
Abstract
Background:
Stronger generalist end-of-life care at home for people with cancer is called for but the quality of end-of-life care delivered by general practitioners has been questioned.
Aim:
To determine the degree of and factors associated with bereaved relatives’ satisfaction with home end-of-life care delivered by general practitioners to cancer patients.
Design:
Population-based mortality followback survey.
Setting/participants:
Bereaved relatives of people who died of cancer in London, United Kingdom (identified from death registrations in 2009–2010), were invited to complete a postal questionnaire surveying the deceased’s final 3 months of life.
Results:
Questionnaires were completed for 596 decedents of whom 548 spent at least 1 day at home in the last 3 months of life. Of the respondents, 55% (95% confidence interval: 51%–59%) reported excellent/very good home care by general practitioners, compared with 78% (95% confidence interval: 74%–82%) for specialist palliative care providers and 68% (95% confidence interval: 64%–73%) for district/community/private nurses. The odds of high satisfaction (excellent/very good) with end-of-life care by general practitioners doubled if general practitioners made three or more compared with one or no home visits in the patient’s last 3 months of life (adjusted odds ratio: 2.54 (95% confidence interval: 1.52–4.24)) and halved if the patient died at hospital rather than at home (adjusted odds ratio: 0.55 (95% confidence interval: 0.31–0.998)).
Conclusion:
There is considerable room for improvement in the satisfaction with home care provided by general practitioners to terminally ill cancer patients. Ensuring an adequate offer of home visits by general practitioners may help to achieve this goal.
There is a need to strengthen generalist end-of-life care in order to support people at home, which is where the majority prefer to die.
There is conflicting evidence regarding the quality of care delivered by general practitioners (GPs) to terminally ill cancer patients.
Obtaining patients’ and families’ views is a research priority for improving generalist end-of-life care, but population-based evidence on their views of the home care provided by GPs is scarce.
Bereaved relatives’ satisfaction with end-of-life home care delivered by GPs to people with cancer was considerably lower than satisfaction with home care by district/community/private nurses or specialist palliative care providers.
The odds of reporting high satisfaction with GP home care increased with more frequent home visits by the GP and halved if the patient died in hospital rather than at home.
There is considerable room for improvement in relatives’ satisfaction with home care provided by GPs to terminally ill cancer patients.
This is particularly important in light of efforts across countries to strengthen the role of generalist palliative care.
Introduction
The demand for palliative care has grown in response to the increasing number of people dying from serious chronic illnesses. 1 More than one in four deaths in the United Kingdom are caused by cancer (around 162,000 or 29% of all deaths in 2012), making cancer the most frequent cause of death.2,3 Advanced cancer patients form a large group among people who could benefit from palliative care, and they are the majority of people who receive specialist palliative care in the United Kingdom.3,4 In response to the rising needs and the preference of a majority of people to die at home, 5 calls have been made for a concerted international effort to strengthen generalist end-of-life care in a coordinated care model with specialist palliative care and to improve end-of-life care at people’s homes.6,7
The involvement of general practitioners (GPs) 8 in end-of-life care and the intensity of home care 9 were suggested to be crucial factors in enabling people to die at home. However, there is conflicting evidence and an on-going debate regarding the quality of care delivered by GPs to terminally ill patients.10–14 Although GPs working in countries with well-developed palliative care services were shown to be able to deliver effective palliative care, 10 patients and families reported greater satisfaction with the end-of-life care provided by specialist palliative care services.14,15 Furthermore, concerns were raised over the fact that most GPs had limited experience and training in this field and themselves expressed problems in providing end-of-life care.10,16 However, the existing data are not recent enough to assess the claim that GPs do not provide good care to terminally ill people because they were collected prior to the implementation of important initiatives in end-of-life care such as the Department of Health’s End-of-Life Care Strategy which coordinated national efforts to improve home end-of-life care and to enable people to die at home if they wish so. 7 Furthermore, only few studies examined how the quality of end-of-life care provided by GPs to patients at home compares to that performed by other health professionals.
A UK national consultation with practitioners, commissioners, academics and service user groups identified the perspective of patients at the end of life and their family carers as a research priority within efforts to improve generalist end-of-life care. 16 Measuring users’ satisfaction provides useful information about patients’ and caregivers’ perceptions of care, 17 and it aligns with wider healthcare policies advocating the inclusion of service users’ views in the evaluation of services. 18 This is particularly relevant in end-of-life care where cure is no longer possible.
The aim of this study was to determine the degree of and factors associated with relatives’ satisfaction with the home care delivered by GPs to cancer patients in the last 3 months of life.
Methods
Study design
This study is part of QUALYCARE, a population-based mortality followback postal survey conducted with bereaved relatives of people who died from cancer in four health districts in London (UK) with the aim to study quality of care in the last 3 months of life. 19 A mortality followback survey methodology is well established and recommended in the UK National End-of-Life Care Strategy, 7 and the last 3 months of life are accepted as a relevant period for studying end-of-life care.20–22
Participants
The Office for National Statistics (ONS) identified from death registrations people who had registered a death from cancer (10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes C00-D48) of people aged 18 years or over between March 2009 and March 2010. The ONS contacted these people between 4 and 10 months after the death had been registered by mailing invitation letters, the study information sheet, a questionnaire, a freepost return envelope, a reply slip to decline participation and a bereavement information leaflet. Cases were excluded if the death was registered by a coroner and if the place of death was other than the deceased’s home, a hospice, nursing home or National Health Service (NHS) hospital or if it was unknown. Because place of death was a crucial factor to the overall aim of QUALYCARE, 19 the sample was stratified by health district and place of death to include all home, hospice, nursing home and a random sample of NHS hospital deaths (if more than 150 eligible NHS hospital deaths per health district; otherwise, all NHS hospital deaths were included). Cases were excluded from the present analysis if the deceased had not spent at least 1 day at home during the last 3 months of life because we wanted to assess the relatives’ satisfaction with home care for all deceased who had the possibility of receiving home care.
