure about the residents’ wishes and experience decision-making as a burden. The majority of the residents had not participated in advance care planning. None of the residents stated challenges connected to end-of-life care or mentioned the wish for euthanasia.
Conclusion:
Although most residents seem to be satisfied with decision-making and end-of life care, there is a need for systematic advance care planning. Advance care planning could help to explore future wishes for care and ease decision-making for the relatives, physicians, and staff and should be offered to all cognitively able nursing homes residents.
Keywords
Many people die in nursing homes.
Nursing homes provide palliative care at the end of life.
Systems for advance care planning (ACP) and inclusion of residents and relatives in end-of-life decision-making are unsatisfactorily implemented in many nursing homes.
Residents trust their relatives, physicians, and nurses to make decisions for them, but in contrast many relatives do not know for sure what their next of kin really wants.
Talking about death and dying in general and especially about the residents’ preferences for treatment and decision-making in end-of-life care are paramount and should be addressed by the staff in order to maintain autonomy and dignity.
Although some nursing home residents stated a wish to die, none expressed the wish for euthanasia or physician-assisted suicide.
Physicians and nursing home staff should engage in ACP and offer the opportunity to discuss death, dying, and wishes for care and treatment at the end of life with nursing home residents and when the resident agrees with their next of kin.
Although most residents and relatives are willing to talk about ACP, they are reluctant to start a conversation on that topic.
Most nursing home residents are unaware that ACP is an option; thus, staff should ensure to offer residents opportunities for these discussions.
Introduction
Older people often need nursing home or home-based care due to multimorbidity and frailty. 1 Across different countries, similar issues need to be addressed. For example, about 70%−80% of nursing home residents in the United Kingdom and Norway suffer from cognitive impairment or dementia.2,3 For many people, a nursing home is their place of death. In the United Kingdom, 35% of the people died in care homes or at home in 2006. 4 In the United Kingdom, between 2001 and 2010 55% of people suffering from dementia died in care homes. 5 In Norway, 48% of all deaths occurred in long-term care facilities and 15% at home in 2012. 6 There are numerous ethical challenges in nursing homes.7–9 Nursing homes are places where end-of-life care is provided. Providing end-of-life care involves overcoming various challenges. One such challenge is advance care planning (ACP). ACP is a process with discussion between an individual and a carer (relative, nurse, and physician) to ensure that the individuals’ wishes and preferences are known.10 –13 Definitions of ACP are provided in Box 1. The practice and legal framework of ACP differs between countries and may include repeated discussions with relatives, nurses and physicians; appointment of a substitute decision maker; and use of written advance directives. The use of ACP has a positive influence on the quality of end-of-life care. 11 Unfortunately, ACP is not yet widely used in nursing homes, and decision-making in end-of-life care may therefore lead to conflicts between the staff and relatives.8,14 Norwegian legislation allows relatives to consent to medical treatment if a patient is unable to make decisions. 14 Residents with capacity can decide whether their relatives shall be included in ACP and decision-making.15,16 Although some elderly Norwegians do have their wishes for future care and participation of relatives in decision-making, ACP is not standard. 15
Advance care planning—definitions.
“Advance care planning (ACP) aims to help patients establish decisions about future care that take effect when they lose capacity.” (Mullick et al.) 12
“ACP is a process of discussion between an individual and their care provider, and this may also include family and friends.” (Thomas and Lobo) 10
“ACP is a voluntary process of discussion and review to help an individual who has capacity to anticipate how their condition may affect them in the future. If they wish, they can set on record choices or decisions about their care and treatment so that these can then be referred to by those responsible for their care or treatment (whether professional staff or family carers) in the event that they lose capacity to decide once their illness progresses. ACP has three possible outcomes: a verbal or written advance statement of wishes and feelings, beliefs and values—a verbal or written advance decision to refuse treatment (ADRT) (must be written with specific requirements if refusing life-sustaining treatment- see below)—a lasting power of attorney.” (NHS England) 13
“ACP is defined as a process of discussion between an individual and their care provider, irrespective of discipline. If the individual wishes, their family and friends may be included.” (Holman and Hockley) 16
Aim
The aim of this study was to explore the views of cognitively able residents and relatives from Norwegian nursing homes on ACP, decision-making, and end-of-life care. We were particularly interested in the views on participation in decision-making and in end-of-life care.
