
Abstract
Background:
Many patient-reported outcome measures have been developed in the past two decades, playing an increasingly important role in palliative care. However, their routine use in practice has been slow and difficult to implement.
Aim:
To systematically identify facilitators and barriers to the implementation of patient-reported outcome measures in different palliative care settings for routine practice, and to generate evidence-based recommendations, to inform the implementation process in clinical practice.
Design:
Systematic literature review and narrative synthesis.
Data Sources:
Medline, PsycInfo, Cumulative Index to Nursing and Allied Health Literature, Embase and British Nursing Index were systematically searched from 1985. Hand searching of reference lists for all included articles and relevant review articles was performed.
Results:
A total of 3863 articles were screened. Of these, 31 articles met the inclusion criteria. First, data were integrated in the main themes: facilitators, barriers and lessons learned. Second, each main theme was grouped into either five or six categories. Finally, recommendations for implementation on outcome measures at management, health-care professional and patient levels were generated for three different points in time: preparation, implementation and assessment/improvement.
Conclusions:
Successful implementation of patient-reported outcome measures should be tailored by identifying and addressing potential barriers according to setting. Having a coordinator throughout the implementation process seems to be key. Ongoing cognitive and emotional processes of each individual should be taken into consideration during changes. The educational component prior to the implementation is crucial. This could promote ownership and correct use of the measure by clinicians, potentially improving practice and the quality of care provided through patient-reported outcome measure data use in clinical decision-making.
Keywords
Introduction
Measurement is a fundamental component of evidence-based medicine and provides the necessary information clinicians require to make decisions in patient management. However, patients are increasingly active in their own treatment; therefore, collecting biological, laboratory information and mortality rates only is no longer adequate. 1 Other outcomes such as health status, level of disability and quality of life are now common in the literature. It is commonly asserted that the patient’s perspective should inform in clinical decision-making and direct collection of outcome data from the patient should be incorporated in clinical practice.1–6 Patient-reported outcome measures (PROMs) are ‘standardised, validated questionnaires that are completed by patients to measure their perceptions of their own functional status and wellbeing’. 2 In the past two decades, many PROMs have been developed, and increasingly, their role in clinical practice has been emphasised.1,2,7,8 PROMs are considered to be the gold standard for outcome measurement of subjective experiences, because the information captured comes directly from the patient and well-validated tools reflect the concerns and main problems of the clinical population.1,9 In palliative care settings, systematic collection of patient-reported outcomes using validated questionnaires may benefit clinical practice both at the population and individual patient level. This may be achieved by the following mechanisms: (a) facilitating identification and screening of physical, psychological, spiritual and social unmet needs that might otherwise be overlooked; (b) providing information on disease progression and impact of treatment prescribed; (c) facilitating patient/family/carer–clinician communication, promoting the model of patient-centred care by shared decision-making and advanced care planning, establishing common priorities and expectations regarding outcomes of treatment and disease progression, which does not mean using a PROM to act as a substitute for the therapeutic relationship, but rather to complement it; and (d) monitoring outcomes by performing audits as a strategy for improvement of the quality of care provided and its costs.10,11 Finally, if funding health-care institutions were to be allocated depending on performance and outcomes of the services, having those data available would be critical.
Models have been developed to fit health-related quality of life (HRQoL) and other PROMs data collection into clinical practice. 12 Building on Wilson and Cleary’s 12 conceptual model of patient outcomes, Osoba developed a model for HRQoL assessment, describing how to incorporate HRQoL measures into clinical practice, throughout the disease trajectory. Outcome measures are used like a conventional laboratory test, that is, to inform the differential diagnosis and monitor a patient’s progress. These types of data can be helpful in several phases of a condition or disease management: during the initial history and physical examination, laboratory and imaging procedures of investigation leading to a diagnosis, all phases of treatment and follow-up. 13 However, despite recommendations, the routine use of PROMs in palliative care clinical practice has been slow to implement, so their optimal role in assisting decision-making and improving quality of care is yet to be achieved.2,14
In other areas, for example, psychiatry, work has been developed on implementing PROMs in clinical practice where it has been suggested that to implement outcome measurement in a clinical unit and have clinicians conduct it as part of their clinical routine, takes at least 1 year. 15 Despite the evidence indicating that routine outcome assessment has benefits for mental health patients, there are a number of reasons as to why it has not been adopted in most services. 16 These include lack of appropriate instruments, time and incentives (financial and professional); lack of consensus regarding what outcome domains to include and what assessment measures to use; and clinicians remaining unconvinced of the benefits of routinely monitoring outcomes. Furthermore, barriers to successful screening for depression in cancer settings involve patient and clinician factors: acceptability of screening is critical to implementation, clinician confidence/skills influence screening success and training may improve confidence but effects upon long-term outcomes are modest. 17 The latter seems to be a consequence of not providing clinicians with interpretation of scores, no mandating follow-up, not linking screening with training or other types of clinician support, and screening being generally ineffective without aftercare. 17
Two frameworks that have been developed are relevant for this review. One pertains to the implementation of clinical practice guidelines that describes five steps: assessment of clinician’s stage of readiness to change, assessment of specific barriers to guideline use, determination of appropriate level of intervention, design of dissemination and implementation strategies and evaluation of the strategies implemented. 18 The other, ‘Promoting Action on Research Implementation in Health Services’ (PARIHS) framework was developed to incorporate research into practice.19–21 It suggests that successful implementation is a function of the relation between the nature of the evidence, the context in which the proposed change is to be implemented and the mechanisms by which the change is facilitated. It is advocated that (a) implementing research into practice is an organisational issue rather than an individual one; (2) there is a need to carefully plan implementation strategies such as interventions that address the need for education, audit and the management of change and (c) criteria for evaluating the impact of the intervention must be identified and agreed upon before implementing any change. The role of the facilitator seems to be paramount as the facilitation is considered to be an intervention for getting research into practice. Finally, the facilitation process is also emphasised in a study, which aimed at implementing two end-of-life care tools in care homes. 22 A model of high facilitation was used. This included an experienced palliative care nurse facilitating the project and visiting the sites multiple times and key champions attending a 4-day facilitative course and cascading this training down to their own staff.