Data collection
We collected the data with the mailed questionnaire. We assessed the care received by the patient at home and relatives’ satisfaction with care using an adapted short form of a questionnaire developed by Cartwright et al. 23 of which versions were used in several other surveys.12,14,21,24,25 It has shown satisfactory discriminatory power, reliability and validity. 17 As we were interested in care that was delivered to people at home, we determined whether patients were visited at home by GPs, palliative care specialists (from hospice, palliative care, Marie Curie or Macmillan or any other specialist) and district/community/private nurses. This analysis did not include telephone or outpatient contacts. By taking home visits as an indicator for home care, we were able to evaluate the different healthcare providers based on the same type of home-based contact and hence increase the comparability of the satisfaction ratings.
To assess the main outcome, the relatives were asked whether they perceived the home care delivered to patients in the last 3 months of life by GPs, palliative care specialists and district/community/private nurses, as well as the overall care at home, to be excellent, very good, good, fair, poor or very poor. We also assessed the relatives’ ratings of the communication with the GP and their views on the GPs’ competence and symptom control.
We measured the deceased’s health status at 3 months before death (EuroQoL EQ-5D) 26 and the respondent’s intensity of grief at present and at the time of the person’s death (retrospectively) (Texas Revised Inventory of Grief (TRIG)). 27 Information on the cause and place of death was provided by the ONS. We assessed the socio-demographic characteristics of the respondent and the deceased, the number of days spent at home during the final 3 months of life, and the deceased’s financial hardship (question from the British Household Panel Survey) 28 as reported by the relative.
Analysis
The analyses were conducted in IBM SPSS Statistics version 20. All statistical tests were performed with a significance level of α < 0.05. Proportional weights were applied to the sample to achieve a percentage of deaths at home, hospital, hospice and nursing home that was representative for all eligible cancer deaths identified by the ONS.
We calculated unweighted frequencies and weighted percentages for the six levels of satisfaction for each group of care providers and for care at home in general. For patients who had received care at home from all three groups of care providers, differences in ratings between care providers were analysed using the Friedman test.
We performed bivariate analyses to test the association between satisfaction with home care by GPs and several health service and non-service factors (factors that were found to be associated with satisfaction,14,18,29–31 factors for which the evidence was conflicting and factors for which we reasoned there was a rationale for a potential association). The bivariate analyses consisted of Pearson’s chi-squared tests for categorical variables (or Fisher’s exact tests if 20% or more of the expected cell frequencies were below 5) and t-tests (if normal distribution) and Mann–Whitney U tests (if non-normal distribution) for continuous variables.
Characteristics that were significantly associated with satisfaction with GP home care in the bivariate analysis were simultaneously entered in a multivariate logistic regression analysis together with the health district to control for any effects of the stratified sampling. We conducted the logistic regression with the unweighted sample, as the variable used to create the weights (place of death) was included as an independent variable in the logistic regression. 32 For both the bivariate and multivariate analyses, we dichotomised the dependent variable, satisfaction with GP home care, as excellent/very good versus good/fair/poor/very poor because we were interested in the percentage of relatives who were highly satisfied with care. In doing so, we followed the example of earlier studies on satisfaction with end-of-life care.30,31,33,34 We grouped continuous data into ordered categories: number of GP home visits (0 or 1 vs 2 vs 3 or more), age of deceased (20–64 years vs 65–84 years vs ⩾85 years), age of respondent (20–64 vs ⩾65) and days spent at home in the last 3 months of life (1–60 vs 61–92).
For each variable, the percentage of missing data was described. If it amounted to more than 10%, we tested whether it was significantly associated with the main outcome variable, satisfaction with home care provided by GPs (Pearson’s chi-squared test).