Methods
Ethics approval and ethical considerations
This study was approved by the Regional Ethics Committee (REK Sør-Øst A, Norway, reference 2009/1339a). All participants gave their written informed consent after receiving both oral and written information about the study. All participants were informed about their right to end the interview at any time without the need to explain the reasons for doing so and without consequences.
Design
A qualitative study design based on interpretive description described by Thorne 17 was used. An interview setting with semi-structured in-depth interviews18,19 with Norwegian nursing home residents and focus group interviews with relatives of nursing home residents were conducted by the first researcher (G.B.). The focus group interviews with relatives were undertaken after primary analysis of the first 11 resident interviews. Box 2 provides an overview over the opening questions used. Reflexivity was sought through repeated comparison of the researchers’ presuppositions with the results, using critical reflection and metapositions 19 as well as repeated discussions with the co-authors about alternative interpretations of the results. We followed the consolidated criteria for reporting qualitative studies (COREQ) guidelines for reporting qualitative research (details in Table 1).
Opening questions for the interviews.
Opening questions for resident semi-structured interview
Have you thought about death and dying?
Have you talked about critical illness, death, and preferences for care at the end of life with your relatives?
Have you talked about critical illness, death, and preferences for care at the end of life with the nursing home staff (nurses or nurse aids) or your family doctor?
Have you been involved in planning for care in critical medical situations or the end of life (advance care planning (ACP))?
If you were not able to decide for yourself anymore due to disease or loss of consciousness …
Who shall make decisions for you? Are your relatives/next of kin able to decide for you? Do your relatives know what you would want?
Opening questions for relatives focus group interview
Have you talked critical illness, death, and preferences for care at the end of life (ACP) with your relative who lives in the nursing home?
Do you know what your relative would want if he or she would become critically ill?
Do you know which type of care or treatment your relative would want at the end of life?
Are you able to explain/define your relatives’ wishes if they will not be able to do it themselves anymore?
Report on accordance with the COREQ guidelines—checklist for reporting qualitative research.

Setting, participants, and sample selection
