
Abstract
Background:
Primary care has the potential to play significant roles in providing effective palliative care for non-cancer patients.
Aim:
To identify, critically appraise and synthesise the existing evidence on views on the provision of palliative care for non-cancer patients by primary care providers and reveal any gaps in the evidence.
Design:
Standard systematic review and narrative synthesis.
Data sources:
MEDLINE, Embase, CINAHL, PsycINFO, Applied Social Science Abstract and the Cochrane library were searched in 2012. Reference searching, hand searching, expert consultations and grey literature searches complemented these. Papers with the views of patients/carers or professionals on primary palliative care provision to non-cancer patients in the community were included. The amended Hawker’s criteria were used for quality assessment of included studies.
Results:
A total of 30 studies were included and represent the views of 719 patients, 605 carers and over 400 professionals. In all, 27 studies are from the United Kingdom. Patients and carers expect primary care physicians to provide compassionate care, have appropriate knowledge and play central roles in providing care. The roles of professionals are unclear to patients, carers and professionals themselves. Uncertainty of illness trajectory and lack of collaboration between health-care professionals were identified as barriers to effective care.
Conclusions:
Effective interprofessional work to deal with uncertainty and maintain coordinated care is needed for better palliative care provision to non-cancer patients in the community. Research into and development of a best model for effective interdisciplinary work are needed.
Keywords
Many people die of non-cancer diseases without enough access to palliative care.
Many patients want to be cared for at home until the last phase of their life.
Primary care plays important roles in providing palliative care in the community.
Non-cancer patients and carers expect general practitioners to provide compassionate care, have appropriate knowledge and play central roles in providing palliative care.
Continuity and coordination of the care are significant gaps in care provision.
Health-care professionals have reciprocal expectations and concerns that sometimes conflict with each other.
Uncertainty was recognised by health-care professionals as a great barrier to the provision of good palliative care.
Effective interprofessional work needs to be enhanced in primary palliative care for non-cancer patients to deal with uncertainty and to assure continuity and coordinated care.
Research is needed on who should be the coordinators of the care, what kind of care models work and how it works.
Introduction