Ethics
Ethics approval for this study was granted in December 2009 by the South East London NHS Research Ethics Committee 3 (ref no. 09/H0808/85). The return of the completed questionnaire was taken as consent to participate. Even though bereaved relatives perceive benefits in participating in bereavement research,13,35,36 several measures were undertaken to minimise harm and to maximise benefits for the respondents. They were contacted a minimum of 4 months after the death of their relative which is a more cautious approach compared to other surveys (3 months). 12 All potential respondents were mailed a bereavement information leaflet produced by the Royal College of Psychiatrists, and a written protocol for dealing with participants’ queries and distress was followed. Returned questionnaires were checked for cases requiring follow-up action. If concerns arose and participants had agreed to be contacted by the researchers, they were informed about local sources of support. 19
Results
Sample characteristics
In total, 596 informants agreed to participate in the survey (39.3% response rate, Figure 1). Of these, 548 were included in the analysis as the deceased had spent a minimum of 1 day at home during the last 3 months of life. Table 1 shows the characteristics of the deceased and the respondents. Of the 548 deceased, 6% spent between 1 and 30 days at home in the last 3 months of life; 15% stayed at home for 31–60 days; and 71% spent between 61 and 92 days at home. Four cases (0.7%) were at home for only 1 day, and seven cases (1.3%) spent between 1 and 5 days at home. A comparison of responders and non-responders in the QUALYCARE study showed that relatives of patients aged 90 years or over were more likely to participate than relatives of patients aged 20–49 years. Participation was lower for respondents for patients who died in hospital than for those who died at home and for male respondents and those who were not spouses/partners or parents. 37
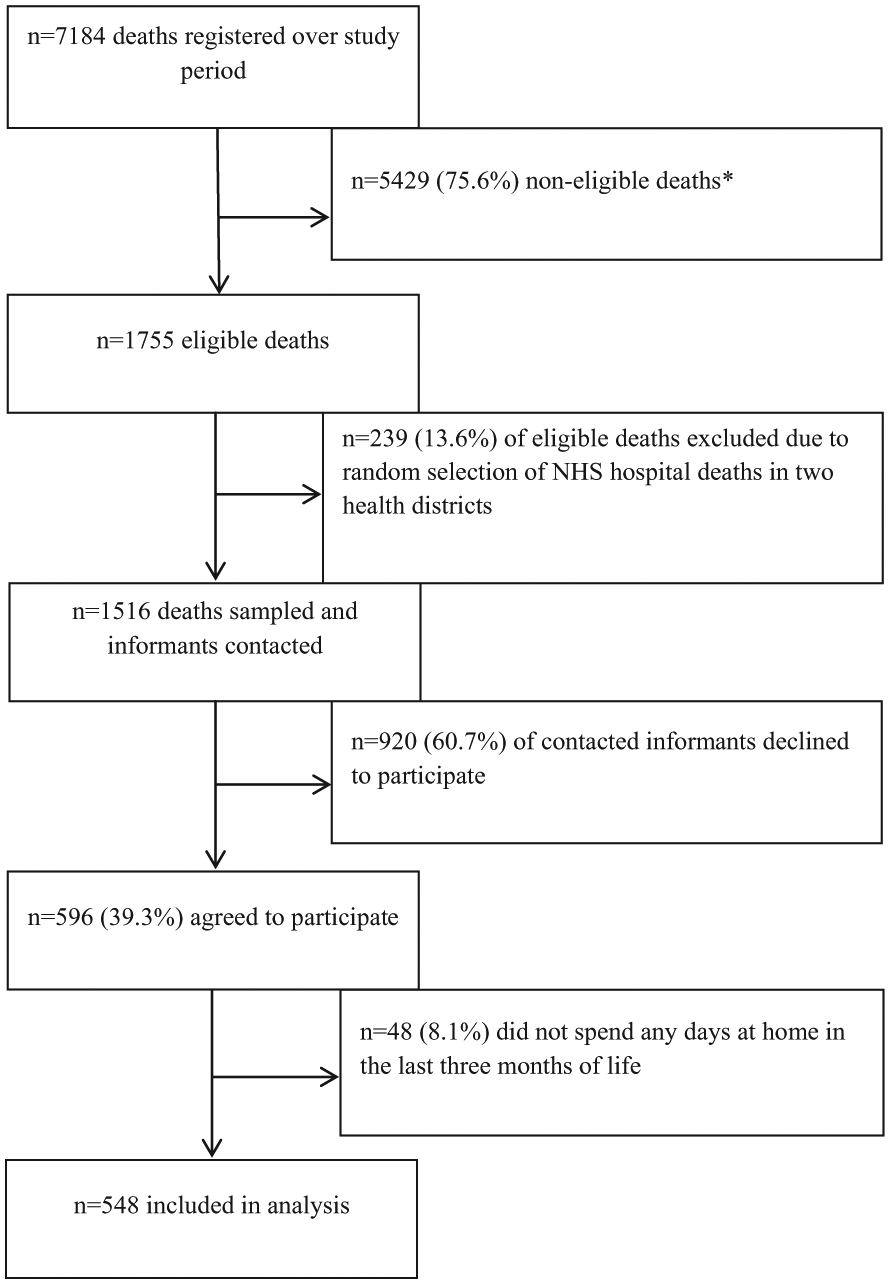
Sampling and recruitment process.
Characteristics of deceased cancer patients who stayed at home for at least 1 day during the last 3 months of life and of their bereaved relatives (respondents); N = 548.