In order to ensure that the greatest possible variation of data was obtained, a purposive sampling technique was utilized. This aimed to recruit participants from a wide geographical spread and location. The participants were the same as in a previous study. 9 Tables 2 and 3 provide an overview of the participants.
Participants—nursing home residents.

In order to protect the residents’ privacy and to ensure that they can stay anonymous, the resident numbers in the table do not correspond with the numbers of the citations. One informant was excluded during the interview because of cognitive impairment.
Participants—relatives of nursing home residents.
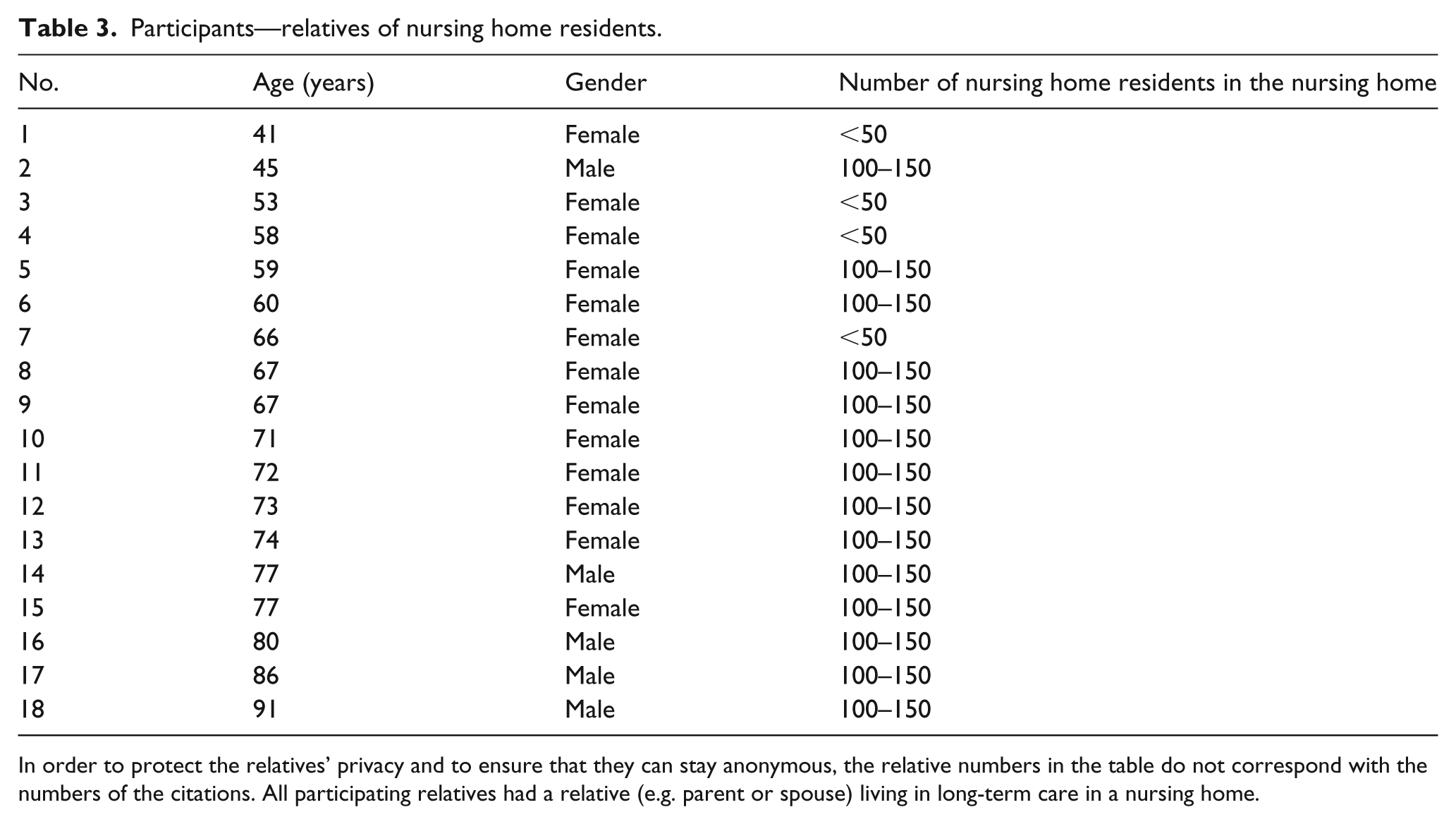
In order to protect the relatives’ privacy and to ensure that they can stay anonymous, the relative numbers in the table do not correspond with the numbers of the citations. All participating relatives had a relative (e.g. parent or spouse) living in long-term care in a nursing home.
Inclusion criteria for residents were as follows:
Capacity to provide informed consent;
Living in long-term care.
Residents with cognitive impairment were excluded. Inclusion criterion for relatives was to have a relative living in long-term care.
Nursing home staff (e.g. nurses or physicians) chose and recruited relatives and residents who were able to give written informed consent as study participants. The staff assessed cognitive function clinically without formal cognitive testing. G.B. (a specialized nursing home physician) made a secondary assessment of the resident’s capacity to give informed consent. One patient was excluded because of cognitive impairment.
The interview technique was open-ended with follow-up questions related to the participant’s answers and responses. Key themes in the interview guide were ACP, decision-making, and ethical challenges in end-of-life care in the nursing home. Data were collected from April 2010 to November 2011.
Transcription and analysis
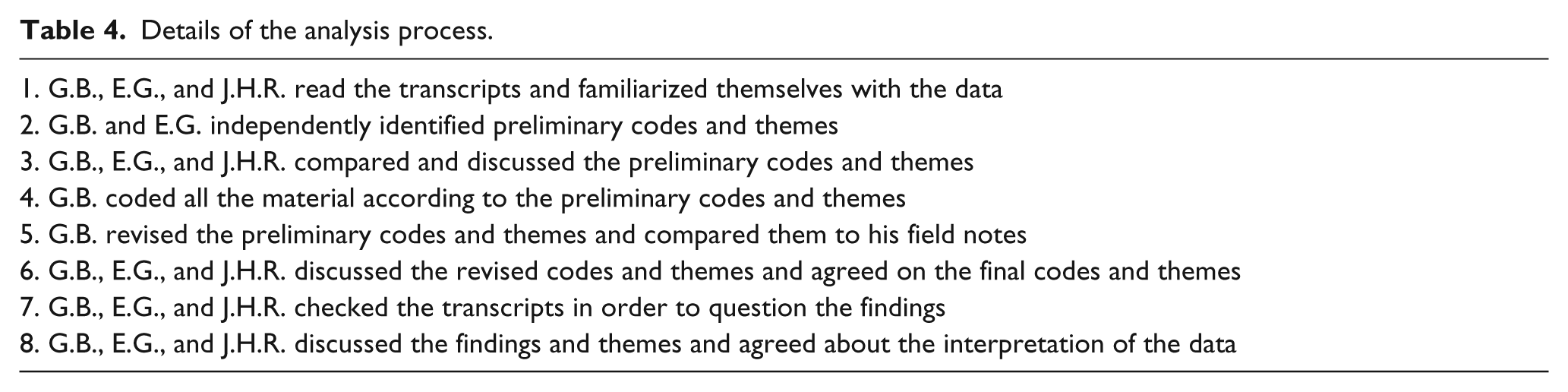
Verbatim transcription of the digital interview recordings was supported by the transcription software f4 from audiotranskription and undertaken by G.B. and two trained assistants. Analysis and coding of the transcripts were conducted systematically, in different phases, aided by the software QSR NVivo 9. A detailed description of the analysis process is provided in Table 4. Analysis of the themes found in the data material and the coded text was repeatedly performed. As a measure to validate the findings, repeated reading of the interview transcripts, in order to question the findings in the interview transcripts, and repeated discussions with the co-authors were undertaken.