Palliative care has been historically developed with the focus on cancer. However, recent rapid global ageing and changes in disease prevalence, which are particularly evident in developed countries, have brought renewed attention to palliative care for chronic non-cancer diseases. Although there are increasing percentages of non-cancer patients among those utilising specialist palliative care services in the United Kingdom and the United States,1,2 many non-cancer patients are still dying in primary care settings without accessing specialist palliative care services. Considering the fact that more people wish to die at home in most developed countries than in hospitals,3,4 the role of primary care providers (PCPs) in palliative care for non-cancer patients is significant.
While some studies have shown that general practitioners (GPs) regard palliative care as a part of their responsibilities towards their patients,5–8 it has been suggested that not many non-cancer patients in the community receive adequate palliative care.7,9
The available evidence on the needs and experience of patients suffering from non-cancer diseases has been reviewed mainly in accordance with diagnoses.10,11 Yet, to our knowledge, this evidence has not been systemically reviewed to allow comparison across different perspectives, for example, those of patients, carers and health-care professionals (HCPs).
Health-care service planning must reflect the needs of service users. 12 It is equally important to know the views of HCPs on the services, as the understanding of conflicts and agreement between HCPs and patients can lead to improvements in the services and clinical practice. The existing evidence regarding the different perspectives on palliative care provision to non-cancer patients in the community needs to be synthesised so as to inform clinicians and policy makers.
This review therefore identifies, critically appraises and synthesises the existing evidence on views on the provision of palliative care for non-cancer patients by PCPs and reveals any gaps in the evidence.
Methods
The definitions of terms used in this review are given in Table 1.
Definitions of terms.
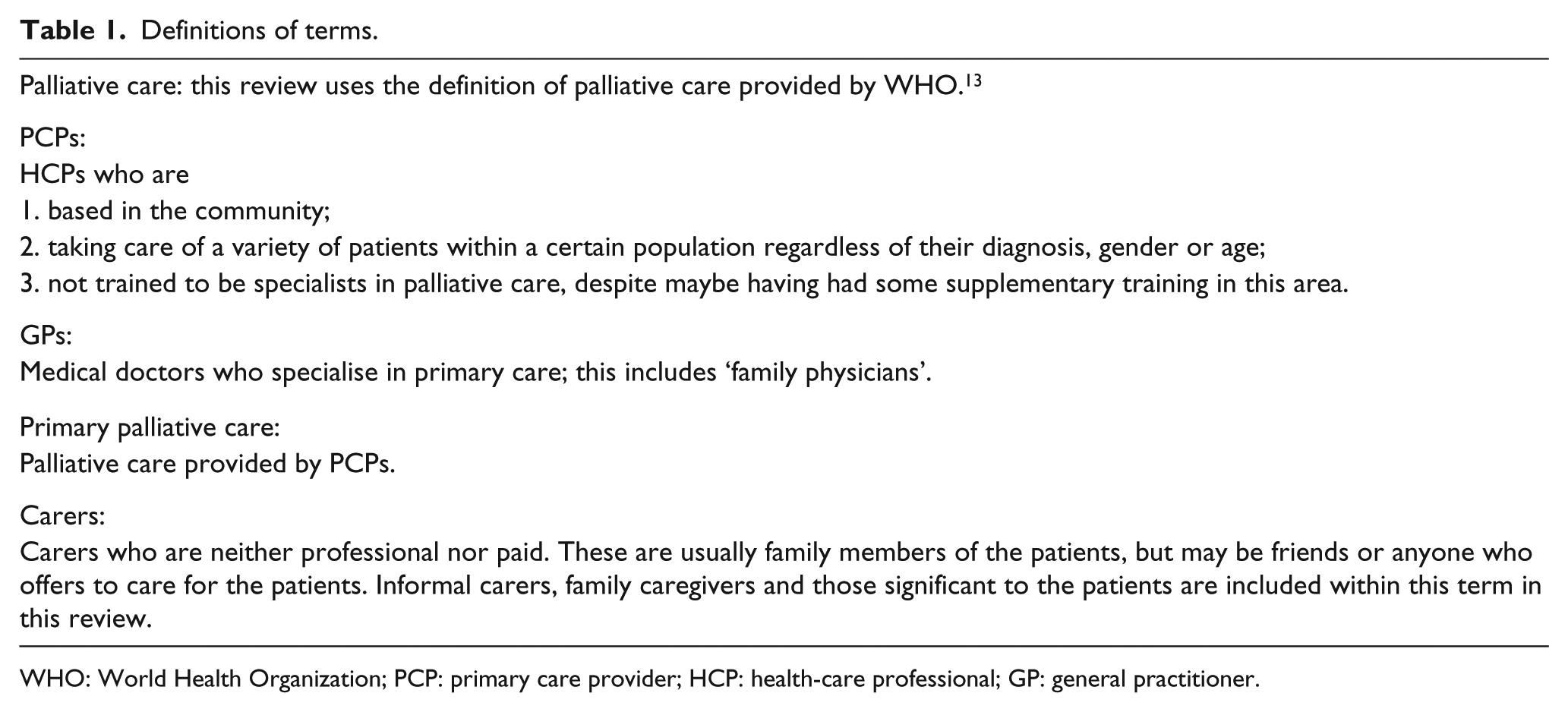
WHO: World Health Organization; PCP: primary care provider; HCP: health-care professional; GP: general practitioner.
The methods for this review are structured according to The Centre for Reviews and Dissemination’s guidance for undertaking reviews in health care 14 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 15 supplemented by guidance on narrative synthesis. 16
Paper searches were conducted using MEDLINE, Embase, CINAHL, PsycINFO, Applied Social Science Abstract and the Cochrane library (all from inception to September 2012). The searches were conducted in September/October 2012.
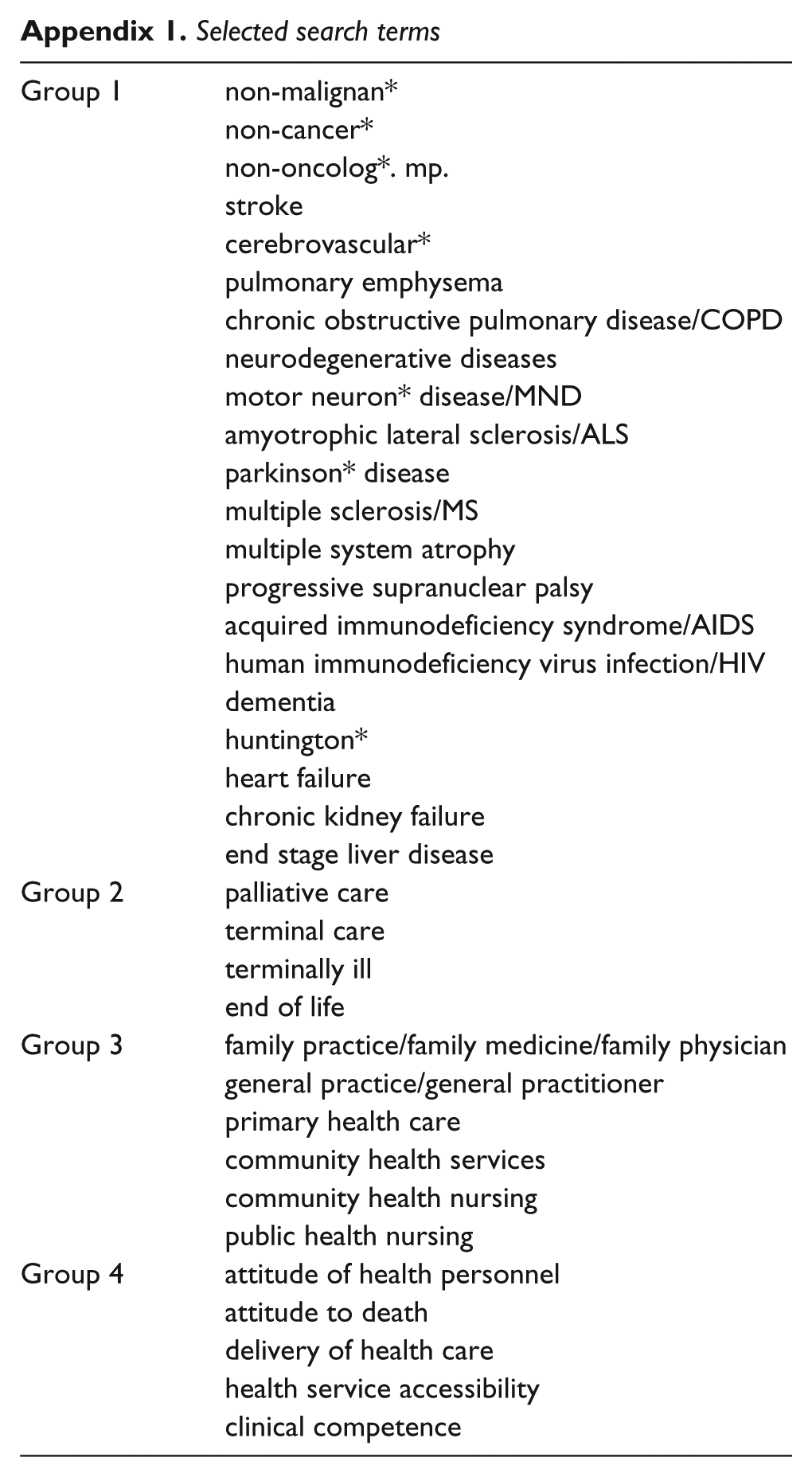
Search terms were categorised into four groups:
Group 1: Disease diagnoses
Group 2: ‘Palliative care’
Group 3: ‘Primary care’
Group 4: ‘Attitude’
(See Appendix 1 for search terms.) These groups were combined with ‘AND’ to complete the search.