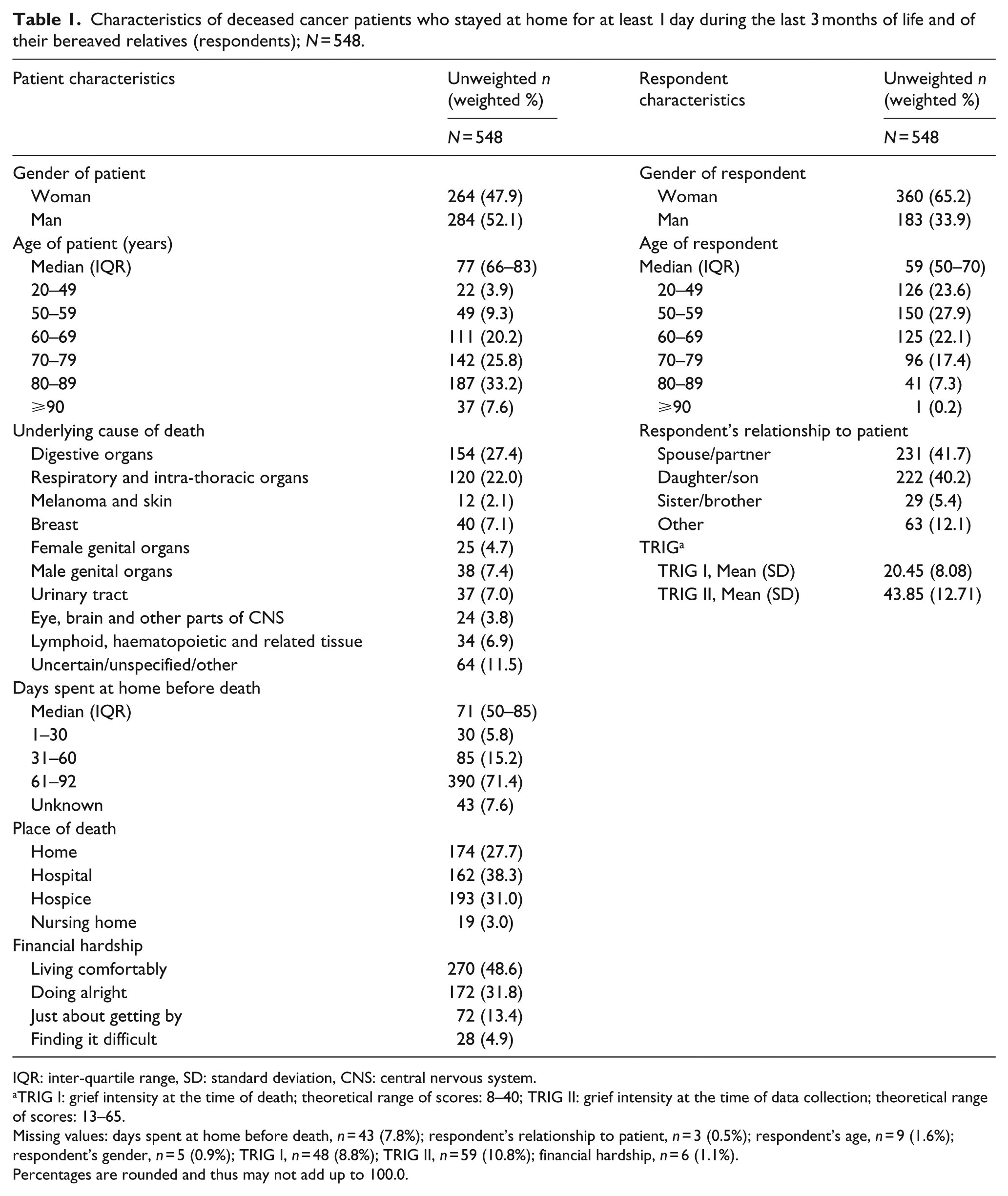
IQR: inter-quartile range, SD: standard deviation, CNS: central nervous system.
TRIG I: grief intensity at the time of death; theoretical range of scores: 8–40; TRIG II: grief intensity at the time of data collection; theoretical range of scores: 13–65.
Missing values: days spent at home before death, n = 43 (7.8%); respondent’s relationship to patient, n = 3 (0.5%); respondent’s age, n = 9 (1.6%); respondent’s gender, n = 5 (0.9%); TRIG I, n = 48 (8.8%); TRIG II, n = 59 (10.8%); financial hardship, n = 6 (1.1%).
Percentages are rounded and thus may not add up to 100.0.
Bereaved relatives’ satisfaction with home care by GPs and other health professionals
According to the respondents, all except five patients had been registered with a GP (n = 543), and 377 (69.4%) of them were visited by GPs at home at least once in the 3 months before death. Specialist palliative care providers made home visits to 385 (70.3%) of patients, and 370 (67.5%) of patients were visited by district, community or private nurses in the last 3 months of life. Around half of the bereaved relatives of patients who had received at least one home visit by a GP (54.8% (95% confidence interval (CI): 50.5–59.1)) rated the home care provided by GPs as very good or excellent (Figure 2). Palliative care specialists received very good or excellent ratings from 78.1% (95% CI: 74.1–82.1) and district/community/private nurses from 68.4% (95% CI: 63.8–73.0) of the respondents. The