Systematic reviews on the use of outcome measurement in clinical practice have focused on the impact and effectiveness of PROMs in clinical practice but none of them covered the process of implementing the measures.23–25 There is a brief review exploring assessment of only quality of life in one particular setting, that is, oncology practice. 26 Understanding the facilitators and barriers to the implementation of PROMs in palliative care settings could potentially inform the process of their implementation. Therefore, this review aimed to systematically identify facilitators and barriers to the implementation process of routine use of PROMs in different palliative care settings and generate evidence-based recommendations, to inform the implementation process in clinical practice. The objectives of this review were to (a) identify barriers and facilitators to the systematic implementation of PROMs in palliative care clinical practice, (b) identify needs and other comments of clinical teams regarding the routine use of PROMs and (c) identify lessons learned on the process of implementation of PROMs in clinical practice.
Methods
Design
This systematic review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations. 27
Study identification
Studies were identified using a systematic search of electronic databases with additional hand-searching of reference lists of included articles. 27
Search strategy
Five databases (Medline, PsycInfo, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase and British Nursing Index (BNI)) were searched and included the literature published between 1985 and August 2011. It was decided to exclude all the literature before 1985 because PROMs only start to emerge in the literature in the late 1980s. The searches were conducted between 29 August 2011 and 2 September 2011. The search was updated on 19 March 2012. Using Medical Subject Heading (MeSH) terms and free text, keyword groups, including ‘palliative care’, ‘PROMs’, ‘clinical practice’ and ‘facilitators and barriers’, were combined in several ways. Slight changes were made according to each database. Appendix 1 has the full search strategy for BNI. Data search was supplemented by hand search of reviews and relevant articles.
Study selection
Inclusion criteria are as follows: (a) primary studies reported in English, Portuguese, Spanish, Italian, German and French because these languages were spoken in the wider study team; (b) studies using a PROM alongside the clinical care of adult patients (18 years old or older) with advanced disease in palliative care settings; and (c) studies reporting barriers and/or facilitators of the implementation of the PROM. Articles had to meet all the inclusion criteria, and no exclusion criteria to be included. All study designs were included.
Exclusion criteria are as follows: (a) published literature other than primary studies (i.e. review articles, books and conference articles); (b) studies reporting exclusively on development and feasibility phases of new measures, which did not include comments of users; and (c) studies of PROMs completed by proxies.
Selection procedure
All titles and abstracts were reviewed by one reviewer (B.A.) to assess eligibility for inclusion in the review. Full texts were retrieved if the inclusion criteria were met or the abstract contained insufficient information. Any uncertainty about eligibility after assessing full text was assessed by a second reviewer (I.J.H.).
Data extraction
Data were extracted by one reviewer (B.A.) and assessed by a second reviewer (N.C.). Tabulation was used as a first step. The author, country, aim, population, study design, measures used, settings, facilitators and barriers were extracted. Clauses were taken and kept as reported.
Analysis
Incorporating qualitative data into systematic reviews has been recognised as an important contribution for providing and analysing non-numerical research data by answering questions that are not easily addressed exclusively by experimental methods.28,29 Hence, a narrative synthesis was conducted following a framework of four elements to ensure robustness of the findings as described in the Guidance on the Conduct of Narrative Synthesis in Systematic reviews. 30 Element 1 concerns the role of theory in evidence synthesis, Element 2 refers to the development of a preliminary synthesis, Element 3 pertains to exploring relationships within and between studies and in Element 4, the robustness of the synthesis is assessed. This method has proved to be useful in synthesising different types of data from different study designs. 31 There is more than one technique to choose from in order to conduct Elements 2–4, depending on the data extracted, and the following were the chosen techniques for each element in this review:
Element 1: the role of theory in evidence synthesis. We present a theory as suggested in the guidance, which will contribute to the interpretation of the findings and the assessment of how widely applicable the findings might be.