A cited reference search using SCOPUS was conducted for further identification of relevant studies. Reference lists of relevant papers were also manually searched. The content pages of Palliative Medicine (1987–1992, and January to November 2012) were hand-searched. Authors of relevant papers and principal researchers of relevant studies identified through UK Clinical Research Network Study Portfolio Database 17 were asked for any further studies related to the review questions. Other search engines such as CareSearch database 18 and Open Grey 19 were searched to identify relevant grey literature.
Selection criteria were set to include studies reporting the views of patients/carers or professionals on primary palliative care provision to non-cancer patients in the community. The SPIDER tool enabled us to conceptualise eligibility criteria (Table 2). 20
SPIDER tool and search term groups.
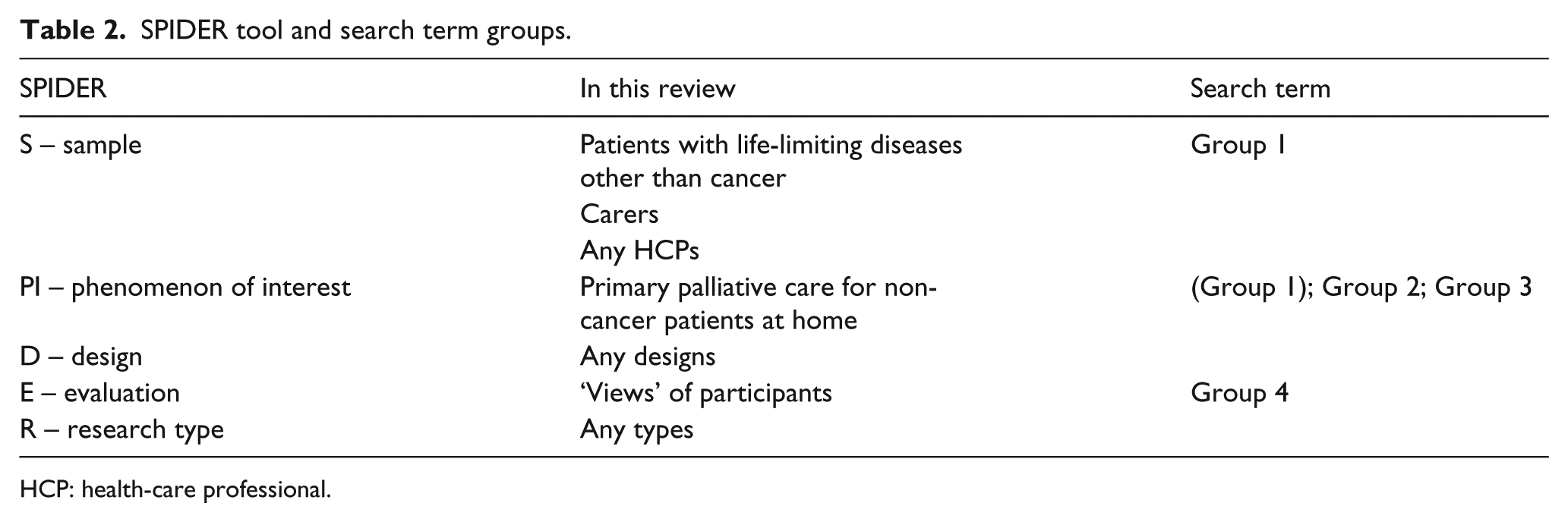
HCP: health-care professional.
In this review, ‘Sample’ of the study is patients, carers or professionals. Studies with patients or carers as participants are considered when 50% or more of the participants or the ones they cared for had non-cancer diagnoses. ‘Phenomenon of interest’ is primary palliative care provision to non-cancer patients at home. ‘Evaluation’ is participants’ views on this phenomenon. Any study designs, both quantitative and qualitative, are considered to be included.
Studies that focused on specific topics in palliative care (e.g. decision-making, symptom management, communication, euthanasia, out-of-hours care or identifying patients) were excluded. Papers that only reported patterns of service uses and did not contain any participants’ views were also excluded. Studies regarding care for special groups of patients, such as those with severe mental illnesses or those who were incarcerated, and for sexual minorities were also excluded, as the needs of these patients were assumed to be quite different from those of the majority of patients. Papers written in languages other than English, without any new empirical data or not providing sufficient information to judge their eligibility, were also excluded. We also decided to exclude the papers with limited reference to the review questions, as they were considered to have no impact on the overall conclusions.21–24
The titles and abstracts of all identified papers were screened by A.O. Of those that were selected for reading of the entire paper, 10% were randomly selected and their agreement with the eligibility requirements was confirmed by F.E.M.M. Any papers for which inclusion or exclusion was unclear were discussed to reach a consensus.
Information about the studies (e.g. study aims, country, study setting, targeting diseases, participants, sampling methods, types of collected data, analysis methods) was extracted from each paper.