satisfaction ratings differed significantly between the care providers (n = 245, χ2(2) = 65.8, p < 0.001). The time between the patient’s death and the completion of the questionnaire was not significantly associated with satisfaction with GP home care (n = 347, χ2(6) = 2.99, p = 0.809).
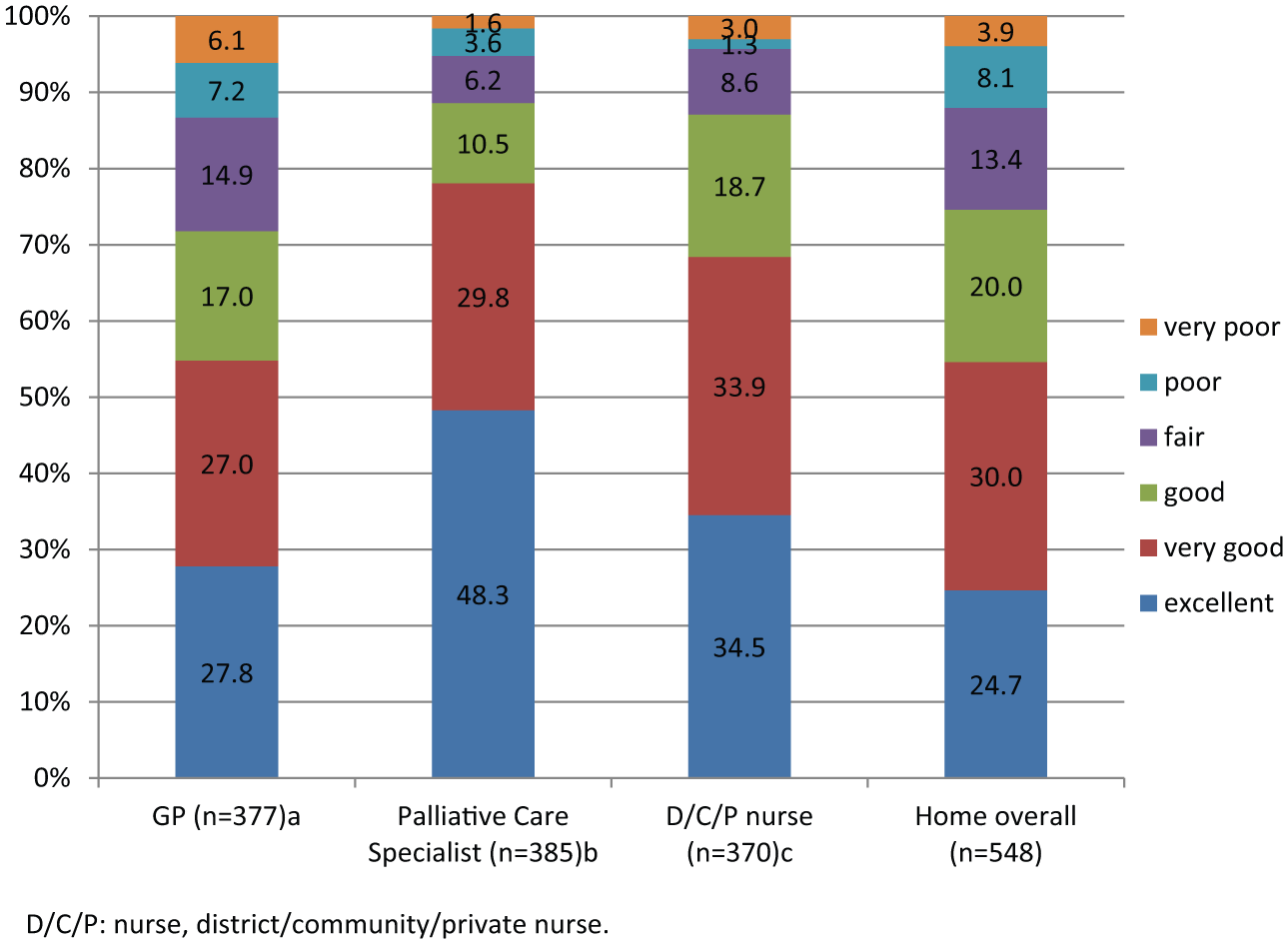
Relatives’ satisfaction with the home care delivered in the last 3 months of patients’ life by GPs, specialist palliative care providers and district, community and private nurses.
Factors associated with high satisfaction with home care provided by GPs: bivariate analysis
All four health service characteristics examined were associated with home care by GPs being described as excellent or very good (Table 2). Six out of 15 non-service characteristics were associated with higher satisfaction with GP home care: respondents’ older age (p = 0.030), patients’ lower financial hardship (p = 0.033), death at home (p = 0.002), a higher number of days spent at home (p = 0.001), less pain or discomfort at 3 months before death (p = 0.002) and respondents’ lower grief intensity at the time of the patients’ death (p = 0.018).
Factors associated with bereaved relatives’ satisfaction with home care delivered by GPs to cancer patients at the end of life: bivariate analysis.
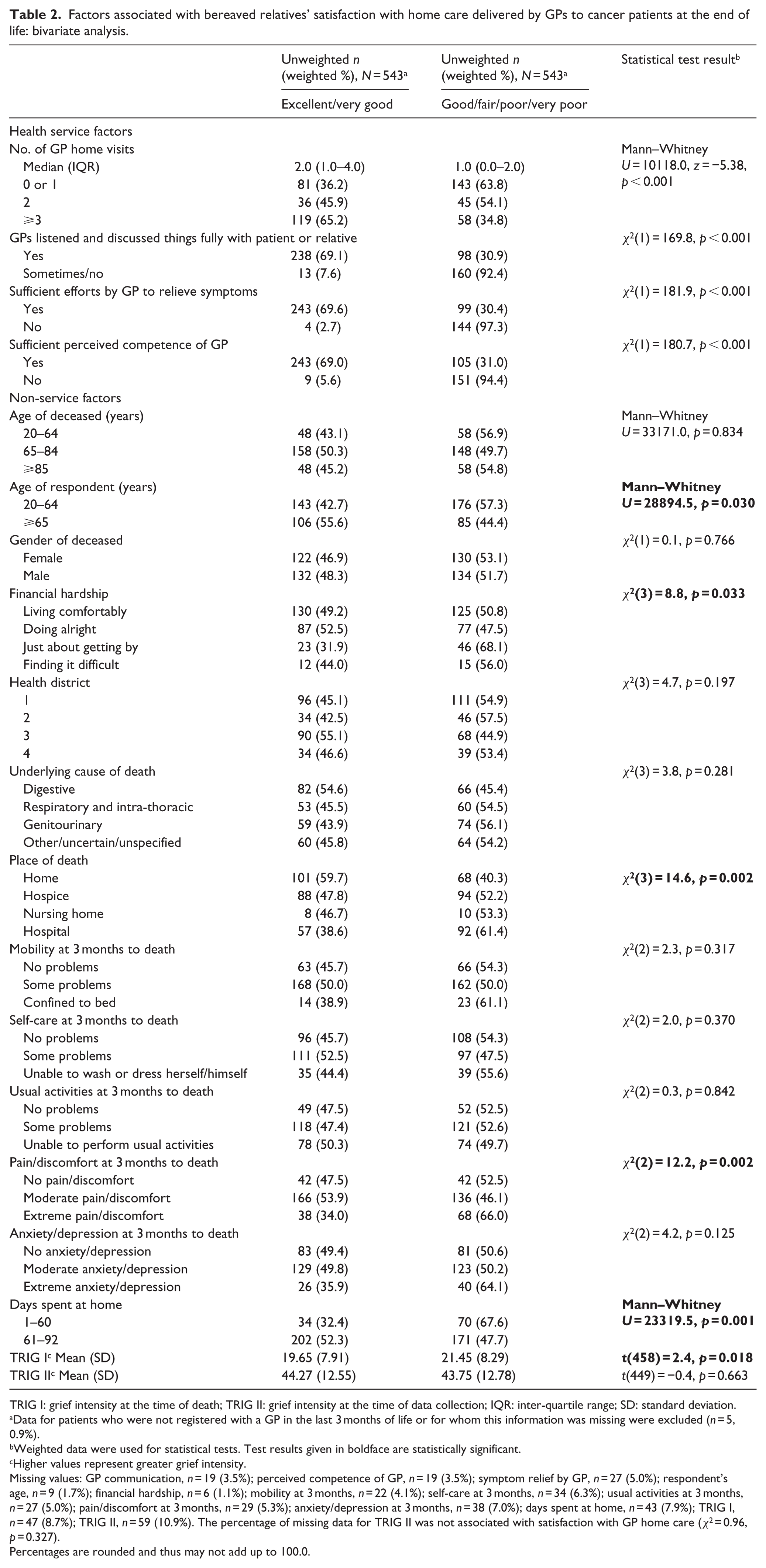
TRIG I: grief intensity at the time of death; TRIG II: grief intensity at the time of data collection; IQR: inter-quartile range; SD: standard deviation.