Details of the analysis process.
Results
Participant characteristics
In all, 43 informants from nine Norwegian public and privately owned nursing homes representing different regions and communities of different sizes participated in the study. In total, 25 nursing home residents participated in in-depth interviews. A total of 18 relatives from three different institutions participated in focus groups. After completing three focus group interviews, data saturation was achieved. Source triangulation was used to compare views from residents and relatives. Mean age of the residents and relatives was 87 (66–100) and 68 (41–91) years, respectively. Participants’ characteristics are shown in Tables 2 and 3. The residents’ relation to the relatives was wife (2), husband (4), mother (9), mother-in-law (1), father (2) and no information (1). One relative had both parents in the nursing home. The residents’ and relatives’ views can be summarized in three main themes within a palliative care framework (Figure 1):
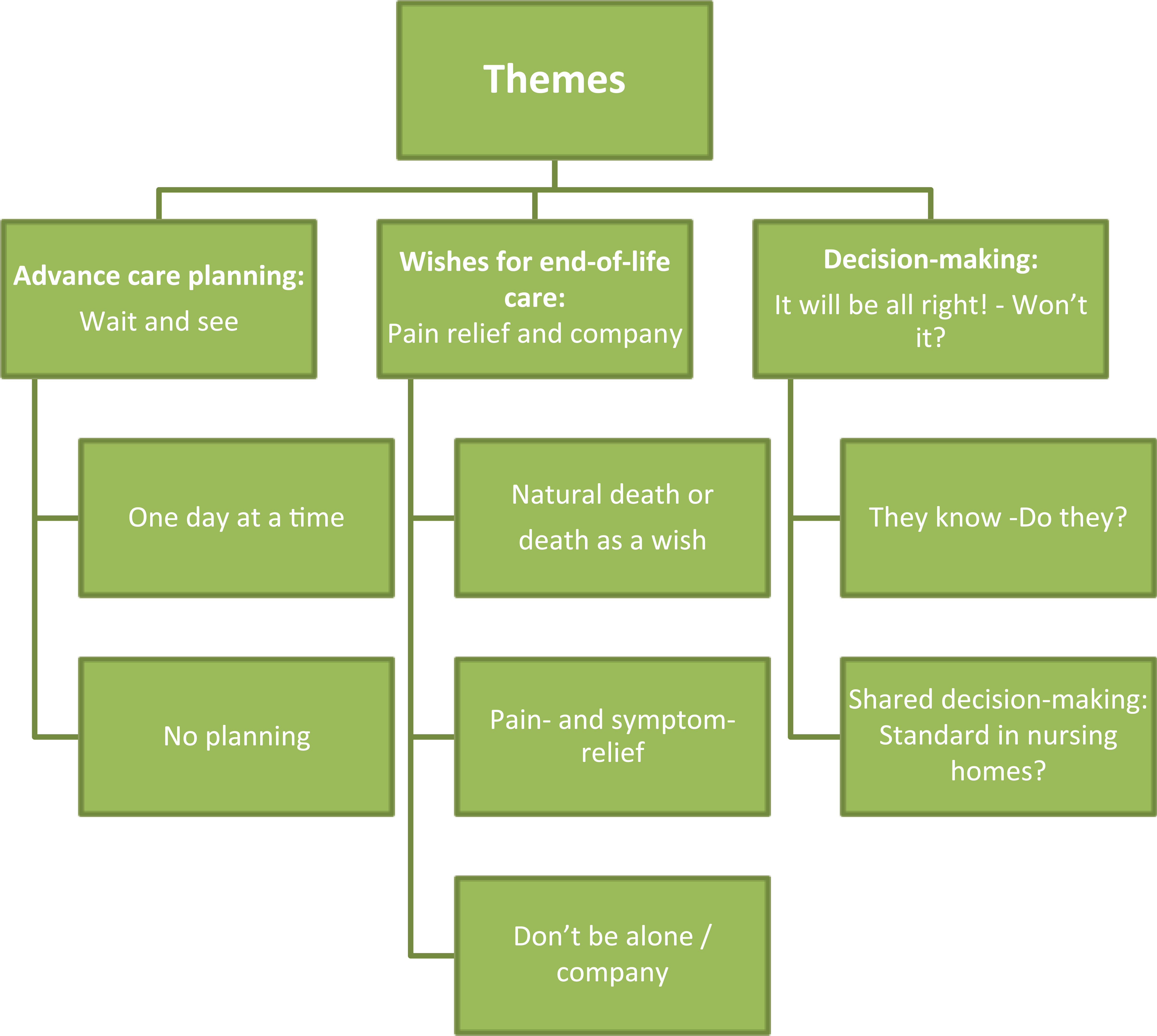
Themes from the interviews of nursing home residents and relatives.
ACP: wait and see
One day at a time
A substantial number of the interviewed residents stated that they had no concern about their coming death, and one of the residents expressed what could be representative for most residents:
I take one day at a time. (Resident 7)
Many residents stated that they had not thought about planning their future at all:
It may sound easy to say but I haven’t thought so much about death. I mean, I live now. (Resident 13)
Some residents talked about their thoughts about accepting death as normal part of life:
There are two things you know for sure: it is to be born and to die. (Resident 18)
In addition, they also talked about their ambivalent attitude to death and the ambivalence of wanting to live and wanting to die at the same time:
My wish has been: Let me die. But this can change. One day you think that you want to die but on another day (you want to live) … When you are back in a somehow normal situation where you receive care and food and (pause) you are able to read a bit and such things, then you are there in that moment at least … But it is obvious, that there are times in-between where I think that I would like … that it ended (life) … I am almost wondering, how long shall I sit here? (Resident 15)
No planning for the future means no ACP
Most residents have not been engaged in ACP. When asked whether they have talked about ACP to relatives or the staff, most answered,
No, we have not talked about that. (Resident 25)
One reason for the lack of ACP may be the lack of time to talk:
No, there is little talk about that (ACP) because they (the staff) are so busy. (Resident 18) It is not possible to talk with them (physicians and staff) about it. (Resident 3)
Or just in part,
I have talked a bit about it (ACP) with a nurse, and I appreciate to talk about death. I don’t have a problem to talk about it (death). Some people put these things aside and do not even want to think about it. (Resident 15)
A few informants talked about ACP, decision-making, and death with their relatives:
Why shouldn’t I talk about it (death and ACP)? …One is afraid … one is afraid of old prejudices, childhood believes … One is afraid to talk about such fundamental things. You don’t need to be afraid of talking about it. (Resident 24)
ACP does not seem to be important at all, although many do have concrete wishes for end-of-life care that they had not told anybody:
I haven’t thought so far … but it is pretty obvious … I would, in this case, like “a smooth passage”* between life and death. But I am not hysterical about it. (Resident 5) *“a smooth passage” was explained to be dying without pain and suffering.