Amended Hawker’s criteria4,25 were used for quality assessment of the included studies. These criteria aim to assess 10 aspects of the study (including aims, method, sampling, data analysis, bias and transferability or generalisability) graded from 1 (very poor) to 4 (very good) and have the advantages of being able to be used for all qualitative, quantitative and mixed-methods studies.
Given the heterogeneity of included studies, Narrative Synthesis 16 is most appropriate for data synthesis in this review. Analysis and synthesis were done by grouping the data by tabulations, thematic analysis and conceptual mapping. Each theme from selected studies was tabulated and then synthesised. The robustness of the synthesis was assessed in the form of a critical appraisal of this review process and is described in the discussion section of this paper.
Results
After the duplicates were removed, 3986 papers were identified for study selection. A total of 31 papers from 30 studies from 1998 to 2012 met the inclusion criteria. A PRISMA flow diagram 15 of study selection is shown in Figure 1.
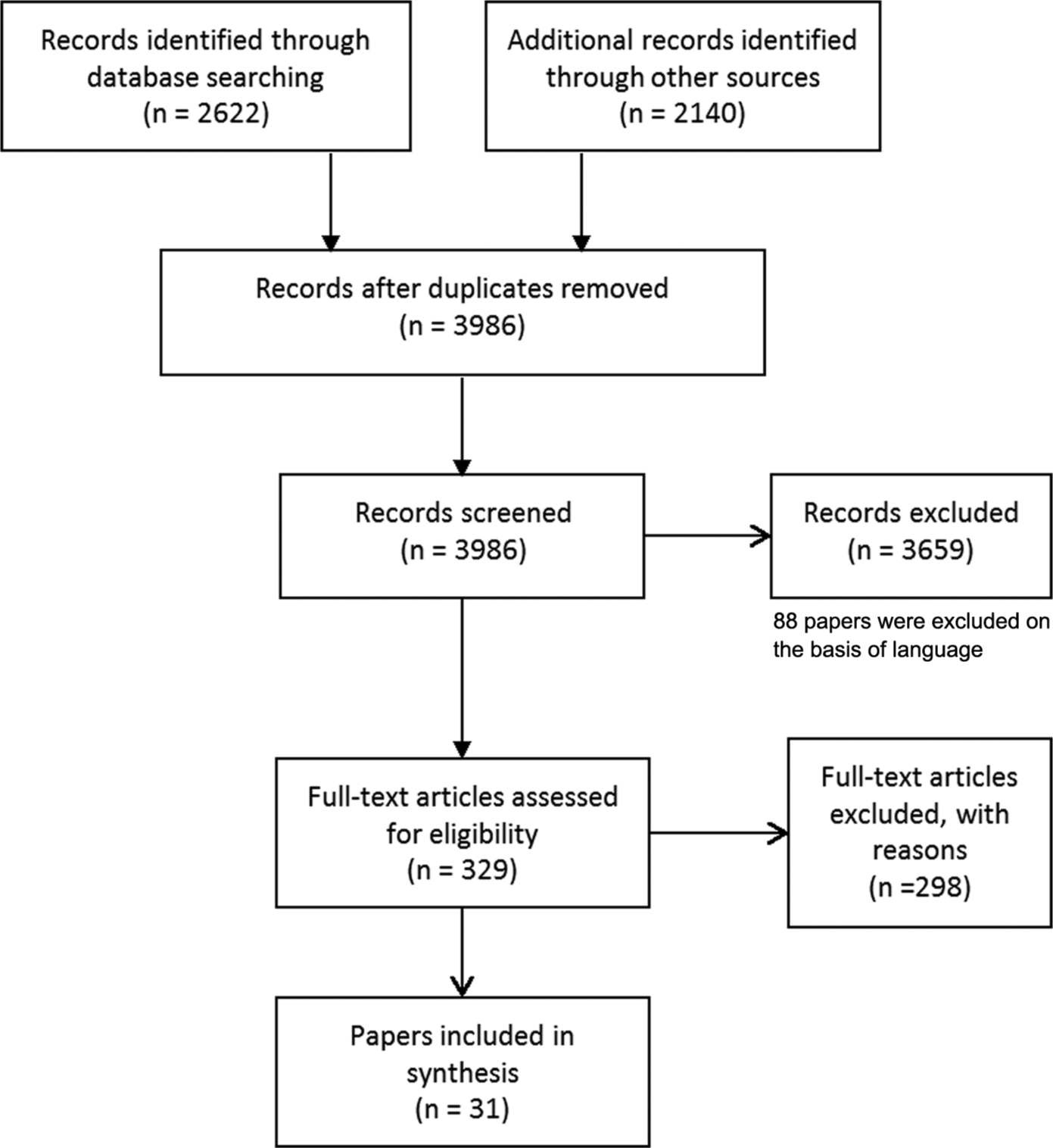
PRISMA flow diagram of study selection. 15
Characteristics of included studies
The overview of included studies is shown in Table 3. Apart from four studies, one from each of the United States, Australia, New Zealand and Sweden, all others were from the United Kingdom. These represent the views of 719 patients, 605 carers and over 400 professionals. Only three exclusively collected quantitative data and another three studies used mixed methods. All others were qualitative. Of the three quantitative studies, one was an intervention study 31 and the other two were observational studies.45,46
Characteristics of included studies.

COPD: chronic obstructive pulmonary disease; GP: general practitioner; HCP: health-care professional; MS: multiple sclerosis; EOL: end-of-life; MND: motor neurone disease; HF: heart failure; DN: district nurse; PD: Parkinson’s disease; RF: renal failure; SPC: specialist palliative care; ICD: implantable cardioverter defibrillator.