Data for patients who were not registered with a GP in the last 3 months of life or for whom this information was missing were excluded (n = 5, 0.9%).
Weighted data were used for statistical tests. Test results given in boldface are statistically significant.
Higher values represent greater grief intensity.
Missing values: GP communication, n = 19 (3.5%); perceived competence of GP, n = 19 (3.5%); symptom relief by GP, n = 27 (5.0%); respondent’s age, n = 9 (1.7%); financial hardship, n = 6 (1.1%); mobility at 3 months, n = 22 (4.1%); self-care at 3 months, n = 34 (6.3%); usual activities at 3 months, n = 27 (5.0%); pain/discomfort at 3 months, n = 29 (5.3%); anxiety/depression at 3 months, n = 38 (7.0%); days spent at home, n = 43 (7.9%); TRIG I, n = 47 (8.7%); TRIG II, n = 59 (10.9%). The percentage of missing data for TRIG II was not associated with satisfaction with GP home care (χ2 = 0.96, p = 0.327).
Percentages are rounded and thus may not add up to 100.0.
Factors associated with high satisfaction with home care provided by GPs: multivariate analysis
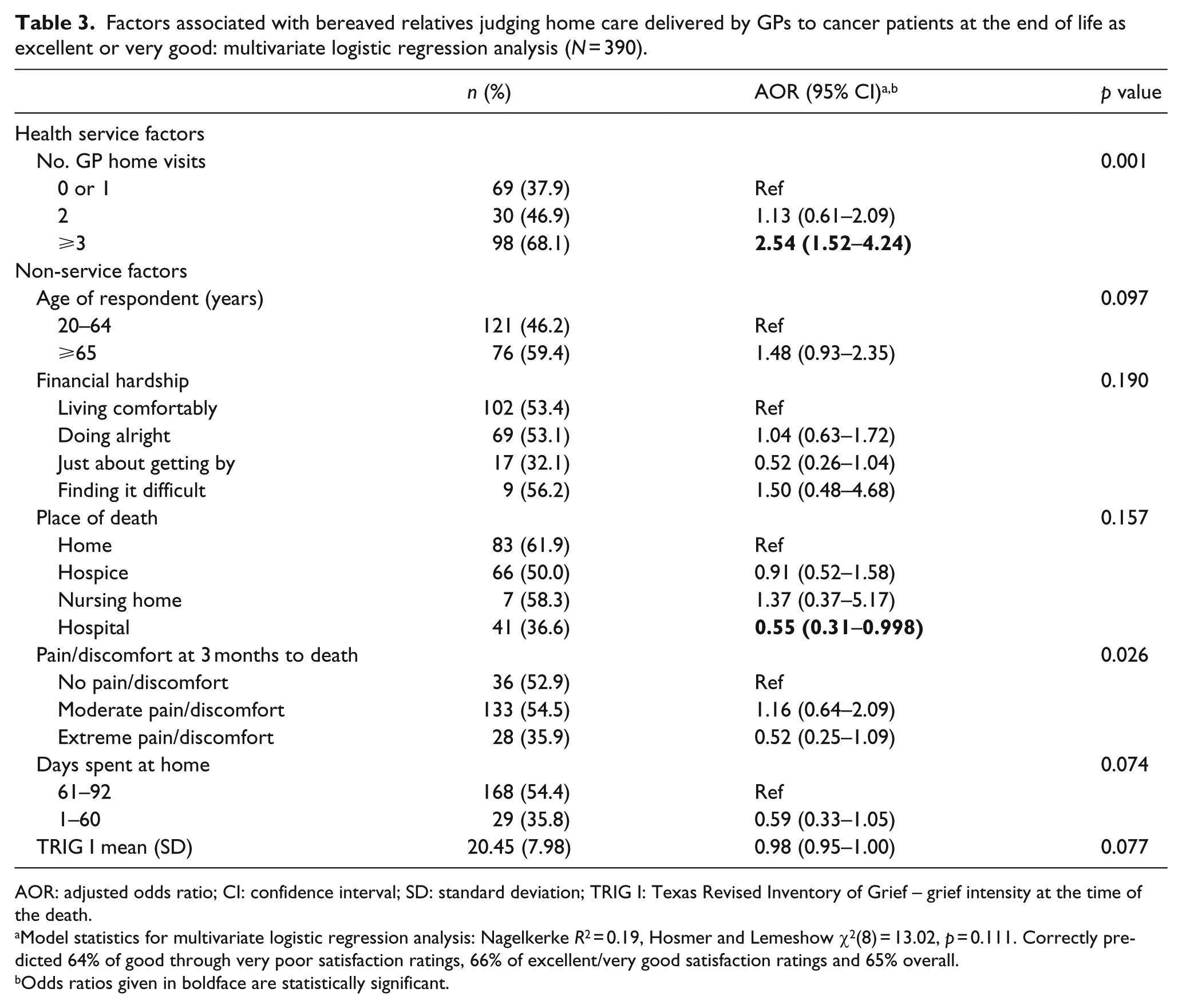
One service characteristic (number of GP home visits) and six non-service characteristics were included as independent variables in the multivariate logistic regression analysis (Table 3). Due to near-zero cell frequencies (Table 2) and multicollinearity with the number of GP home visits, the other non-service characteristics were not included as independent variables. When the other factors were adjusted for, bereaved relatives had twice greater odds of reporting high satisfaction with the home care provided by GPs if the patient had three or more home visits by the GP during the last 3 months of life as opposed to one visit or none (adjusted odds ratio (AOR): 2.54 (95% CI: 1.52–4.24)). The odds of reporting high satisfaction with home care by GPs halved if the patient died in hospital rather than at home (AOR: 0.55 (95% CI: 0.31–0.998)).