Although many residents mentioned the absence of regular physician visits, some had discussed their wishes for end-of-life care with both their family and a physician:
Yes, I have talked about it (death and ACP) with my family. And I have told them very early and told the doctor too … that I would say no if they tried to keep me alive! (Resident 24)
Functional status in daily life seems to be more important than choosing between different treatment options. Some residents expressed the view that they want to participate in life and that living without consciousness and the ability to communicate is not worth living:
I don’t want to become a vegetable. (Resident 17)
Many relatives are reluctant to talk about end-of-life care and treatment decisions with the residents. It seems that many fear this topic:
I do not dare. We are too afraid to take this up (ACP). (Relgr 1/2) This (ACP and dying) is a subject that you do not talk about. (Relgr 3/4)
Therefore, many relatives do not know the residents’ wishes when decisions have to be made. One reason could be that the residents frequently use denial as a coping strategy:
I wish we had talked about it (ACP) before, but we have not. (Relgr 2/6)
In contrast, it can be experienced as a release if the relatives have talked about wishes and preferences in advance. This can positively lead to certainty about the resident’s wishes and preferences:
It was a difficult process. It really was. But I am very happy that we could talk about it (ACP), he (my husband) and me. (Relgr 2/1)
Wishes for end-of-life care: pain relief and company
Although many informants seemed to feel slightly uncomfortable talking about death and dying in the beginning, most of them were not frightened and talked openly about death as a normal part of life. Many residents had wishes for end-of-life care, but most had not communicated their wishes to the staff or their relatives.
Natural death or death as a wish
Many informants stated that, even when moving in, it was clear to them that they would die in the nursing home:
It is obvious for most people when they come in here, that this is their last stop. (Resident 15)
Some of them even expressed the wish to die:
I have said before that I would like to die. I have lived my life. I am done with life … I am not afraid to die. (Resident 20)
Some informants stated that they want to die as natural as possible:
Yes, I would appreciate a calm and natural death. (Resident 16)
Some stated that a natural death means that physicians should not prolong life without meaning:
I wish that I do not have to lie there suffering … If the physicians see that it (treatment) will not help any longer, they should not continue. (Resident 7)
In addition, many residents do not want artificial nutrition or life-prolonging medical treatment:
If it became the norm to withhold life with every technical means possible, it would just postpone that time (death) for many years. And then it is not sure that there will be quality of life … It won’t be there, I doubt it … It is just, I want to die with dignity. (Resident 24)
A feeling of control and the certainty of not being kept alive against ones wishes can enhance quality of life:
If you ask about quality of life, it may sound weird, but to know that you can end your life with dignity has something to do with quality of life. (Resident 24)
The use of life-prolonging treatment is in contrast to the wishes for a natural death of many informants. Resuscitation efforts or life-prolonging treatment, commonly, are not wanted:
I don’t want to receive life-prolonging means. I want to follow the course of nature… No life-prolonging treatment because what would it lead to? A life without living. You are more than just half-dead. Does that make sense? It does not work, it is unreasonable, its’ inhuman … to lie there … probably paralyzed and just able to stare at the ceiling … Does it make sense? No there is no sense with it… When life is fading away, you should not extend life with force. This is unnatural and uncomfortable if it will just make you live two days longer. (Resident 24)
Some of the informants seemed to be relaxed and stated that they were waiting to die:
I do know that I will die soon. That is the only thing I know … I do not know if it will be in 14 days or two years (laughs) … It cannot last much longer, I think. (Resident 14)
Some wished to die because life is troublesome, filled with waiting and suffering, and perhaps, boredom. Waiting was also part of the researcher’s own observations. The researcher observed that residents had to wait to get help from the staff on some occasions during the fieldwork:
Death can be a release, and for me it will be. (Resident 24)
None of the informants expressed the wish for euthanasia or physician-assisted suicide although several residents stated that they waited for death.
Some relatives do know that the residents’ wish would be to die and that life-prolonging treatment is definitely not intended:
I am sure that my mother often wishes to pass away. (Relgr 1/2)
Natural death can also mean to die in the nursing home instead of being sent to a hospital. In Norway, many relatives do have to decide whether the residents shall receive end-of-life care in the nursing home or whether they shall be transferred to a hospital:
This is a decision we as relatives have to make … Shall they be sent to hospital or not? … I am struggling with that decision. (Relgr 3/4)
Some relatives believe that holistic care is better in nursing homes compared to hospitals because death is more accepted. In hospitals, the intention is to save lives, and as a result, sometimes the needs of dying people are neglected:
I think it (dying) is calmer in the nursing home than in a hospital. (Relgr 3/3)
Pain- and symptom-relief
Many informants were afraid of pain and expressed their expectations to receive adequate pain relief when needed:
I have no other wishes than just to be able to die in a peaceful and quiet way without pain or other terrible things. (Resident 22)
Pain medication, as treatment in end-of-life care, is wanted by most informants and does not seem to interfere with the residents’ concept of a natural death:
There is something I am afraid of, which I don’t like to think about. That is to experience pain. I don’t want to be in pain. I don’t like it … And therefore they have told me that they will start to give me morphine injections. So that I won’t feel pain. (Resident 20)
Relatives agree with the residents that relief from pain and suffering is most important in end-of-life care:
If they only are not in pain … Yes, no pain … This is most important. (Relgr 2/5, 6) She (the resident) has made it clear that she does not want life-prolonging treatment but that we shall take care that she won’t die in pain. (Relgr 2/5)
Don’t be alone/company
Not to be alone when facing death is a frequently mentioned wish by many residents:
You need a hand to hold on to. (Resident 12)
Many would appreciate their relatives to be there:
Of course I want them (the relatives) to be there when I die. Because this is something unknown … It is not easy for us to be alone then. (Resident 25)
In addition, residents want to be able to contact relatives:
I would like to be able to talk to my relatives as long as possible. (Resident 5)
Decision-making: it will be all right!—won’t it?