Nine of the included studies were about chronic obstructive pulmonary disease (COPD).26–30,32,35,43,49 Eight studies had heart failure (HF) as their main topic.36–39,50–53,55 Three studies investigated the experience of motor neurone disease (MND),34,40,44 two were on Parkinson’s disease (PD)47,48 and one each was about patients with multiple sclerosis (MS) 33 and dementia. 54 Two survey studies examined stroke patients.45,46
More than half of the studies (17 studies) included patients as participants.26–42 Sixteen included bereaved or current carers.32–38,40–48
The average age of patient participants was approximately 70 years, with the exception of the MND and MS studies, which had younger populations.33,34,40
Most of the COPD and HF studies recruited participants through general practices while MND and MS studies employed a variety of recruitment methods, which probably reflected the prevalence of the diseases.
The results of the quality assessment of all included studies are displayed in Table 3. The mean score was 30.1 (range from 26 to 37).
Expectations of GPs
The identified themes were categorised as follows: service users’ expectations of GPs, roles of professionals and barriers to effective primary palliative care provision to non-cancer patients.
Patients and carers expressed various expectations of GPs based upon their experience and understanding of illness either explicitly or indirectly.
Five studies (on stroke, COPD, HF and renal failure) reported high satisfaction with GPs’ care.26,41,42,45,46 The same number of studies were interested in physicians’ views on palliative care for non-cancer patients.5,51,52,54,55 Three studies on COPD attempted to depict patients’ and carers’ views on professionals other than GPs in the primary care setting, but neither patients nor carers responded.27,28,30 For this reason, expectations of GPs – that is, compassionate care, knowledge and skills, central role and quick response – are presented in this section.
A compassionate attitude toward care is highly valued by patients and carers.30,37,38,42,43 In these studies, the willingness of GPs to spend time with patients and to understand their concerns is greatly welcomed. In contrast, dismissive attitudes (e.g. ‘carrying on writing’) are severely criticised. 43
All three MND, two PD and one of the COPD studies convey the concerns of patients or carers over GPs’ lack of knowledge about the disease in question.29,34,40,44,47,48 The patients and carers attribute this lack of knowledge to either low prevalence of the disease 40 or GPs’ time constraints. 44 Lack of knowledge on the part of GPs leads to a lack of information for patients about available services 40 or hinders patients from accessing general practices when needed. 29 While some participants insist that GPs should have sufficient knowledge and skills, one carer of PD patients puts an emphasis on maintaining contact with neurologists for symptom management, doubting the ability of GPs in this area. 48 In studies investigating HF care, some hospital doctors 55 and specialist palliative care nurses 38 are concerned about the quality of care provided by primary care teams.
Patients and carers report that GPs play a central role in their care.37,43 Some even convey their perceptions of GPs as partners in their journey with illness.44,47 This notion, of the GP as the central person in the care, is also shared by other HCPs including GPs themselves.37,50,51
Quick responses to urgent needs, including out-of-hours, are considered highly important by patients and carers.37,41 GPs are expected to be able to prevent unnecessary hospital admissions by responding to emergency needs. This may be related to some patients’ negative impressions of hospital admissions 37 and carers’ beliefs that admission to hospital should be avoided.34,37
Roles of professionals
The unclear boundaries of the roles of each professional are recognised by HCPs themselves, as well as by patients and carers.
Both patients and nurses consider the nurses’ role to be task-oriented.26,49 However, one of the studies supporting this was ranked as relatively low in quality. 26 Carers appreciate having nurses with good technical skills, 34 which can be contrasted to their expectation of doctors to have a compassionate attitude. Moreover, primary care nurses think of themselves as lacking experience in end-of-life care for cardiorespiratory diseases.41,49 GPs, on the other hand, expect nurses to act as coordinators and to provide education and holistic care to patients with HF. 53
Various views on the role of specialist nurses are shown across the studies. In one study conducted in a rural area, patients saw specialist respiratory nurses as less useful. 32 Other studies report that nurses specialising in HF or COPD are seen as linking primary and secondary HCPs and as potentially useful.37,39,42,43,55 This disparity may be caused by the difference in settings, but it should be noted that the former study 32 was assessed as low in quality and conducted by GPs, which potentially leads to bias towards generalists. Some studies show particular expectations of other HCPs for specialist HF nurses to take more active roles in the regular monitoring and coordination of care.52,55
Ambivalent feelings of PCPs towards specialist services are described in some studies, using words such as ‘sidelined’ and ‘taken over’ to express their feeling of specialist services taking over care of the patients.41,49 Those who have such feelings consider that specialist nurses should be restricted to an advisory role rather than providing direct care to the patients. 41 While the importance of the role of specialist doctors in symptom management is cited by a PD carer, 48 in other studies, patients cite specialist doctors as inaccessible. 32 However, again, the latter study was conducted by GPs, and it is unclear whether they recruited participants from their practice, which could impact the results of the study.