Factors associated with bereaved relatives judging home care delivered by GPs to cancer patients at the end of life as excellent or very good: multivariate logistic regression analysis (N = 390).
AOR: adjusted odds ratio; CI: confidence interval; SD: standard deviation; TRIG I: Texas Revised Inventory of Grief – grief intensity at the time of the death.
Model statistics for multivariate logistic regression analysis: Nagelkerke R2 = 0.19, Hosmer and Lemeshow χ2(8) = 13.02, p = 0.111. Correctly predicted 64% of good through very poor satisfaction ratings, 66% of excellent/very good satisfaction ratings and 65% overall.
Odds ratios given in boldface are statistically significant.
Discussion
This epidemiological study found that just over half of bereaved relatives perceived the home care provided by GPs to cancer patients during the last 3 months of life as excellent or very good. GPs received significantly less favourable ratings than other health professionals. Respondents for patients who had a higher frequency of GP home visits or who died at home rather than in hospital showed greater odds of reporting high satisfaction with the home care provided by GPs.
The findings of this study support existing concerns about the quality of home care delivered by GPs to cancer patients at the end of life. 10 Our results echo those of earlier studies,12,14,15 but despite a well-known tendency of satisfaction measures to yield ceiling effects we obtained even lower percentages of very good and excellent ratings for GP care than previous studies in the United Kingdom.12–15 Families’ satisfaction with GP care may have worsened over time, but our findings could also be a consequence of a better discriminatory power of our measure, as we added a response category named ‘very poor’ following pilot findings suggesting that respondents perceived the original scale as positively biased. 38 This study suggests that the frequency of home visits by GPs may be an important factor within families’ evaluations of the home care they provide. A number of other factors could also explain the relatively low satisfaction with GP home care. Although GPs perceive palliative care to be a central part of their role, 39 they often have limited training and experience in this field, and research suggests that their skills and confidence in managing pain and other symptoms as well as their knowledge of the availability of specialist home palliative care services and out-of-hours district nursing can be improved.10,16,39–41
Surveying bereaved relatives retrospectively is the most feasible way to obtain a population-based perspective on the care delivered during a particular time period prior to death. 42 Prospective patient surveys carry a high risk of including only healthcare service users and excluding those not recognised as dying. The agreement between bereaved relatives’ and patients’ service evaluations is adequate. 43 Postal surveys are well established in end-of-life care research, 7 and response rates and respondents’ characteristics are comparable to those in face-to-face surveys. 35 Finally, postal surveys are less likely than face-to-face surveys to yield top-ranked satisfaction ratings which suggest less socially desirable answers. 35
However, our study has limitations. First, the response rate was not high. Although it is within the range of similar surveys,12–14 there is a potential for non-response bias as we have no data from well over half of our sample. The comparison of responders and non-responders showed that this survey better represents the experiences of patients who died at home rather than in hospital, older patients and those for whom the respondents were women and spouses/partners or parents. These factors should be taken into account when interpreting the findings because the non-responders may have had a different view of the care that was provided to the patients. The fact that patients who died in hospital were under-represented may have led to an overestimation of positive satisfaction ratings for GPs because hospital death was associated with lower satisfaction ratings. Second, the data from the four London health districts differed somewhat from average England and Wales data. There was a higher percentage of hospice deaths and lower percentage of nursing home deaths in our sample 44 and a higher percentage of patients who were visited by specialist palliative care providers. 4 We must therefore be cautious in generalising our findings to areas with lower access to specialist palliative care services. Third, our data do not permit conclusions regarding causal relationships between variables. Fourth, there are limitations related to defining and measuring satisfaction with care18,29,45 and to its use in studying the quality of end-of-life care. 29 We did not assess respondents’ expectations of care but research has shown that around two-thirds of the variation in satisfaction levels are not explained by the discrepancy between expectations and perceptions. 46 However, we did take into account bereavement-related emotions and patients’ and respondents’ socio-demographic characteristics. Earlier research has demonstrated considerable variation in satisfaction ratings across different sources of care, thereby suggesting that this outcome is sensitive to differences in perceived quality of care. 17 Finally, we cannot exclude recall bias, but we did not find a significant association between time from death and satisfaction ratings.