Element 2: developing a preliminary synthesis. Element 2 was achieved by (a) grouping the data by tabulation and (b) performing thematic analysis. This allowed for the systematic identification of the main themes.
Element 3: exploring relationships within and between studies. Element 3 was achieved by (a) exploring the influence of heterogeneity by focusing attention on the characteristics of the different studies and their potential relationships to the findings, (b) reciprocal translation by identifying common concepts across studies and (c) conceptual mapping was performed linking multiple pieces of evidence extracted from the different studies representing the relationships between them. Categories were first developed for each main theme. Data were then organised in a timeline, by implementation steps and sequenced actions. Any discrepancies were resolved by discussion (B.A. and N.C.).
Element 4: assessing robustness of the synthesis. There are two steps to carry out described in the guidance, as follows: (a) assessing the methodological quality of included studies and (b) being rigorous in the methodology used to synthesise findings and being critical regarding limitations of methods used. The latter will be included in the ’Strengths and limitations’ section given under the ‘Discussion’ section. There are no universally accepted guidelines for either assessing the quality of specific qualitative methods nor an accepted set of criteria to assess the quality of qualitative and quantitative studies in order to incorporate their findings in a systematic review.28–30,32–36 We used the modified Harden criteria to assess the methodological quality of the included studies (Table 1).37,38 Two reviewers (B.A. and V.S.) assessed the quality of the studies independently. Discrepancies were resolved by discussion. Studies with a qualitative design were assessed according to 16 criteria subdivided into two dimensions: clarity of reporting and robustness of the study methods. The first dimension refers to a clear description of context, study aims, research question, choice of specific study design, sampling, data collection, analysis and findings and has a maximum score of 8. The second refers to a comprehensive sampling strategy, reliability and validity of the data collection and analysis. It roots the findings in the perspectives and experiences of the respondents, logically proceeding from data to interpretation and reflexivity, which has a maximum score of 8. Regarding the studies with a quantitative design, 13 criteria were used, also subdivided in those two dimensions. The maximum possible score for robustness of study methods was 5. If the study used a mixed-methods approach, then the methodology that provided the data of interest for this review, was rated. Each criterion was rated as ‘yes’ or ‘no’, and if there was insufficient information, the score was ‘no’. Studies were rated by both reviewers as ‘high’, ‘medium’ or ‘poor’ quality. However, no studies were excluded based on the quality score because there is no consensus on the minimum quality assessment score required for inclusion in a review. 29
Quality assessment instruments for qualitative and quantitative studies.
The original 10 criteria from Harden are printed in italic format.
Results
Identification and inclusion of studies
The search strategy yielded a total of 3863 hits. Following screening of titles and abstracts (Figure 1), 421 articles were reviewed in full detail and 393 were excluded for not having comments on PROMs use, implementation of the measure(s), nor use in clinical practice. Twenty-six studies were included within 31 articles.
Flow chart based on PRISMA recommendations reporting the literature search and selection of articles.
Eleven studies were conducted in the United Kingdom, seven in the United States, two in the Netherlands and one in each of the following countries: Australia, Canada, Israel, Italy, Malaysia and Vietnam (Table 2). There were no intervention studies testing the introduction of facilitators to overcome barriers when implementing PROMs in clinical practice. Eight studies used qualitative methods and provided structured, in-depth information about the facilitators, barriers and lessons learned when implementing PROMs in palliative care clinical practice. These studies used a range of designs (n = 4) including web-based online surveys, semi-structured interviews with patients and clinicians either face to face or by phone and meetings with clinical teams and focus groups. Seventeen studies used quantitative methods (n = 7) and none looked at facilitators or barriers to the implementation of PROMs as a primary outcome. One randomised controlled trial evaluated the efficacy of standardised HRQoL assessments used in facilitating patient–physician communication. The PROMs used in the studies include seven measures on pain, seven on symptoms, eight on quality of life and six measuring other concepts (Table 2).
Characteristics, measures used and quality assessment of included studies (N = 31).