Most residents trust their relatives when coming to a decision concerning treatment options, whereas the relatives feel insecure about the resident’s wishes.
They know—do they?
Asked whether the relatives knew the residents’ preferences about their wishes for end-of-life care and decision-making, most residents stated that their relatives did know their wishes:
Yes, they know how I feel. I don’t think that this will be a problem. (Resident 8)
Many relatives are afraid of making important decisions for the residents and are concerned that they do not know what to choose if being asked to decide:
I have never talked about that with my husband because he had not accepted that he was ill. So we have not talked about his wishes. And now he is not able to talk anymore … I have not been asked (to decide something for him yet), but I do see … No, this is so complicated … Sometimes I think that this is undignified as he sits there not being able to do anything. I have not accepted the situation myself (sniffles). We (relatives) become so egoistic. We want to retain them. But how can I say what is the best for him? (Relgr 1/5)
Many relatives experience it as a burden to make decisions without knowing the wishes and opinions of the residents:
I do hope that I will not have to make a decision … I do not want to decide. I cannot decide. (Relgr 1/6)
Shared decision-making: standard in nursing homes?
All residents were asked who should decide if they were incapable to decide themselves. Most of them stated that their relatives should decide:
My relatives shall decide for me. (Resident 12)
Some believed that shared decision-making is standard and that this means that relatives and physicians talk together in order to make decisions:
I suppose that the doctor and my children talk together (in order to make decisions). (Resident 14)
Many residents trust in the physicians’ ability to make decisions about their medical treatment and feel comfortable when just being informed:
You know. They (the physicians) decide. I cannot decide anything myself. But they do provide me with information first. (Resident 19)
Many residents think that the withdrawing of life-prolonging treatment is exclusively a medical decision that should be made by the doctor:
That I do not have to suffer … When the doctors see that it (life-prolonging treatment) does not help anymore, they should not carry on doing it. (Resident 7)
Treatment decisions were often seen as “purely medical decisions” by residents, and although many want their relatives to participate in the decision-making, they want the doctor to decide on issues that the residents regard to be solely medical matters:
The family cannot decide everything, can they? If it is something that has to do with disease, it shall be decided by the physician. (Resident 8)
Most of the residents trust in the ability of physicians and staff to make decisions for them, but some primarily trust the nurses who know them best:
I do not think that I can decide such things. I think this has to be done by the staff … I have no contact with the doctors who work here … They are so seldom around that I hardly know them. (Resident 3)
As many residents do not have regular contact with their physician, they prefer shared decision-making by nurses and physicians:
I just trust in the ones who care for me. What they think is best. (Resident 25)
Many of the relatives seemed to be used to take over decision-making and organization of most things for the residents:
It is almost as if they hand it (decision-making) over to us. We have already taken over most things … Probably they change when they get old. Maybe they cannot bear to make decisions anymore … Uff? … They just want others to do it. They are tired of it … Maybe she (the nursing home resident) thinks that I know best (laughing). (Relgr 3/2)
Although many relatives do not want to decide alone, they want to participate in decision-making and to be heard. They prefer shared decision-making undertaken together with nurses and doctors:
But I think that it is important that one of course will be heard and that one can participate in decision-making when the situation turns up … this should be done in cooperation with the nurses and the doctor. (Relgr 1/6)
ACP has been described as an ongoing process with repeated meetings and communication. Some would appreciate regular meetings with the nursing home staff:
There should be regular meetings between the relatives and the staff at least once a month. (Relgr 1/7)
Discussion
The main findings of the study are that residents trust their relatives, physicians, and nurses to make decisions for them and that most residents believe that the relatives would know their wishes. In contrast, however, many relatives do not know what the resident wants. ACP is lacking in nursing homes.