This study shows that there is considerable room for improvement in the satisfaction with home care provided by GPs to terminally ill cancer patients. This is particularly important in light of calls to strengthen generalist palliative care as a consequence of restrictions in healthcare expenditure and limited access to specialist palliative care. Encourag-ing and enabling GPs to offer frequent home visits may be an important step towards achieving this goal. We recommend that this research be replicated in people with non-malignant diseases, who have lower access to specialist palliative care and whose satisfaction with end-of-life care and associated factors may differ from those of people with cancer.
Footnotes
Acknowledgements
We are particularly grateful to the people who, having recently lost a relative or friend to cancer, considered taking part in the study and to the funders of QUALYCARE – Cicely Saunders International – for their dedicated support, which made this study possible. We also thank the Department of Health and the four health districts (Primary Care Trusts) for their partnership in the study and the members of the project steering group and international advisors. A special thanks to the staff at the Office for National Statistics for their crucial help with sampling, mailings and datasets (Myer Glickman, Peter Davies, Justine Pooley and Stephen Rowland); Dr Jonathan Koffman for his help in setting up the study; Dr Gao Wei for her advice on sample size calculations and statistical issues; Dr Elizabeth Davies from the Thames Cancer Registry for her help in the ecological analysis to select the health districts; our local Cancer Research Network (South East London) for administrative support; Kerry Hylands for help with data entry; Sian Best for the development of the study website pages (![]() ) and other members of the Cicely Saunders Institute. Lara Pivodic undertook this analysis as part of her work within the project EURO IMPACT, during a secondment at King’s College London, Cicely Saunders Institute. EURO IMPACT (European Intersectorial and Multidisciplinary Palliative Care Research Training) aims to develop a multidisciplinary, multi-professional and inter-sectorial educational and research training framework for palliative care research in Europe. In recognition of the collaborative nature of EURO IMPACT, we thank the following EURO IMPACT members: Van den Block Lieve1, De Groote Zeger1, Brearley Sarah2, Caraceni Augusto3,4, Cohen Joachim1, Francke Anneke5, Harding Richard6,7, Higginson Irene J6,7, Kaasa Stein8, Linden Karen9, Miccinesi Guido10, Onwuteaka-Philipsen Bregje5, Pardon Koen1, Pasman Roeline5, Pautex Sophie11, Payne Sheila2 and Deliens Luc1,5. EURO IMPACT is coordinated by Prof Luc Deliens and Prof Lieve Van den Block of the 1End-of-Life Care Research Group, Ghent University & Vrije Universiteit Brussel (VUB), Brussels, Belgium. Other partners are as follows: 2International Observatory on End-of-Life Care, Lancaster University, Lancaster, UK; 3EAPC Research Network, Trondheim, Norway; 4Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; 5VU University Medical Center, EMGO Institute for Health and Care Research, Amsterdam, The Netherlands; 6King’s College London, Cicely Saunders Institute, London, UK; 7Cicely Saunders International, London, UK; 8Norwegian University of Science and Technology, Trondheim, Norway; 9Springer Science and Business Media, Houten, the Netherlands; 10Cancer Research and Prevention Institute, Florence, Italy; 11EUGMS European Union Geriatric Medicine Society, Geneva, Switzerland.
) and other members of the Cicely Saunders Institute. Lara Pivodic undertook this analysis as part of her work within the project EURO IMPACT, during a secondment at King’s College London, Cicely Saunders Institute. EURO IMPACT (European Intersectorial and Multidisciplinary Palliative Care Research Training) aims to develop a multidisciplinary, multi-professional and inter-sectorial educational and research training framework for palliative care research in Europe. In recognition of the collaborative nature of EURO IMPACT, we thank the following EURO IMPACT members: Van den Block Lieve1, De Groote Zeger1, Brearley Sarah2, Caraceni Augusto3,4, Cohen Joachim1, Francke Anneke5, Harding Richard6,7, Higginson Irene J6,7, Kaasa Stein8, Linden Karen9, Miccinesi Guido10, Onwuteaka-Philipsen Bregje5, Pardon Koen1, Pasman Roeline5, Pautex Sophie11, Payne Sheila2 and Deliens Luc1,5. EURO IMPACT is coordinated by Prof Luc Deliens and Prof Lieve Van den Block of the 1End-of-Life Care Research Group, Ghent University & Vrije Universiteit Brussel (VUB), Brussels, Belgium. Other partners are as follows: 2International Observatory on End-of-Life Care, Lancaster University, Lancaster, UK; 3EAPC Research Network, Trondheim, Norway; 4Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; 5VU University Medical Center, EMGO Institute for Health and Care Research, Amsterdam, The Netherlands; 6King’s College London, Cicely Saunders Institute, London, UK; 7Cicely Saunders International, London, UK; 8Norwegian University of Science and Technology, Trondheim, Norway; 9Springer Science and Business Media, Houten, the Netherlands; 10Cancer Research and Prevention Institute, Florence, Italy; 11EUGMS European Union Geriatric Medicine Society, Geneva, Switzerland.
Declaration of conflicting of interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by Cicely Saunders International. Lara Pivodic was funded to undertake this analysis as part of the EURO IMPACT project, supported by the European Union Seventh Framework Programme (FP7/2007-2013, under grant agreement no. 264697). Irene J Higginson is a UK NIHR (National Institute of Health Research) Senior Investigator.