PROM: patient-reported outcome measure; CMS: Centers for Medicare and Medicaid Services; PCOC: Palliative Care Outcomes Collaboration; MND: motor neurone disease; HRQoL: health-related quality of life; GP: general practitioner; RCT: randomised controlled trial; QoL: quality of life; ART: antiretroviral treatment; PSAR: The Ottawa pain and symptom assessment record; POS: Palliative care Outcome Scale; N/A: not applicable; ESAS: Edmonton Symptom Assessment Scale; MVQOLI-R: Missoula-VITAS Quality of Life Index–Revised; MSAS: Memorial Symptom Assessment Scale; EQ-5D: European Quality of Life-5 Dimensions; SAS: symptom assessment scale; RUG-ADL: Resource Utilization Group/Activities of Daily Living; KPS: Karnofsky Performance Score; PCPSS: Palliative Care Problem Severity Score; EORTC QLQ-C30: European Organization for Research and Treatment of Cancer, Quality of Life Questionnaire Core 30; COOP: Dartmouth Primary Care Cooperative Information Functional Health Assessment; WONCA: World Organization Project of National Colleagues and Academics; SF-36: Medical Outcomes Study 36-Item Short-Form Health Survey; ECOGS: Eastern Cooperative Oncology Group scale; PSQ C: Patient Satisfaction Questionnaire C; NRS: numeric rating scale; PACA: Palliative Care Assessment; CAMPAS-R: comprehensive measure for palliative care for patients; VAS: visual analogue scale; CAMPAS-P: comprehensive measure for palliative care for professionals; APCA POS: African Palliative Care Association African Palliative care Outcome Scale; RSCL: Rotterdam symptom checklist; MCPAC: multidimensional continuous pain assessment chart; FACT-L: Functional Assessment of Cancer Therapy-Lung; EC: Emergency Centre.
Articles ordered by quality assessment sum score. Articles, which do not present scores, describe the same study as the article immediately above.
Narrative synthesis framework
Element 1: the role of theory in evidence synthesis