Relatively, few people have written ACP documents: 8% in England and 10%−20% in the United States, Canada, Australia, Germany, and Japan. 20 There are guidelines on ACP and decision-making in end-of-life care in the United Kingdom13,20,21 and Norway. 22 Nevertheless, in Norway, limitation of life-prolonging treatment on the family’s request might be more frequent than the law permits. 23 Few older adults have expressed their wishes for end-of-life care and many do not talk openly about death. 24 Even if preferences had been discussed, documentation and a systematic approach are lacking.25,26 Our data show that there is a striking difference between the views of the residents and the relatives concerning the knowledge of the residents wishes for end-of-life care. The absence of ACP seems not to be problematic for the residents but may lead to psychological stress for the relatives. When decisions in end-of-life care have to be made without knowing what the resident would want, problematic situations occur.27–29 This may cause moral distress for the relatives, 28 nurses, and physicians. Challenges in decision-making, communication, or even conflicts between staff and relatives are described in the literature.8,14,27,30–32 Many relatives in our study felt that it was problematic to decide for the residents and that they tried to avoid making important health-related and end-of-life care decisions.
A systematic approach to ACP with repeated conversations is needed as many residents and relatives seem to need a third person with knowledge of the residents medical history to initiate a discussion on ACP.33,34 Both systems to involve residents and relatives in end-of-life care in nursing homes14,27,35 and training of the staff to enable them to discuss ACP are needed.36–38 Our findings suggest that residents do not oppose ACP, but that the opportunity is lacking. This is in accordance with findings from other researchers.39,40 As many residents in nursing homes have cognitive impairment, ACP discussions should be offered much earlier in their disease trajectory.41,42
The resident’s wishes for end-of-life care in our data were as follows: not to be alone, pain relief, and no life-prolonging treatment. These findings are in accordance with previous findings. 43
Although some residents talked about death as a wish or relief, none of them mentioned a wish for euthanasia or physician-assisted suicide. One possible reason for a wish to die could be the lack of subjectively felt quality of life perhaps due to lack of activities and contact. Dignity is threatened by illness and the perception of insufficient care. 44 Residents’ dignity can be supported and enhanced in many ways including dignity therapy and even by participating in research.45,46 Interestingly, most informants in our study were grateful to take part in our research and to be able to contribute.
In summary, providing residents with opportunities for ACP and talking about death and preferences for end-of-life care are paramount. Besides planning for end of life, ACP helps the residents to prepare for death 47 and can reduce moral distress for the relatives. ACP has a positive impact on quality of end-of-life care.48,49
Strengths and weaknesses of the study
G.B.’s experience as a nursing home physician and consultant in palliative medicine and thus talking regularly about death may be considered both as a strength and as a weakness of this study. It is a strength that the interviewer was comfortable talking openly about death and dying in an empathic manner. Nevertheless, it might be a risk for “going blind” to unknown aspects of the nursing home world. The researcher used metapositions and repeated reflection of his presuppositions during the interviews and analysis. The fact that many participants thanked the interviewer for talking about these matters indicates that there was an open atmosphere that enabled the informants to share their views and concerns. One possible weakness could be the selection of informants by nursing home staff to provide a positive picture of their nursing home. Most informants reported, however, both positive and negative aspects. Nevertheless, it should be noted that they represent only a small part of the nursing home residents. A limitation is the exclusion of residents with cognitive impairment due to ethical considerations.
Implications for clinical practice and future research
ACP should be initiated by healthcare workers (nursing home staff and/or medical doctors) and should be an integral part of nursing home care. It seems that most people do need a third person from outside the family to start conversations about ACP. Future research should focus on methods and communication arenas that can enable residents, relatives, and staff to talk openly about end-of-life care and to solve emerging ethical dilemmas.
Conclusion
Communication about the end of life with the residents and relatives including ACP should be routine in all long-term care facilities. In nursing homes, there is a need to talk about ACP and preferences for end-of-life care in order to enable decision-making.
Footnotes
Acknowledgements
We are grateful for all help and support by residents, relatives, and staff from the participating nursing homes and all the other people who supported the research study by different means.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research project has been financially supported by the Norwegian Extra Foundation for Health and Rehabilitation through EXTRA funds (grant no. 2008/2/0208).