
Abstract
Background:
Previous end-of-life cancer research has shown an association between increased family physician continuity of care and reduced use of acute care services; however, it did not focus on a homecare population or control for homecare nursing.
Aim:
Among end-of-life homecare cancer patients, to investigate the association of family physician continuity with location of death and hospital and emergency department visits in the last 2 weeks of life while controlling for nursing hours.
Design:
Retrospective population-based cohort study.
Setting/participants:
Cancer patients with ≥1 family physician visit in 2006 from Ontario, Canada. Family physician continuity of care was assessed using two measures: Modified Usual Provider of Care score and visits/week. Its association with location of death and hospital and emergency department visits in the last 2 weeks of life was examined using logistic regression.
Results:
Of 9467 patients identified, the Modified Usual Provider of Care score demonstrated a dose–response relationship with increasing continuity associated with decreased odds of hospital death and visiting the hospital and emergency department in the last 2 weeks of life. More family physician visits/week were associated with lower odds of an emergency department visit in the last 2 weeks of life and hospital death, except for patients with greater than 4 visits/week, where they had increased odds of hospitalizations and hospital deaths.
Conclusions:
These results demonstrate an association between increased family physician continuity of care and decreased odds of several acute care outcomes in late life, controlling for homecare nursing and other covariates.
Introduction
Family physicians (FPs) have an important role in providing palliative and end-of-life care, particularly in home- and community-based settings, as noted in Canadian and international settings.1–4 Studies have shown that a majority of patients prefer to be cared for and die at home, rather than in hospital or acute care settings.5–8 As well, home- and community-based settings are important to investigate because of the policy trends to shift more care for patients outside the acute care hospital system. Often, the patients receiving end-of-life and palliative care in the community have a diagnosis of cancer, mostly because of cancer’s more predictable disease trajectory. 9 Cancer patients at the end of life and their families rely on FPs’ clinical expertise to manage symptoms, which are often multiple and complex, as well as psychosocial issues, prescriptions, and treatments. 10
Cancer researchers have investigated the involvement of FPs in end-of-life care through the lens of continuity of care,11–14 defined as the “degree to which a series of discrete healthcare events are experienced as coherent and connected and consistent with the patient’s medical needs and personal context.” 15 Having an involved FP can lead to successfully caring for the patient at home by being better able to prevent clinical problems and providing immediate response to urgent issues; moreover, having a consistent FP who understands the patient and family needs, the changing disease trajectory, and family dynamics can improve the quality of care.3,16–18 This in turn could lead to decrease in the use of hospital and emergency department (ED) resources, which are important factors to improve quality and the efficiency of the health-care system.19,20 In one systematic review analyzing continuity of care, eight of nine high-quality studies found a significant association between increased continuity and decreased hospitalizations and ED visits; 21 these studies, however, did not focus on cancer patients or the end-of-life phase. Another systematic review focusing on interventions to improve continuity of care for cancer patients identified 51 studies but could not conclude on the effectiveness of the interventions because of the variation between intervention models and phases of cancer care. 22 A limited amount of research has focused on continuity of cancer care at the end-of-life phase specifically: Burge et al.23,24 conducted research that demonstrated increased continuity of care with an FP was associated with decreased hospital deaths and ED visits. However, these analyses did not control for end-of-life homecare nursing visits, which have also been shown to independently reduce ED visits, hospitalizations, and hospital deaths. 25 Thus, a major gap in knowledge involves examining the independent role of the FP in end-of-life home setting while controlling for homecare nursing visits because often both the FP and homecare providers deliver important clinical services to patients and family during end-of-life care.
This research will investigate the association between FP continuity of care among a population-based cohort of end-of-life homecare cancer patients and three acute care outcomes while controlling for homecare nursing hours. The three acute care outcomes are validated measures of end-of-life care quality: hospitalization and ED visits in the last 2 weeks of life, respectively, and dying in hospital.