We draw on work conducted in other fields, including an adaptation of the Slade 70 model, and on the early social and behavioural psychology theories, which are the base for organisational theories of change.15,18 The model (Figure 2) takes into consideration that implementation is an ongoing dynamic process, and that staff from any setting with particular characteristics and rules are individuals with ongoing cognitive and emotional processes. These influence how they relate and work with colleagues, patients and families and how they react to change.
Model describing implementation steps and the presence of facilitators and barriers throughout the process.
Element 2: developing a preliminary synthesis
Tabulation allowed us to find, at an early stage of the analysis, that there were no intervention studies of implementing facilitators to overcome barriers when using a PROM in palliative care clinical practice. This was an important finding, which allowed for the integration and analysis of the data in a way that was most informative but still answered our question. Then, thematic analysis was performed. We first applied our a priori three main themes: facilitators, barriers and lessons learned (see Appendix 2 for all data extracted). Most data extracted from the included studies were in the form of narrative observations located in the ‘Discussion’ and ‘Conclusion’ sections. In-depth data explicitly reported in the ‘Results’ section were also extracted, mainly from the focus groups studies and the web-based online survey study.
Element 3: exploring relationships within and between studies
After integrating the data in the main themes, in-depth inductive analysis led to the creation of five different categories for facilitators and lessons learned and six categories for barriers, namely, management, education, tool specific, clinical utility, financing and attitudes. All categories are presented in Table 3 accompanied by an illustrative quote per category.