Barriers to effective primary palliative care
Along with expectations, many barriers to effective primary palliative care have been identified in the included studies. The impacts of an uncertain and unpredictable illness trajectory are most frequently cited across studies.35,36,40–42,50,54,55 It is more evident that COPD starts without a clear onset and is punctuated by sporadic periods of exacerbation.26,27,35 HF and dementia, on the other hand, are conveyed as a rather gradual deterioration.39,54 The punctuated illness trajectory results in ad hoc care, which is prominent in COPD and HF.26–28,32,35,38,43,55 All HF, COPD, PD and MS patients and their carers expressed the need for continuity of care and regular monitoring.27,28,32,33,38,41,43,47,48,55
The uncertain illness trajectory results in difficulty in identifying the right timing for the transition of care.35,38,41,50,52,54 This is also related to difficulty in accepting their dying conditions for patients and carers.27,41,54
The lack of communication between care providers is also frequently pointed out.33,38,41,42,47,48,54 Not only are the boundaries of the roles of professionals unclear,38,47,50,51,55 but carers are often required to act as the coordinators of the care. 33 One randomised controlled trial confirms that coordinated care can raise levels of satisfaction of patients. 31
A lack of access to services for non-cancer patients is often cited across the disease groups.5,26,33,34,36,40–42,49,52 The importance of home visits to compensate for the limited access is also pointed out in the highest quality study exploring the access to general practices for people with advanced COPD. 30 Some studies suggest that there are only a few existing available services,41,49 while others point out that information to access the service is not well organised.33,40
Some studies convey the patients’ notion that ‘GPs are busy’.28,38,39,44 Patients regard GPs’ time constraints as a reason for their not having received enough information or care from GPs. 44 MND patients also claim that this situation has even hindered patients from seeking help from GPs.30,44 Some patients, particularly those from a COPD/HF cohort, think little or nothing could be done by HCPs to improve their situation, which is why the patients end up not seeking help.27,29,36,37,41 Some are anxious about bothering HCPs inappropriately, for fear this may have a negative impact on their treatment decision. 27 Two studies respond to this notion of patients with comments from GPs, admitting that they indeed lack adequate time for sufficient care.38,52,53
Discussion
Principal findings of the review
A majority of the 30 included studies are on HF or COPD with small numbers of other diseases, for example, MND, stroke, PD, MS and dementia. In all, 27 of the studies use qualitative methods, 3 use mixed methods and another 3 are quantitative. In all, 27 studies are from the United Kingdom. The review represents the views of 719 patients, 605 carers and over 400 professionals.
First, patients and carers highly value PCPs’ compassionate care, appropriate knowledge and skills, quick responses to urgent needs and maintenance of the coordination and continuity of care. Second, the unclear boundaries of the roles and responsibilities of each professional are recognised by HCPs themselves, as well as by patients and carers. HCPs also report their reciprocal expectations and concerns, which sometimes conflict with each other (Figure 2). While many patients, carers and other HCPs regard GPs as having a central role, GPs are juggling competing priorities with a limited amount of time, expecting nurses to take more active roles. In addition, uncertainty caused by unpredictable illness trajectory, lack of available resources and PCPs’ lack of expertise are listed as additional barriers to palliative care for non-cancer patients.
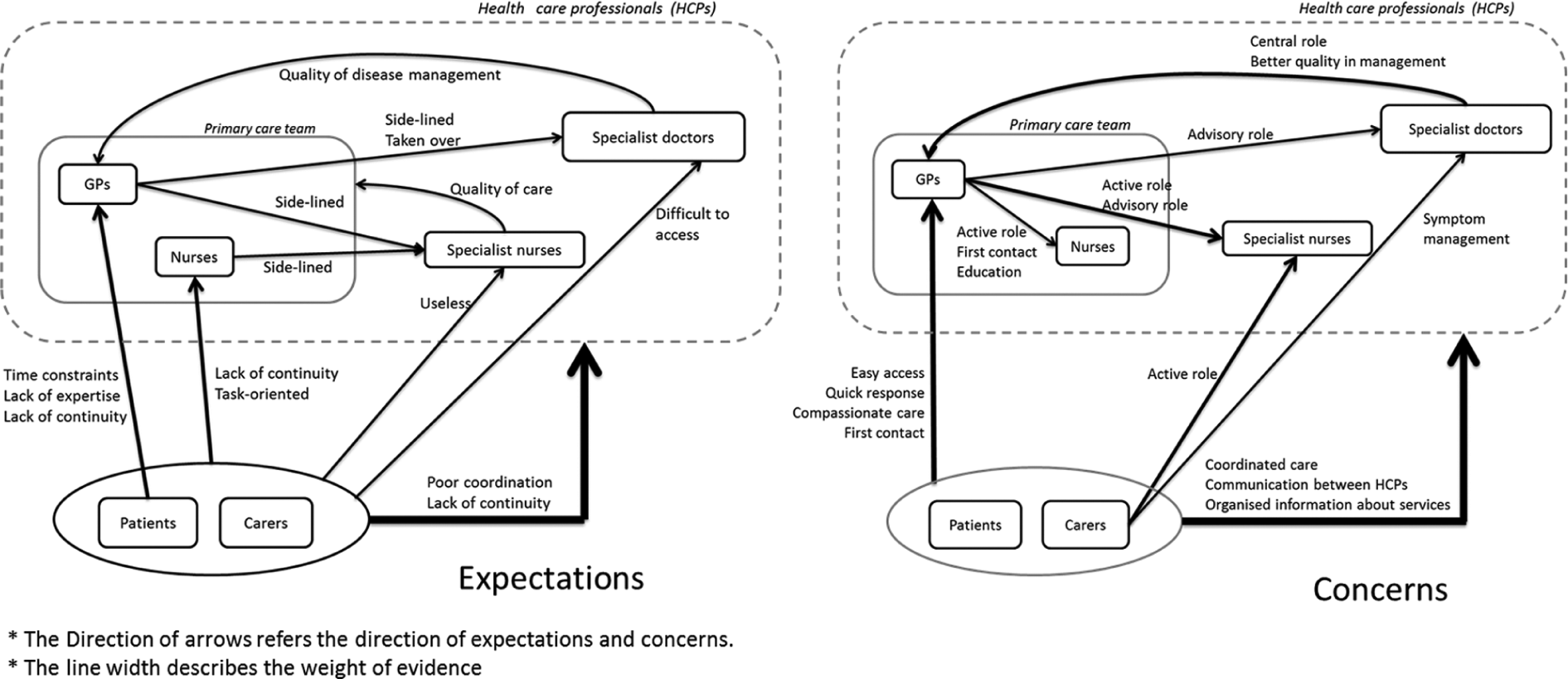
Expectations and concerns between patients, carers and health-care professionals.