Methods
Study design
This study examined a population-based cohort of cancer patients in Ontario, Canada during the calendar year 2006, which was the most recent year for which cancer registry data were available at the time of analysis. Patients had to have a confirmed cancer diagnosis, had to be older than 18 years, and have a valid provincial health insurance number. The exposure period was defined as the date of end-of-life homecare designation (up to a maximum of 365 days prior to death) until 14 days prior to date of death, the last 14 days during which the outcome events were measured. Thus, we also excluded those who were referred to homecare <2 weeks before death. We examined patients who had zero FP visit after end-of-life homecare designation distinctly and did not use them as the reference group since the independent variables measured level of FP involvement, and reason for no FP visit varies considerably.
Data sources
The study involves the retrospective analysis of the population of Ontario, obtained through the linkage of individual data contained in the following administrative health databases: (1) Registered Persons Database (RPDB); (2) Ontario Health Insurance Plan (OHIP) database; (3) Discharge Abstract Database (DAD); (4) National Ambulatory Care Reporting System (NACRS); (5) Homecare Database (HCD); (6) 2001 Census; and (7) Ontario Cancer Registry (OCR). The cohort was identified by using the RPDB, 26 which records gender and date of death. Date of death was assigned as time zero and then counted backwards in days from death to homecare admission, which ensured that patients were compared equally across time. The OHIP database provided information about number and dates of specialty and FP visits provided to each patient. The DAD contained data for all hospital admissions, including death in a hospital, 27 and was also used to assess comorbidities via the Charlson score. 28 NACRS contained data for all ED visits. HCD provided data on date of end-of-life homecare designation and amounts and dates of homecare nursing services used. Census data were used to classify patients according to their postal code by income quintile and rurality. Finally, the OCR confirmed cancer diagnosis and cause of death by cancer.29,30
Variables
Outcomes (dependent variables)
There were three outcomes of interest related to acute care utilization in late life: (1) having a hospitalization in the last 2 weeks of life (yes/no); (2) having an ED visit in the last 2 weeks of life (yes/no); and (3) dying in hospital (yes/no).
Variables of interest (independent variables)
A systematic review of indices for continuity of care 31 identified 44 articles that included 32 different measures of continuity of care. We chose two different measures of FP continuity of care to allow for greater understanding of the role of FPs in end-of-life cancer care and analyzed them separately.
Modified Usual Provider of Care (MUPC) continuity score. The original UPC was used in 1432–43 of the 44 articles cited in the systematic review, 31 making it the most widely used, defined as the “fraction of visits made to the usual provider.” However, we modified this definition as applied to our study because our administrative data linkage is not able to identify individual providers, but instead provider specialty, where FP specialty is one category. Therefore, MUPC measures continuity of FP involvement. Second, our data showed that over 85% of all physician visits in the last year of life were made to either the oncologist or FP specialty, and we excluded the other subspecialties as they were likely unrelated to patients’ end-of-life cancer care. Thus, MUPC is calculated by taking a fraction of total FP visits made during the exposure period over the total number of visits made to FPs plus oncology physicians.

MUPC measure yields scores ranging from 0.01 to 1, with the lowest indicating low continuity within the FP specialty. These scores were further categorized into low (<0.5, reference group), medium (0.5 to <0.8), and high (0.8 or greater) continuity as per prior research. 24 Note, in Canada, the palliative care is a subspecialty within family medicine. Therefore, we are not able to differentiate care by an FP versus palliative care physician. However, the number of full-time palliative care physicians in the community is very small in Ontario, meaning most patients do not get access to a palliative care specialty physician. The remaining physicians in the community, with palliative care expertise, also have a family practice.
FP visits/week. This measures the frequency of visits to an FP on a weekly basis to assess continuity and involvement. It is defined as the average number of FP visits/week during the exposure period, excluding the days patients spent in hospital.
Confounding variables
Several confounding variables, identified in previous studies, were controlled for in adjusted analyses: age at death, sex, income quintile, duration of time in homecare (exposure time), rurality (community of <10,000 people),
44
comorbidities via the Charlson score (dichotomized as 0
Statistical analysis
Logistic regression analysis was conducted to analyze the odds of having each of the outcomes of interest. Analyses were performed separately for each outcome. All variables were retained for the multivariate model to compare these results with previous research. Statistical significance was defined as a p value of 0.05 or less, and all tests were two-sided. All analyses were conducted using SPSS (version 19). An analysis was performed excluding those having no FP, which produced similar results, thus only the results including all patients are presented for brevity. This study was approved by the research ethics committee of Sunnybrook Health Sciences Centre and followed privacy guidelines of the Institute for Clinical Evaluative Sciences.