Categories of extracted facilitators, barriers and lessons learned.
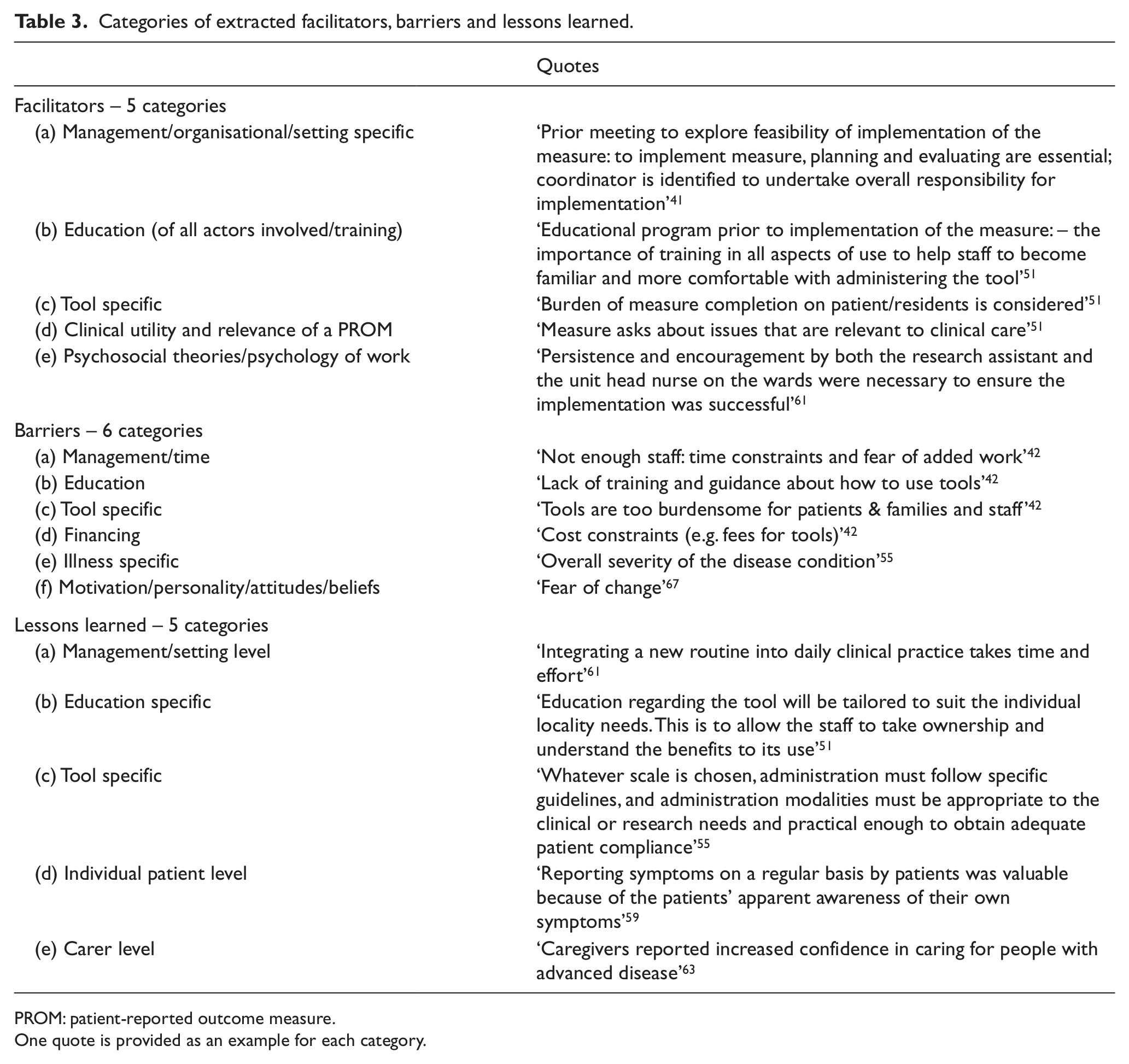
PROM: patient-reported outcome measure.
One quote is provided as an example for each category.
In addition, as analysis continued, a different typology emerged. This led us to reorganise the data in a timeline. We suggest three sequential steps at different levels (see Appendix 3 for detailed data): (a) preparation, with different actions put in place simultaneously at management level, health-care professional level and patient level; (b) implementation, in which the measure is taken into clinical practice, and different tasks are fulfilled at different levels and (c) assessment and improvement, which begins with the implementation step and involves discussion and potential changes of actions previously implemented. Hence, data were organised by those three sequential steps including barriers, facilitators and lessons learned for each. Similarities between studies emerged as some facilitators, barriers and lessons learned appear to be common to all sequential steps. Furthermore, by categorising the data as described (Figure 3), it seemed that some barriers discussed in some studies were being answered/resolved by facilitators and lessons learned mentioned in other studies. By exploring these relationships, we were able to link different concepts and synthesise them in the form of recommendations for implementing PROMs in palliative care clinical practice (Table 4).
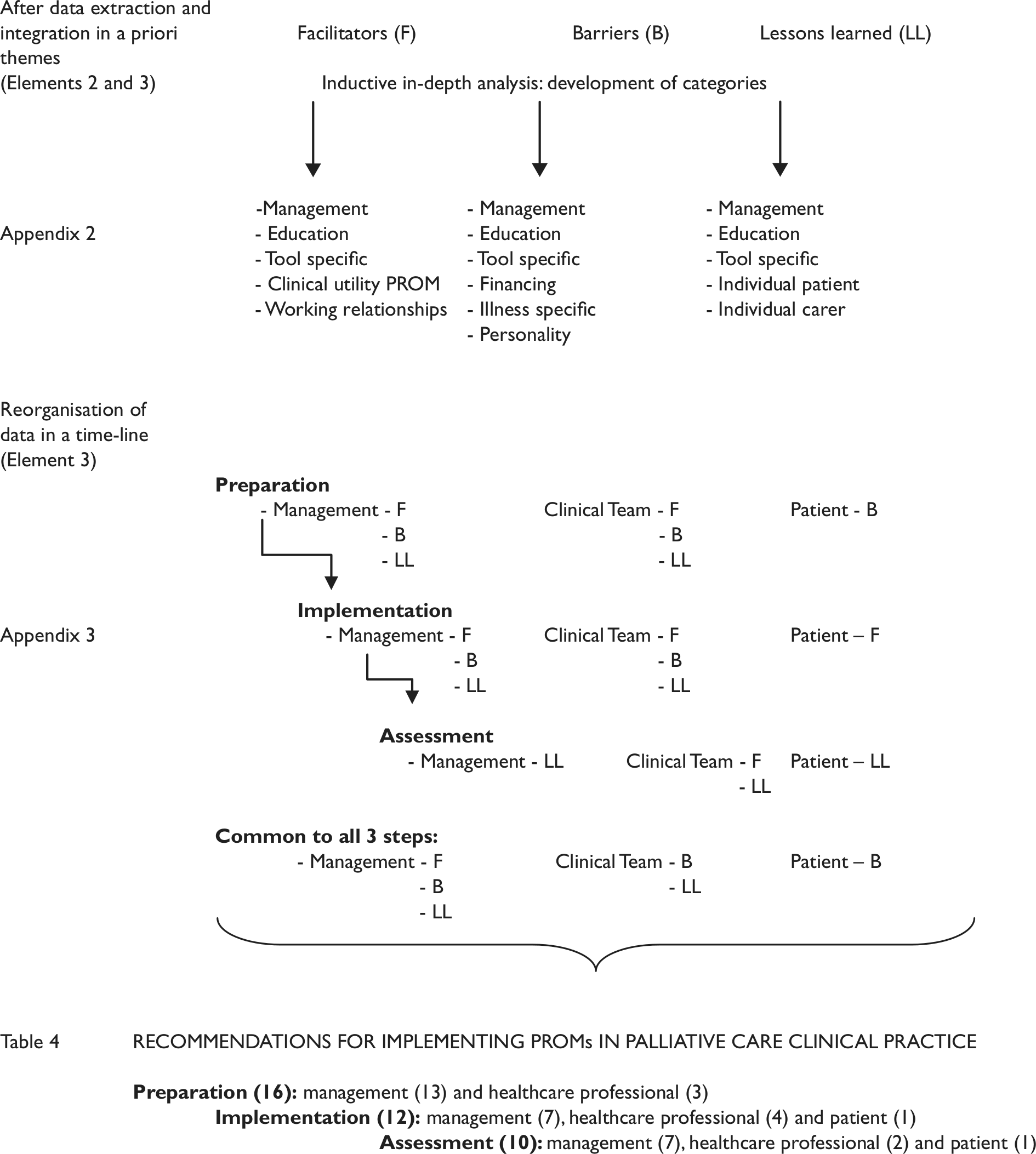
Sequential steps of analysis from the data extraction stage leading to the creation of the final recommendations.
Recommendations for implementation of PROMs in clinical practice per phases and at different levels.
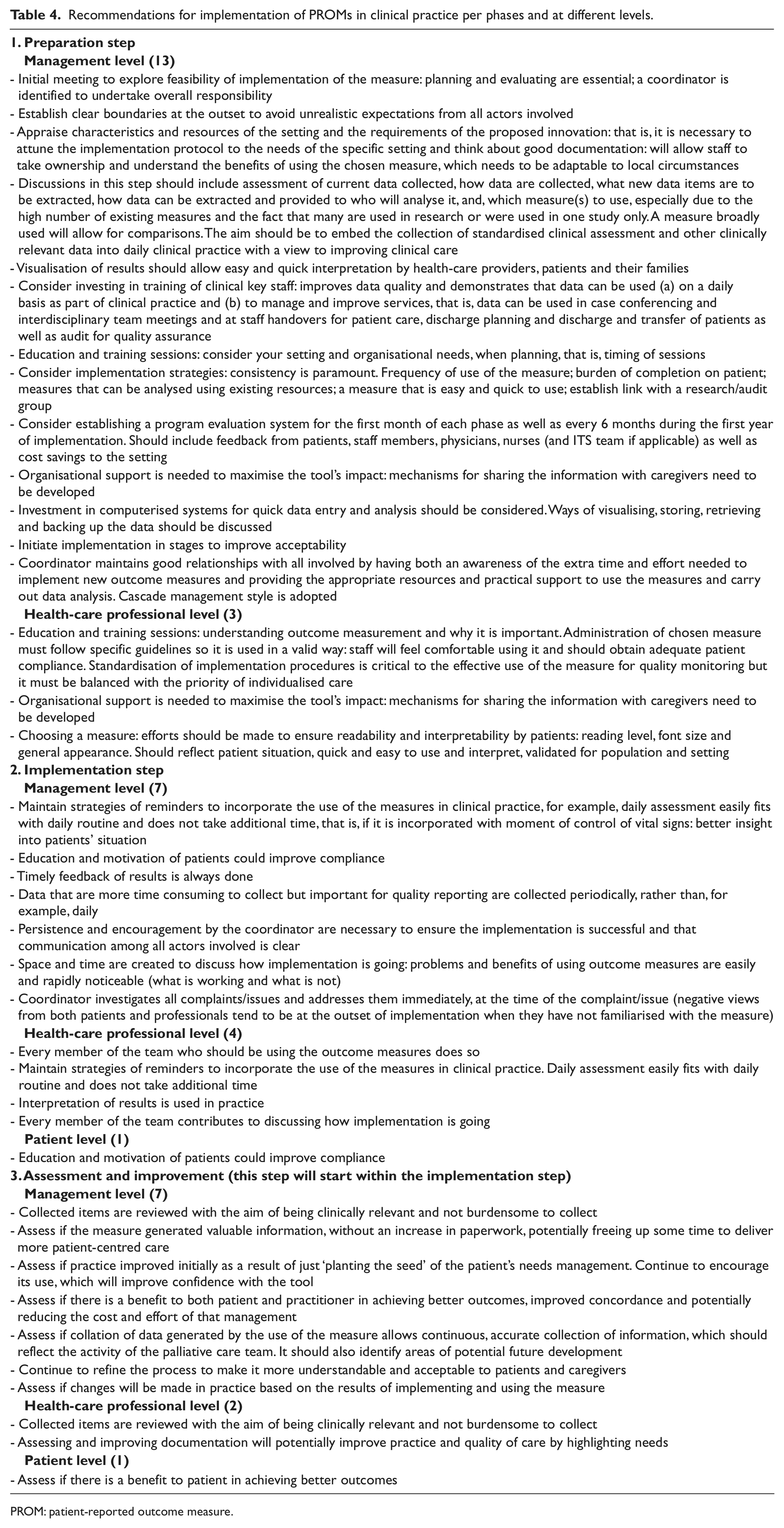
PROM: patient-reported outcome measure.