How the results fit in
There are two main challenges identified in this review, one is how to maintain continuity and coordination of care as a multiprofessional team and the other is how to deal with uncertainty. Patients’ expectations of GPs such as a compassionate attitude, availability for home visits and out-of-hours care to maintain continuity of care are consistent with those identified in previous studies.56–58 What has been newly added in this review is that uncertainty in non-cancer diseases makes meeting these expectations more difficult.
Uncertainty is likely to contribute to other barriers to effective care, for example, provision of care on an ad hoc (rather than planned) basis and failure to identify dying. This has been recognised as a challenge in palliative care for non-cancer patients.59–61 While many efforts have been made to develop a model to predict the right timing to introduce palliative care to non-cancer patients, there are as yet no definite tools.54,62 In COPD patients, for example, the gradual deterioration punctuated with exacerbations leads to ad hoc care.
Less available services and resources for non-cancer patients in the community aggravate the situation. In general, PCPs are required to achieve more with fewer resources. Table 4 summarises these expectations and barriers.
Expectations and barriers in palliative care in primary care settings.
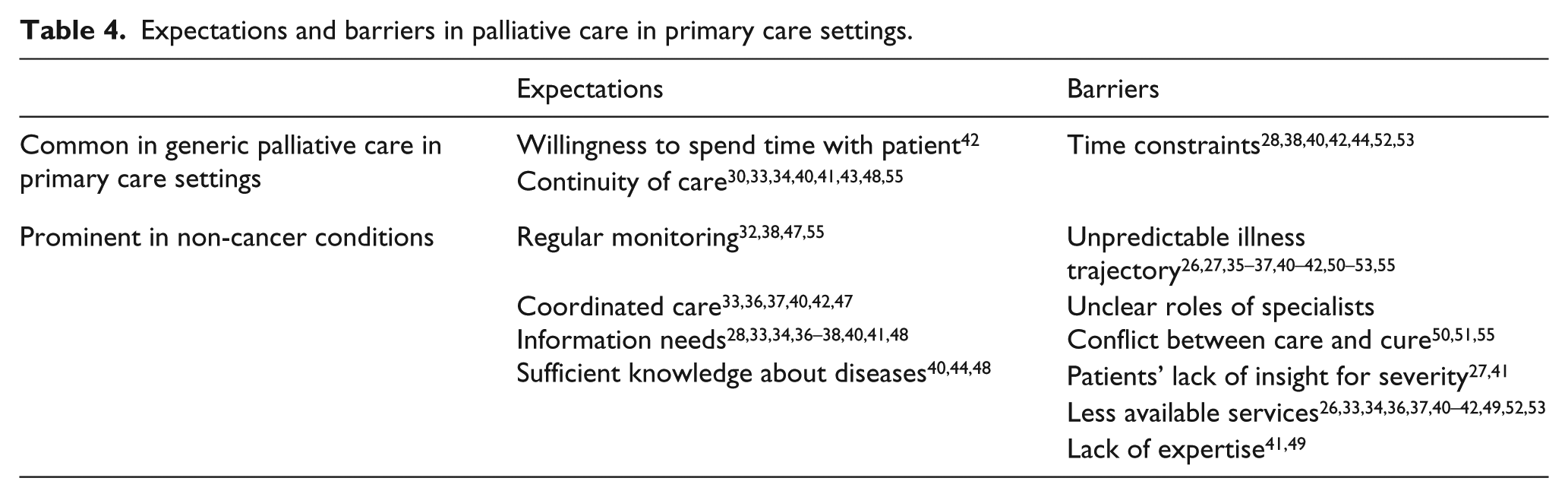
Figure 2 shows the reciprocal expectations and concerns between patients, carers and HCPs. What is notable is that no expectations of primary care nurses were directly expressed by patients, while concerns over their lack of continuity were voiced. This is supported by other evidence showing the low prevalence of access to community nurses. 63 Moreover, no other primary care team members were discussed in the included studies. In one study, the interviewers attempted to draw out opinions about other professionals but participants did not respond, 41 showing that they minimally consider other professionals in the primary care team. It is hence plausible that patients and carers predominantly consider GPs to be the main professional of their care in primary palliative care.
Regarding the role of primary care nurses, the results of the present review are by and large consistent with a previous systematic review. 64 One exception is that while primary care nurses regarded palliative care as holistic care in the previous review, this was not clearly shown in the present review. Moreover, the unpredictability of illness trajectory and a lack of expertise and awareness were identified as additional barriers to provision of palliative care to non-cancer patients. This is concordant with the findings in Table 4.
From GPs’ point of view, they expect nurses to take more active roles.50–53 This might be a reflection of GPs’ excessive workloads and the expectations placed upon them. In fact, it seems impossible for GPs to take on all responsibilities given the multi-dimensional principle of palliative care. 13 Taking these findings into account, it seems that collaborations between GPs and primary care nurses are not efficiently undertaken, with primary care nurses roles being minimally considered by patients.