Results
In Ontario, 34,625 cancer patients died during 2006, of which 9467 patients received end-of-life homecare services for at least 2 weeks before death. Of those, 1380 had no visits to an FP after end-of-life homecare designation, whereas 8078 patients had at least 1 FP visit (see Table 1). Among those with at least 1 FP visit, half were males. Those aged 70–79 years comprised about one-third of the cohort. Of all five cancer categories, a quarter of patients died of lung cancer, compared to 9% for breast and 12% for colorectal cancer. The majority (86%) resided in urban areas. Of the patients, 36% were in homecare for 5 to 12 weeks, with 10% in homecare for duration of 3 to 4 weeks. The mean homecare nursing hours/week received was 2.85 (standard deviation (SD) = 2.72). Conversely, among those with no FP visits, the demographic characteristics were very similar, except that they were more likely to be referred to end-of-life homecare close to death, with over half being referred in the last month of life.
Patient characteristics.
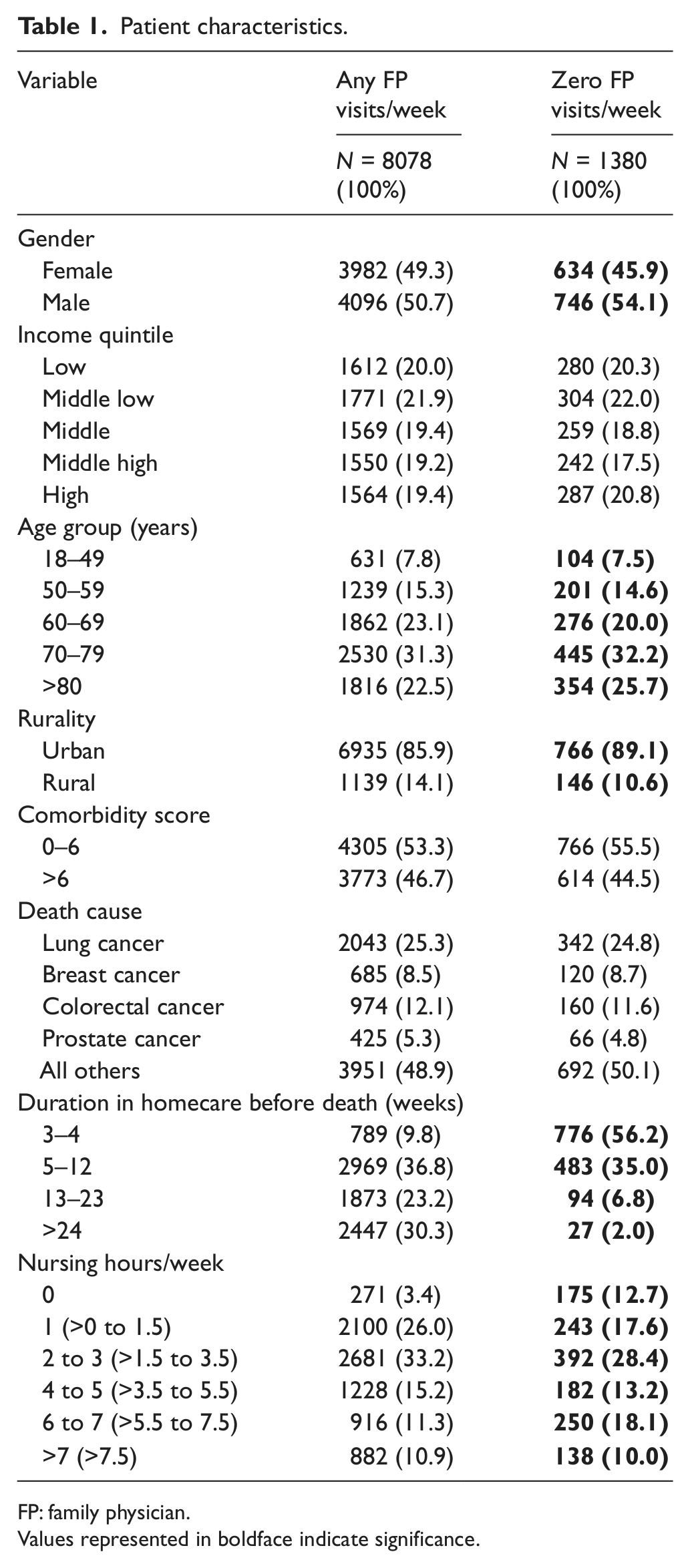
FP: family physician.