Element 4: assessing the robustness of the synthesis
We applied our quality criteria and categorised six qualitative studies as high quality because these scored 13 or more, two as medium quality having scored between 10 and 12 and one as poor quality since it scored below 10. Regarding the quantitative studies, 10 were rated high quality for scoring 11 or higher, and a score of 10 was rated as medium quality; however, there were no studies with this score, and seven studies scored 9 or below and so were rated as poor quality (Table 2).
Discussion
To our knowledge, this is the first systematic review that specifically identifies and appraises facilitators and barriers and draws recommendations of implementation of PROMs in clinical practice in palliative care. Although there were no intervention studies identified in this review, the qualitative data provided structured, in-depth information about the facilitators, barriers, needs and lessons learned when implementing PROMs in palliative care clinical practice. The quantitative studies identified did not meet our inclusion criteria as primary aims but provided useful data as secondary outcomes or process data from the original studies.
Our main findings are in line with our initial theory based on work conducted in other fields. First, during the implementation process, there is the need to acknowledge interpersonal relationships between the clinical team members and the ongoing emotional and cognitive processes that occur in each individual. Fear of change, feeling that one is being assessed and that one’s work is open to criticism due to the results that PROMs might show, and fear of added work are a few of the concerns that may lead to behaviour, which opposes change. Therefore, a firm but sensitive leadership seems to be needed to motivate individuals and reassure them that the use of PROMs is beneficial and ultimately aims to improve the quality of care provided to patients (Appendix 2, management category). Allowing individuals to take ownership of the measures rather than mandating their use may be important to avoid conflict. Providing feedback to clinicians appears to be a powerful tool to influence beliefs and attitudes towards the use of PROMs in clinical practice (Appendix 2, clinical utility). Some authors have used organisational theories as a backdrop to inform and design indicators to measure the quality of delivery of health care in general practice. 71
Second, implementing a PROM in palliative care clinical practice appears to benefit from careful planning of three distinct phases or steps (Appendix 3). The preparation phase involves (a) ensuring all health-care professionals are comfortable with changes planned and having a coordinator who will be in charge, (b) an education component and (c) selection of the measure(s) to be used. The latter is becoming more complex due to the high number of existing measures, many used only in research and/or just used in one study. This may not provide enough information about the measure in terms of using it in practice. Hence, the educational component seems to be key because if met, it will allow for clinicians to (a) understand why a measure is needed and how it could potentially benefit their practice; (b) learn about the measure(s), which will be implemented, namely, measurement properties, design and scoring system(s); (c) provide role play on how to explain PROMs usage to patients; (d) explore interpretation of results at different levels to benefit not only the individual patient but also the population, which the setting serves; (e) discuss the best options for storing and managing the collected data; and (f) understand the evaluation, which will follow. This seems to be the most time-consuming step. During the actual implementation, the results of each assessment point (previously decided, for example, daily, weekly, at each appointment) provide feedback on monitoring the patient’s progress and disease management. Having timely feedback on patient outcomes aids clinical decision-making and may enhance communication not only between patient and clinician but also within the multidisciplinary team. Finally, acknowledging what could be changed throughout the process is important in order to make the necessary enhancements with the overall aim of improving practice and the quality of care.
Implications for research
There are potential implications for future research that can be drawn from the findings, namely, whether the introduction of the measure(s) is an intervention in itself, regardless of the primary outcome of the study. Perhaps, there is an adjustment phase that needs to be taken into account before the actual main data collection takes place. It might be important to consider whether study protocols should include this period. There may be an impact on timing, that is, will the baseline be measured immediately after implementing the use of the PROM(s) or will there be a period of adjustment for the users to become more familiar with the measure(s). The same could be said about analysis: thought must be put into whether or not to include the data collected in that period of time in the analysis, considering that misuse of the measure(s) may have an impact on the strength and validity of results.