GPs also expect specialists to play advisory roles rather than to take full responsibility for the patients. GPs expressed discomfort about their role towards the patients being completely taken over, and this discomfort was also shared by primary care nurses. On the whole, interprofessional work in primary palliative care settings is relatively ineffective despite the importance of collaboration having been repeatedly emphasised.65–67 This is even more relevant for non-cancer patients because the fluctuating trajectory of their illnesses can cause frequent exacerbations and admissions. 68
This raises an issue as to how we can promote coordinated care and who should be the coordinator of the care. In the United Kingdom, the National Gold Standard Framework has been introduced as a systematic approach to enhance coordinated care. 69 While its effectiveness has been shown,70–73 it is also suggested that an adequate amount of time to maintain shared vision, mutual respect and inclusive decision-making are important for its successful implementation. 74 Moreover, good networks are usually based on personal liaison rather than on a systematic approach. 75
Allocating key care workers has been suggested to be important to maintain the continuity of care; 76 however, it is difficult from the present review to conclude who should be the coordinator of the care. While GPs are usually seen as the multidisciplinary team lead in the present review, they obviously lack time and resources. Some evidence within and outside of this review supports specialist nurses can possibly be the key workers.37,39,42,43,52,53,76 The decision is probably better made locally, however, according to available resources and local preference.
Strengths and limitations
This review, to our knowledge, is the first systematic review of views on palliative care provided by PCPs to non-cancer patients in community. It combines both qualitative and quantitative evidence with a wide range of views from different perspectives across the diseases. The completeness of the search with expert consultation and hand searching maximised the identification of the studies.
However, there are some limitations that should be considered in included studies. Many studies lacked detailed information about their participants, for example, patients’ medical conditions or specialties of HCPs and the settings in which they were working.35–38,40–42,49 Second, reporting by whom the findings are conveyed was also often missed. Despite the fact that having interviewed patients and carers together may affect the data, reports often failed to mention if they had interviewed them together or separately.34,38 Only Edmonds et al. 33 mentioned this issue in their discussion.
At the review level, a majority of the included studies are from the United Kingdom, which may impact the generalisability of the findings. Cultural impacts on end-of-life care issues have to be considered when interpreting the results of this review. However, we believe our findings are useful to other nations with similar care models to that in the United Kingdom.
Another potential bias is that only one reviewer conducted the review process, with appraisals of a second reviewer at each step. As narrative synthesis is still regarded as a somewhat subjective method, having more reviewers would be preferable, but was not possible due to the limited resources available for this review.
Finally, excluding some papers with only a limited reference to the review questions21–24 can be considered a weakness. This approach was adopted to make the review more feasible and the synthesis more appropriate. Furthermore, because the synthesis does not rely on quantitative concepts, and the contents extracted from included studies were sufficient, we believe excluding these papers did not affect the overall results.
Implications for practice, policy and research
Continuity and coordination of care seemed to be significant gaps in care provision along with the great challenge of uncertainty. The important point is to acknowledge uncertainty of illness trajectory – and for HCPs to share this acknowledgement with patients and carers – and develop a joint strategy or care plan to help manage it. To accept and deal with uncertainty has in fact been suggested as being a part of medical generalist services. 77 Paying attention to detail, being sensitive to patients’ and carers’ concerns and creating innovative solutions that are pertinent to compassionate care are ways to overcome the challenges caused by uncertainty.61,78
Enhancing interdisciplinary work not only increases the capacity as a team to support patients with a great extent of uncertainty in their illness trajectory but also enables more coordinated care to assure continuity. It is necessary to develop a better framework or better ways to utilise existing frameworks to achieve effective collaboration particularly in relation to palliative care for non-cancer patients. The existing care models should receive more in-depth evaluation in terms of how they work and what impact they have on multidisciplinary teams to inform future policymaking. Based on the findings of this review, as Barclay mentioned, 79 palliative care specialists should probably concentrate on short-term intensive input to more complicated cases rather than maintaining long-term relationships with patients.
Conclusion
Our review found that patients expect GPs to provide compassionate care, have appropriate knowledge and play central roles in coordinated care. Uncertainty of the illness trajectory, unclear definition of the role of professionals and lack of collaboration between professionals are identified as barriers to effective primary palliative care provision to non-cancer patients. It is crucial to increase the capacity to deal with uncertainty as a team through effective interdisciplinary work. Clear role definitions of each professional and effective interprofessional collaboration will help to manage many challenges encountered in delivering palliative care to non-cancer patients in the community. Research into and development of a best model for effective interdisciplinary work are needed for better primary palliative care provision for non-cancer patients.
Footnotes
Appendix
Selected search terms
| Group 1 | non-malignan* |
| non-cancer* | |
| non-oncolog*. mp. | |
| stroke | |
| cerebrovascular* | |
| pulmonary emphysema | |
| chronic obstructive pulmonary disease/COPD | |
| neurodegenerative diseases | |
| motor neuron* disease/MND | |
| amyotrophic lateral sclerosis/ALS | |
| parkinson* disease | |
| multiple sclerosis/MS | |
| multiple system atrophy | |
| progressive supranuclear palsy | |
| acquired immunodeficiency syndrome/AIDS | |
| human immunodeficiency virus infection/HIV | |
| dementia | |
| huntington* | |
| heart failure | |
| chronic kidney failure | |
| end stage liver disease | |
| Group 2 | palliative care |
| terminal care | |
| terminally ill | |
| end of life | |
| Group 3 | family practice/family medicine/family physician |
| general practice/general practitioner | |
| primary health care | |
| community health services | |
| community health nursing | |
| public health nursing | |
| Group 4 | attitude of health personnel |
| attitude to death | |
| delivery of health care | |
| health service accessibility | |
| clinical competence |
Acknowledgements
Thanks to Ms Denise Brady for review of search headings and to Professor Popay and colleagues for development of guidance on narrative synthesis. The authors also would like to thank Professor Masato Matsushima for his helpful comments on the paper.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.