Values represented in boldface indicate significance.
Among those with any FP visits, the mean MUPC score was 0.66 (SD = 0.294). Approximately 41% had a high MUPC continuity score (0.8 or higher), 29% had a medium score (0.5 to <0.8), and 30% had a low score (<0.5) on the continuity scale. In addition, the median FP visits/week was 0.75 (10th% = 0.19; 90th% = 2.63). A third of patients had an average of ≤0.5 FP visit/week, 25% had >0.5 to 1 visit/week, and 9% had >4 visits/week. Of all FP visits, the proportion that was home visits was 15.8%, meaning the majority were in-office visits. In the 2 weeks before death, about half (49%) had a hospitalization and 24% had an ED visit, while 40% died in a hospital.
MUPC continuity score
The multivariate analysis indicates that higher MUPC continuity scores were associated (p < 0.001) with lower likelihood of having any of the three outcomes (see Table 2). Compared to those with low continuity scores, those with medium MUPC scores were 0.76 (95% confidence interval (CI): 0.68–0.85) times as likely to visit the hospital in the last 2 weeks of life, while those with high MUPC continuity scores were 0.51 (95% CI: 0.46–0.57) as likely, after controlling for other covariates. The same dose–response trend was evident for increasing MUPC continuity score and lower likelihood of death in hospital and having an ED visit in the last 2 weeks of life.
Association of continuity of FP care and acute care outcomes in late life, controlling for other covariates.