Strengths and limitations
One strength of this review is the heterogeneity of the included studies. These come from a large number of different countries as well as from different settings, which suggests that issues related with implementing PROMs are common and universal to clinical practice in palliative care. Furthermore, the fact that different measures were used in the included studies helps to clarify that challenges in implementing PROMs are not exclusive to the characteristics of the chosen measure, but actually depend on an additional number of factors. The same can be said with regard to the different populations in which the included studies were conducted. This suggests that the findings from this review are applicable to a variety of settings. In addition, we originally aimed at identifying facilitators and barriers to the implementation of PROMs in clinical practice in palliative care only. Using the narrative synthesis approach allowed us to go further and explore the relationships between the different studies. This led to reorganise and synthesise the data in the form of recommendations.
Nevertheless, there are some limitations, starting with the quality assessment, which was not an exclusion criterion, and therefore, articles were not excluded even if rated as poor quality. Second, there was some discussion between reviewers on how to categorise and present these data, mainly because some clauses fit more than one theme, and repeating those clauses would be more beneficial and accurate. However, the size of the appendices was already substantial, and there was no information lost by not using repetition. Third, the wording in the literature is somewhat confusing: the ‘benefits/advantages’ of using PROMs is not the same as facilitators of implementation and ‘disadvantages’ of usage of PROMs is not the same as barriers to implementation. This is subjective and open to personal interpretation. Another potential bias in this review is that there was only one reviewer including/excluding articles, although a second reviewer would be consulted if there were doubts after assessing the full text. Furthermore, only one reviewer developed the categories to synthesise the data, although a second reviewer appraised those and commented on them. In addition, the grey literature was not searched.
Conclusion
Implementing PROMs in palliative care clinical practice is an ongoing interactive and continuous process. There is a need to identify and address potential barriers to a successful implementation of PROMs in clinical practice, using appropriate facilitators, tailored to the characteristics of each setting. A key facilitator has to do with the role of a coordinator/facilitator throughout the implementation process. It is important to recognise the ongoing cognitive and emotional processes of individuals when change is being planned and implemented. The educational component for health-care professionals prior to the implementation is also paramount. This could promote ownership and correct use of the measure selected. Ideally, this measure should be short and screen for different palliative needs. Online resources and training courses on outcome measurement and PROMs for clinicians and researchers are starting to emerge. 72 Collaborations such as the Outcome Assessment and Complexity Collaborative (OACC) project are also a step forward in implementing PROMs is clinical practice in palliative care. 73 In conclusion, there is a need for guidance on implementing PROMs in palliative care clinical practice, which could potentially improve practice and the quality of care provided by assisting in clinical decision-making.
Footnotes
Acknowledgements
The authors would like to thank Vera Sarmento (V.S.) and Natália Calanzani (N.C.) for being the second reviewers and helping to achieve robust reliability procedures; all the colleagues at the Cicely Saunders Institute for very helpful comments and insights into earlier stages of the article; and Tom Osborne for valuable comments on the final version of the article. The authors also acknowledge EUROIMPACT collaborators: Van den Block Lieve, Meeussen Koen, Brearley Sarah, Caraceni Augusto, Costantini Massimo, Francke Anneke, Harding Richard, Higginson Irene, Kaasa Stein, Linden Karen, Miccinesi Guido, Onwuteaka-Philipsen Bregje, Pasman Roeline, Pautex Sophie, Payne Sheila and Deliens Luc.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
European Intersectorial and Multidisciplinary Palliative Care Research Training (EURO IMPACT) is funded by the European Union Seventh Framework Programme (FP7/2007-2013, under grant agreement number [264697]). EURO IMPACT aims to develop a multidisciplinary, multi-professional and inter-sectorial educational and research training framework for palliative care research in Europe. EURO IMPACT is coordinated by Prof. Luc Deliens and Prof. Lieve Van den Block of the End-of-Life Care Research Group, Ghent University and Vrije Universiteit Brussel, Brussels, Belgium. Other partners are VU University Medical Center, EMGO Institute for Health and Care Research, Amsterdam, the Netherlands; King’s College London, Cicely Saunders Institute, London, Cicely Saunders International, London, and International Observatory on End-of-Life Care, Lancaster University, Lancaster, United Kingdom; Norwegian University of Science and Technology, and EAPC Research Network, Trondheim, Norway; Regional Palliative Care Network, IRCCS AOU San Martino–IST, Genoa, and Cancer Research and Prevention Institute, Florence, Italy; EUGMS European Union Geriatric Medicine Society, Geneva, Switzerland; Springer Science and Business Media, Houten, the Netherlands.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.