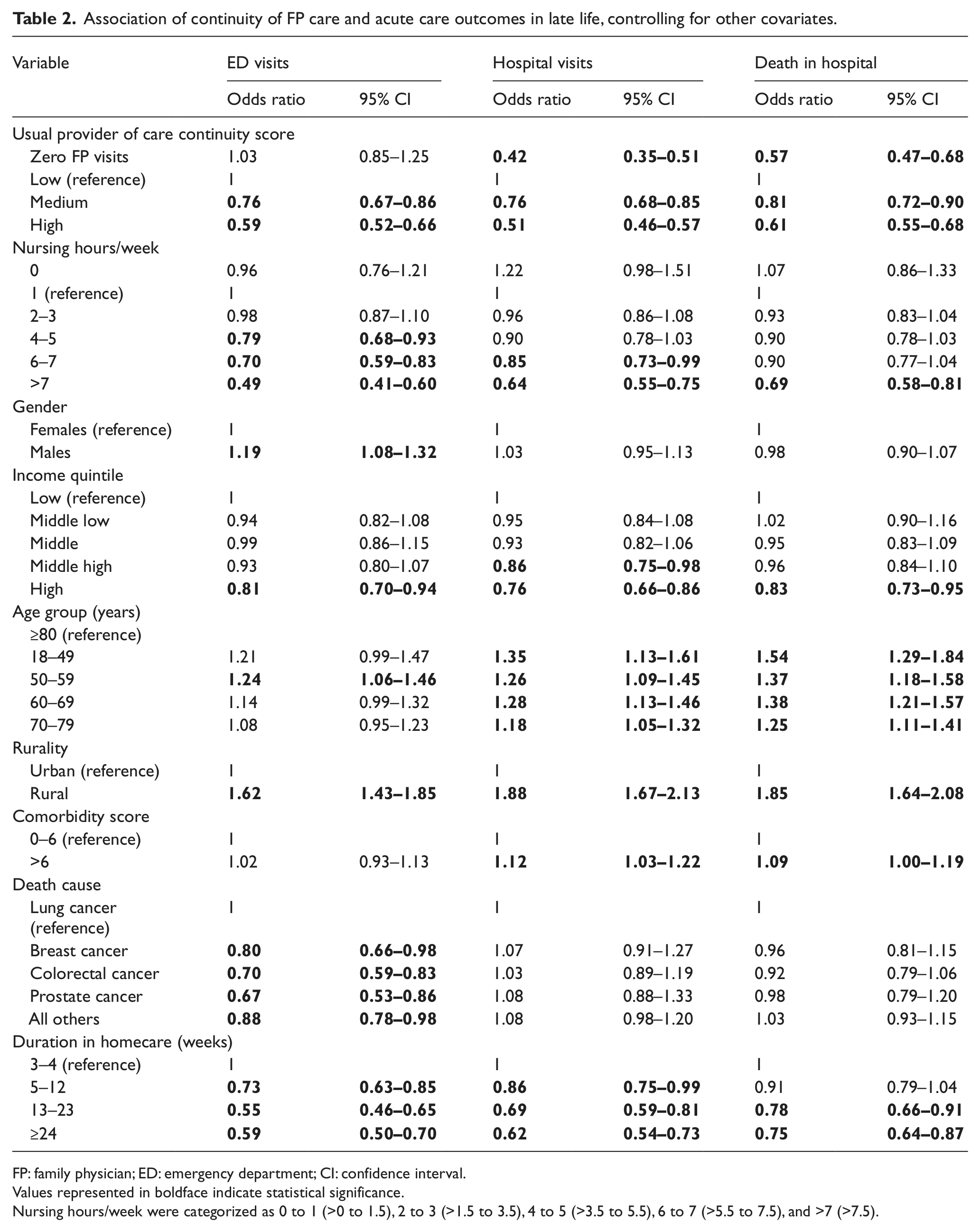
FP: family physician; ED: emergency department; CI: confidence interval.
Values represented in boldface indicate statistical significance.
Nursing hours/week were categorized as 0 to 1 (>0 to 1.5), 2 to 3 (>1.5 to 3.5), 4 to 5 (>3.5 to 5.5), 6 to 7 (>5.5 to 7.5), and >7 (>7.5).
FP visits/week
The association between FP visits/week and the three outcomes was varied, after controlling for other covariates (see Table 3). Increased FP visits/week reduced the likelihood of having an ED visit in the last 2 weeks of life in a dose–response manner: compared to control patients with >0 to 0.25 FP visits/week, patients with >0.25 to 0.50 visits/week had a 24% decreased odds of an ED visit (95% CI: 0.64–0.89), while those patients with greater than 4 visits/week had an 85% decreased odds (95% CI: 0.11–0.20). Moreover, compared to control patients, those receiving between 0.25 and 4 visits/week had an approximate 15% decrease in the odds of dying in hospital; however, those patients with >4 visits/week were 1.67 times more likely to die in hospital (95% CI: 1.38–2.01). Increasing FP visits were not significantly associated with fewer hospital visits, except those patients with greater than 4 FP visits/week, who were 2.25 times (95% CI: 1.85–2.74) more likely to have a hospital visit in the last 2 weeks of life compared to the control patients.
Association of FP visits/week and acute care outcomes in late life, controlling for other covariates.
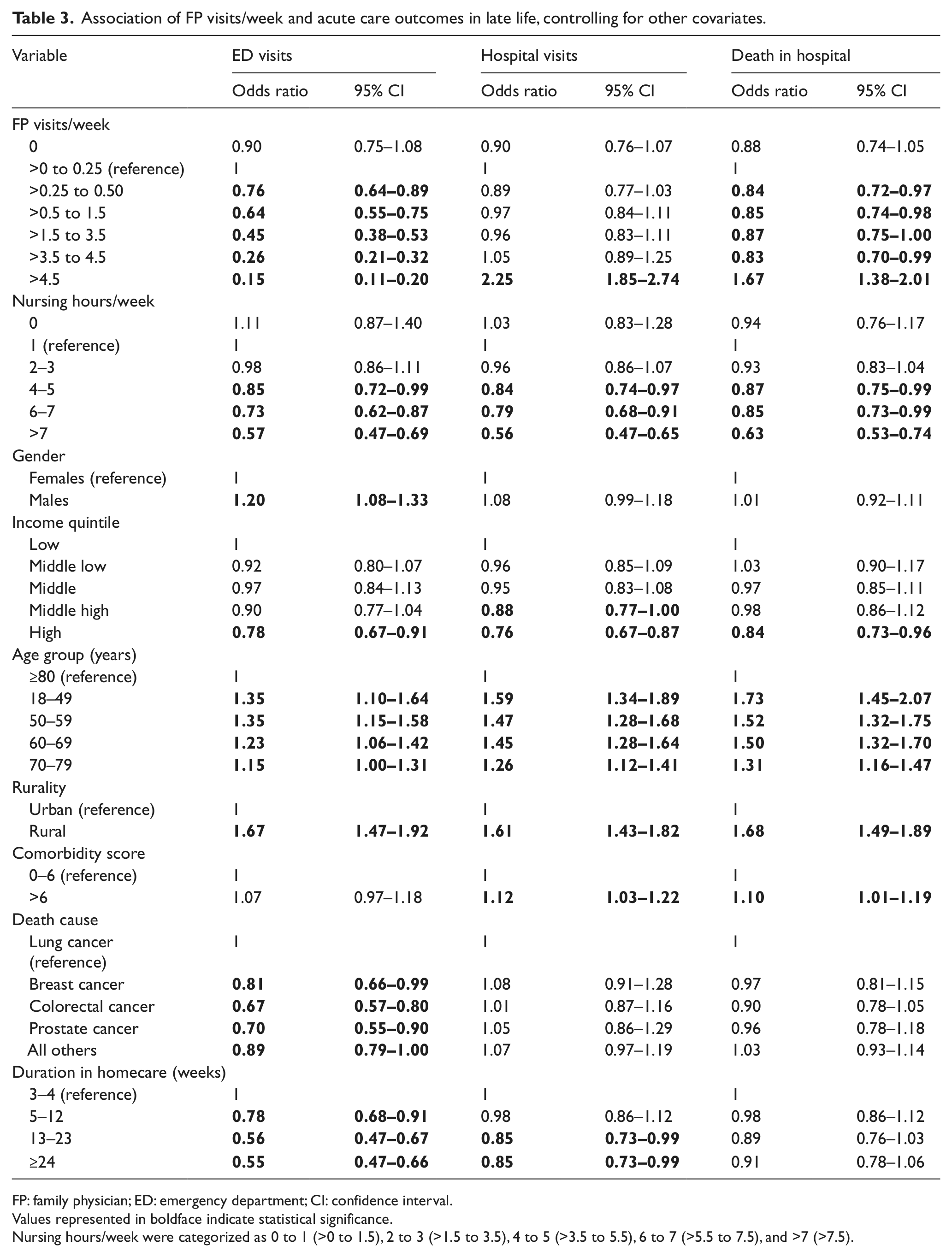
FP: family physician; ED: emergency department; CI: confidence interval.
Values represented in boldface indicate statistical significance.
Nursing hours/week were categorized as 0 to 1 (>0 to 1.5), 2 to 3 (>1.5 to 3.5), 4 to 5 (>3.5 to 5.5), 6 to 7 (>5.5 to 7.5), and >7 (>7.5).
Other covariates
When examining the association between either mean FP visits/week or continuity of care and the three outcomes, a few variables consistently decreased the odds of having the outcomes. When using the FP visits/week measure, the more nursing hours patients received (>3 h/week), the less likely they were to have any of the three outcomes in a dose–response manner; however, when using MUPC measure, they were significantly less likely to have any of the three outcomes only when average nursing hours/week was greater than 7. Similarly, for duration in homecare generally, the odds of having any of the outcomes are reduced when patients are enrolled in end-of-life homecare earlier. Other factors that were consistently associated with a decreased likelihood of having any of the three outcomes included being in the highest income quintile, increasing age, living in a nonrural community, and having a lower comorbidity score (0–6).
Discussion
Our population-based analysis of end-of-life homecare cancer patients with any FP visits found a significant dose–response relationship—as FP continuity of care score (MUPC) declines (i.e. more oncologist involvement as a proportion of all visits), hospital and ED use and the likelihood of dying in the hospital increase, even after controlling for covariates known to be prognostic. Similarly, more FP visits/week led to lower odds of ED use in the last 2 weeks of life in a dose–response fashion. We found a 15% threshold of decreased odds of dying in hospital with more FP visits compared to the reference, except for patients with >4.5 FP visits/week—they were 1.67 times more likely to die in hospital and 2.25 times more likely to have a hospitalization in the last 2 weeks of life. Our study is novel in that it examined continuity of FP care at end of life by relying on two measures: FP visits/week and MUPC score. Although continuity is measured at the specialty level, and not at the individual provider level, our key finding suggests that generally more involvement from an FP in the community is independently associated with less acute care use at late life, even after controlling for homecare nursing.
These results advance prior research findings23–25 by controlling for both FP involvement and homecare nursing. When considering FP visits/week, our multivariate model corroborated the dose–response relationship with greater than 3 nursing hours/week found by Seow et al. 25 across all three outcomes; however, when using MUPC, nursing hours only showed significance across all three outcomes for 7 or more hours/week. Our results also supported other research findings. For example, earlier referral led to less use of acute care services, and lung cancer patients used more acute care services than other cancer types. 19
Perhaps the most interesting finding in this study was that more FP visits/week were associated with fewer ED visits in a dose–response manner (like continuity of care), but an opposite trend of more hospitalizations and more hospital deaths when greater than 4 physician visits/week was observed. These are related as a late-life hospital admission often leads to a hospital death as the patient does not have sufficient time to become well enough to leave the hospital. One hypothesis for this finding is that the patients with ≥4 FP visits/week were more medically complex compared to other patients. Thus, having a hospitalization in the last 2 weeks of life may have been necessary and appropriate, perhaps even planned by the physician as a direct admission. Conversely, data show that ED visits occur because of inadequate symptom control, such as uncontrolled pain, and failure to cope. 45 Thus, more visits with the FP may avoid these emergencies by anticipating and identifying problems early and making care arrangements in advance, particularly for those who can appropriately be cared for at home. Another noncompeting hypothesis is that the increase in hospitalizations for those with greater than 4 FP visits/week could be admissions to a hospital’s palliative care unit, which would likely be appropriate care for sicker patients; unfortunately, our data analysis could not determine the type of unit for hospital admissions.
The study is limited in the inability to attribute visits to an individual provider–only FP specialty. However, we assume that most patients have only one FP. Also, we were not able to differentiate FPs with palliative care specialty from “regular” FPs. However, our interpretation of results holds that more care from an FP in the community is associated with fewer acute care visits. Using administrative databases cannot determine the appropriateness of any ED or hospital visits, patient and family preferences for treatment and goals of care, which could affect location of death or service choices, and the quality of the care delivered by providers. Moreover, within the administrative data, a hospitalization in an inpatient ward could not be differentiated from a palliative care bed, which might explain the high rates of hospitalization and hospital death among the sicker patients with greater than 4 FP visits/week.
In this study examining cancer patients receiving end-of-life homecare services, more FP continuity of care (MUPC) was associated with lower acute care service use, and more FP involvement (visits/week) was associated with less ED visits and hospital deaths, except for the presumably sickest patients receiving an average of >4 visits/week. These results support the evidence base that providing increased homecare and FP involvement together in community- and home-based settings are associated with reduced odds of using acute care services late in life. These results could support policies that encourage FPs to provide care to dying cancer patients in the community.
Footnotes
Declaration of conflicting interests
The authors have no conflicts to declare. The opinions, results, and conclusions reported in this article are those of the authors. No endorsement by ICES, CCO, or the Government of Ontario is intended or should be inferred.
Funding
This study was conducted with the support of the Ontario Institute for Cancer Research and Cancer Care Ontario through funding provided by the Government of Ontario and with the support through provision of data by the Institute for Clinical Evaluative Sciences (ICES) and Cancer Care Ontario (CCO) and through funding support to ICES from an annual grant by the Ministry of Health and Long-Term Care (MOHLTC).